


ABSTRACT
Background: The purpose of this study was to determine if oblique magnetic resonance imaging (MRI) sequences affect the surgical treatment recommendations for patients with cervical radiculopathy.
Methods: In this cohort study consecutive clinical cases of persistent cervical radiculopathy requiring surgical intervention were randomized, blinded, and reviewed by 6 surgeons. Initially each surgeon recommended treatment based on the history, physical examination, and axial, coronal and sagittal preoperative magnetic resonance (MR) images; when reviewing the cases the second time, the surgeons were provided oblique MR images. This entire process was then repeated after 2 months. Change in surgical recommendation, interobserver and intraobserver reliability and the average number of levels fused was determined.
Results: The addition of the oblique images resulted in the surgical recommendation being altered in 49.2% (59/120) of cases; however, the addition of oblique images did not substantially improve the interobserver reliability of the treatment recommendation (κ = .57 versus.57). Similarly, the overall intraobserver reliability using only traditional MRI sequences (κ = .64) was only slightly improved by the addition of oblique images (κ = .66). Lastly, the addition of oblique images did not change the average number of levels fused (traditional MRI = 1.38, oblique MRI = 1.41, P = .53), or the total number of 3-level fusions recommended (6 versus 6, P = 1.00)
Conclusions: The additional oblique images resulted in a change to the surgical plan in almost 50% of cases; however, it had no substantial effect on the reliability of surgical decision making. Further studies are needed to see if this alteration in treatment affects clinical outcomes.
Level of Evidence: 3
INTRODUCTION
Cervical radiculopathy is a common condition with an age-adjusted incidence rate of 83.2 per 100 000 people. It most commonly affects patients in their sixth decade of life and is often caused by compression of the exiting cervical nerve root in the neural foramen.1 It classically presents with pain radiating from the neck down the arm in a dermatomal pattern, and it may be associated with concomitant motor and sensory deficits2; however, often the symptoms do not follow the classic dermatomal distributions, such that the pain and numbness affects multiple dermatomes.3 Because of this, the surgical treatment algorithm for persistent cervical radiculopathy is based off of the combination of patient symptoms as well as advanced imaging studies demonstrating compression of the neural elements.
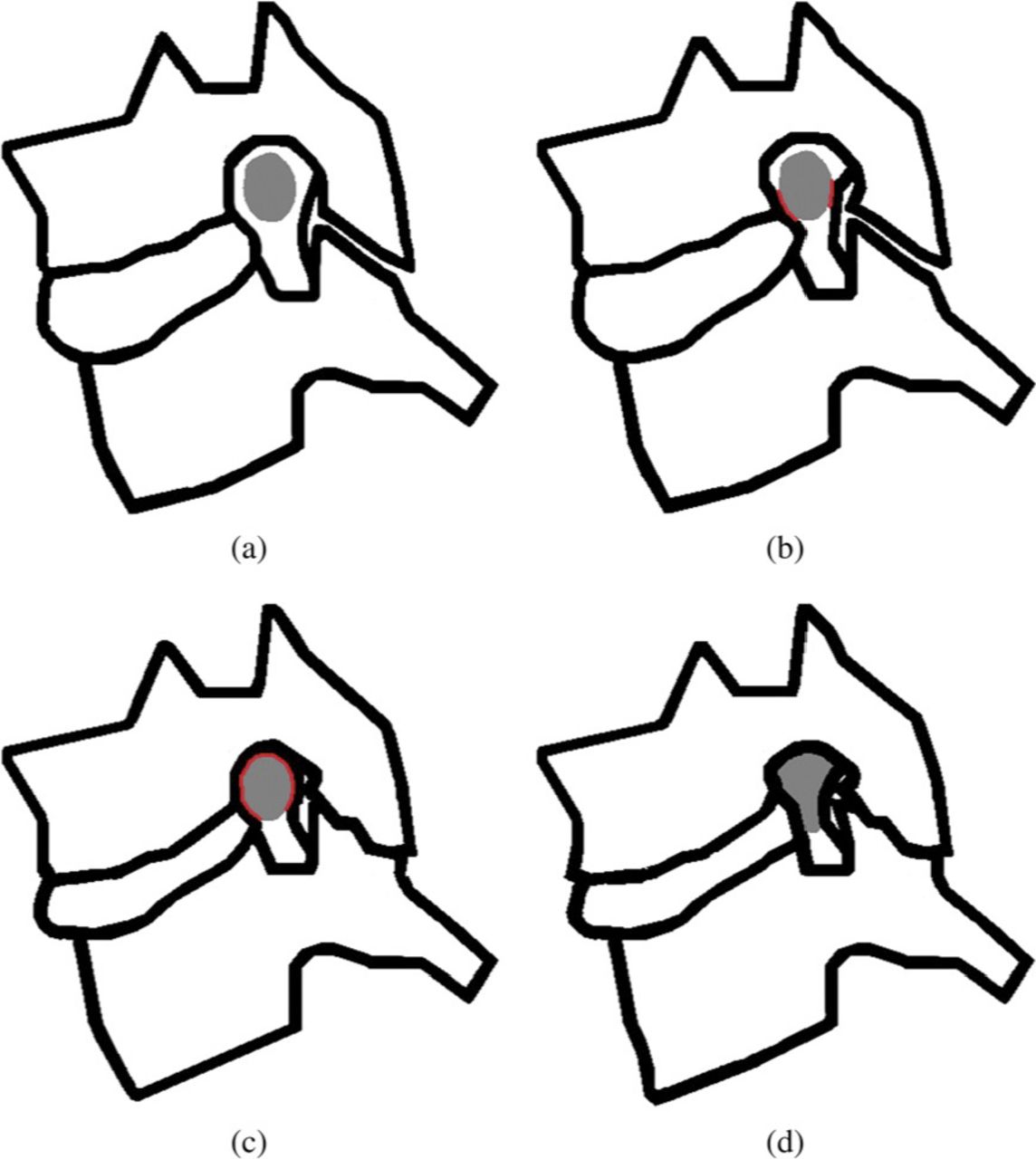
Magnetic resonance imaging (MRI) is the most commonly used advanced imaging technique for the diagnosis of cervical radiculopathy, and while this modality offers excellent details of the neural structures, it traditionally consists of images in the axial, sagittal, and coronal plane. With the cervical foramen oriented at approximately a 45-degree oblique angle, these sequences often do not provide clear views of neural foramen. This fact has long been recognized, with Modic et al4 reporting in 1987 that the additional information obtained from oblique MRI sequences can provide information that may affect the treatment of cervical radiculopathy. More recently, a new classification for foraminal stenosis based on T2 oblique magnetic resonance (MR) images (Figure 1) has been proposed.5,6 The aim of the current study is to determine if oblique MRI sequences affect the surgical treatment recommendations for patients with cervical radiculopathy.

The Park classification for foraminal stenosis based off of T2 oblique magnetic resonance images: (a) no stenosis, (b) mild stenosis, (c) moderate stenosis, (d) severe stenosis.
METHODS
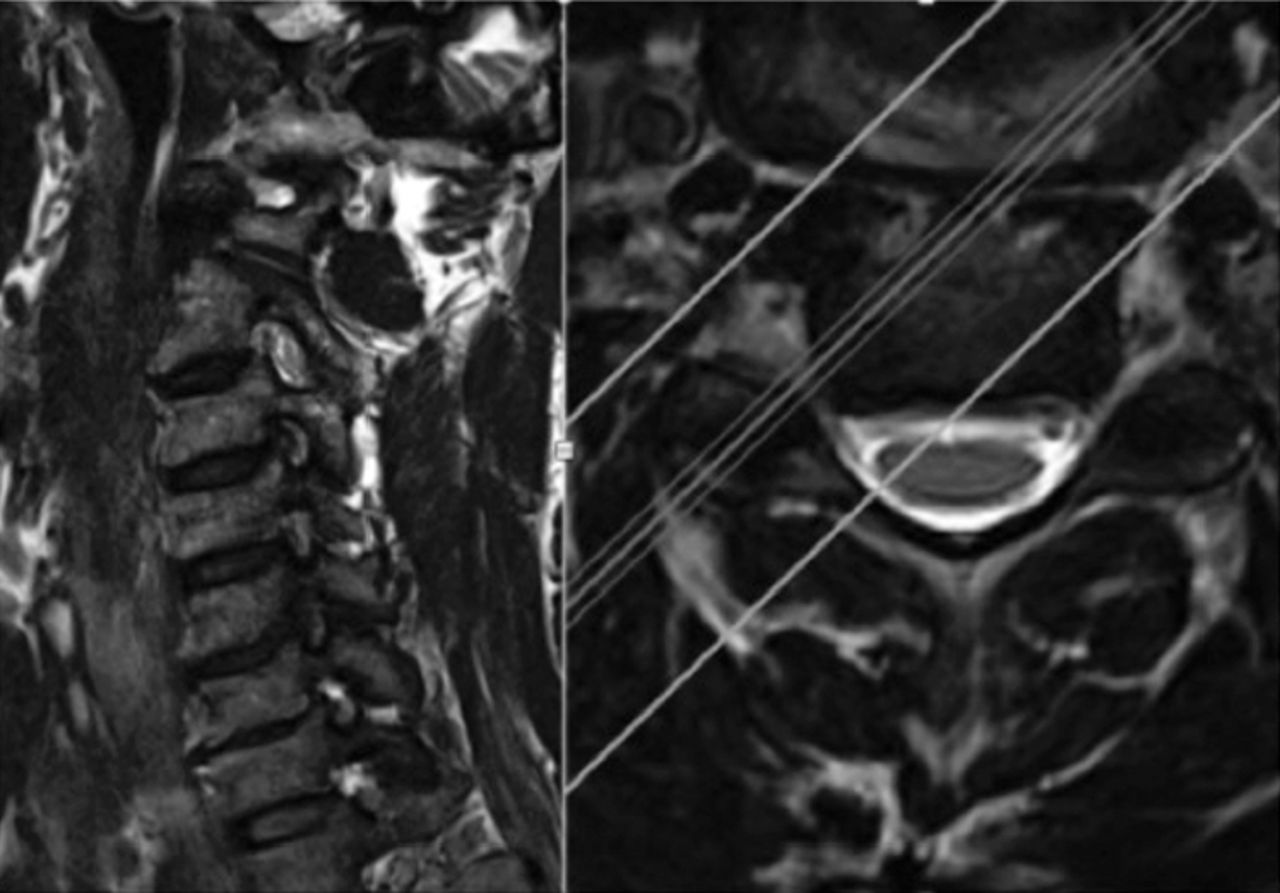
Twenty consecutive patients who underwent an anterior cervical discectomy and fusion (ACDF) for persistent cervical radiculopathy, and who had an MRI performed at a single institution, with T1 and T2 sagittal, coronal, and axial sequences, as well as T2 oblique sequences available were identified. After the imaging studies were deidentified and the cases were randomized, 6 surgeons (3 fellowship-trained orthopedic spine surgeons and 3 trainees—1 orthopedic spine fellow and 2 orthopedic surgery residents) reviewed each case and identified the levels that they felt warranted surgical intervention. The cases were reviewed a total of 4 times. Initially each surgeon recommended treatment based on the history, physical exam (Table 1), and axial, coronal and sagittal preoperative MR images; 1 week later the cases were randomly reorganized and the surgeons were provided with all of the previous information as well as the oblique MR images (Figure 2). Finally, this entire process was repeated after 2 months.
The history and physical exam for each case that was provided to the reviewers.
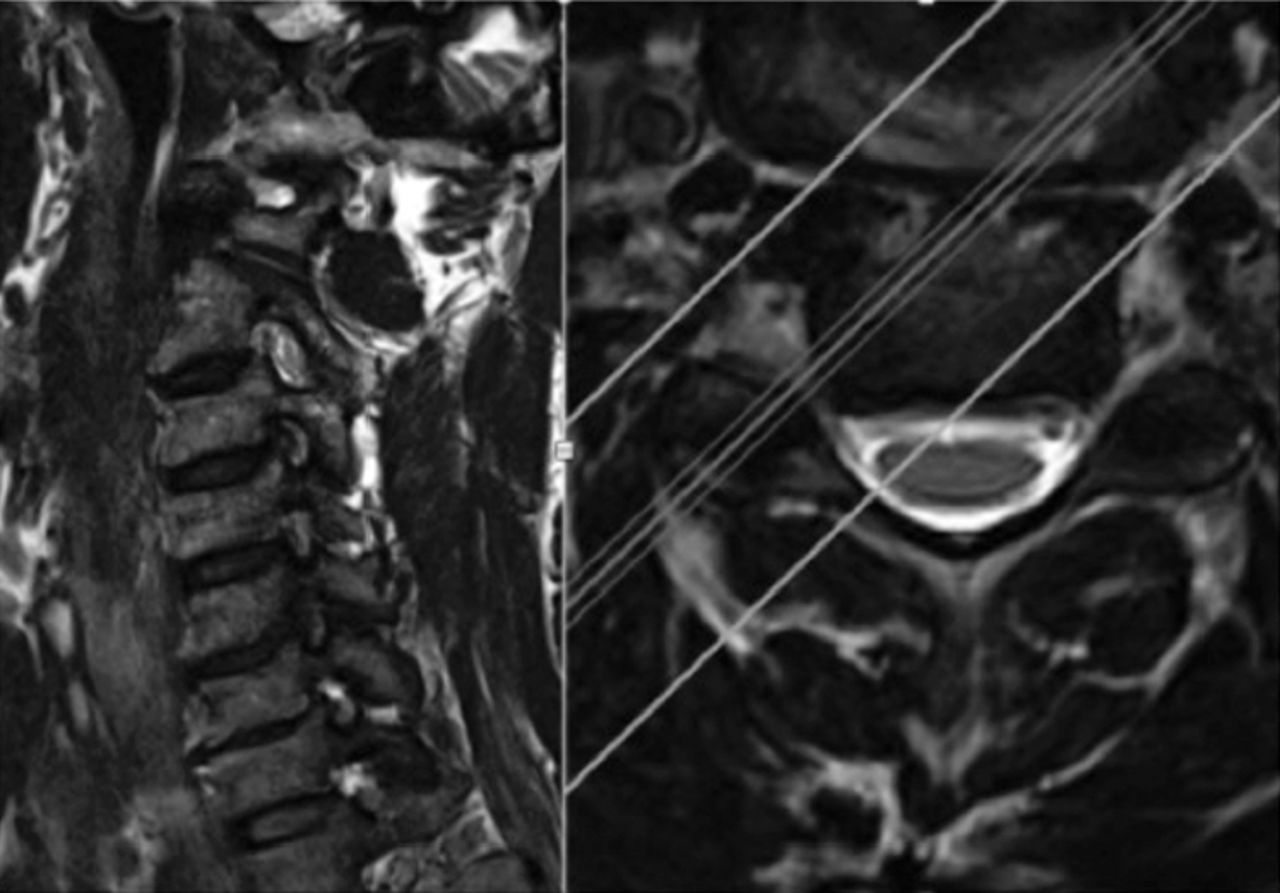
A representative oblique image. The oblique image is on the left, and it clearly demonstrates C5/6 right-sided foraminal stenosis. The image on the left is the corresponding axial image.
Statistical Methods
The Fleiss kappa coefficient (κ) was used to assess the agreement of the treatment recommendations with and without the oblique images among the 6 surgeons (interobserver reliability). Additionally, the reproducibility of the treatment recommendation for the same observer with the same information available 2 months apart (intraobserver reliability) was established. The Landis and Koch grading system was used to interpret the kappa values. In this system a value of less than .2 is consistent with slight agreement; a value between .2 and .4 represents fair agreement; a value between .4 and .6 indicates moderate agreement; a value between .6 and .8 indicates substantial agreement, and a kappa value greater than .8 indicates excellent agreement.
The continuous variables of each cohort were compared using a 2-sided (tailed) Student t test for normally distributed data, and a Fisher exact test was performed to analyze the categorical data. Statistical significance was accepted with a P value < .05. All of these analyses were performed using the statistical software language R version 3.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
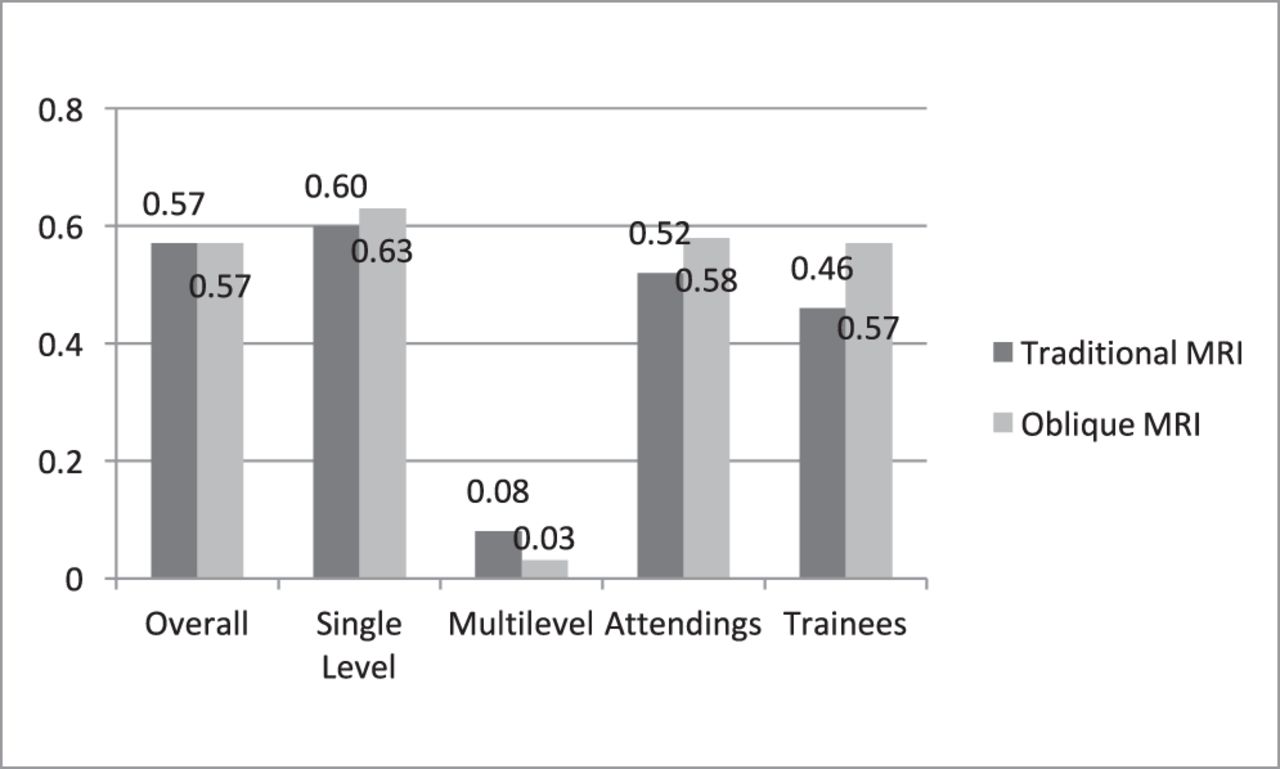
The addition of oblique images led surgeons to alter their surgical plan in 49.2% (59/120) of cases; however, it did not substantially affect the reliability analysis. The overall interobserver reliability (Figure 3) of the treatment recommended when only traditional MRI sequences were provided (κ = .57) was moderate, and it was not improved by the addition of oblique images (κ = .57). Similarly, in the cases in which the definitive surgery performed (defined as the treatment that the patient actually underwent) was a single-level ACDF (13 cases), the interobserver reliability was similar between the 2 groups (traditional MRI: κ = .60, oblique MRI: κ = .63). Cases in which the definitive procedure performed was a multilevel ACDF (7 cases, all two-level surgeries) had only slight interobserver reliability, and this was slightly worse with the addition of oblique images (traditional MRI: κ = .08, oblique MRI: κ = .03). The addition of oblique images did slightly improve the interobserver reliability for both attending spine surgeons (traditional MRI: κ = .52, oblique MRI: κ = .58) and for trainees (traditional MRI: κ = .46, oblique MRI: κ = .57).

Graphic representation of the interobserver reliability. Abbreviation: MRI, magnetic resonance imaging.
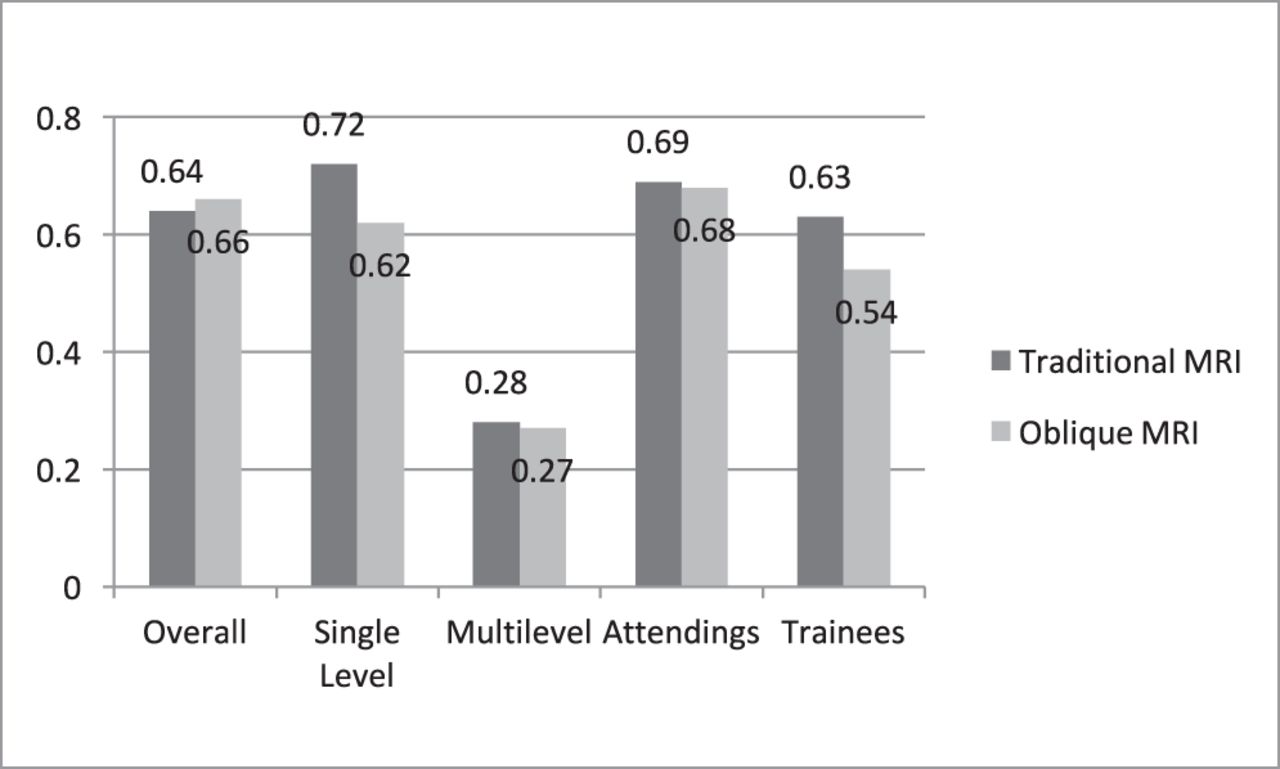
The overall intraobserver reliability (Figure 4) of the treatment recommended when only traditional MRI sequences were provided (κ = .64) was substantial, and it was slightly improved by the addition of oblique images (κ = .66). Intraobserver reliability for single-level pathology was actually worsened by the addition of oblique images (traditional MRI: κ = .72, oblique MRI: κ = .62), and the addition of oblique images had no effect on the intraobserver reliability for multilevel pathology (traditional MRI: κ = .28, oblique MRI: κ = .27). Similarly, the addition of oblique images did not improve the interobserver reliability of attending surgeons (traditional MRI: κ = .69, oblique MRI: κ = .68), and having the oblique views available lowered the intraobserver reliability of trainees (traditional MRI: κ = .63, oblique MRI: κ = .54). Lastly, the addition of oblique images did not change the average number of levels fused (traditional MRI = 1.38, oblique MRI = 1.41, P = .53), or the total number of 3-level fusions recommended (6 versus 6, P = 1.00).
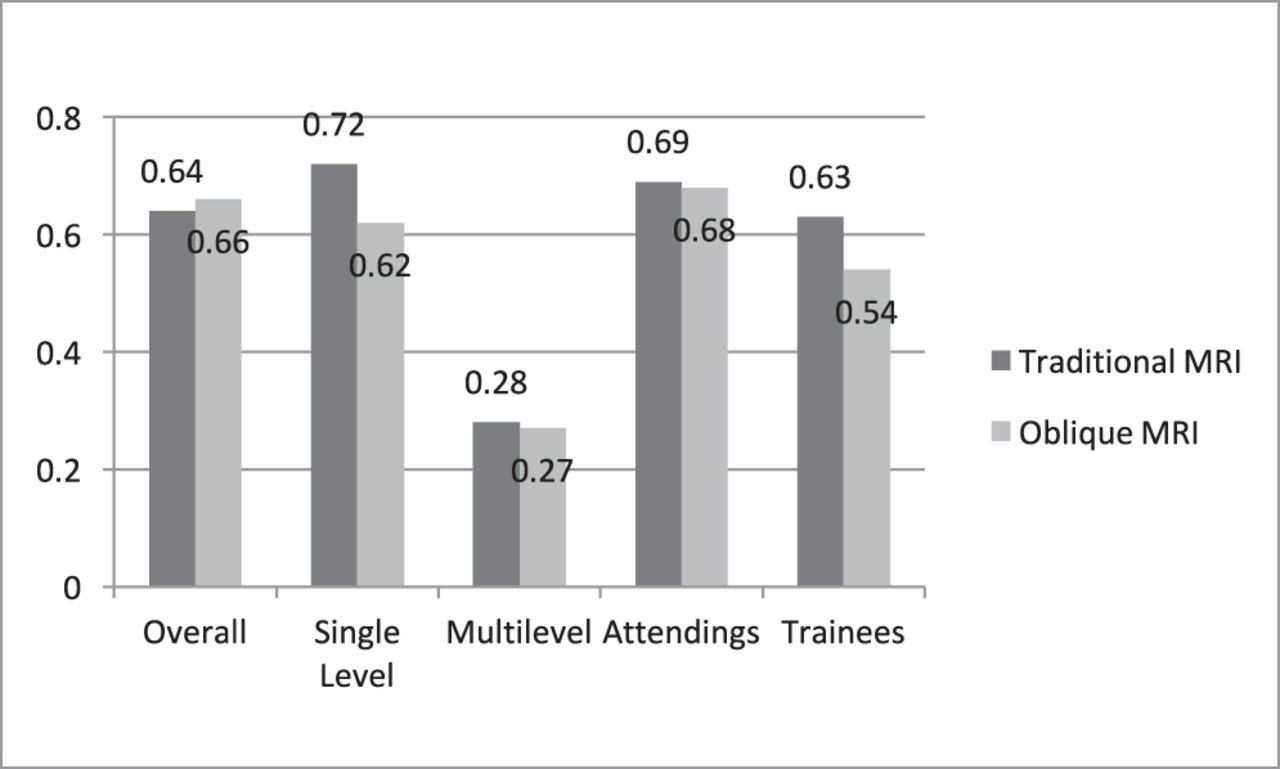
Graphic representation of the intraobserver reliability. Abbreviation: MRI, magnetic resonance imaging.
DISCUSSION
The purpose of the current study was to determine if oblique MRI sequences affect the surgical treatment recommendations for patients with cervical radiculopathy. Our results demonstrated that additional oblique images altered the treatment plan in almost 50% of the cases; however, it had no substantial effect on either the interobserver or intraobserver reliability of surgical decision making.
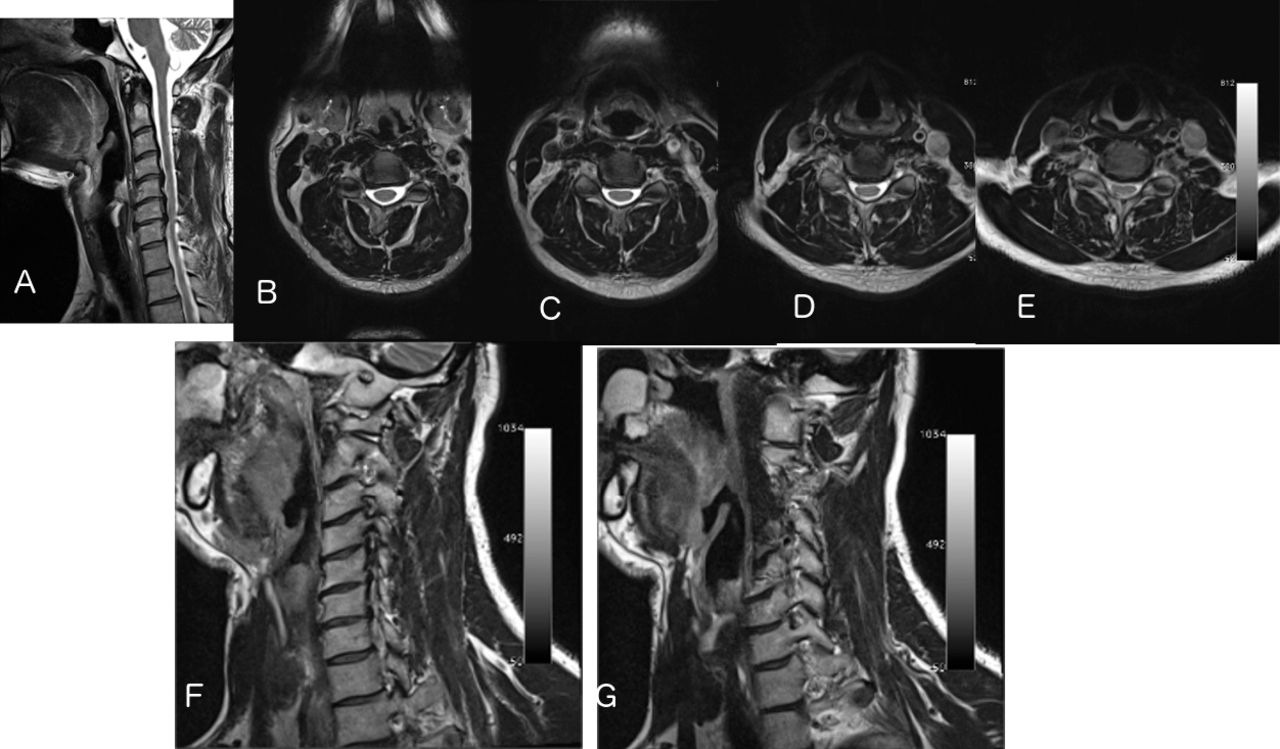
This alteration of the surgical plan associated with the addition of oblique images is the most important finding of the study with regard to individual patient care, as it is possible that the additional information obtained from the oblique views may improve the clinical results. Classically, an ACDF for cervical radiculopathy has been reported to be successful in 80% to 90% of patients7; however, the reason some patients fail to see improvement is unclear. It is possible that failure of treatment in these patients is the result of a prefixed or postfixed cord that alters normal patterns of cervical innervation, and with the suboptimal foraminal views afforded by traditional MRI sequences, surgeons may select the incorrect level for the symptoms. Because the oblique views allow surgeons a clearer view of the compression occurring in the neural foramen, they may be better able to correlate the symptoms to the location of nerve compression. Figure 5 is a case example of how the oblique view changed management. The patient presentenced with persistent radicular pain in the entire right arm. One of the reviewers recommended a C3-C6 ACDF without the oblique views, and a C4-C7 ACDF when the oblique views were present. Because of the retrospective nature of this study, it is unclear if this alteration in the treatment plan would have resulted in improved clinical outcomes. Future prospective clinical studies are needed to determine if the addition of oblique images increases the clinical outcomes of patients undergoing an ACDF for cervical radiculopathy.

(A) T2 sagittal magnetic resonance imaging (MRI); (B-E) axial images at C3/4, C4/5, C5/6, and C6/7, respectively. (F) Oblique MRI with an enface view of C3/4. (G) Oblique MRI with an enface view of C6/7.
The lack of an improvement in the reliability analysis with the addition of the oblique images was somewhat surprising given the literature suggesting that the use of oblique MRIs significantly improved the ability of surgeons to identify foraminal stenosis. Modic et al4 reported on 9 patients undergoing an ACDF at 11 levels, and they found that the oblique MR images correctly identified foraminal compression in 9 of 11 levels (82%). Furthermore, 3 levels had foraminal stenosis that was only evident on the oblique images. In a more recent study comparing the imaging findings to the intraoperative findings of 43 patients undergoing an ACDF, Shim et al8 reported that an oblique MRI had a sensitivity of 96.3% and a specificity of 95.7% for identifying cervical foraminal stenosis. Comparatively, MR imaging with the traditional coronal, sagittal, and axial sequences only had a sensitivity of 40.7% and a specificity of 91.3%.8
While in the current study the addition of oblique MR imaging did not result in an improvement in interobserver or intraobserver reliability in the treatment recommendation for persistent cervical radiculopathy, oblique MR images have proven beneficial to radiologists. In a study in which 2 attending radiologist graded the amount of foraminal stenosis on oblique cervical MR imaging in 50 patients, Park et al reported that the overall interobserver and intraobserver reliability was excellent (κ > .80) for all cervical levels,5 and furthermore, an increase in the grade of foraminal stenosis was moderately correlated with the presence of neurologic symptoms.6 Additionally, the presence of moderate or severe foraminal stenosis (Park grade 2 or 3) was 99.0% specific for the presence of radicular symptoms.6 There are a few possible explanations for the discrepancies between the current study, and the studies by Park et al.5,6 First, the current study involved 6 reviewers, including 3 trainees, whereas the reliability analysis performed by Park et al only involved 2 attending radiologists, both with a minimum of 10 years of experience. Secondly, Park et al reviewed 50 consecutive cervical spine MRIs, and they do not indicate if the MRIs were performed for persistent radiculopathy; however, 70% of the foramen that were evaluated were identified to have no signs of foraminal stenosis. Comparatively in the current study, all patients had severe enough radicular symptoms that they had already elected to undergo an ACDF. The reviewers in this study were not only trying to identify if a level had stenosis, but rather they had to identify the level or levels that were leading to the clinical presentation and would be included in a surgical plan.
Limitations to this study exist, including the retrospective nature of the study. Secondly, the use of oblique MR images is relatively new to our institution, and while all of the reviewers were familiar with the oblique images and how to interpret them, not all routinely used the images in clinical practice. It is possible that a dedicated training module on the use of oblique MR images may have allowed for these images to increase the reliability of the treatment algorithm. Furthermore, the 20 cases included 13 cases in which the patient ultimately underwent a single-level ACDF, and 7 cases in which the patient underwent a 2-level fusion. The decision was made to use a consecutive case series, because the kappa statistic is best used to interpret consecutive case series, as preferentially selecting cases in which an oblique view might be beneficial may artificially inflate the kappa values. However, it is likely that the oblique imaging may be more beneficial in more complex cases in which the patient has some radiographic evidence of stenosis at 3 or 4 levels. So while the current study would indicate that obtaining an MRI on all cervical radiculopathy patients does not improve the reliability, it should not be interpreted that the oblique sequences will not improve reliability in selected patients with unclear foraminal stenosis. Lastly, although the addition of the oblique images resulted in a change in the treatment in almost 50% of the current study, we cannot determine if the alteration in treatment due to the additional information available with the oblique images will result in improved clinical outcomes. However, it is the hope of the authors that this manuscript will encourage future research on the topic.
CONCLUSION
The additional oblique images resulted in an alteration to the surgical plan in almost 50% of cases; however, it had no substantial effect on either the interobserver or intraobserver reliability. Future prospective clinical studies are needed to determine if the addition of oblique images increases the clinical outcomes of patients undergoing an ACDF for cervical radiculopathy.
Footnotes
Disclosures and COI: No funds were received in support of this work. The authors disclose no direct or indirect conflicts of interest in the preparation of this manuscript. No pharmaceutical or medical devices were utilized during this study. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. This included the National Institutes of Health (NIH); Wellcome Trust; Howard Hughes Medical Institute (HHMI). The authors had password-protected access to the data with nonessential patient demographics deidentified.
Ethics Board Review Statement: This study was approved by the Institutional Review Board at Thomas Jefferson University Hospital. Each author certifies that our institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}