


Abstract
Background Navigation increases the precision and safety of pedicle screw placement and has been used to place interbody cages for lateral lumbar interbody fusion. Single-position surgery shortens its duration and that of anesthesia. The aim of this study was the feasibility of simultaneous cage and screw placement in a single prone position using intraoperative navigation without the need for additional fluoroscopy and a detailed technical description of this procedure.
Methods We retrospectively analyzed 15 patients who underwent simultaneous navigated lateral lumbar interbody fusion and posterior instrumentation in a single prone position. A detailed technical description of the procedure is provided. Surgery duration, blood loss, complications, and radiographic parameters were recorded.
Results A total of 24 cages were placed in 15 patients. The mean time taken for cage placement was 21 ± 6.70 minutes, and there were no major complications. Mean surgery duration and blood loss per case, including posterior instrumentation, were 263 ± 94 minutes and 315 ± 143 mL, respectively. There were significant improvements in pre- to postoperative Oswestry Disability Index scores (51.38 ± 15.93 vs 32.81 ± 17.18, P < 0.001) and segmental lordosis (3.26° ± 8.97° vs 13.09° ± 15.25°, P < 0.001).
Conclusion The present study’s results showed the feasibility of lateral lumbar interbody fusion using simultaneous posterior pedicle screw instrumentation and intraoperative navigation in a single prone position.
Clinical Relevance Navigated lateral lumbar interbody fusion and posterior instrumentation in a single prone position possibly reduces operating time and blood loss and reduces exposure of operation room personnel to radiation.
Level of Evidence 4.
- extreme lateral interbody fusion (XLIF)
- lateral lumbar interbody fusion (LLIF)
- intraoperative navigation
- prone
- minimally invasive spine surgery (MIS)
- single-position spine surgery
Introduction
The sagittal balance of the spine is a critical determinant of clinical outcomes in the surgical management of degenerative spine diseases. Le Huec et al conducted an extensive literature review that revealed a robust relationship between sagittal balance and postoperative results.1 They underscored the paramount importance of maintaining optimal sagittal alignment to ensure favorable outcomes. Positive sagittal balance and misalignment, suggesting an anterior shift of the gravity line, stand out as a significant contributing factor to adult spinal deformity and its ensuing complications, further corroborating this correlation and illustrating the pivotal role of radiographic spinopelvic parameters in assessing disability in adult spinal deformity patients.2,3 Therefore, positive sagittal balance has been extensively associated with chronic back pain and decreased quality of life.1,2,4 Restoring sagittal alignment and balance not only reduces pain but also enhances quality of life while reducing the risk of adjacent segment disease and mechanical instrumentation failure.1,5–10 Moreover, comparative studies by Smith et al reinforced the imperative of surgical intervention in achieving satisfactory outcomes for adult spinal deformity.7 Nevertheless, the quest for optimal postoperative standing balance remains challenging, as outlined by Schwab et al and Scheer et al, who delved into the ramifications of the under- and overcorrection of sagittal deformities.8,9
Sagittal alignment and balance can be corrected effectively using a variety of surgical techniques, including osteotomies. A spectrum of minimally invasive spine surgery approaches has emerged, including anterior or lateral approaches using hyperlordotic cages for interbody fusion.11 Techniques such as pedicle subtraction osteotomy also provide substantial corrections of sagittal imbalance, albeit with greater surgical invasiveness than with lordotic cages. Among minimally invasive spine surgery techniques, the lateral lumbar interbody fusion (LLIF) approach has distinct advantages. LLIF facilitates the positioning of large interbody cage implants through the retroperitoneal space and psoas muscle. The cage spans the ring apophysis of the vertebral body, thereby allowing copious corrections of lost disc height and lordosis while minimizing the risk of subsidence. This procedure also has the advantages of providing indirect decompression and diminishing soft tissue trauma.12–14
This is commonly a 2-staged procedure involving interbody cage placement accompanied by posterior pedicle screw instrumentation that provides a rigid construction facilitating interbody fusion and further minimizing subsidence risk.15,16 While other techniques have been described, placement of the posterior screw construct is commonly performed after moving the patient into a prone position.17–19 Pedicle screw placement using computer-assisted navigation has proved to be safer and more accurate than conventional, nonnavigated guided fluoroscopy techniques.20–26 Although the placement of pedicle screws guided by intraoperative navigation has become a widespread standard in spine surgery, the placement of interbody cages continues to rely on fluoroscopy, thereby exposing the surgical team to elevated doses of radiation.27,28 Single-position protocols have since emerged, allowing simultaneous access to the anterior and posterior spine, streamlining surgical procedures, and decreasing the duration of surgery and anesthesia.18,19,29
The present study aimed to provide a detailed description of a surgical technique for simultaneous cage and screw placement using intraoperative navigation without the need for additional fluoroscopy, all performed in a single prone position. We present a series of 15 case studies demonstrating the approach’s feasibility and efficacy. The inclusion of complementary direct decompression procedures further enhances this surgical intervention’s efficacy.
Materials and Methods
The present analysis included 15 patients who underwent surgical restoration of their sagittal alignment using hyperlordotic cages placed using an LLIF approach between April 2021 and June 2023. All patients underwent simultaneous dorsal stabilization, including decompression if required, and posterior fusion performed by a second surgical team via pedicle screw instrumentation using a minimally invasive, paraspinal muscle–sparing approach30 in a prone position. In patients with degeneration of the L5/S1 segment, an anterior lumbar interbody fusion was also performed before repositioning the patient in a prone position. Age, sex, body mass index, pre- and postoperative Oswestry Disability Index (ODI),31 American Society of Anesthesiologists classification, total surgery duration, and blood loss were retrospectively recorded from patient files. Radiological data recorded included pelvic incidence, lumbar lordosis (LL), the segmental lordosis of each instrumented segment, and sagittal vertical axis, all measured preoperatively and at the last follow-up.
Surgical Technique
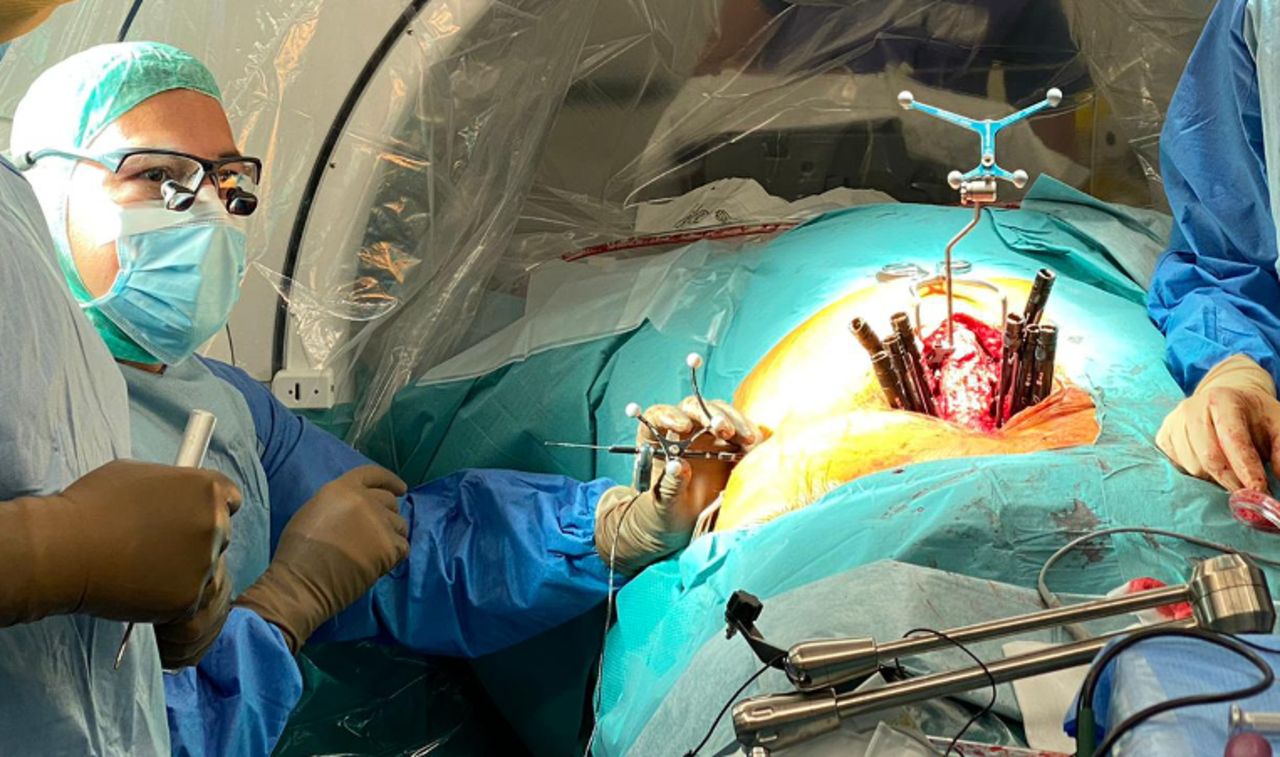
After general anesthesia and the placement of the electrodes necessary for continuous, triggered neuromonitoring (NV5, Nuvasive Inc., San Diego, CA, USA), all patients were placed on a Jackson table (Mizuho OSI, Union City, CA, USA) in a prone position, slightly tilted to the right (15°) to expose their left flank. The table’s hip pads were positioned as distal as possible to allow safer additional tilting if needed, and the authors secured patients with thick tape across their upper thoracic region and hips (Figure 1). To allow for additional table tilting and to provide resistance for implant placement, a cushioned chest support was mounted on the Jackson table on the contralateral side of the incision for the transpsoas approach (Figure 2). On the ipsilateral side of the incision, a second rail was mounted on the Jackson table for the clamp serving as an attachment point for the articulated arm needed to position the MAS retractor (Maxcess, Nuvasive Inc., San Diego, CA, USA; Figure 3).

Patient positioned on the Jackson table and draped for simultaneous access using the posterior and lateral approaches, slightly tilted to the contralateral side of the extreme lateral interbody fusion incision.

A post mounted on the contralateral side of the extreme lateral interbody fusion incision avoids moving the patient and provides resistance for implant placement.

The cage trajectory and size are planned using intraoperative navigation.
The placement of pedicle screws and interbody cages was guided via free-running neuromonitoring (NV5, Nuvasive Inc., San Diego, CA, USA) that mapped the lumbosacral plexus and via intraoperative stereotactic navigation (StealthStation S8, Medtronic Sofamor Danek, Memphis, TN, USA) that acquired image data intraoperatively using the O-Arm imaging system (Medtronic Sofamor Danek, Memphis, TN, USA). After prepping and draping the patient in a way that would allow simultaneous posterior and lateral access, a midline skin incision was made, and the reference frame of the navigation system was mounted on an exposed spinous process (Figure 4). Placing the reference frame required careful selection of the appropriate spinous process according to the preoperative surgical plan—it is paramount to avoid the need for repetitive image acquisition. Whether the reference frame is cranial or caudal, the ensuing cages should be placed, in order, from the distal spinal levels toward the reference frame. Screw instrumentation and cage placement were performed simultaneously by 2 surgical teams after the intraoperative acquisition of the required image data for the navigation system. Intraoperative images were acquired with the surgical team outside the operating room to minimize exposure to radiation. Posterior instrumentation was performed using a minimally invasive, muscle-splitting approach in all cases.30 In cases involving bony nerve root compression at the level of the lateral recess, where indirect decompression alone might fail, a complementary direct decompression was performed by removing the inferior and superior articular processes at the corresponding levels using a high-speed burr and chisel via the same approach.32

A post mounted on the contralateral side of the extreme lateral interbody fusion incision avoids moving the patient and provides resistance for implant placement.
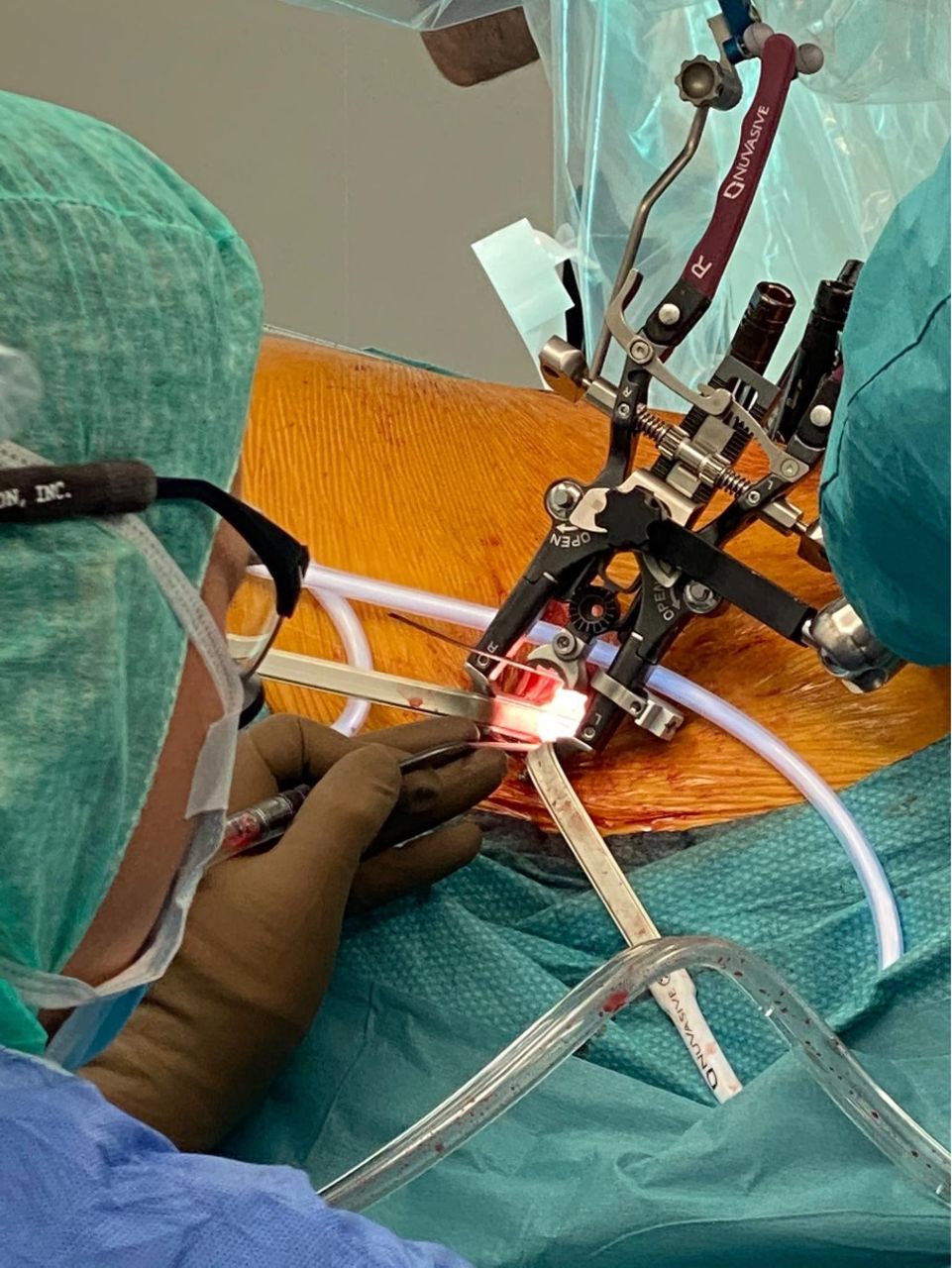
All patients underwent a left-sided transpsoas placement of the interbody cages, as previously described.11,33 An incision was made at the height of the index disc space after locating the adequate level and saving the projection of the trajectory of the cage using the navigation system (Figure 3). At this stage, rotating the table away from the surgeon by 15° helps to achieve a more ergonomic working position. The initial incision was followed by splitting the abdominal wall’s 3 muscle layers and the blunt dissection of the retroperitoneal space. On reaching the level of the psoas muscle’s lateral aspect, sequential dilation was used to split the muscle fibers for the final placement of the Kirschner wire and the standard retractor. The dilator was navigated using the SureTrak® System (Medtronic Sofamor Danek, Memphis, TN, USA; Figure 5). This system allows the surgeon to calibrate third-party instruments to integrate them with the navigation system; it was used in conjunction with triggered electromyography neuromonitoring (NV5, Nuvasive Inc., San Diego, CA, USA) to position the Kirschner wire in the appropriate disc, avoiding damage to the lumbar plexus by mapping its position. With the Kirschner wire in place, the retractor was docked and secured to the index level using an intradiscal shim.

Navigation of the dilator using the SureTrak system for positioning the Kirschner wire.
Placement and opening of the retractor were followed by the discectomy and the final placement of an appropriately sized cage filled with synthetic bone filler (Attrax, Nuvasive Inc., San Diego, CA, USA; Figure 6). To reduce the risk of neurapraxia of the lumbar plexus, surgeons strived for the shortest retraction time possible. The time from opening the retractor to the final placement of the cage was defined as the duration of cage placement.

Docking and fixation of the standard retractor.
This study was approved by the local ethics committee (No. 2021–00663).
Statistical Analysis
Statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are reported as mean ± SD, whereas categorical variables are reported as frequencies and proportions. Statistical significance between paired samples was calculated using the Wilcoxon signed rank test. A P value of 0.05 was considered statistically significant.
Results
Fifteen patients with different indications underwent successful LLIF using a lateral transpsoas approach in a single prone position using intraoperative navigation without the need for fluoroscopy. The mean patient age was 63 ± 15.60 years, and 12 (80%) were women. Further demographic data and surgical details are shown in Table 1. Median follow-up was at 12.5 months, ranging from 9 to 23 months. The mean ODI score was 51.38 ± 15.93 preoperatively vs 32.81 ± 17.18 (P < 0.001) postoperatively. The mean pelvic incidence was 53.53° ± 8.69°.
Demographic and surgical data of patients undergoing LLIF using a transpsoas approach.
LLIF was performed at 24 separate levels, with a mean duration of 21 ± 6.70 min/level. Mean surgery duration and blood loss per case, including posterior instrumentation, were 263 ± 94 minutes and 315 ± 143 mL, respectively. An additional foraminotomy (complementary direct decompression) was performed on 13 levels, either 1 or 2 foramens. Two cases benefitted from fully indirect decompression alone. In 4 cases, the instrumentation was complemented by an anterior lumbar interbody fusion at the L5/S1 level, using an anterior approach. No fluoroscopy was used to place the cages and screws. In 9 cases, just 1 intraoperative O-arm scan was performed, with 2 scans performed in 4 cases, and 3 scans performed just once, depending on the fusion levels. Regarding intraoperative complications, cerebrospinal fluid leakages occurred in 2 cases due to dural tears, and cage subsidence was recorded once.
One patient required a surgical revision of their posterior incision 3 weeks after the index procedure because of a delay in superficial wound healing. Otherwise, no postoperative complications were noted.
Radiographic parameters were recorded preoperatively and at the last follow-up. There was a significant difference between the pre- and postoperative segmental LL in segments where an interbody fusion had been performed (3.26° ± 8.97° preoperatively vs 13.09° ± 15.25° postoperatively, P < 0.001). However, there were no significant differences in pre- and postoperative total LL or sagittal vertical axis. A detailed description is shown in Table 2.
Radiologic data: pre- vs postoperative findings.
After 1-year follow-up, none of the patients in this cohort required revision surgery as a result of implant loosening.
Case Study
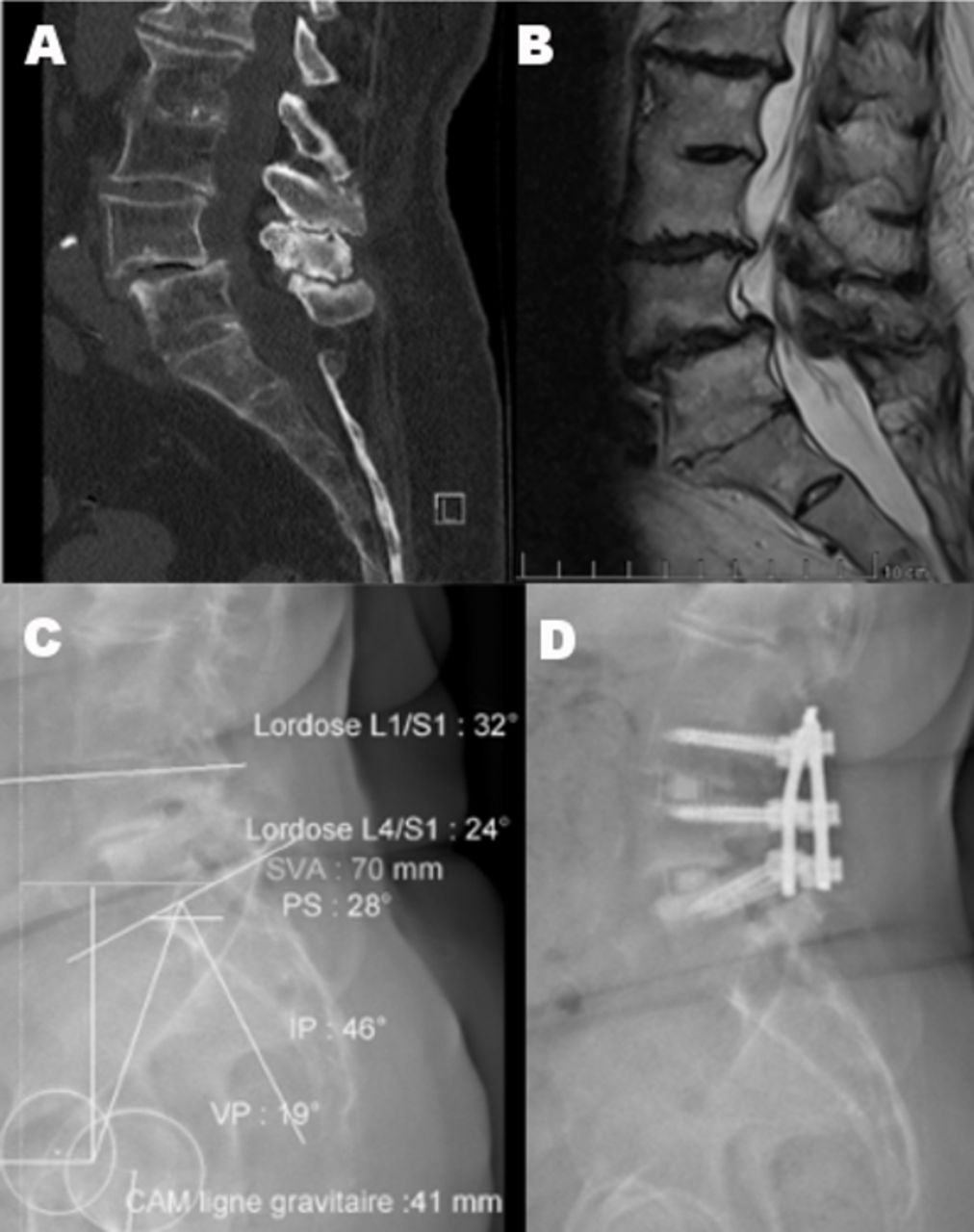
An 81-year-old woman presented with long-standing lower back pain and bilateral radiculopathy with shooting pain radiating into the L4 dermatome. She had not been responsive to nonoperative therapy. A radiologic work-up involving computed tomography (CT), magnetic resonance imaging, and full-spine x-ray(EOS imaging) revealed an L3-L4 discopathy with right-sided foraminal stenosis and a degenerative, mobile Meyerding Grade I slip spondylolisthesis at L4-L5 with a concurrent Schizas C lumbar spinal stenosis.34,35 The L3-L4 and L5-S1 segments were fused (Figure 7). The patient underwent simultaneous navigated LLIF and posterior pedicle screw instrumentation with bony decompression at L3-L4 and L4-L5 via a paraspinal muscle-sparing approach, as described above. The patient was discharged 8 days after surgery and had complete resolution of preoperative pain, no significant postoperative pain, and no complications.

(A) Computed tomography image showing degenerative spondylolisthesis. (B) Magnetic resonance imaging showing lumbar spinal stenosis. (C) Preoperative radiograph. (D) Postoperative radiograph.
Discussion
Intraoperative stereotactic navigation is widely used for the placement of pedicle screws and has proved to be safer and more accurate than free-hand or fluoroscopy-guided techniques.20–26 Several authors have reported their experiences of using stereotactic navigation for LLIF in a prone position.29,36–43 However, literature considering navigated simultaneous screw and cage placement in a prone position is sparse.29 The present study aimed to provide a detailed description of the authors’ experiences with 15 consecutive cases and demonstrate the feasibility of LLIF and simultaneous posterior pedicle screw instrumentation in a prone position using intraoperative navigation only.
A total of 24 cages were placed, in an average time of 21 min/cage. This finding reflected the results of other authors reporting on the duration of implant placement in prone or lateral positions.18,19 In addition to the time required for a surgical approach and the implant’s actual placement, a standard, fluoroscopy-guided LLIF procedure demands precise and time-consuming patient positioning to achieve exact anteroposterior and lateral views of the index level in order to avoid misplacement of the interbody implant. Furthermore, operating table adjustments and fluoroscopic confirmation are highly recommended for each level in multilevel surgery.17,33
Although multiple studies have demonstrated a linear correlation between poor quality of life and a positive sagittal imbalance, data showing a correlation between surgical correction of those sagittal imbalances and quality of life are lacking.44 After a median follow-up of 12.5 months, the patients in our study reported significant improvements in their ODI scores and in their segmental lordosis. However, there were no significant improvements in their sagittal vertical axis or total LL values. The literature presents mixed findings regarding the effect of LLIF on LL. Several studies indicate that LLIF can lead to significant improvements in LL, while other studies suggest that the degree of improvement in LL may not be uniform across all patients or surgical contexts.45–48 Different authors reported comparable results in patients treated with LLIF where, although significant changes in segmental lordosis were observed, the change in LL did not reach statistical significance.48,49 This highlights the fact that pain associated with lumbar degeneration and subsequent sagittal dysbalance, particularly in the context of a compensated deformity with preserved global sagittal parameters, might be attributed to compensatory mechanisms including pelvic retroversion.50 Hence, the reported improvements in this cohort might be attributable to the relief of compensatory mechanisms, including knee and hip flexion or increased pelvic tilt.51
The technique described in the present study enables multilevel surgery via a single approach by simply moving the standard retractor, under the navigation system’s guidance, without the need for further imaging or adjustments to the patient’s position. Furthermore, in cases where direct access and a straight trajectory to the disc space are complicated by the iliac crest or the position of the lumbar plexus, the combination of stereotactic navigation and triggered neuromonitoring enabled dynamic adaptations to the retractor’s position and the cage’s trajectory to the patient’s anatomy. We also observed, as described in the literature, that the lumbar plexus was positioned more posteriorly than anticipated after studying the preoperative images.52 In this case series, we used intraoperative stereotactic navigation based on intraoperatively acquired imaging using the O-arm to determine the level of the index disc as well as the trajectory and final placement of the cage, including its size in the anteroposterior and lateral directions. This completely eliminated the need for intraoperative fluoroscopy. This approach reduces the radiation exposure of surgeons and surgical teams.27,28,43 However, in 5 cases, more than 1 intraoperative scan was needed to obtain the necessary imaging data for intraoperative navigation. Additional O-arm scans were required either when the navigation system’s precision was found to be insufficient or when the required posterior instrumentation’s length exceeded the O-arm’s technically possible scanning width (40 cm). The navigation system uses an electro-optical camera to track probes and instruments relative to passive markers on a patient-mounted reference frame. Precise placement of the reference frame is essential to avoid inaccuracies in the navigation system and the need for multiple scans that would expose the patient to elevated levels of radiation. Segmental distraction caused by the placement of the hyperlordotic cages will lead to navigation system inaccuracies on adjacent segments. This must be considered when planning the order of screw and cage placement, which should be performed from the most distal level relative to the reference frame back toward the reference frame level. Specifically, in a construct involving multiple segments, simultaneous screw instrumentation must always start with the most cranial segment, followed by the placement of the interbody cage. In cases involving fused segments within the planned construct, mounting the reference frame to a spinous process within the fused segments is recommended.
Lateral interbody fusion with posterior pedicle screw placement is commonly performed in 2 stages, with the patient being repositioned from a decubitus lateral position to a prone position for dorsal instrumentation.17 However, both the single lateral and single prone procedures have previously been described in the literature, demonstrating a shorter total time under anesthesia, a smaller number of manipulations needed to change the patient’s position, a shorter total surgical time, and less time spent in the operating room.18,19,53–56 The present study was unable to reproduce these surgical time savings, most likely as a result of the team’s ongoing learning curve and the inefficiencies of a newly implemented workflow.
The present study’s main limitations were its small sample size and the lack of a control group, both factors that limited the possibilities for statistical inference. Regarding the lack of a control group, the authors considered a comparison with sufficient data from the literature to be satisfactory. Furthermore, at the final follow-up, CT data to accurately determine radiographic fusion were not available. However, all patients achieved positive clinical outcomes without clinical signs of implant-related complications, such as loosening or nonunion on conventional radiographs, obviating the need for further CT imaging to confirm fusion status.
Nevertheless, the present results show the feasibility of using the LLIF procedure in a prone position guided by intraoperative navigation without the need for additional fluoroscopic imaging, thereby reducing surgical personnel’s exposure to radiation. All 15 patients included in this study underwent successful interbody fusion and posterior stabilization procedures with clinical outcomes and surgery durations comparable to those in the literature.
Conclusion
The study demonstrates the feasibility and effectiveness of performing simultaneous cage and pedicle screw placement using intraoperative navigation in a single prone position without additional fluoroscopy, resulting in significant improvements in patient outcomes comparable to existing literature.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests D.D. is an educational consultant for NuVasive Inc. The remaining authors have no disclosures.
Ethics Approval This study was approved by the local ethics committee (No. 2021-00663).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.