


ABSTRACT
Background: Several studies have compared outcomes between hospital-based centers (HBCs) and ambulatory surgery centers (ASCs) following minimally invasive lumbar decompression (MIS LD). However, the association between narcotic consumption and pain in the immediate postoperative period has not been well characterized. As such, this study aims to examine pain, narcotic consumption, and length of stay (LOS) among patients discharged on postoperative day 0 following a 1-level MIS LD between HBCs or ASCs.
Methods: Patients who underwent a primary, 1-level MIS LD were retrospectively reviewed and stratified by operative location. Differences between groups in patient demographics were assessed using independent-sample t tests for continuous variables and χ2 analysis for categoric variables. The operative location and its effect on perioperative characteristics, inpatient pain scores, and narcotics consumption were analyzed using multivariate linear regression adjusted for significant patient characteristics.
Results: There were 235 patients identified, of whom 90 and 145 underwent surgery at an HBC or ASC, respectively. The HBC cohort exhibited an increased comorbidity burden and had a greater percentage of privately insured patients. The HBC cohort recorded shorter operative time and greater total estimated blood loss. Patients in the HBC cohort experienced prolonged LOS, and consumed greater total oral morphine equivalents compared with the ASC cohort. No differences were observed in the remaining outcomes.
Conclusions: The results of the current study suggest that patients who underwent MIS LD at an ASC received fewer narcotics than patients treated at an HBC, which may contribute to shortened LOS. Additionally, there was no difference in patient-reported pain between cohorts despite the differences in narcotic use. As such, postoperative narcotics administration varied, indicating HBC patients perhaps required more narcotic pain medications to achieve the same pain scores that were sufficient enough to allow patient discharge, thus prolonging LOS.
Level of Evidence: III
- lumbar decompression
- narcotic consumption
- inpatient pain
- same-day discharge
- hospital
- ambulatory surgery center
INTRODUCTION
Minimally invasive lumbar decompression (MIS LD) is one of the most common spinal procedures performed for the treatment of degenerative conditions.1,2 As the US population ages, the need for surgical treatment of degenerative conditions in elderly patients will continue to increase.1,3,4 With the rising demand for treatment of degenerative spinal pathology, outpatient surgery has received the attention of hospital institutions and private practices alike as a mechanism for efficient delivery of care.4–6 Several studies have demonstrated the feasibility, efficacy, and safety of outpatient lumbar decompression.3–8 When compared to hospital-based procedures, outpatient lumbar decompression procedures have demonstrated shorter operative and recovery times, reduced hospital costs, improved patient satisfaction, and risk of perioperative complications.2,4,9–11 As such, outpatient lumbar decompression has been increasingly used.
Narcotic consumption remains a significant concern within the spine community. The prevalence of narcotic use in the treatment of acute and chronic pain leads to the potential for dependence and abuse.12–14 As such, minimizing preoperative and postoperative narcotic use following MIS LD is an important topic of investigation. Despite evidence demonstrating successful clinical outcomes following outpatient MIS LD, few studies have evaluated narcotic use in the immediate postoperative period. In this context, the aim of the current study is to evaluate early postoperative pain and narcotic consumption between MIS LD performed in a hospital versus ambulatory setting.
MATERIALS AND METHODS
Patient Population
Institutional review board approval was obtained for this study (ORA no. 14051301). A prospectively maintained surgical registry of patients was retrospectively reviewed. Patients were included in this analysis if they underwent a primary, single-level MIS LD for degenerative lumbar spine pathology between 2013 and 2017. Each MIS LD procedure included a foraminotomy, facetectomy, laminectomy, and discectomy. All procedures were performed by the senior author (K.S.) at a single institution. Patients were stratified by operative location: a hospital-based center (HBC) or an ambulatory surgery center (ASC). Only patients who were discharged on the day of surgery were included in the analysis. Pain management was standardized according to a multimodal analgesia protocol developed by a team of surgeons and anesthesiologists at our institution.
Data Collection
All data were obtained from the aforementioned surgical registry. Patients were classified according to demographic, comorbidity, and operative factors. Demographic factors included age, sex, smoking status, body mass index (<30 kg/m2, ≥30 kg/m2), and primary insurance payer. Comorbidity was analyzed with the Charlson Comorbidity Index. Perioperative factors, such as operative time, estimated intraoperative blood loss, and length of stay, were recorded. Inpatient visual analog scale pain scores, as assessed by the nursing staff according to normal protocols, were averaged over the duration of stay. Inpatient narcotic consumption was recorded in oral morphine equivalents (OMEs), using the conversion ratios described by Gordon et al15 Narcotic consumption was evaluated as a sum of the total OMEs consumed on postoperative day 0 and as an average over the duration of stay.
Perioperative complications were also recorded, including transient urinary retention, altered mental status, ileus, postoperative transfusion requirement, cardiac arrhythmia, acute renal failure, urinary tract infection, aspiration/reintubation, deep venous thrombosis, pulmonary embolism, pneumothorax, and pneumonia. Transient urinary retention was classified as a complication if postoperative recatheterization was required.
Statistical Analysis
Statistical analysis was performed using Stata/MP 13.1 for Mac (StataCorp LP, College Station, Texas). Differences between groups in patient demographics were assessed using independent-sample t tests for continuous variables and χ2 analysis for categoric variables. The operative location and its effect on perioperative characteristics, inpatient pain scores, and narcotics consumption were analyzed using multivariate linear regression adjusted for significant patient characteristics. A P value <.05 was used to determine statistical significance.
RESULTS
A total of 235 patients who underwent a primary 1-level MIS LD were included in the analysis. Of these, 90 (38.3%) underwent surgery at an HBC and 145 (61.7%) at an ASC. The average patient age was 41.4 years for the HBC cohort and 40.7 years for the ASC cohort (P = .632). Most of the patients in both cohorts were male (HBC, 67.7%; ASC, 75.9%; P = .126). A greater number of patients in the HBC cohort held private insurance compared with patients in the ASC cohort (76.7% vs. 37.2%, P = .026). Patients in the HBC cohort exhibited a higher Charlson Comorbidity Index compared with the ASC cohort (1.1 vs. 0.8, P = .041). The HBC patients also reported no difference in preoperative visual analog scale back pain scores compared with the ASC cohort (6.6 vs. 6.0, P = .144). Similarly, no difference was determined between the HBC and ASC cohorts when comparing preoperative visual analog scale leg pain scores (6.5 vs. 6.2, P = .938). No other significant differences in preoperative demographics existed between cohorts (Table 1).
Baseline characteristics.a
Table 2 details the perioperative outcomes between groups. Patients in the HBC cohort demonstrated shorter operative times (30.9 vs. 41.3 minutes, P < .001) and increased total estimated blood loss (34.4 vs. 26.3 mL, P < .001) compared with the ASC cohort. However, these differences were not clinically significant. The HBC cohort exhibited longer lengths of stay (5.8 vs. 2.6 hours, P < .001) than the ASC cohort. When examining pain scores, there were no differences observed between cohorts (HBC, 3.7 versus ASC, 3.9; P = .714). Two patients who underwent MIS LD at an HBC experienced transient urinary retention that required recatheterization. P values were calculated using multilinear regression controlling for insurance status and Charlson Comorbidity Index. No other complications were identified in either group.
Perioperative outcomes.a
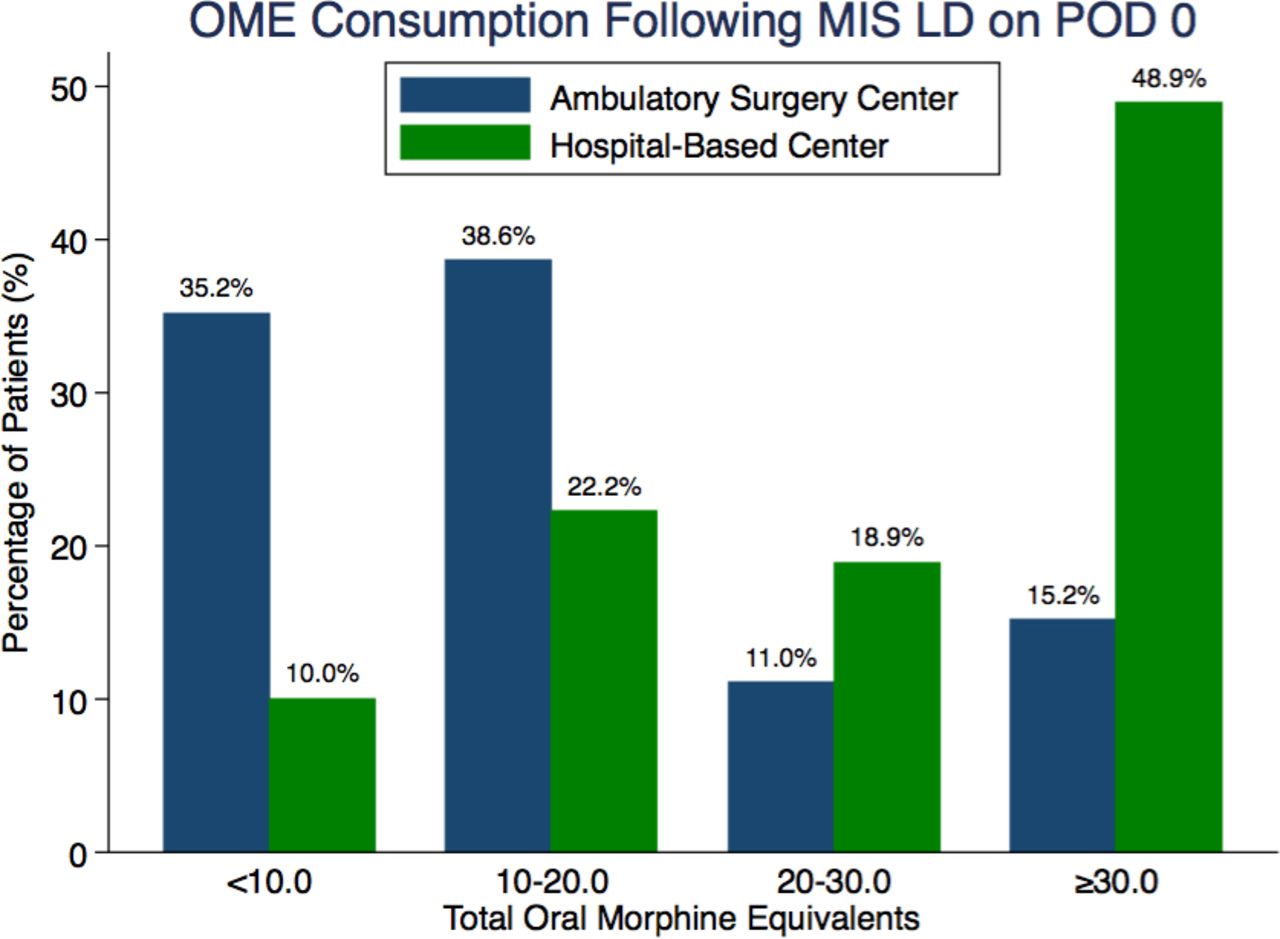
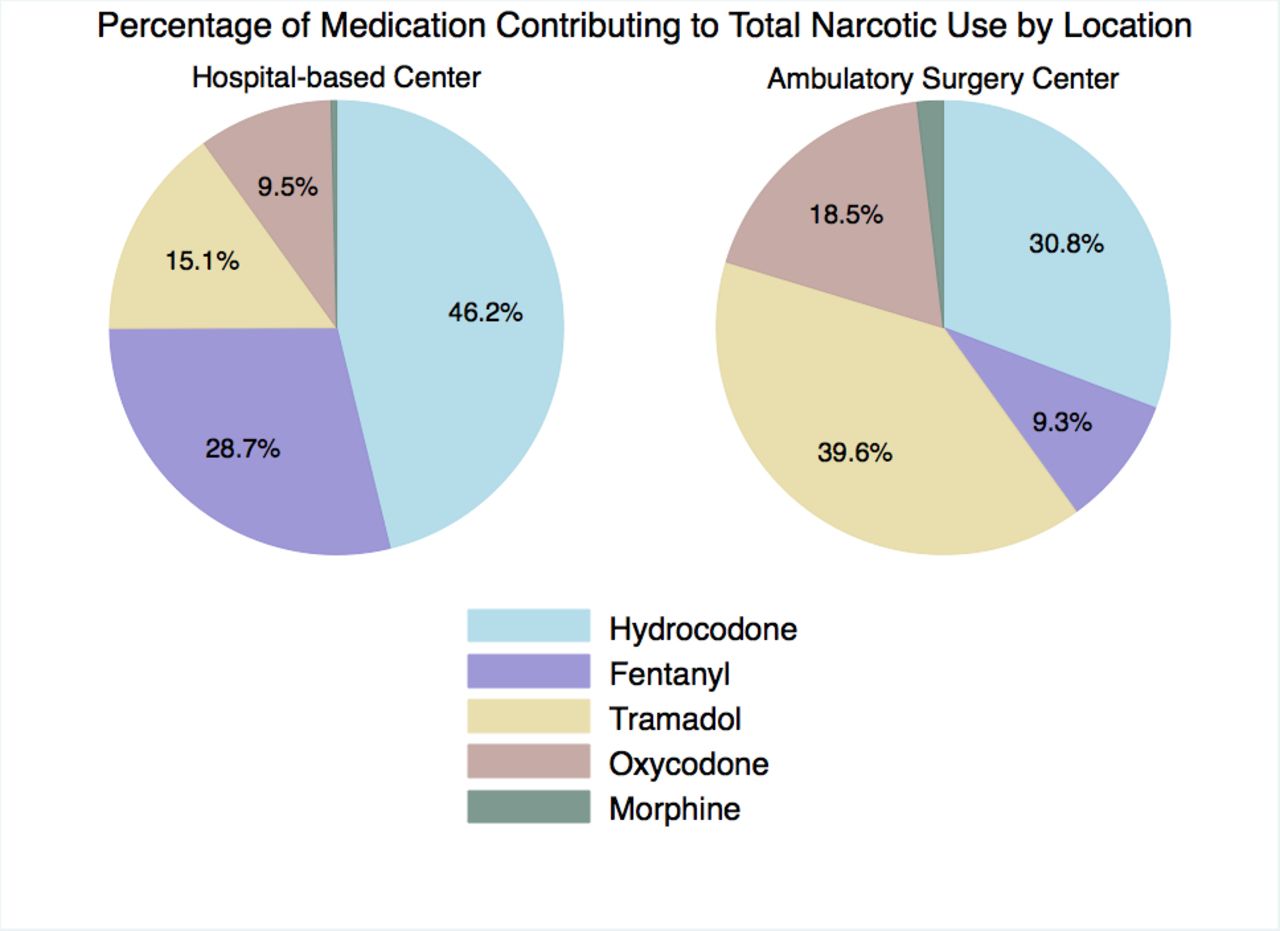
Table 3 describes the OME consumption on postoperative day 0 between cohorts. Patients in the HBC cohort consumed greater total OMEs (35.7 vs. 15.0, P < .001) compared with the ASC cohort (Figure 1). The HBC cohort consumed greater amounts of hydrocodone (13.8 vs. 4.2 OMEs, P < .001) and fentanyl (16.7 vs. 2.3 OMEs, P < .001). The ASC cohort consumed greater amounts of tramadol (5.0 vs. 3.3 OMEs, P = .028) and oxycodone (3.8 vs. 1.7, P = .053); however, this did not reach statistical significance. P values were calculated using multilinear regression controlling for insurance status and Charlson Comorbidity Index. Figure 2 illustrates the percentage of medications contributing to total OME administered in each setting. Hydrocodone and fentanyl were the most used narcotics in the HBC (46.2% and 28.7%). In contrast, tramadol was the most commonly administered narcotic in the ASC (39.6%), followed by hydrocodone (30.8%).
Oral morphine equivalent consumption on postoperative day 0.a

Bar graph illustrating the total oral morphine equivalent consumption between cohorts. Abbreviations: OME, oral morphine equivalents; MIS LD, minimally invasive lumbar decompression; POD, postoperative day.

Pie chart illustrating the percentage of medication contributing to total narcotic administration in each setting.
DISCUSSION
With the current trend toward outpatient spinal procedures, recent literature has emphasized the setting's safety and efficacy compared with hospital-based procedures.1–8,11,14,16 However, there has been limited research comparing narcotic administration between these two settings, specifically in the immediate postoperative period. Narcotic consumption is associated with a significant side effect profile, including drowsiness, nausea, vomiting, constipation, difficulty with deep breathing, coughing, impaired bowel and bladder function, and transient impairment of psychomotor skills.17–19 The potential hazards of narcotic toxicity have resulted in an effort to reduce the amount of postoperative narcotic consumption. In this context, the goal of the current study was to measure narcotic consumption among patients who underwent MIS LD in an ASC versus HBC.
The results of the present study suggest patients who underwent MIS LD at an ASC consumed significantly less total narcotics compared with patients who underwent MIS LD at an HBC. Additionally, patients in both cohorts reported similar pain levels prior to discharge despite patients in the ASC cohort receiving less total narcotic medication. When comparing total OME consumption, more than two thirds (73.8%) of the ASC cohort consumed less than or equal to 20 mg OME. In contrast, only one third (32.2%) of the HBC cohort consumed less than 20 mg OME. Relative to total OME consumption, the HBC administered a greater percentage of hydrocodone and fentanyl, whereas the ASC administered a larger percentage of the less-potent narcotic, tramadol. The ASC patients received a reduced quantity of high-potency narcotics, instead receiving an increased quantity of a lower-potency narcotic, which may have contributed to their decreased length of stay. The reduced narcotic administration in the ASC may be reflective of a greater motivation to discharge patients in this setting in a timely manner. Models of care designed used in same-day surgery populations have sought to reduce narcotic administration as a means to promote cost-efficiency and to expedite discharge.20–23
Excess narcotic administration in the early postoperative period has been associated with a significant side effect profile and can contribute to delayed discharge.17–19,24,25 In a retrospective analysis of a heterogenous orthopedic population, Hansen et al26 investigated the effect of narcotic consumption on length of stay between patients receiving a combination of intravenous (IV) acetaminophen and IV narcotics to patients receiving IV narcotics alone. The authors demonstrated patients receiving a combination of narcotic and nonnarcotic medication recorded shortened lengths of stay compared with patients receiving narcotic medication alone. In a prospective randomized study, Padda et al27 investigated the recovery profile of ophthalmologic surgical patients comparing the use of rectal acetaminophen or intravenous fentanyl-droperidol. Study results illustrated that patients receiving fentanyl experienced longer time in the postsurgical unit compared with the acetaminophen-treated group. The authors concluded the administration of fentanyl provided no discrete benefit over acetaminophen.
Although patients at the ASC received less narcotics than the HBC patients, there were no differences in pain scores observed between cohorts. These results suggest patients undergoing MIS LD can receive a reduced quantity of narcotics in the immediate postoperative period without conceding adequate pain control. Previous studies investigating the efficacy of narcotic alternatives, such as tramadol, for treatment of postoperative pain have demonstrated that the centrally acting analgesic provides less sedation, less euphoria, and less respiratory depression compared with frequently administered narcotic agents.28–30 In a randomized controlled trial by Ng et al,31 patient-controlled analgesia administration of tramadol and parenteral fentanyl were investigated to determine effect on pain relief following abdominal surgery. When comparing verbal pain scores, no differences were found between groups at rest in the first 24 hours (fentanyl group, 4.2; tramadol group, 3.6; P = .417). The authors demonstrated the use of a narcotic alternative, such as tramadol, can produce equivalent analgesia, without the use of the higher-potency narcotic, fentanyl. In the current study, no differences in pain scores were observed between cohorts despite the differences in fentanyl administration between groups. However, it is imperative to also consider that patients in the HBC setting could potentially have needed more narcotics in order to have equal pain relief relative to the patients in the ASC setting. As such, that patients in each setting achieved the same reported pain outcomes indicates hospital-based patients perhaps require more pain medication than those at an ASC. Further study is required in order to reassess postoperative narcotic medication administrative schedules in order to reduce high-potency narcotic medication and increased use of narcotics alternatives and lower-potency narcotics.
The current study is not without limitations. First, all procedures were performed by a single surgeon, limiting the generalizability to the greater population Second, because of the retrospective nature of the study, there may have been a selection bias between cohorts, because patients at greater preoperative risk for adverse events are more likely to be treated at an HBC than at an ASC for possible hospital admission. Third, a potential for a confounding variable may exist to explain shorter operative times and prolonged length of stay in the patients treated at the HBC. However, only 2 postoperative adverse events were recorded, and both occurred in the HBC cohort. Additionally, the risk of bias was minimized by use of statistical analyses that adjusted for the preoperative characteristics that varied between cohorts. Lastly, no measurement of preoperative narcotic use was available, resulting in the inability to quantify the effect of narcotic tolerance on postoperative pain scores and narcotics use.
CONCLUSIONS
To further advance the safety and efficacy of outpatient lumbar decompression procedures, the investigation of differences in narcotic consumption in the early postoperative period is necessary. The results of the current study suggest that patients who underwent MIS LD at an ASC receive fewer narcotics than patients treated at an HBC, which may contribute to shortened length of stay. Additionally, there was no difference in patient-reported pain between cohorts despite the differences in narcotic administration. As such, postoperative narcotics administration varied, indicating HBC patients required more narcotic pain medications to achieve the same pain scores that were sufficient to allow patient discharge, thus prolonging length of stay.
ACKNOWLEDGMENTS
Preliminary portions of this work have been presented at the Society for Minimally Invasive Spine Surgery in 2016 and 2017 and at The International Society for the Advancement of Spine Surgery in 2017.
Footnotes
Disclosures and COI: No funds were received in support of this work. No benefits in any form have been or will be received from any commercial party related directly or indirectly to the subject of this manuscript.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.