


ABSTRACT
Background: Nonspecific low back pain (NSLBP) is a term used to describe low back pain of unknown origin with no identifiable generators. Over a decade ago, it was reported to account for about 85% of all cases of low back pain, although there is some doubt about the frequency. The purpose of this study was to determine the frequency of NSLBP in adolescent athletes diagnosed by general orthopedic surgeons and by spine surgeons.
Materials and Methods: A total of 69 adolescent athletes consulted our sports spine clinic to seek a second opinion for low back pain. Data on age, sex, type of sport played, the previous diagnosis made by general orthopedic surgeons, and the final diagnosis made by spine surgeons were collected retrospectively from medical records.
Results: The frequency of NSLBP diagnosed by general orthopedic surgeons was 18.9% and decreased to 1.4% after careful imaging and functional nerve block examination by spine surgeons. The final diagnoses made by spine surgeons for those patients previously diagnosed as having NSLBP by general orthopedic surgeons were as follows: early-stage lumbar spondylolysis, discogenic low back pain, facet joint arthritis, lumbar disc herniation, and lumbar apophyseal ring fracture.
Conclusions: In adolescent athletes, the rate of NSLBP diagnosed by general orthopedic surgeons decreased markedly when the diagnosis was made by spine surgeons. A thorough medical interview, careful physical examination, appropriate diagnostic imaging, and selective nerve block examination can effectively identify the cause of low back pain.
INTRODUCTION
Low back pain (LBP) is not uncommon in children and adolescents. Burton et al1 reported that the incidence of LBP increased with age and that 50.4% of adolescents had experienced LBP by the age of 15 years. These patients are often overlooked, so it is important for spinal specialists to be familiar with the conditions underlying spinal pain in this age group.
Nonspecific low back pain (NSLBP) is a term used to describe LBP of unknown cause and accounts for about 85% of all cases of low back pain.2,3 In many of the past studies, however, the first authors were generally family physicians rather than orthopedic surgeons, and no mention was made of the final orthopedic diagnoses. Furthermore, these reports were published more than 15 years ago, and there have subsequently been remarkable advances in the development of imaging systems, including magnetic resonance imaging (MRI) and computed tomography (CT). It is now becoming possible to identify the cause of LBP using various types of functional nerve block examinations, such as facet joint block, discography, and selective nerve root block. We hypothesized that these newer high-quality imaging and functional block techniques should be able to identify most pain generators in adolescents, given that there is little degeneration of the lumbar structures in this age group. To test this hypothesis, we compared initial diagnoses made by general orthopedic surgeons and final diagnoses made by spine surgeons in adolescent athletes with LBP.
The purpose of this study was to identify the frequency with which initial and final diagnoses of NSLBP in adolescents were made by general orthopedic surgeons and spine surgeons, respectively. Our data suggest that low back pathology is more likely to be diagnosed as NSLBP by general orthopedic surgeons.
MATERIALS AND METHODS
Subjects were 69 adolescent athletes (54 boys, 15 girls; aged <20 years). All of them had first consulted with nearby general orthopedic doctors and next consulted our sports spine clinic, seeking a second opinion for low back pain between January 2013 and November 2015. Age, sex, type of sport played, the previous diagnosis made by general orthopedic surgeons, and the diagnosis subsequently made by spine surgeons were reviewed.
All general orthopedic surgeons and spine surgeons had diagnosed them by physical examination and some imaging systems, x-ray, CT scan, and/or MRI as the occasion may demand. Spine surgeons routinely performed T1- and T2-weighted MRI and short tau inversion recovery (STIR) imaging. The STIR-MRI is particularly useful for detecting bone marrow edema. Using a multi-detector CT scanner, reconstructed sagittal, axial, and coronal images were acquired. Using this device, it is possible to acquire oblique axial slices at different angles for detection of the early phase of a pars fracture. When images did not show obvious evidence of pathology, we performed a facet joint block, discography, or selective nerve root block examination.
RESULTS
The mean age of the subjects was 15.2 ± 2.3 years (range, 9–19 years). Figure 1 shows the types of sports that the patients have played, the most common of which were baseball and soccer. The average of the time from the initial general orthopedic diagnosis to consulting with spine surgeons was 3.4 months.

Types of sports played by adolescents with low back pain.
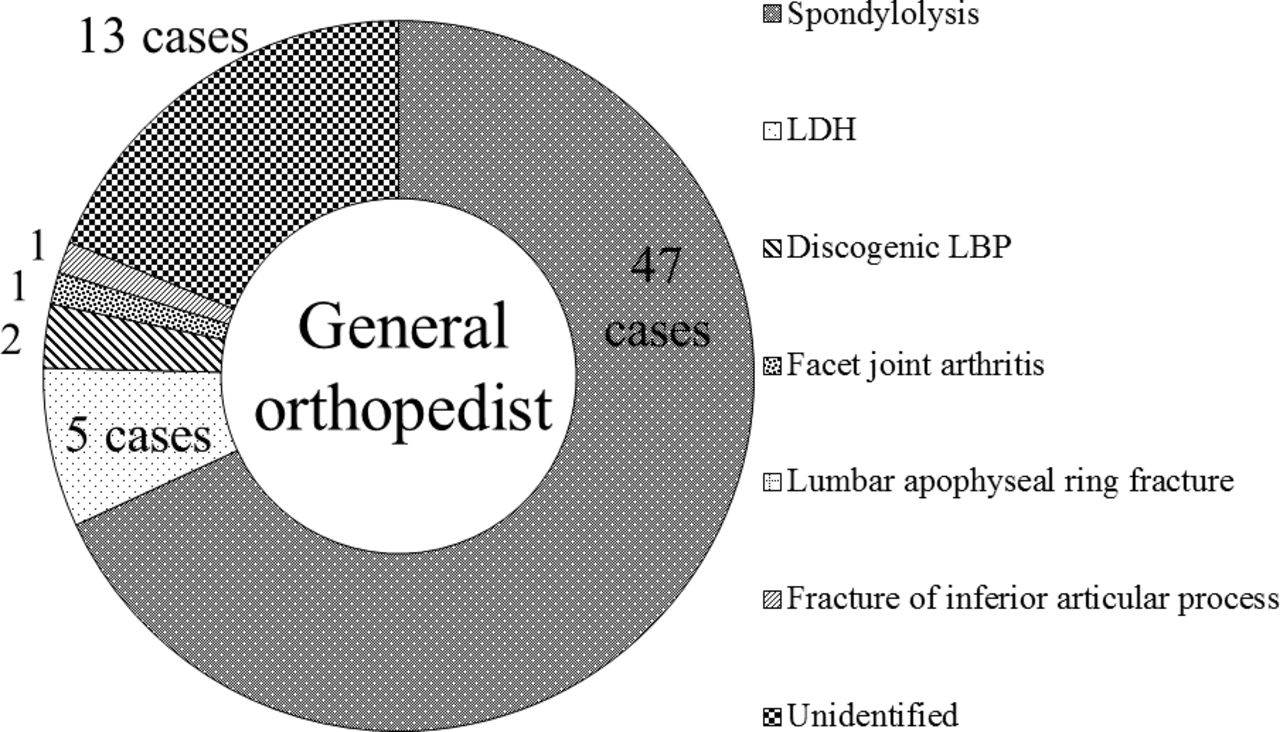
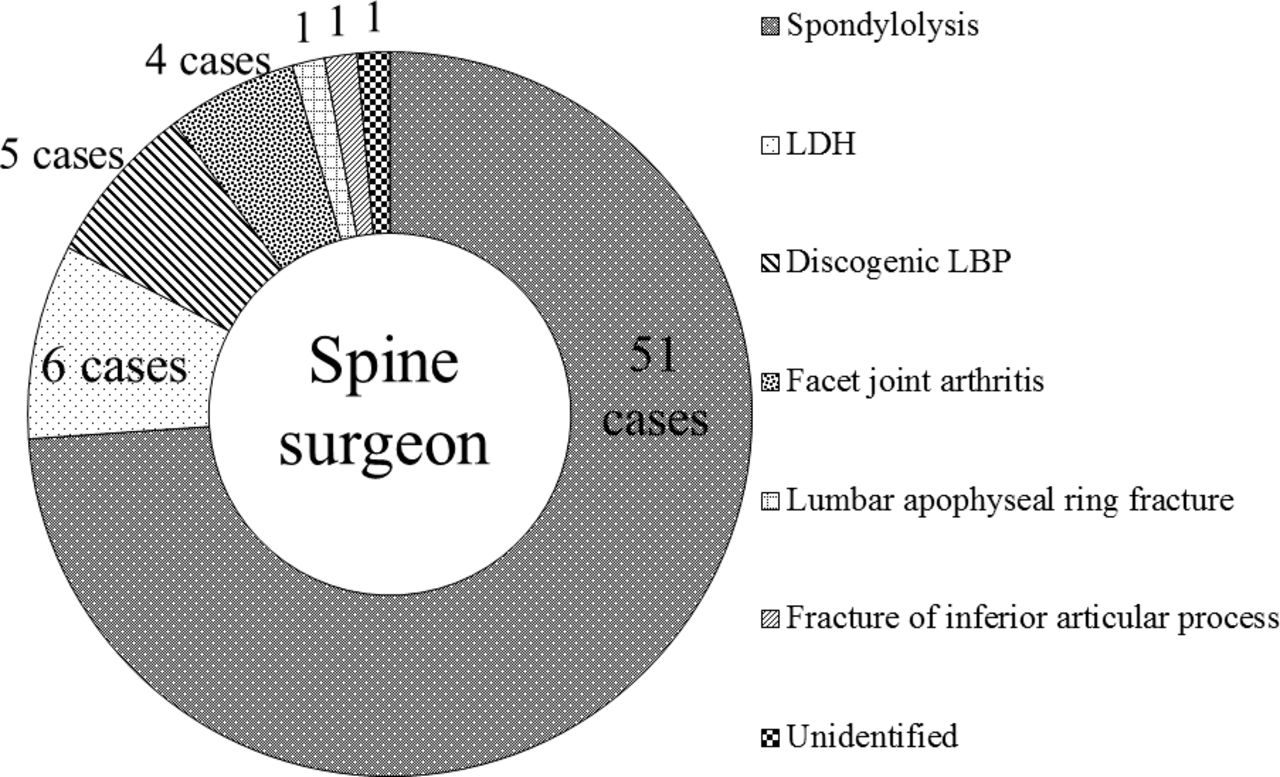
The diagnoses made previously by general orthopedic surgeons were lumbar spondylolysis (n = 47), lumbar disc herniation (n = 5), discogenic low back pain (n = 2), facet joint arthritis (n = 1), an inferior articular process fracture (n = 1), and unidentified cause (n = 13; Figure 2). The diagnoses made by spine surgeons were lumbar spondylolysis (n = 51), lumbar disc herniation (n = 6), discogenic low back pain (n = 5), facet joint arthritis (n = 4), inferior articular process fracture (n = 1), lumbar apophyseal ring fracture (n = 1), and unidentified (n = 1; Figure 3).
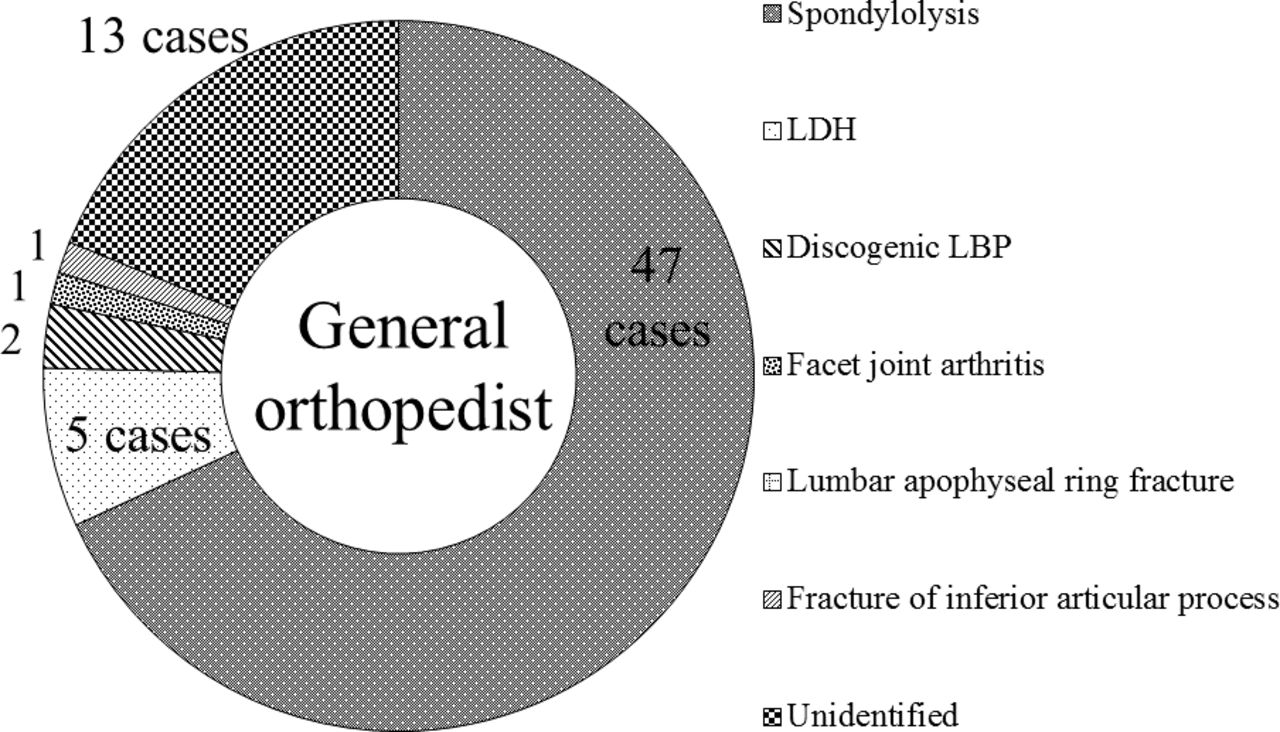
Diagnoses of low back pain made by general orthopedic surgeons. Abbreviations: LBP, low back pain; LDH, lumbar disc herniation.

Diagnoses of low back pain made by a spine surgeon. Abbreviations: LBP, low back pain; LDH, lumbar disc herniation.
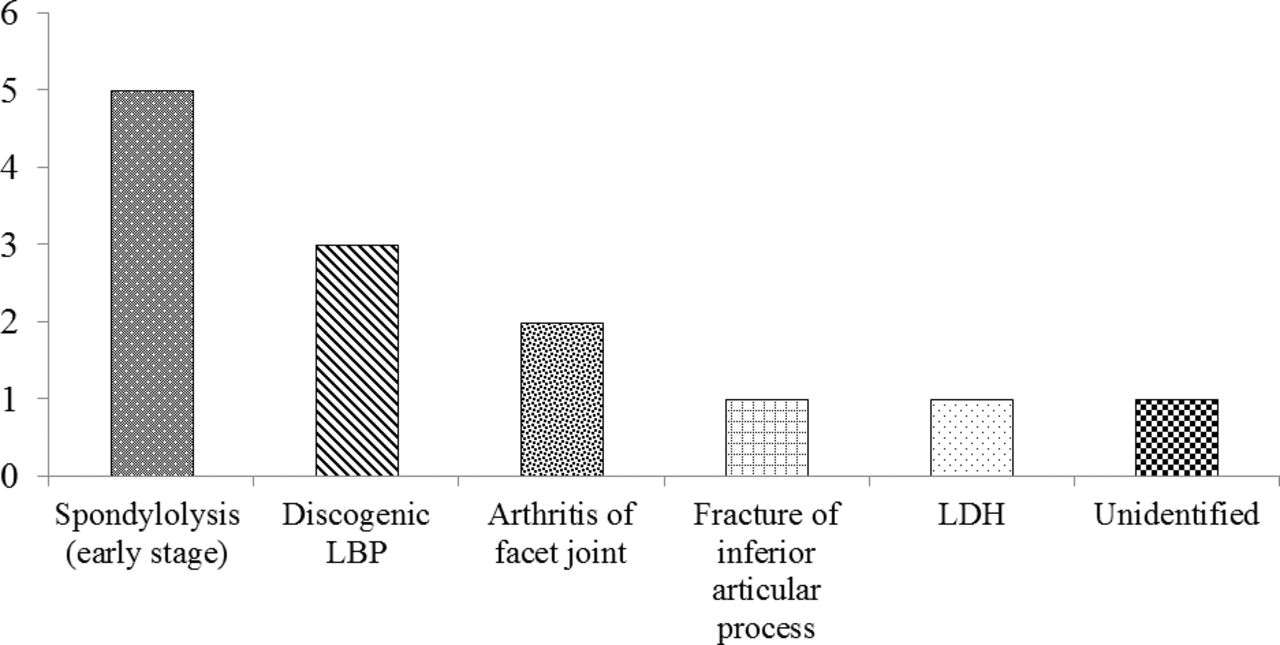
The final diagnosis in the 13 patients previously diagnosed with unidentified low back pain by general orthopedic surgeons were as follows: early-stage lumbar spondylolysis (n = 5), discogenic low back pain (n = 3), facet joint arthritis (n = 2), lumbar disc herniation (n = 1), and lumbar apophyseal ring fracture (n = 1). The diagnosis made by the spine specialist in the remaining case was also unidentified low back pain (Figure 4).
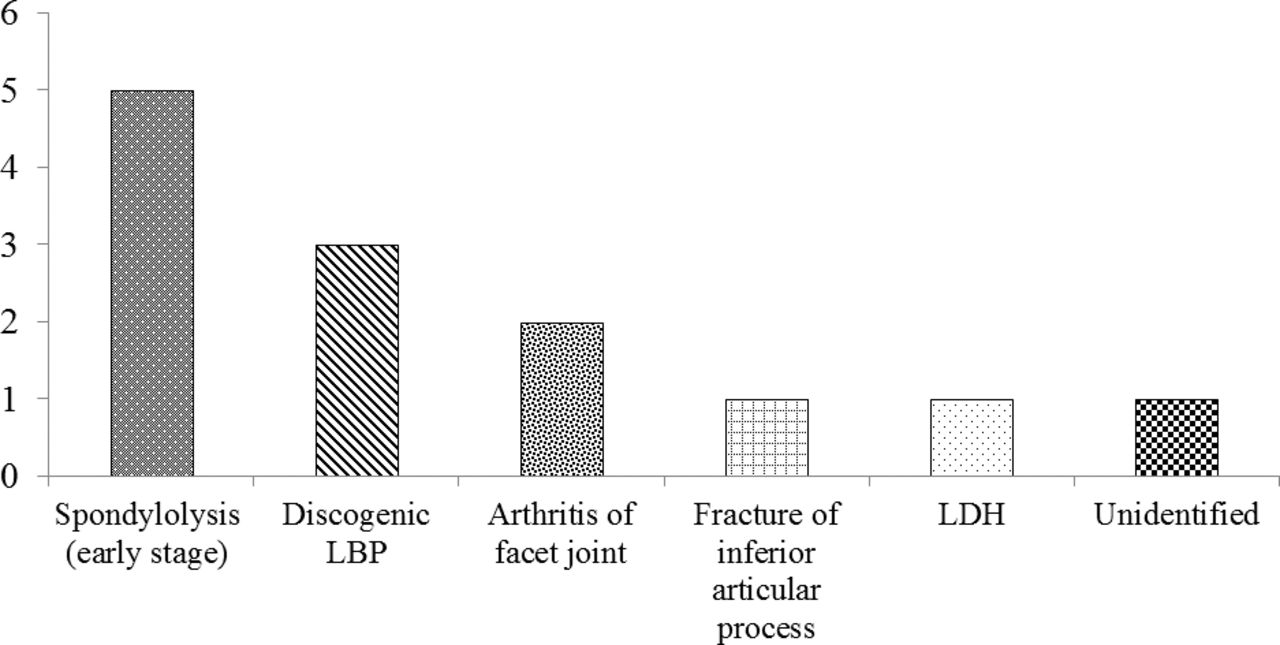
Final diagnoses by a spine surgeon for 13 patients in whom symptoms were classified as NSLBP by general orthopedic surgeons. Abbreviation: LBP, low back pain; LDH, lumbar disc herniation; NSLBP, nonspecific low back pain.
The frequency of NSLBP in adolescent athletes diagnosed by general orthopedic surgeons was 18.9% and decreased to 1.4% after careful imaging and functional block examination by spine surgeons.
CASE PRESENTATION
Case 1: Early-Stage Lumbar Spondylolysis
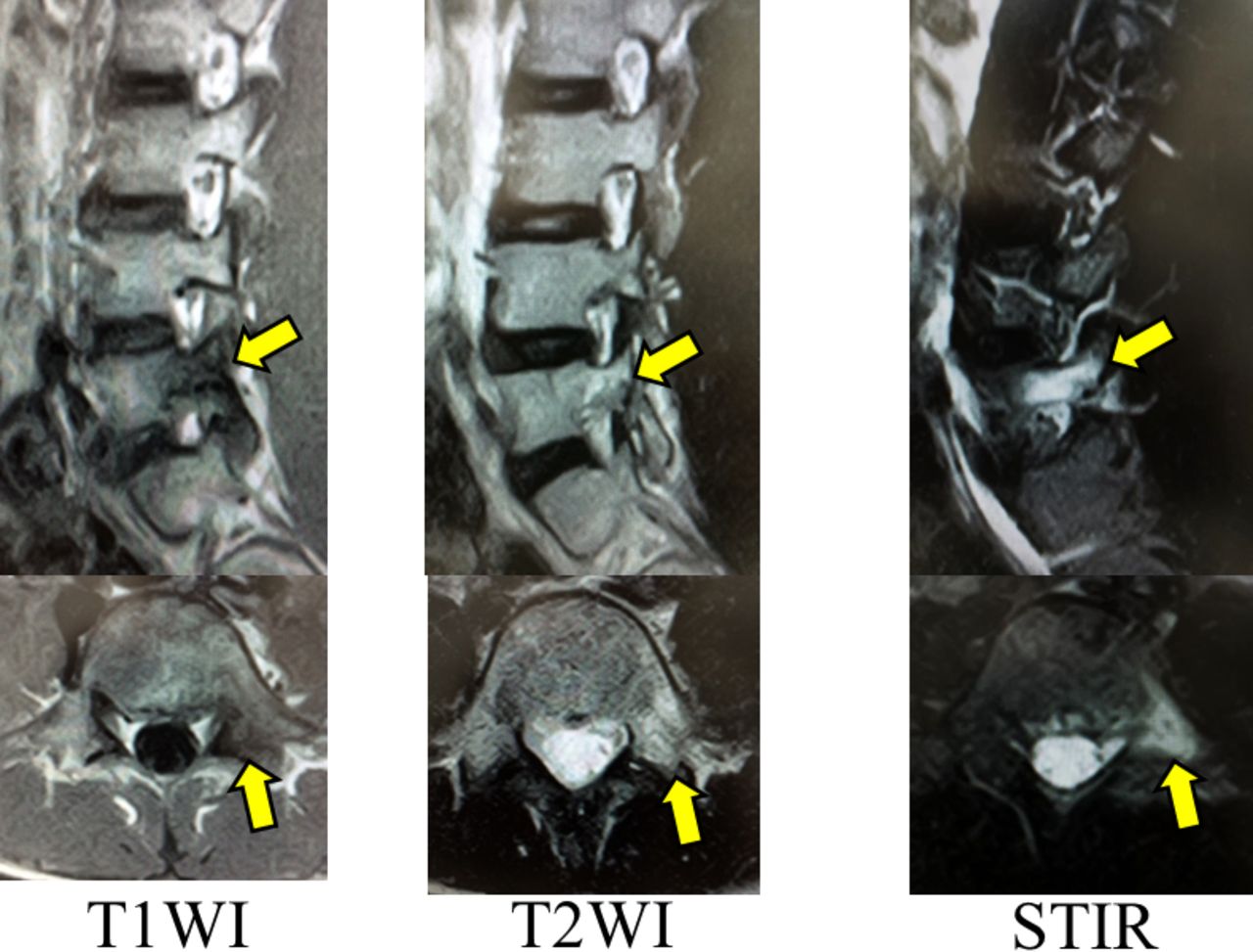
A 13-year-old boy had felt sharp LBP after landing following a jump while playing tennis 4 months earlier. Since then, he had experienced LBP while playing tennis and while running. He was taken to a local doctor, but an x-ray did not provide a diagnosis. He was then brought to our sports clinic for a second opinion. An MRI showed an area of low signal intensity at the left pedicle of L5 on T1-weighted images and an area of high iso-intensity on T2-weighted images. A STIR-MRI showed high signal intensity at L5 (Figure 5), indicating a diagnosis of early-stage lumbar spondylolysis at L5. He was advised to wear a trunk brace and to avoid playing tennis for 3 months, after which his pain resolved.
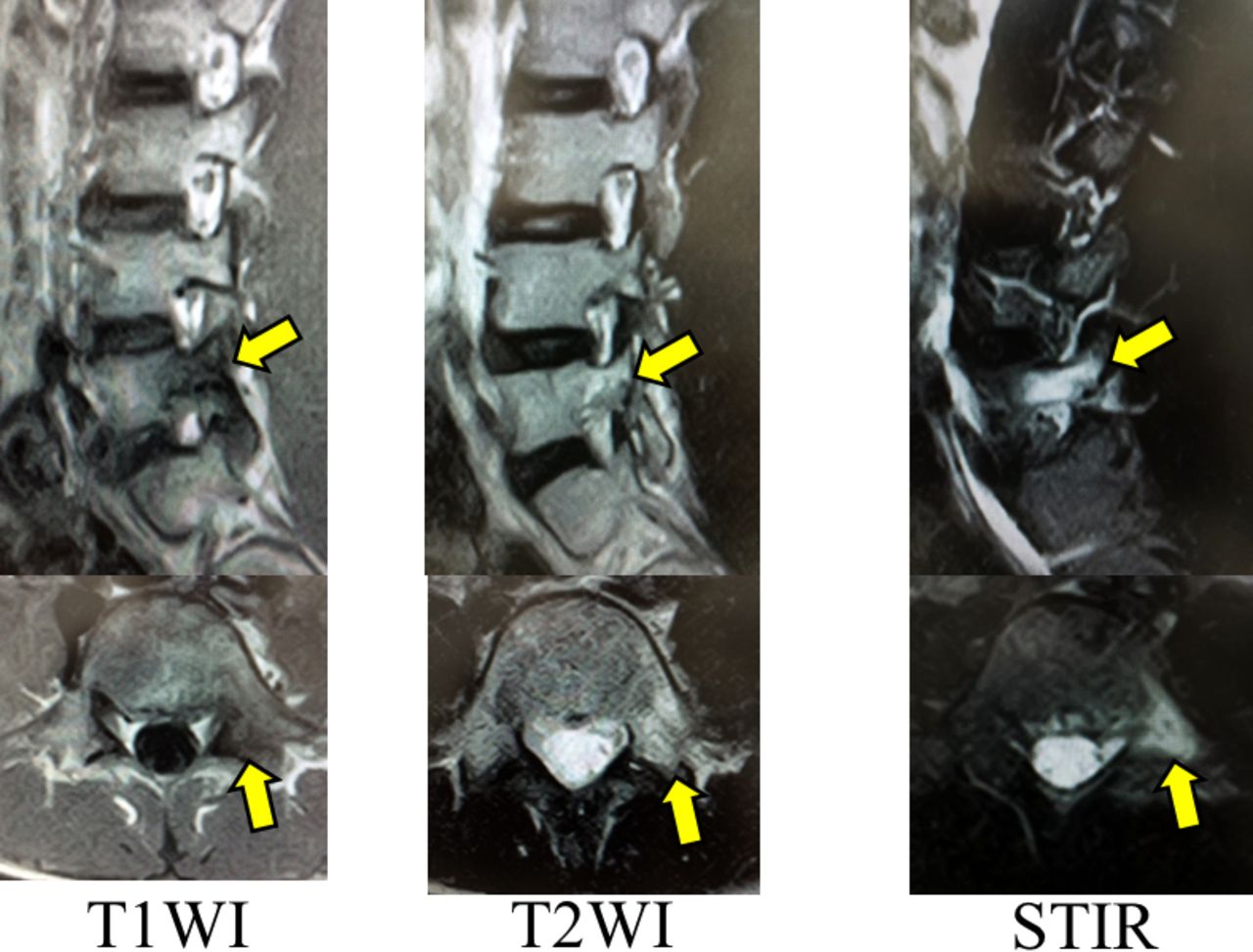
T1- and T2-weighted magnetic resonance imaging (MRI) and short tau inversion recovery (STIR)-MRI for case 1 (a 13-year-old with early-stage lumbar spondylolysis). The STIR-MRI showed the high signal change (arrow) at the left pedicle of L5 more clearly than the T1- and T2-weighted images. Left: T1-weighted image (T1WI). Middle: T2-weighted image (T2WI). Right: STIR.
Case 2: Disc-Related LBP
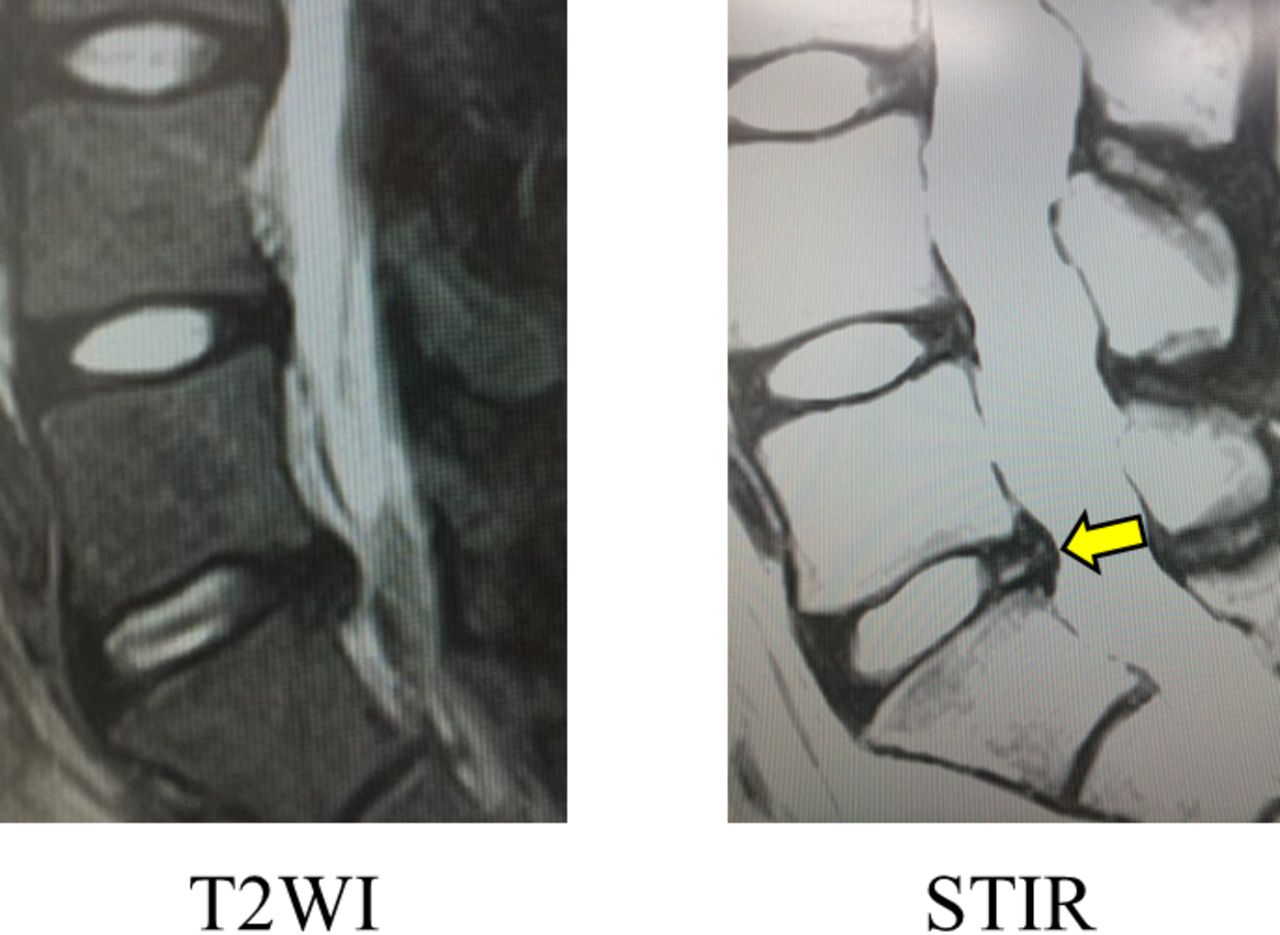
An 18-year-old male baseball player presented with a 2-month history of LBP. The pain occurred only while playing baseball and would worsen during lumbar anteflexion. The cause of his pain was unclear to a local doctor, who referred him to our clinic. A T2-weighted MRI showed only a slight bulging of the disc at L5-S1. A subsequent STIR-MRI showed a high signal intensity zone (HIZ) at the same level (Figure 6). His pain resolved after discography and a nerve block injection.

Magnetic resonance imaging (MRI) T2-weighted image (T2WI) and STIR-MRI for case 2 (an 18-year-old with disc-related low back pain). Only STIR-MRI revealed a HIZ (arrow) at the posterior annulus fibrosus at L5-S1. Abbreviations: HIZ, high signal intensity zone; STIR, short tau inversion recovery.
Case 3: Facet Joint Arthritis
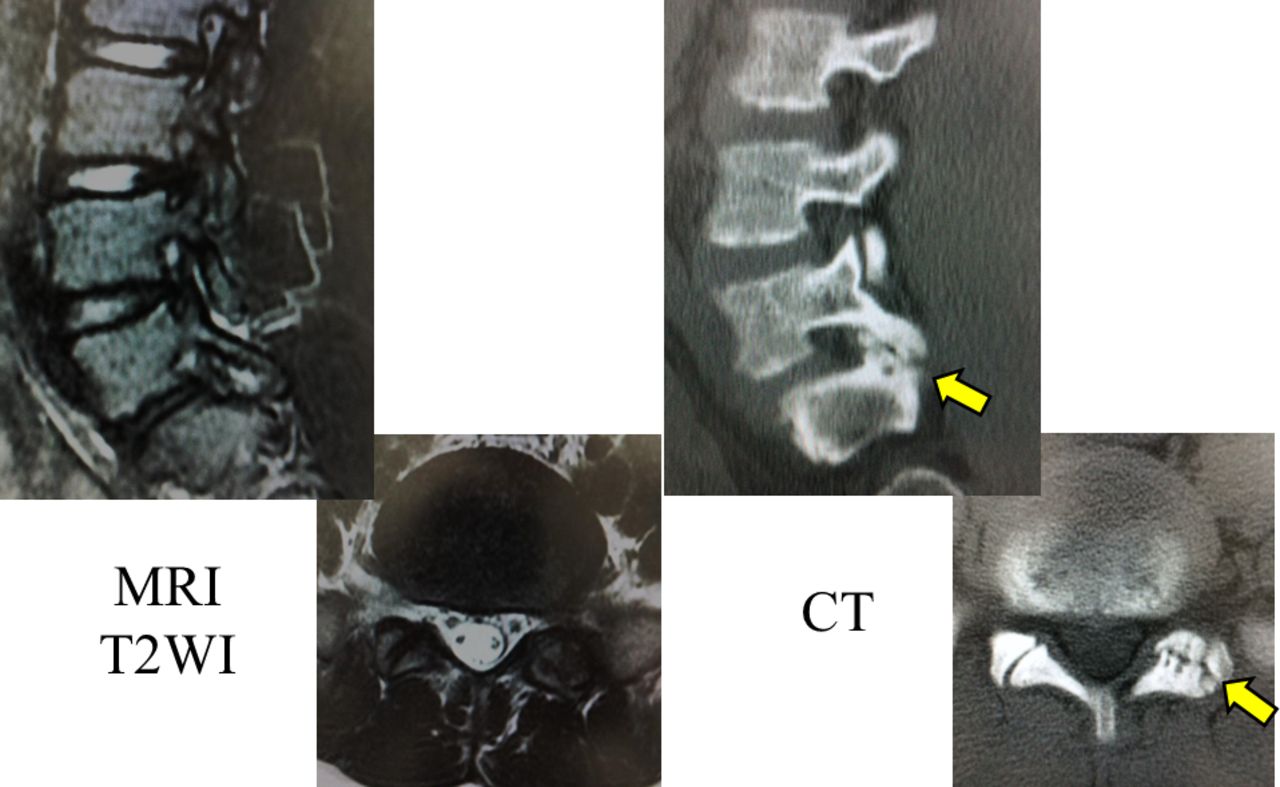
A 15-year-old boy had felt severe LBP at the time of a head-on collision with an opponent in a rugby game 3 years ago. His pain then decreased gradually, but persisted and tended to worsen during lumbar retroflexion and left rotation. A local doctor was unable to identify the cause of his LBP, so the boy visited our clinic. The cause of his pain could not be identified on plain radiography or MRI, but CT revealed left facet joint osteoarthritis at L5-S1 (Figure 7). His pain disappeared temporarily after a facet joint injection, confirming a diagnosis of facet joint arthritis.

Magnetic resonance imaging (MRI) T2-weighted image (T2WI) and CT scan for case 3 (a 15-year-old with facet joint arthritis). Although there were not obvious abnormal findings on MRI, CT clearly showed osteoarthritis of left facet joint (arrow) at the level of L5-S1. Left: MRI T2-weighted image. Right: CT. Abbreviations: CT, computed tomography.
Case 4: Lumbar Apophyseal Ring Fracture
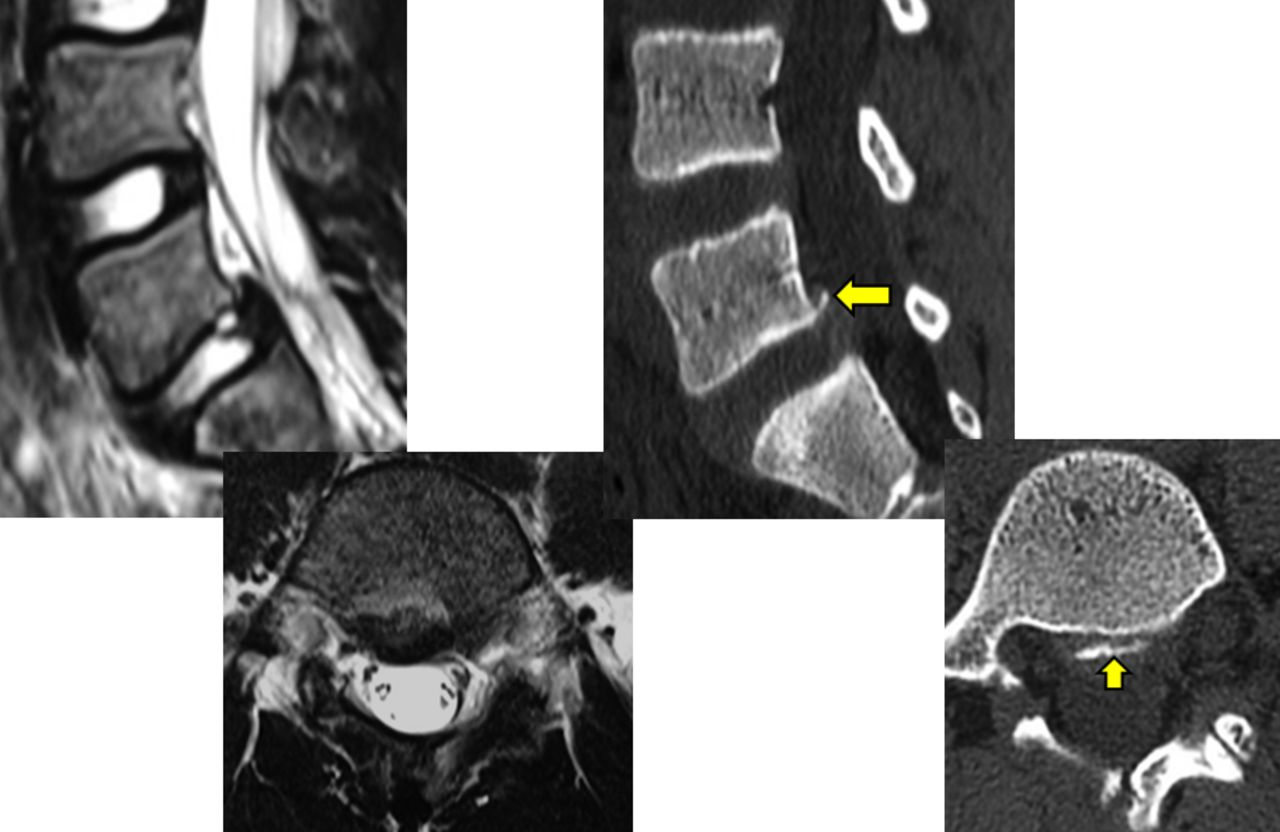
A 12-year-old boy who played soccer presented with a diagnosis of L5 isthmic spondylolysis made by another doctor. Two months earlier, he had felt severe acute LBP during a soccer game; the pain did not resolve and was causing severe problems in activities of daily living. The previous doctor explained that the cause of his severe pain was worsening of isthmic spondylolysis. He was brought to our clinic for a second opinion. A T2-weighted MRI showed only slight central bulging of the L5-S1 disc without compression of the neural tissue. Computed tomography revealed an apophyseal ring fracture at the level of the caudal L5 endplate (Figure 8). A semirigid brace was recommended and a nonsteroidal anti-inflammatory drug was prescribed for 1 month. His pain subsequently resolved, and 3.5 months after onset, he was able to return to soccer practice.

Magnetic resonance imaging (MRI) T2-weighted image and CT scan for case 4 (a 12-year-old with a lumbar apophyseal ring fracture). T2-weighted MRI showed only slight central bulging of the L5-S1 disc, whereas CT revealed an apophyseal ring fracture (arrow) at the level of the caudal L5 endplate. Abbreviations: CT, computed tomography.
DISCUSSION
This study yielded 2 important findings. The first was a rate of NSLBP in adolescent athletes of 18.9% when patients were examined by general orthopedic surgeons that decreased to 1.4% when the same patients were examined by spine surgeons. The second finding was that early-stage lumbar spondylolysis, discogenic LBP, facet joint arthritis, and lumbar apophyseal ring fractures are not easily diagnosed by general orthopedic surgeons.
According to international reports,1,4–10 the annual prevalence of LBP in children and adolescents varies between 13% and 60.3%. On reviewing the literature for children and adolescents, Balague et al11 reported that older age, history of spinal trauma, family history of LBP, trunk asymmetry, being taller, smoking, female sex, playing competitive sport, strenuous physical activity, depression, and emotional or stress factors were significantly associated with low back pain.
More than a decade ago, Deyo et al2,3 reported that NSLBP accounted for approximately 85% of all cases of LBP. However, this number was reported by a family physician, and the radiological diagnostic tools used then were not as good as the current devices. Very recently, Suzuki et al12 reported finding NSLBP in only 22% of 320 patients with LBP, which is in contrast with the 85% reported by Deyo et al.2,3 Suzuki et al12 used meticulous radiological examination and functional regional blocks, as used in our practice. However, unlike those in the present report, all their patients were adults over 20 years of age. Taking the standpoint of a pediatric orthopedic surgeon, Gennari et al13 investigated the etiology of adolescent LBP diagnosed using a medical interview, clinical examination, and imaging and reported the rate of NSLBP to be approximately 30%. In our study, this rate was around 20% when the diagnosis was made by a general orthopedic surgeon.
The orthopedic surgeons did not perform routine functional block examinations or STIR-MRI. When we performed these additional diagnostic procedures, the rate of NSLBP decreased to around 2%. It is possible that this low rate of diagnosis of NSLBP by the spine surgeon was because the patients were seeking a second opinion, so their LBP was not in the acute phase. Sometimes strain of a back muscle or a facet joint sprain may cause acute LBP; however, it is difficult to reach a diagnosis on the basis of radiological findings.
MRI is reported14,15 to be very useful for investigating inflammatory conditions. The STIR-MRI is an inversion technique that nulls the fat signal change on the basis of T1 values16; furthermore, it is a powerful visualization tool because the image can provide useful information about intra-articular effusion or inflammation as a very clear high-signal area.17 In patients 1 and 2, STIR-MRI clearly showed a high intensity area at the pedicle and disc, respectively. We were then able to diagnose early-stage lumbar spondylolysis in patient 1 and disc-related LBP in patient 2. The following are disorders that may be overlooked as a cause of LBP and misdiagnosed as NSLBP by a general orthopedic surgeon.
Early-Stage Lumbar Spondylolysis
Lumbar spondylolysis is a well-known defect of the pars interarticularis that is common in young athletes and occurs in around 6% of the general population.18,19 According to several biomechanical studies,20,21 the pathogenesis of lumbar spondylolysis is considered to be stress fracture. It has been reported22,23 that the spondylolysis seems unrelated to LBP in adult patients, but in young athletes, it is a common cause of LBP. Computed tomography is considered to be the best tool for making an accurate diagnosis and for determining the stage of lumbar spondylolysis,24 but it is unreliable for detecting early-stage disease. Recent advances in MRI have made early diagnosis of spondylolysis possible.25,26 A high signal change in the adjacent pedicle on T2-weighted MRI and STIR-MRI can indicate spondylolysis before discontinuity of the pars interarticularis appears.27 In general, T2-weighted MRI appears able to detect abnormal findings, but sometimes the signs can be missed. A STIR-MRI can show high signal change in the pedicle, making it easy to identify lumbar spondylolysis in the early stages when it is possible to achieve successful bone union.
Discogenic LBP
Chronic LBP is attributed to intervertebral disc damage in more than 40% of patients, of whom 70% are found to have no nerve root compression.28,29 Disc-related LBP due to internal disc disruption is considered to be the most common cause of chronic LBP.29,30 Provocative discography has been considered the “gold standard” for diagnosis and management of disc-related LBP in spite of its invasiveness and associated complications. In 1992, Aprill and Bogduk31 described HIZ on MRI for diagnosing disc-related LBP. They demonstrated a prevalence of 28.6% for HIZ, with sensitivity, specificity, and positive predictive values of 71%, 89%, and 86%, respectively, for diagnosing symptomatic LBP. The HIZ was originally defined as a high-intensity signal on T2-weighted MRI located posteriorly in the annulus fibrosus and clearly dissociated from the signal of the nucleus pulposus.31 Some histological studies32–34 have shown inflammatory granulation tissue at sites of HIZ. These inflammatory tissues produce proinflammatory cytokines and mediators that sensitize the nociceptors within the disc and cause pain. Reliable and sophisticated measures are needed for precise detection of HIZ to improve the clinical utility of this finding.35 In case 2, STIR-MRI was effective for detecting HIZ.
Facet Joint Arthritis
The facet joints are the only synovial joints in the spine, and each consists of hyaline cartilage overlying subchondral bone, a synovial membrane, and a joint capsule. Owing to their high level of mobility and the large forces affecting the facet joint, especially in the lumbar area, the facet joints can develop significant degenerative changes and be a potential source of pain and disability. In comparison with standard radiographs, CT improves anatomic evaluation of the facet joints because of its ability to image the joint in the axial plane and the high contrast between bony structures and the surrounding soft tissue.36 Due to its precise demonstration of osseous details37 and relatively low cost, CT is the preferred imaging method for lumbar facet joint osteoarthritis. However, several studies38 have reported that CT was not reliable for identification of a painful facet joint, and MRI has not been investigated in this regard. Furthermore, the efficacy of intra-articular injection therapy for LBP potentially associated with facet joint osteoarthritis has not been clearly established. Lewinnek and Warfield39 reported that 96% of their patients with facet joint osteoarthritis responded to such injections, whereas Schwarzer et al38 were unable to demonstrate a significant correlation between the degree of osteoarthritis on CT and the LBP following intra-articular facet joint block. In case 3 here, the pain disappeared temporarily after a block injection to the facet joint using lidocaine. There was no other abnormal finding around the lumbar spine, so we were able to diagnose facet joint arthritis.
Apophyseal Ring Fracture
Separation of the posterior apophyseal ring occurs mainly in children and adolescents due to the process by which the apophyseal ring forms.40,41 Ossification of the ring apophysis occurs at the age of 6 to 9 years. The ossified apophysis then fuses with the vertebral body at about 17 years and is completely fused by approximately 20 years.42 The attachment between the posterior ring apophysis and the vertebral body is a relatively weak point until osseous union is complete; therefore, herniation of a lumbar disc may be associated with separation of the posterior apophyseal ring after acute or chronic trauma in children and adolescents.42,43 The diagnosis can be difficult even on MRI. Tamaki et al44 described 3 adolescent athletes who had both lumbar spondylolysis and a lumbar posterior apophyseal ring fracture. The researchers stressed that it is important to perform not only MRI and radiography but also CT to identify these fractures. Furthermore, they emphasized that only CT, which offers superior definition of bony tissues, can clarify the exact diagnosis in such cases.
We recognize that the current study has 3 limitations. First, the diagnoses by spinal surgeons were made in 1 institution and we examined only adolescent athletes. A multicenter study that includes a larger number of spine surgeons is needed for more accurate assessment of the frequency of NSLBP. Second, we did not investigate psychosocial factors in our patients, so we cannot exclude the contribution of psychogenic LBP to our results. Our patient in whom the cause of pain could not be identified even by a spine specialist might have had a psychogenic cause of LBP. Third, we recognize that there is selection bias between these 2 cohorts because it took a longer time to attend spine surgeons compared with general orthopedic surgeons. There is the possibility that the symptom complex becomes more specific with time and may lead to an improve rate of diagnosis. In addition, the extensive evaluation using MRI or CT scan requires additional cost. We did not evaluate the additional cost in extensive examinations in this study. Further research about the cost for them will be expected.
However, in spite of these limitations, this is the first report comparing rates of unidentified LBP diagnosed in adolescent athletes by general orthopedic surgeons and spine surgeons and reveals the pathology in patients with NSLBP.
CONCLUSIONS
In this study, the frequency of NSLBP in adolescent athletes diagnosed by general orthopedic surgeons was 18.9%. This rate decreased to 1.4% when LBP in the same patients was investigated by spine surgeons. A thorough medical interview, a careful physical examination, and appropriate diagnostic imaging, such as STIR-MRI, are important when looking for the cause of LBP.
Footnotes
Disclosures and COI: None of the authors have a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.