


ABSTRACT
Background: Surgical treatment for lumbar degenerative spondylolisthesis has been shown to provide better long-term outcomes than conservative treatment. However, there is variation in surgical approaches employed by surgeons. This study investigates current surgical practice patterns and compares perioperative outcomes of 3 common surgical treatments for this pathology.
Methods: A survey was administered to surgeons who attended the Lumbar Spine Research Society (LSRS) meeting in 2014. Data were extracted from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) from 2005 to 2014 to characterize the same responses. The 2 data sets were compared. Perioperative outcomes of those in the ACS-NSQIP posterior fusion subcohorts were characterized and compared.
Results: Posterior surgical approaches utilized by surgeons who responded to the LSRS survey were similar to those captured by ACS-NSQIP where 72% of those with degenerative spondylolisthesis were fused. Of those that were fused, 8% had an uninstrumented posterior fusion, 33% had an instrumented posterior fusion, and 59% had an instrumented posterior fusion with interbody. On multivariate analysis, there was no difference in risk of postoperative adverse events, readmission, or length of stay between these 3 common types of fusion.
Conclusions: Practice patterns for the posterior management of lumbar degenerative spondylolisthesis were similar between LSRS survey responses and ACS-NSQIP data. The ACS-NSQIP perioperative outcome measures assessed were similar regardless of surgical technique. These findings highlight that cost-benefit considerations and longer-term outcomes have to be the measures by which surgical technique is chosen for degenerative spondylolisthesis.
- lumbar degenerative spondylolisthesis
- Lumbar Spine Research Society
- survey
- posterior fusion
- complications
- perioperative outcomes
INTRODUCTION
Lumbar degenerative spondylolisthesis with resultant stenosis is a common condition typically seen at L4-L5, in females more commonly than males, and in individuals older than 50 years of age.1,2 The slippage is generally due to degenerative changes in the zygapophyseal joints between the 2 vertebrae with accompanying degeneration of the disc at that level.3,4 Although conservative treatments are generally tried, surgery is often appropriately considered in the management of this condition if symptoms warrant.1,4
The benefits of surgery were verified by the Spine Patient Outcomes Research Trial (SPORT), which compared the effectiveness of surgical and nonsurgical treatment among participants with confirmed diagnoses of lumbar degenerative spondylolisthesis. Patients who were treated surgically showed substantially greater improvement in pain and functional status at 2 and 4 years follow-up.5–7
Although decompression is the primary surgical intervention for stenosis, fusion is generally considered in the setting of spondylolisthesis. This approach dates back to the seminal papers of Herkowitz and Fishgrund.8,9 If performing fusion, instrumentation has been accepted as a way to increase fusion success.9,10 Interbody techniques have been suggested as ways to increase fusion success, potentially improve alignment, and/or allow for grafting with minimally invasive techniques.10
However, there is debate on which fusion technique is best. Arguments for uninstrumented fusion include similar long-term results with and without instrumentation, poor cost-effectiveness of instrumentation, and risk of implant-related issues.11,12 Arguments for instrumented fusion include increasing fusion success and decreasing the rate of pseudarthrosis, a condition that leads to inferior long-term outcomes.1,13 The long-term advantages for instrumented posterior fusion with interbody are also inconclusive, largely from a lack of cost-benefit evidence.4,14,15
The goals of the current study are first to gauge current surgical practice trends for lumbar degenerative spondylolisthesis in a group of spine surgeons who attend the Lumbar Spine Research Society (LSRS) annual meetings and compare them to national trends from data available via the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. The second goal is to compare short-term perioperative outcomes for patients who underwent common posterior-based approaches for this pathology: uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody. We hypothesized that there would be no clinically significant differences in perioperative outcomes between the 3 common surgical treatments.
MATERIALS AND METHODS
Data Sources
The LSRS was founded in 2008 and is affiliated with other spine societies such as AOSpine North America, Cervical Spine Research Society, and Scoliosis Research Society through membership in the Council of Surgical Spine Societies. The mission of the LSRS is to fill the need for a scientific gathering focused on the surgical treatment of the lumbar spine. The society accomplishes this by maintaining an academic annual meeting with no corporate funding, which offers an opportunity for research presentations followed by discussion amongst spine surgeons.16
The ACS-NSQIP database has been collecting chart-abstracted data from over 500 participating institutions in the United States since 2005.17 The database employs trained clinical reviewers to abstract over 150 specifically defined variables including preoperative comorbidities, intraoperative variables, and postoperative adverse outcomes through the 30th postoperative day regardless of hospital discharge.18 This data set has proved to be a valid data source in orthopedic surgery literature.19 The current study was found to be exempted from review by the Human Investigation Committee at our institution. The level of evidence in this study is Level III.
Comparison of LSRS Survey and ACS-NSQIP Practice Patterns
A survey was designed and circulated to spine surgeons who attended the LSRS annual meeting held in April 2014. A part of the survey, from which data were drawn for the current study, is included in the appendix. Data were then analyzed to determine common practices used for treatment of patients with degenerative spondylolisthesis (primary, nonrevision, single level).
The same cohort of patients referred to in the survey handed out at LSRS was selected from the ACS-NSQIP database (2005–2014) using the International Classification of Disease 9th Revision (ICD-9) code for spondylolisthesis (738.4). Single-level cases and posterior approaches were isolated by current procedural terminology (CPT) codes. Multiple-level cases, anterior, and lateral approaches were excluded. If the surgeons who attended the LSRS meeting are practicing in a hospital that feeds data to the NSQIP database, then their practice patterns may also be recorded in the NSQIP database. We did not attempt to determine whether or not the 2 data sources were overlapping or mutually exclusive since we believe the large difference in number of data points between the 2 sources would wash out any biases from any small overlaps.
This ACS-NSQIP cohort of patients was further separated using CPT codes into subsets that underwent decompression, posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody. Instrumented posterior fusion with interbody was treated as a subset of instrumented posterior fusion. Instrumented posterior fusion was in turn treated as a subset of posterior fusion.
Cases in which local autograft was solely used, iliac crest autograft was harvested, or bone marrow was aspirated, were also made into distinct groups. The ACS-NSQIP extracted data were then analyzed and compared to the survey data to determine if the national common practices used to treat patients with spondylolisthesis matched common practices utilized by LSRS surgeons.
Analysis of Perioperative Outcomes of the ACS-NSQIP Population
Further analysis was performed on 3 distinct groups of patients identified above: patients who underwent uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody. In this analysis, the 3 techniques are treated not as subsets of each other but as distinct groups. Patients who received only fusions and no decompression or who had a diagnosis other than degenerative spondylolisthesis were excluded. Anterior or lateral approaches were not included in the analysis, as that was not the population evaluated by the initial LSRS questionnaire and not the focus of this study.
Age, gender functional status prior to injury, and other comorbidities are directly reported in the ACS-NSQIP database. For each case, a modified version of the Charlson Comorbidity Index (CCI)20 that has been adapted to the ACS-NSQIP database was calculated.21 Several studies have shown that modified CCIs predict similar prognoses as the original CCI.22,23 Modified CCIs has also been previously used with ACS-NSQIP Data.24,25
The ACS-NSQIP database tracks patients for individual adverse events during the first 30 postoperative days.17 These events were used to generate 3 categories of adverse event outcomes as previously defined.26 The occurrence of a minor adverse event (MAE) was defined as the occurrence of any of the following: urinary tract infection, pneumonia, blood transfusion, readmission to hospital, wound dehiscence, deep vein thrombosis, superficial surgical site infection, deep surgical site infection, organ/space surgical site infection, sepsis without shock, return to the operating room, progressive renal insufficiency, unplanned intubation, and failure to wean from ventilation. The occurrence of a serious adverse event (SAE) was defined as the occurrence of any of the following: death, pulmonary embolism, acute renal failure, myocardial infarction, septic shock, stroke, and cardiac arrest requiring CPR. As there is some subjectiveness to the characterization of MAEs versus SAEs, the occurrence of any adverse event (AAE) was also evaluated (defined as the occurrence of any of the MAEs or SAEs listed above).
Operative time (time from incision to closure), postoperative length of stay (LOS), and readmission were also directly reported in the ACS-NSQIP database. LOS is one of the few postoperative variables in the database that is reported beyond 30 days. In order to limit the influence of outliers on data analysis, any postoperative LOS that is longer than 30 days was coded as a LOS equal to 30 days instead. Occurrence of readmission within 30 days is reported in the ACS-NSQIP database for cases that occurred in 2011–2014 but not for earlier cases.
Statistical Methods
Statistical analyses were conducted using Stata version 13.0 (StataCorp, LP, College Station, Texas). Pearson's χ2 tests were used to compare patients who underwent uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody by age, gender, functional status prior to injury, and modified CCI. Unpaired T-tests with unequal variances were used to compare these 3 techniques by operative time and LOS. Pearson's χ2 tests and T-tests were conducted using a level of significance of α = 0.05.
Poisson regressions with robust error variance were used to calculate the relative risks of MAEs, SAEs, AAEs, and readmission.27 A Bonferroni correction (n = 4) was used, and a level of significance was set at α = 0.0125.28
RESULTS
Comparison of LSRS Survey and ACS-NSQIP Practice Patterns
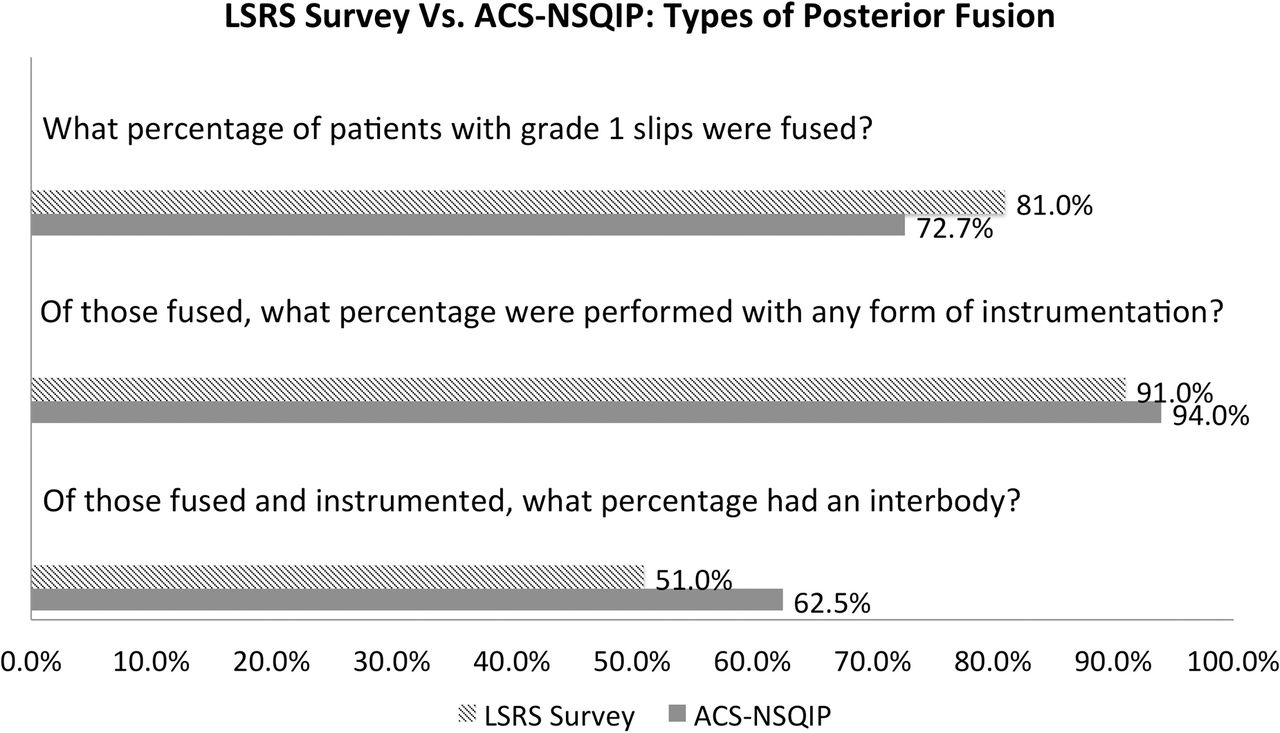
For the LSRS questionnaire, there was a response rate of 37 out of 61 (60.7%). The responses were then analyzed and the following results reported. In the first part of the questionnaire, surgeons reported that they fused 81% of patients with a grade 1 spondylolisthesis. Of these, 91% of these posterior fusions were performed with instrumentation, and 51% of these instrumented posterior fusions included an interbody (Figure 1).
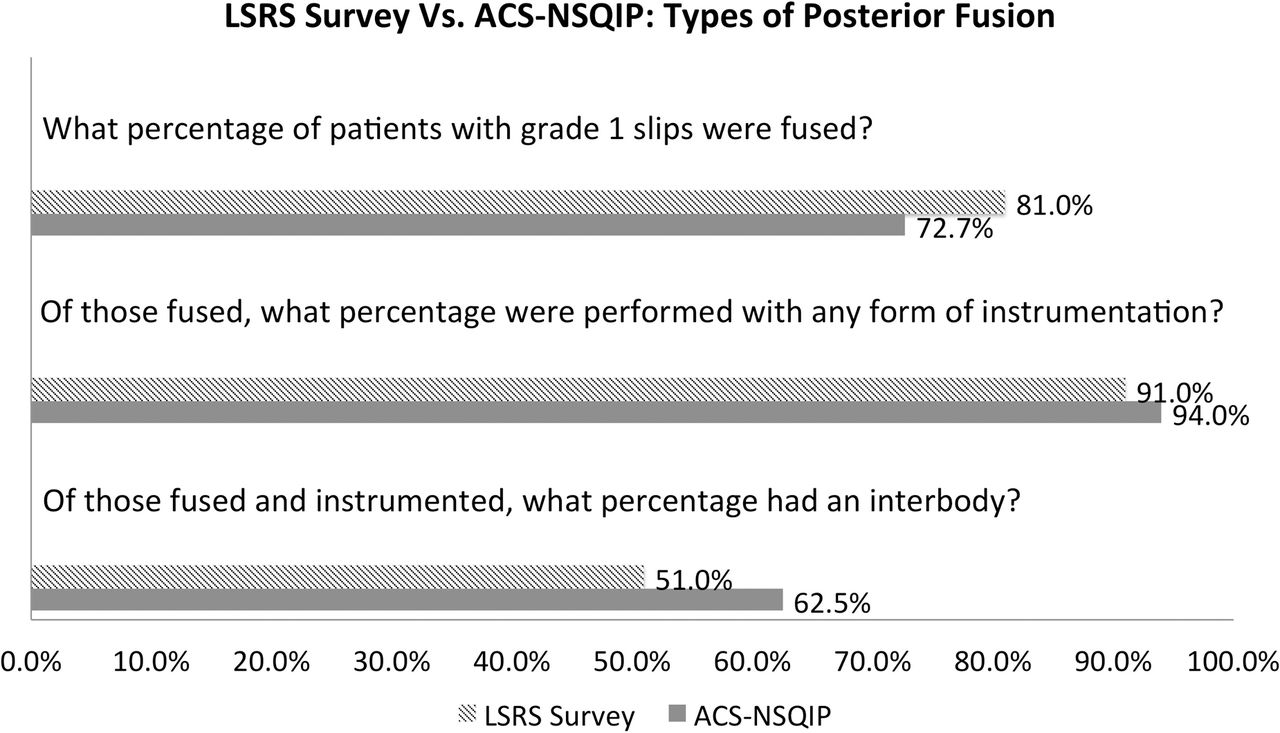
Types of posterior fusion used to treat lumbar degenerative spondylolisthesis. Abbreviations: LSRS, Lumbar Spine Research Society; ACS-NSQIP, American College of Surgeons National Surgical Quality Improvement Program.
For the matching ACS-NSQIP data, it was identified that posterior fusion was performed for 72.7% of patients with a grade 1 spondylolisthesis. Of these, 94% of these posterior fusions were performed with instrumentation, and 62.5% of these instrumented posterior fusions included an interbody (Figure 1).
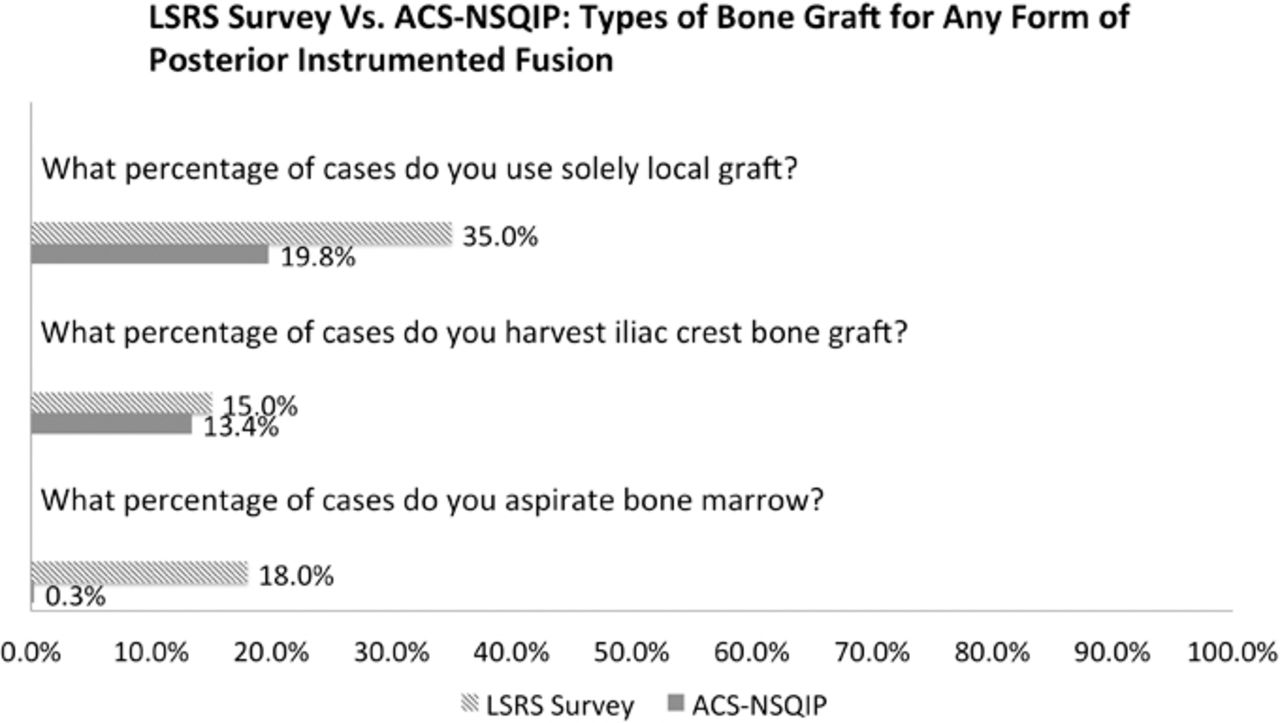
For the second part of the LSRS questionnaire, questions focused on those who had undergone a primary L4-5 laminectomy and instrumented posterior fusion. Solely local autograft was used in 35% of these cases, iliac crest bone graft was harvested in 15% of these cases, and bone marrow was aspirated in 18% of these cases (Figure 2).

Types of bone graft used for instrumented posterior fusion. Abbreviations: LSRS, Lumbar Spine Research Society; ACS-NSQIP, American College of Surgeons National Surgical Quality Improvement Program.
For the matching ACS-NSQIP data, it was identified that solely local autograft was used in 19.8% of these cases, iliac crest bone graft was harvested in 13.4% of these cases, and bone marrow was aspirated in 0.3% of these cases (Figure 2).
Analysis of Perioperative Outcomes of the ACS-NSQIP Population
Patient Characteristics
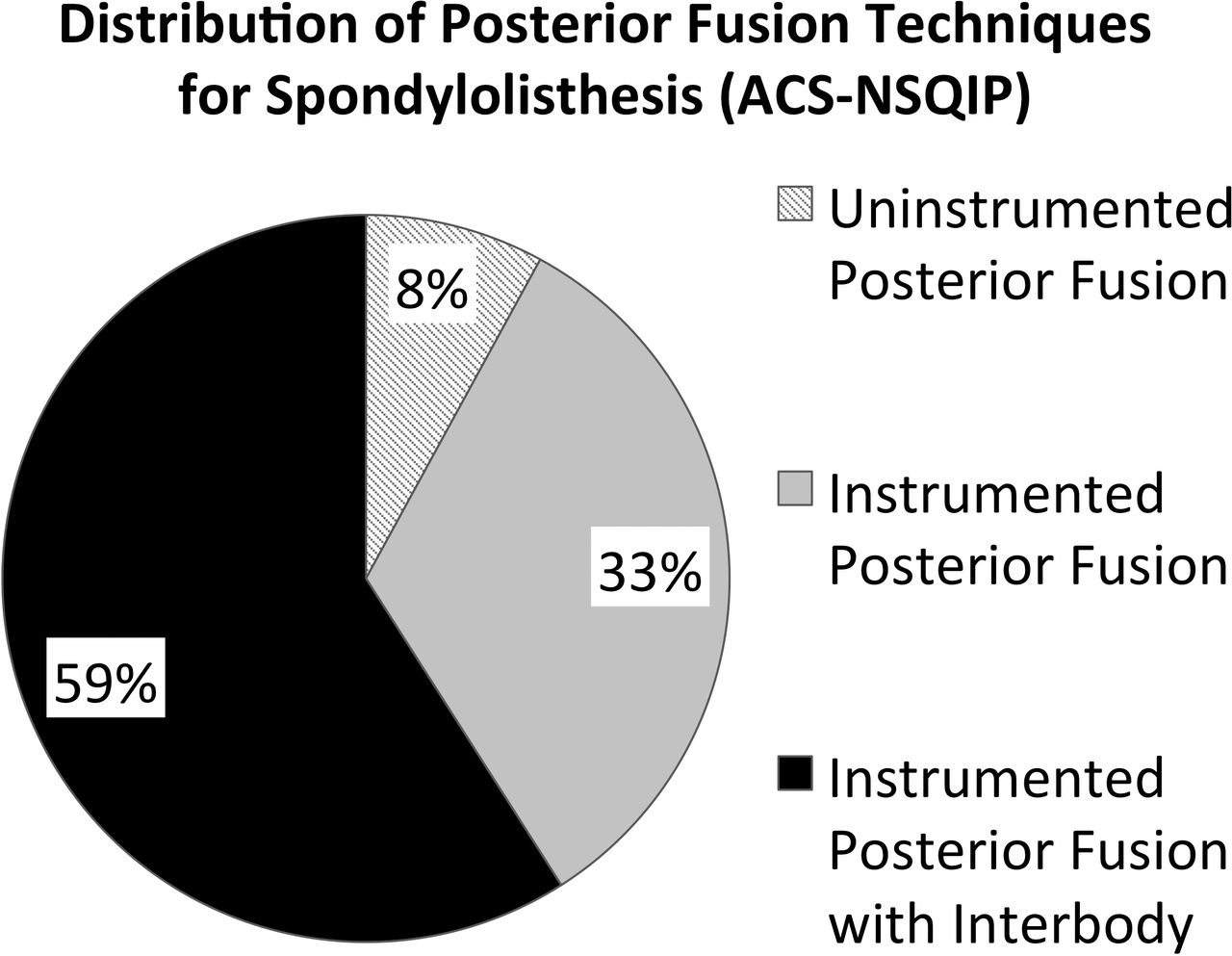
For perioperative outcomes analysis, a total of 1884 cases met the inclusion criteria. Of these, 150 (7.96%) were uninstrumented posterior fusion cases, 622 (33.01%) were instrumented posterior fusion cases, and 1112 (59.02%) were instrumented posterior fusion with interbody cases (Figure 3; Table 1).
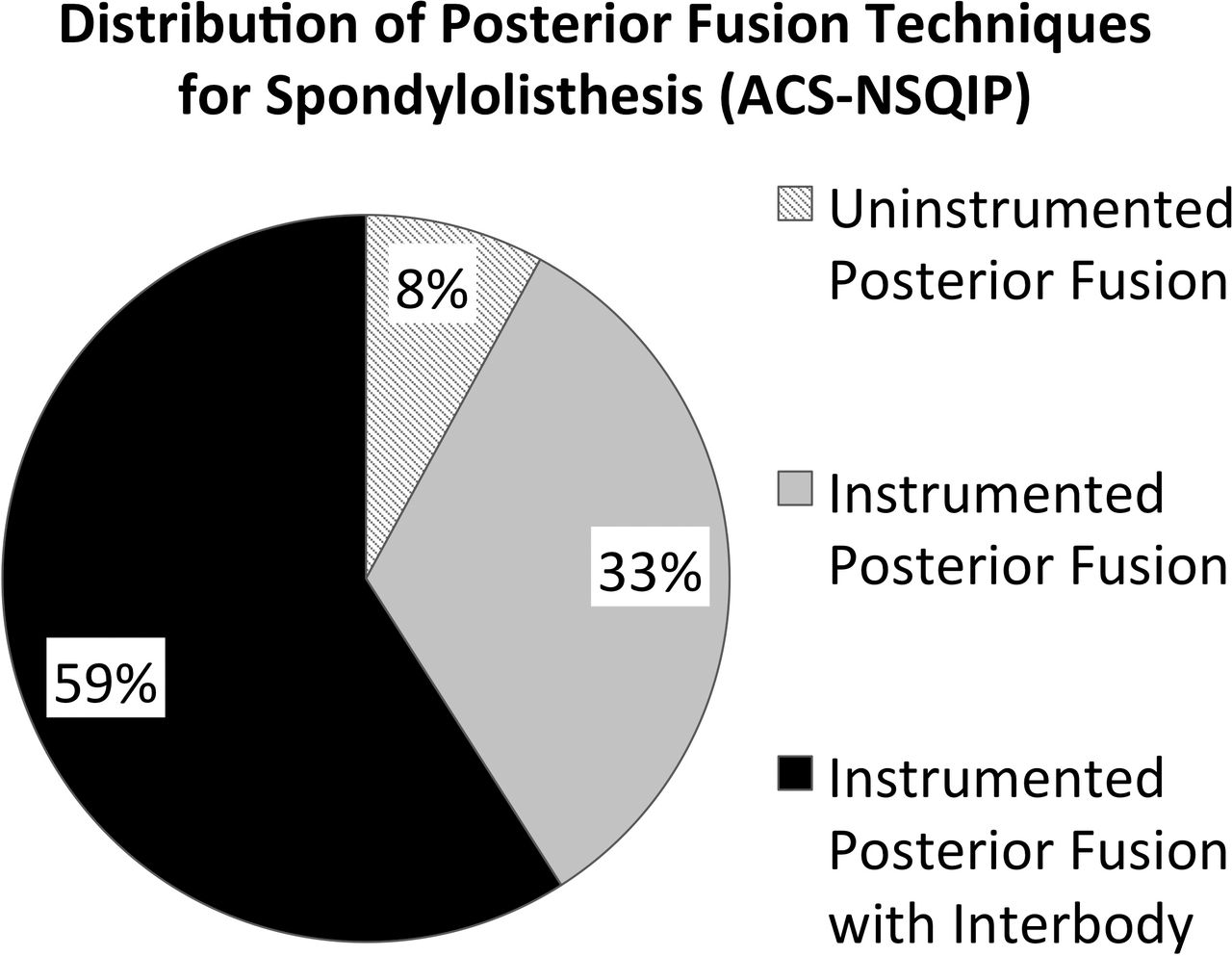
Distribution of posterior fusion techniques used to treat lumbar degenerative spondylolisthesis in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) population.
Demographic and comorbid characteristics of patients who underwent uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody.
Patients treated with these 3 techniques did not differ in their distribution of gender or functional status prior to injury (Table 1; P ≥ .05 for each). However, these 3 techniques were statistically different in their distribution of age and modified CCI (Table 1; P < .001 for each). Therefore, further analyses were adjusted for modified CCI to ensure that demographics and comorbidities did not confound the results. Age was not adjusted separately because age is already part of the calculation for modified CCI. The average work relative value units for uninstrumented posterior fusion is 21.22, for instrumented posterior fusion is 20.40, and for instrumented posterior fusion with interbody is 22.18.
Perioperative Outcomes
When controlling for modified CCI, the rate of MAE, SAE, and AAE were not statistically different between patients who underwent uninstrumented posterior fusion and instrumented posterior fusion or between those who underwent instrumented posterior fusion and instrumented posterior fusion with interbody (Tables 3 and 4; P ranged from .384 to .922).
Mean operative times for patients who underwent uninstrumented posterior fusion and instrumented posterior fusion was statistically different (Table 3; P = .005). The average difference was 22 minutes. Mean operative times for patients who underwent instrumented posterior fusion with interbody and instrumented posterior fusion was also statistically different (Table 4; P < .001), but again this difference was relatively small with the average difference being only 19 minutes.
LOS was not statistically different for the 3 techniques analyzed. The mean LOS for uninstrumented posterior fusion is 3.2 days, while the LOS for instrumented posterior fusion and instrumented posterior fusion with interbody was 3.4 days for both (Table 2).
Number of adverse events, operative time, and length of stay for patients who underwent different posterior fusion techniques.
Uninstrumented posterior fusion relative to instrumented posterior fusion.
Instrumented posterior fusion with interbody relative to instrumented posterior fusion.
The rate of readmission within 30 days of surgery was also not statistically different for the 3 techniques analyzed. The rate of readmission for uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody was 4.32%, 4.87%, and 4.85%, respectively (Table 2).
DISCUSSION
The purpose of the present study was to first obtain an understanding of the posterior surgical treatment approaches to grade 1 spondylolisthesis that spine surgeons utilize and then to evaluate the similarity of those methods with those captured by ACS-NSQIP. Secondarily, this study aimed to evaluate the short-term, general health outcomes following different posterior fusion options: uninstrumented posterior fusion, instrumented posterior fusion, and instrumented posterior fusion with interbody using the ACS-NSQIP sample.
The LSRS survey component of this study was used to gain a yardstick of treatments being utilized for posterior treatments of degenerative spondylolisthesis. The response rate of greater than 60% was favorable in comparison with other physician survey studies.29,30 The most surprising finding from our perspective was the high rate of interbody fusions (51.0%) for posterior instrumented cases.
Given the high rate of reported interbody fusions for instrumented posterior surgeries for degenerative spondylolisthesis, we proceeded to evaluate this trend in the ACS-NSQIP database. This revealed remarkably similar trends. The ACS-NSQIP study found that 72.7% cases of posterior surgery for degenerative spondylolisthesis were fused, of those 94% were instrumented, and of those 62.5% had interbody fusion performed.
Overall, it is clear from the data sets analyzed that most posterior surgeries for degenerative spondylolisthesis do employ instrumented posterior fusion. This is well supported by recent studies such as SPORT.5–7 Further, the majority of those use interbody devices. These findings support past studies that have reported increasing usage of interbody fusion.2 This is of particular interest, as there is no robust data to support clinical superiority of adding interbody devices to instrumented posterior fusion.10,15,31,32 It might be that this is being driven by the rise in popularity of minimally invasive surgery (MIS) that requires the interbody space for a surface area for fusion. Unfortunately, we cannot determine the percent of cases that were done with MIS techniques using the data sets employed here.
In terms of bone grafts utilized for these surgeries, the utilization of iliac crest autograft was reported similarly for LSRS survey as identified in ACS-NSQIP (15% and 13.4%, respectively). On the other hand, greater differences were seen for local autograft only (35% vs 19.8%, respectively) and bone marrow aspirate (18% and 0.3%, respectively). It is hypothesized that this is due to coding limitation for these low reimbursement codes in ACS-NSQIP, but this cannot be confirmed.
The low rate of utilization of iliac crest autograft is of interest. Although this has long been considered the “gold standard” grafting material, it is clear that trends have shifted away from its use and it is only used in the minority of cases. This is presumably related to the concerns over related morbidity.33
The variations in posterior surgical techniques used for lumbar degenerative spondylolisthesis lead us to want to compare the perioperative outcomes of treatment options. Clearly if differences in morbidity and postoperative course were noted, this might argue for or against certain surgical options. Perioperative adverse events were analyzed in ACS-NSQIP for this population and, when controlling for CCI, no significant differences were identified for the occurrence of adverse events within 30 days of the procedure, hospital LOS, or readmission for the posterior techniques used to address lumbar degenerative spondylolisthesis studied here. These results validated our hypothesis and correlated with previous studies that reported similar short-term complications between uninstrumented fusion, instrumented fusion, and instrumented fusion with interbody in a different patient sample.2
This observation makes it clear that perioperative adverse events are not the driver by which one can differentiate the surgical procedures evaluated for addressing lumbar degenerative spondylolisthesis. The driver should therefore be long-term outcomes, patient choice, or surgeon preference. While our data cannot conclusively determine if revenues or commercialization/marketing from instrumentation companies affect surgical decision-making regarding which fusion technique to utilize, we did demonstrate somewhat similar work relative value units for the 3 fusion techniques in our patient cohort. It is the authors' opinion that surgeons should always have patients' best interests in mind when making any treatment decisions.
It is of note there were statistically significant differences in operative time. Compared to uninstrumented posterior fusion, instrumented posterior fusion took an average of 22 minutes of additional time (P = .005). Compared to instrumented posterior fusion, instrumented posterior fusion with interbody took an average of 19 minutes of additional time (P < .001). Although operative time has been associated with an increased risk of adverse events in other studies,34,35 the differences were not associated with different perioperative morbidity in the current study. Thus, the clinical significance of these relatively small differences is thought not to be great in this setting.
This paper has clear strengths. The most current observed practice trends to date were confirmed from 2 sources (LSRS survey and ACS-NSQIP). Further, the large and validated ACS-NSQIP population was able to evaluate the perioperative outcomes of posterior surgical techniques used to address lumbar degenerative spondylolisthesis.
There are limitations to the current study. As with any survey study, the LSRS study is prone to surgeon recall bias. That said, that is why the current study was supplemented with ACS-NSQIP data. With regard to the evaluation of perioperative morbidity, the ACS-NSQIP population does not contain spine specific outcome variables that might be of clinical significance such as characterizations of surgical pathology and neurologic injury. Further, the ACS-NSQIP database does not record spine structural variables such as facet orientation, dynamic instability, and coronal or sagittal deformity. Thus, these potentially important variables and certain subsets of patients could not be analyzed. The methodology of the current study also inherently poses limitations on studying subsets of patients with degenerative spondylolisthesis. National population data and recall questionnaires often aggregate patients and only allow ballpark responses. Thus, treatment\utilization trends may be different among subsets of patients with degenerative spondylolisthesis, but the methodology of the current study is not suited to detect these differences. In addition, this study only evaluated posterior fusion approaches (anterior and lateral approaches may be considered for lumbar degenerative spondylolisthesis, but these were not evaluated in the current paper). Lastly, the ACS-NSQIP database only records data through the 30th postoperative day, so longer-term outcomes could not be evaluated in the current study.
In summary, there are significant variations in the surgical management of lumbar degenerative spondylolisthesis. Of the posterior approaches used to address this pathology, the data presented here demonstrate that most cases used to address this pathology include posterior instrumentation and the majority is with interbody fusion. The lack of differences in general health adverse events, hospital LOS, and readmission rates between these techniques suggest that the decision for the appropriate intervention should focus on other metrics such as surgeon preference, patient experience, cost-benefit considerations, and longer-term outcome variables. In the future, large national databases should perhaps consider recording these variables so meaningful analyses could be undertaken.
ACKNOWLEDGMENTS
The authors have no ownerships, patents, or participations with entities whose products or category of products are mentioned in the current manuscript.
Our institutional review board granted an exemption for studies using this data set because all data are deidentified and anonymous.
APPENDIX
Lumbar Spine Research Society Questionnaire
Lumbar Fusion and Bone Grafting: Practices and Beliefs*
Introduction: Lumbar degenerative spondylolisthesis is the most common diagnosis leading to spinal fusion surgery in the United States. Over the past several years, marked changes in practice patterns have occurred in terms of surgical technique and use of bone graft alternatives. The purpose of this survey is to determine prevalent practice patterns and beliefs among a select group of leading lumbar spine specialists regarding fusion surgery and graft materials in this patient population.
The following questions refer to your treatment of patients with degenerative spondylolisthesis and stenosis who are considered appropriate candidates for surgery (primary, nonrevision, single level):
1. Over the past year, what percentage of patients with a grade 1 slip did you fuse?
1a. What percentage of these fusions were performed with instrumentation?
1b. What percentage of these were performed with an interbody fusion?
The following questions refer to your “average” patient with a grade 1 slip undergoing a primary L4-5 laminectomy and posterior instrumented fusion:
1. In what percentage of instrumented cases do you use solely local graft without any additional material or extenders?
2. In what percentage of cases do you harvest iliac crest bone graft?
3. In what percentage of cases do you aspirate bone marrow?
*The presented form is a subset of the full questionnaire focusing on the questions used for the current study.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.