


Abstract
Background Fibrous dysplasia (FD) is an uncommon benign intramedullary fibro-osseous lesion. Cervical spine compromise is rare with only cases reported. Currently, the natural history of cervical FD is poorly understood, and its treatment remains controversial.
Methods A review of the literature was performed to analyze and discuss the management of cervical FD through a case report and literature review.
Results Cervical FD is a rare benign pathology. Clinical presentation is usually casual or only clinical pain. Computed tomography (CT)-guided percutaneous biopsy is a safe and effective technique for evaluation of spinal lesions; however, the accuracy of the preoperative biopsy findings has been disappointing. Although all treatments are valid, no one has been demonstrated to be better. Our proposed treatment, a corpectomy and fixation with a titanium mesh cage filled with allograft bone and an anterior cervical plate, showed good results.
Conclusions The rarity of cervical FD and the lack of detailed reports with long-term follow-up periods complicate the research on the optimal treatment approach in these cases, but apparently all are valid for pain control. In our case, a corpectomy and fixation with a titanium mesh cage filled with allograft bone and an anterior cervical plate was carried out and showed good results. We submit this surgery option to be considered in these rare type of injuries.
INTRODUCTION
Fibrous dysplasia (FD) is an uncommon benign intramedullary fibro-osseous lesion.1 The etiology of FD has been linked to an activating mutation in the gene that encodes the α subunit of stimulatory G protein located at 20q13.2–13.3.2 In FD the normal lamellar cancellous bone of medullar canal is replaced with immature fibro-osseous tissue, resulting in poorly formed trabeculae of immature woven bone, leading to its expansion, distortion, and structural weakness.3,4 This disease presents in either a monostotic (MFD) or polyostotic (PFD) form, and with or without endocrinopathy. The MFD form is the most frequent (70% of the cases reported).4
Typically, the FD is asymptomatic and discovered incidentally. However, some cases present with painful bone swelling or pathological fractures.1,3 Cervical spine compromise is rare with only 36 cases reported.1,3–30 Currently, the natural history of cervical FD is poorly understood, and its treatment remains controversial.4 The aim of this paper is to analyze and discuss the management of cervical FD through a case report and literature review.
CASE REPORT
A 46-year-old woman underwent cervical spine magnetic resonance imaging (MRI) for the investigation of a submandibular bultoma. MRI revealed a lytic lesion on the C6 right vertebral body involving the homolateral pedicle with hypo-intensity in T1 and T2, and hyperintensity in STIR that spread to soft tissues, with enhancement after intravenous contrast administration.
There was no family history of bone disease. Her medical history included history of cigarette smoking and hypothyroidism after hemithyroidectomy. On physical examination, the patient denied cervical pain, but reported occasional radiating pain down the left arm without loss of strength. She presented no abnormal pigmentation of the skin. Regular laboratory examinations including hemogram, thyroid, and hepatic function tests were normal. Serum calcium, inorganic phosphate, bone alkaline phosphatase, parathyroid hormone, and 25-hydroxyvitamin D were also normal.
Computed tomography (CT) scans of the cervical spine showed an expansive lytic lesion that affected the 2/3 of the C6 vertebral body and a discontinuity of the upper vertebral plate, compatible with a fracture, and alterations in bone trabeculation. Similar lesions were found in L5, S1, and S2. No other body lesions were detected by full body CT scan. The patient underwent a CT-guided percutaneous needle biopsy that revealed no signs of malignancy; however, no etiological diagnosis was obtained. With the results of the biopsy, FD was suspected, but other bone tumors and vertebral infection were also considered. Based on the radiologic findings, the lesions were thought to be PFD of the cervical spine.
The decision to proceed with surgery in this case was made based on the presence of C6 radiculopathy, and the risk of vertebral body collapse. According to Weinstein, Boriani, Biagini (WBB) stage, the lesion was considered as stage 3 benign tumor involving A–C layers and 6–9 zones extension (A–C; 6–9). Following WBB criteria, a wide excision was considered. An anterior cervical approach was performed, exposing C6 vertebral body. Subsequently, a biopsy and C6 corpectomy were carried out. The bone involved was easily removed with curettage and rongeurs. Vertebral reconstruction was performed with insertion of anterior titanium mesh cage (Moss-Miami System; De Puy Spine, Warsaw, Indiana) with allograft bone. Fixation plate and screws at C5-C7 (Sonoma Anterior Cervical Plate, Sea Spine, San Diego, California) were used for additional internal fixation. There were no perioperative complications. Histopathologic examination showed fibrous tissue within medullary bone and irregularly shaped bony trabeculae embedded in the fibrous stroma, consistent with FD. At the end of follow-up, 2 years after surgery, the patient progressed favorably without clinical or radiological recurrence. The L5-S2 lesion remained painless and there were no signs of vertebral collapse.
DISCUSSION
FD represents 2.5% of all bone neoplasms and 7% of benign bone neoplasms.31 MFD is more frequent (70%) than PFD (27%) or McCune-Albright (3%).1 FD affects children and young adults with equal sex distribution; only in McCune-Albright syndrome is there a female preponderance.3 Although any skeletal bone may be affected, cervical spine affection is rare.32 The aim of this study was to analyze and discuss the management of cervical FD through a new case report of polyostotic cervical FD and literature review on this matter. We conducted a systematic review of the available literature using various search strategies. The following databases were searched: MEDLINE, Scopus, PubMed, and Cochrane systematic reviews, using the terms “Fibrous Dysplasia,” “cervical tumors,” and “vertebral tumors.” Two authors (NJH and G-TP) completed the search separately, and the results were compared twice by each. The inclusion criteria were papers written in English and cases with sufficient epidemiologic data to be studied.
Since its first description, only 37 cases including ours have been reported to date, as summarized in Tables 1 and 2.1,3–30 There have been 22 cases of MFD (62%) and 14 cases of PFD (38%). All cervical spine levels were affected by the disease, especially C2 (16/36 cases). Sixty-seven percent of the patients reported were men; only in 2 studies the patient's sex was not indicated. Most patients were young adults with age between 11 and 61 years old. In most patients, the most common symptom was cervicalgia (16/36 cases) in some cases initiated after trauma. Neurological involvement happened only in 10 cases. It should be noted that information regarding gender, age, trauma, and symptoms was not always reported. Of 14 cases of PFD, 8 (57%) were men and 6 (43%) were women and they had a mean age of 37.6 years old (SD +/− 13). Our case was a PFD case, a woman 46 years old, with an incidental diagnosis and similar properties as those published.
Details of reported cases of fibrous dysplasia (FD) of the cervical spine.
Summary of reported cases of fibrous dysplasia of the cervical spine.
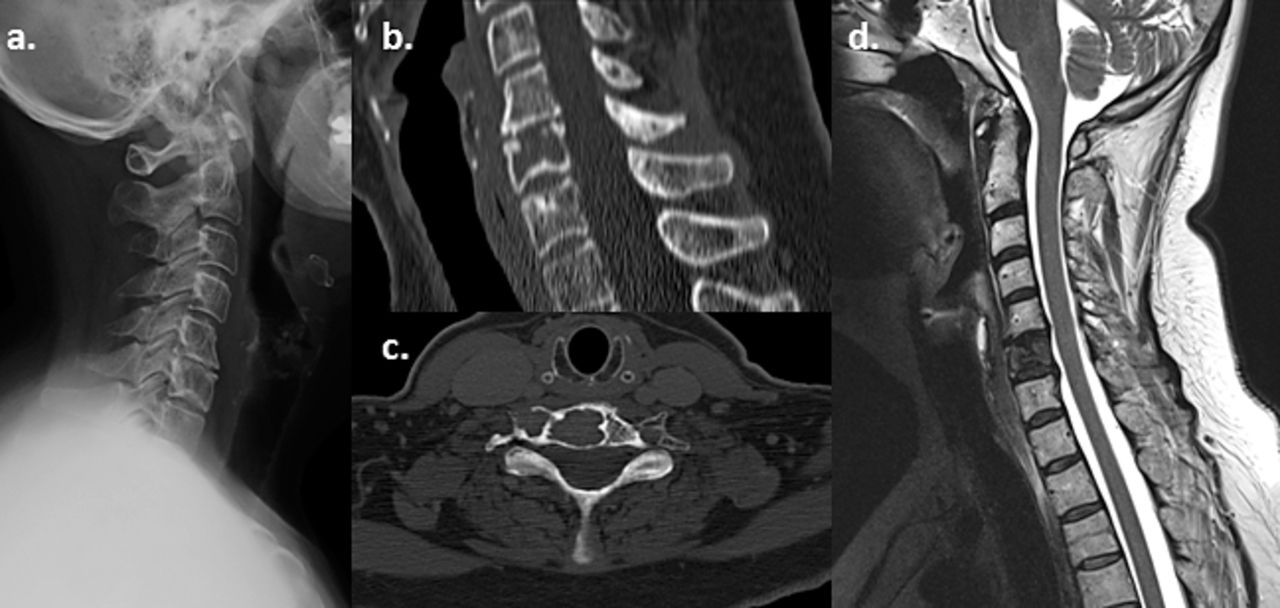
As in our case, the patients reported were studied by simple radiography. Expansive and lytic types were the most common radiological patterns.3,4,26 Our patient also underwent a CT scan and a MRI. CT is the best diagnostic tool to demonstrate the radiographic features of dysplasia.1,24 CT can confirm the reduction of lamellar cancellous bone and cortical thinning, as well as collapse of the vertebrae (Figure 1).28,32 In our patient, FD was associated with a solid component of soft tissue, with contrast enhancement. MRI is thought to be a sensitive tool to demonstrate the extent of tumor involvement, assess neural compression, and to establish differential diagnoses.4,24,32 FD appears as a hypointense homogeneous lesion in T1, except for pathological fractures.21 In T2, the lesion is heterogeneous depending on the amount of fibrous tissue, bone tissue, cellularity, cystic alterations, hemorrhage, and cartilaginous tissue.1,21,28 Administration of intravenous gadolinium produces a homogeneous lesion enhancement, like in our patient.21 Although we suspected cervical FD in our patient, a differential diagnosis was carried out. The differential diagnosis of FD includes hemangiomas, giant cell tumor, bone aneurismal cysts, Paget's disease, and osteoblastomas. In older patients, multiple myeloma or metastases should also be considered.1,21,32
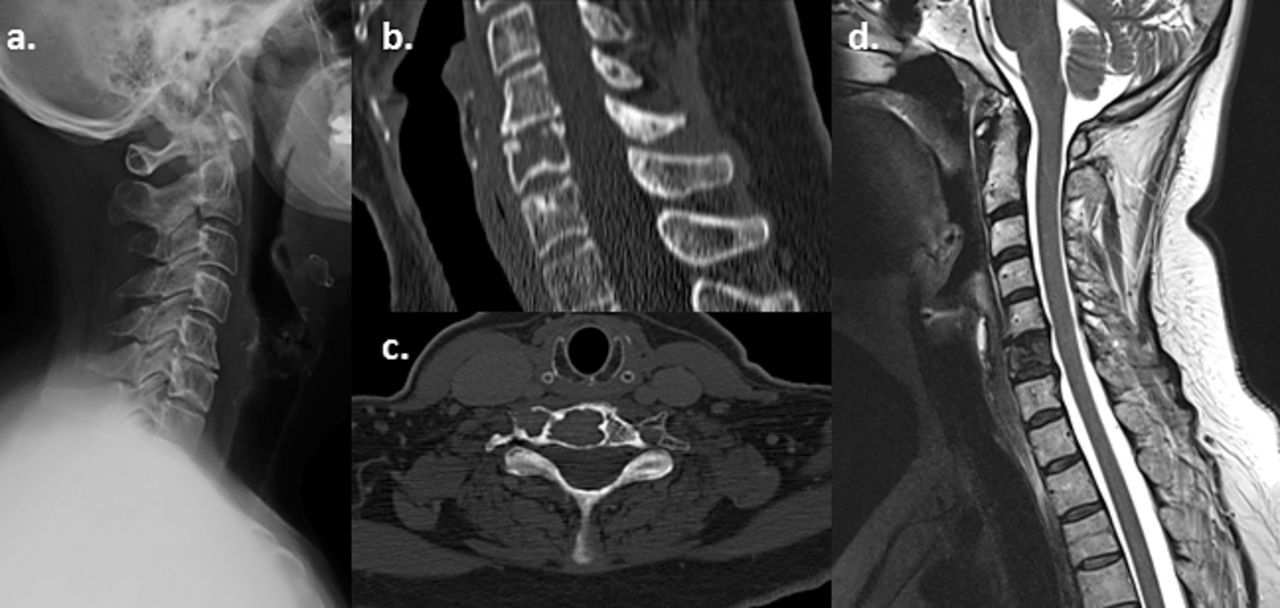
Preoperative imagings of our patient with cervical fibrous dysplasia. (a) Lateral cervical x-ray. (b, c) Sagittal and axial section of computed tomography showing an osteolytic image with a sclerotic margin in the C6 vertebral body and a superior vertebral disc discontinuity compatible with a fracture. (d) Sagittal section of magnetic resonance imaging shows a lytic lesion at C6 with hypointense sign in T2.
We performed a CT-guided percutaneous biopsy that ruled out malignancy, but failed to provide an etiological diagnosis. CT-guided percutaneous biopsy is a safe and effective technique for evaluation of spinal lesions, and the reported global diagnostic accuracy is approximately 90%.4,33 However, the accuracy of the preoperative biopsy findings in FD series has been disappointing.4 A possible factor that could explain the low diagnostic accuracy of FD may be its benign nature. Biopsies of benign tumors have an accuracy rate lower than that of malignant lesions. It could also be because FD is composed of different parts, including lytic, sclera, and soft tissue parts. To obtain a precise result, a representative specimen must be obtained with all components, especially in sclerotic lesions.34,35 As recommended by the literature, an open biopsy was carried out on suspicion of vertebral FD.4,21,32 In our patient, open biopsy and treatment were performed at the same time. Due to the risk of vertebral collapse, surgery was the treatment of choice in our case. The role of surgical treatment for FD is still controversial.23 In most cases of FD involving the nonaxial skeleton, conservative treatment is recommended, even after pathological fractures. The curative potential for all fracture sites has been reported to be 94%.35 Conservative treatment, particularly with PFD, has also been recommended in vertebral FD.36 Although, because of the low incidence of cervical spine FD and the scarcity of detailed reports with long-term follow-up, it is difficult to compare the effectiveness of the different treatment approaches.1,3–30 Moreover, some reports did not report the type of treatment of choice neither the follow-up period.6,11,18 The mean follow-up period of the 32 cases that did report the treatment's outcome was 28 months,1,3–30 with the exception of 1 case with a 20-year follow-up period.32 In our case, our follow-up was 24 months, at the end of this period our patient progressed favorably without clinical or radiological recurrence.
Nowadays, surgical treatment is indicated for persistent pain, neurological deficits, vertebral collapse, instability and/or cord compression.1,3–5,7–17,19–30,32 For these reasons, we decided to operate only on the C6 lesion and not on the L5-S2 lesions. Surgical goals in the present case were as follows: pathological diagnosis, removal of the lesion, and stabilization of the spine. In our patient, a biopsy, an anterior C6 corpectomy, and fixation with a titanium mesh cage filled with allograft bone and plate C5-7 was carried out. In our case, anterior instrumentation was sufficient; however, in the cases reported, surgical approaches varied. The anterior approach was used in cases in which, like in our case, the vertebral body was involved.1,3–5,7,9,28 Posterior decompression was performed when vertebral involvement was complete and when there was no clear anterior compression.4,8,10–12,14,15,17–27,29,30 A combined surgical approach, anterior and posterior, was used in only 5 cases.4,13,16,17
Like in our patient, and regardless of the therapeutic intervention, almost all surgically treated patients, as summarized in Table 2, demonstrated good outcomes, even those cases with demonstrated invasion of the graft by FD.16 In 8 of the studies in which the type of treatment was reported, the diagnosis was confirmed by biopsy and no additional treatment was instituted.4,5,7,9,19,28 In 1 case, only a decompression was performed.13 In 2 cases a vertebroplasty was done.4,23 Seven cases were managed with curettage and grafting4,8,12,14–16 and 14 cases were managed with complete excision with or without fusion on the basis of the resulting degree of spinal instability.1,3,4,17,20–22,24–27,29,30 Only 1 major complication has been reported: 1 patient who underwent combined anterior-posterior surgery developed a complete quadriplegia 4 hours postsurgery, and died eventually after 11 days.13

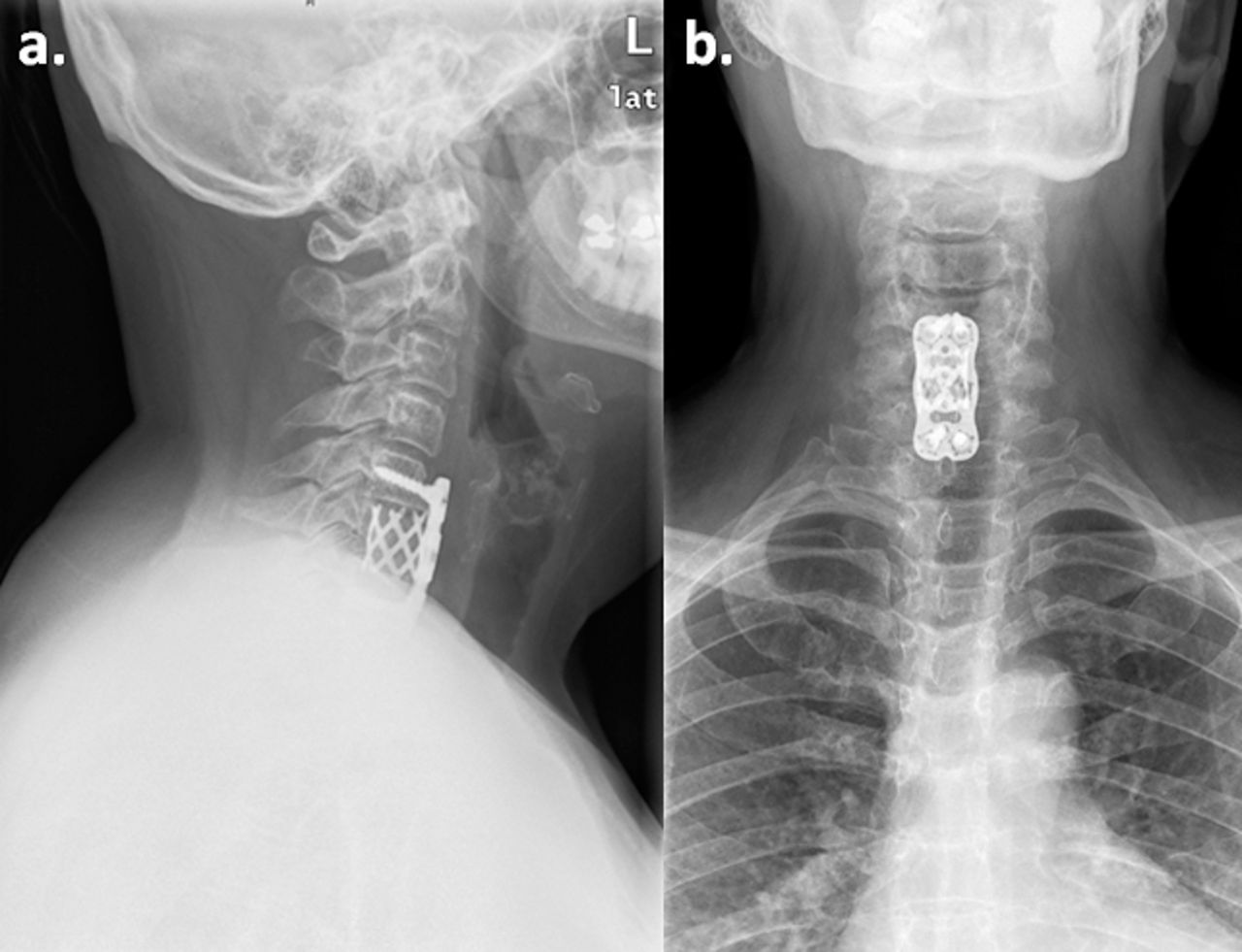
Postoperative imagings of our patient with cervical fibrous dysplasia. (a, b) Lateral and anterior-posterior cervical x-ray showing fixation with a titanium mesh cage with allograft bone at C6 level and an arthrodesis C5-C7 with ad anterior cervical plate.
CONCLUSIONS
FD has an approximately equal percentage of women/men, especially in PFD, and young patients (mean age of 37.6 years old [SD ± 13]). Clinical presentation is usually casual or only clinical pain. CT-guided percutaneous biopsy is a safe and effective technique for evaluation of spinal lesions; however, the accuracy of the preoperative biopsy findings in FD series has been disappointing. The rarity of cervical FD and the lack of detailed reports with long-term follow-up periods complicate the research on the optimal treatment approach in these cases, but apparently all are valid for pain control. In our case, a corpectomy and fixation with a titanium mesh cage filled with allograft bone and an anterior cervical plate was carried out and showed good results.
ACKNOWLEDGMENTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent was obtained from the participant included in the study.
Footnotes
Disclosures and COI: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2018 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.