


ABSTRACT
Background: Anterior transarticular screw fixation (ATSF) of C1/C2 can be used for the treatment of unstable dens fractures. Here, we evaluated the feasibility of an anterior C1/C2 fixation in elderly patients with unstable dens fractures. Furthermore, we tried to analyze safe entry zones for ATSF surgery.
Methods: A consecutive cohort of 13 patients with unstable dens fractures were treated with ATSF of C1/C2 between January 2015 and October 2016. If necessary, an additional screw was placed into the odontoid process. The placement was radiographically analyzed using the 3D Arcadis Orbic (Siemens, Erlangen, Germany). Additionally, computed tomography scans of the cervical spine from 50 trauma patients were analyzed to evaluate safe entry zones for anterior odontoid screw fixation and for ATSF.
Results: ATSF was performed in 13 cases (7 female, 6 male; mean age 81.80 years). One screw had to be corrected intraoperatively due to initial malplacement. Neurological deficits or an injury of the vertebral artery were not observed. All patients suffered from swallowing difficulties during the postoperative course, without lesions of the esophagus or the trachea. In 4 patients (30.8%), an additional posterior fixation was offered to the patients due to progressive loosening of the screws.
The anatomical-radiographic analyzes revealed a significantly shallower angle of trajectory for anterior odontoid screw fixation (24.9° ± 5.85°) than for ATSF (39.1° ± 6.44° (left); 40.5° ± 6.79° (right) P = 0.02).
Conclusions: The ATSF of C1/C2 might be a valuable option in the treatment of instable C1/C2 fractures, especially in the elderly or in patients with short necks and/or high body mass index due to the steeper trajectory compared with odontoid screw placement. Yet available screws seem to be of inferior resistance compared with the biomechanical properties of a dorsal fixation. Further studies should focus on screws with better mechanical properties and probably additional cement augmentation.
Level of Evidence: 4.
INTRODUCTION
Odontoid fractures contribute to 9% to 15% of all cervical spine injuries in adults1 and are the prevalent type of spine injury in elderly patients.2 According to the Anderson-D'Alonzo classification3 type II fractures are the most common type (65%–74%) of C2 fractures. They account for 38% to 46% in the younger population4,5 and for about 82% to 95% in the older population.6–8 The demographic change in the population leads to a rising number of elderly patients.9 Consequently, this leads to a rising number of patients with fractures of the cervical spine, especially C2 fractures.10 In general, these elderly patients carry more comorbidities that in turn may increase the perioperative risk of a surgical intervention. Not surprisingly, a high morbidity and mortality rate associated with the surgical treatment of odontoid fractures, especially in elderly patients, has been published.11–13
There is a general consensus for the treatment of type I and type III fractures according to the Anderson-D'Alonzo classification. Those fractures should be preferably treated nonoperatively.14,15 However, for type II fractures, this consensus is lacking, and the treatment of these fractures is still a subject of great controversy, especially in elderly patients, despite numerous recent studies. The anterior stabilization of the odontoid process by screw fixation, several posterior fusion methods, or, in particular, the conservative management of dens fractures by external immobilization are accepted treatment options.
The anterior transarticular screw fixation (ATSF) technique, first described by Barbour in 1971, is an alternative technique.16 Lu et al17 adopted this topic and performed an anatomical study for ATSF in 1998. In 2003, Reindl et al18 reported on the technique using a standard Smith–Robinson approach and performed a biomechanical study confirming the effectiveness of this surgical treatment in atlant-oaxial stabilization.19 In 2006, Koller et al20 described a modification of the surgical technique of Lu et al,17 placing the screw entry point underneath the pinafore of C2. Thus, the screw grabs into the bone of the C2, and the stability of the construct was enhanced.20
Our study analyzes the ATSF in regard to feasibility and complication rate in an elderly multimorbid group and compares it with recently published articles regarding this topic. Furthermore, an anatomical analysis of 50 randomized cervical computed tomography (CT) scans from trauma patients was performed to evaluate safe entry zones for ATSF seen in the Appendix.
METHODS
Patients Undergoing ATSF
Between January 2015 and December 2016, 35 patients with an atlantoaxial instability attended our department. Surgery was indicated in 31 cases due to an acute neurological deficit or due the radiographically appearance of the C2 fracture (type II n = 27, type III n = 2, so-called Hangman's fracture n = 2). A conservative management was performed in 4 cases (2 type II fractures and 2 type III fractures).
ATSF was chosen in 13 patients (7 female, 6 male). All patients suffered from a type II fracture. The mean age was 81.80 ± 7.3 years (range 70–91 years). The median American Society of Anesthesiologists (ASA) score was 3.09.21 The main reasons for employing ATSF were either a barrel chest of the patient, making a transodontoid screw placement difficult, or associated fractures requiring extensive stabilization. ATFS was chosen for the assumed lower operative burden for the patient compared with a posterior fixation. A thin-sliced CT scan and a CT angiogram of the craniocervical junction to evaluate the anatomy of the vertebral artery were performed in every case on admission to the department.
Including and Excluding Criteria
Patients with congenital abnormalities of the C1 and C2 with metastatic or rheumatoid disease, fractures of unknown age, or instability of the cervical spine without any fracture were excluded.
Surgery
Patients were placed supine on a radiolucent table. The head was fixed with strips to the table under fluoroscopy control (Arcadis Orbic, Siemens, Erlangen, Germany). A right-sided skin incision at the level of C3–C4, medial to the right sternocleidomastoid muscle, was performed. The dissection of the platysma, parallel to the fiber bundles, and the fascia of the sternocleidomastoid muscle along its medial border was followed by blunt dissection onto the spinal column. The level of C2/C3 was identified. The longicollus muscle was displaced laterally until the transverse process of the vertebral body could be identified. Through a guiding tube, a 1-mm-diameter Kirschner wire (K-wire; Vostra GmbH, Aachen, Germany) was drilled through the transverse process directing toward the apical dorsal aspect of the massa lateralis of C1. The operative angle was 20° to 30° medially on the anteroposterior view and 20° to 30° cephalic on the lateral view, respectively. After advancing the K-wire, the canal was bored with a 3-mm drill, followed by the placement of the screws (4.5 mm/24 mm; DePuy Synthes Deutschland, Umkirch, Germany) guided by the K-wire. Screws were crossing the atlantoaxial joint just anterior to the midline plane. Correct positioning was radiographically assessed using an intraoperative 3D fluoroscopy.
Follow-Up Examination of the Patients
Routine assessment consisted of clinical examination and radiographic evaluation of the fracture healing and assurance of a correct alignment of the fracture and the screws by performing a CT scan 1 day after surgery (Figure 1) and 3 months after surgery. The last clinical examination of the patients was routinely performed 12 months after surgery. Additional follow-up CT scan was performed in cases of newly reported symptoms.

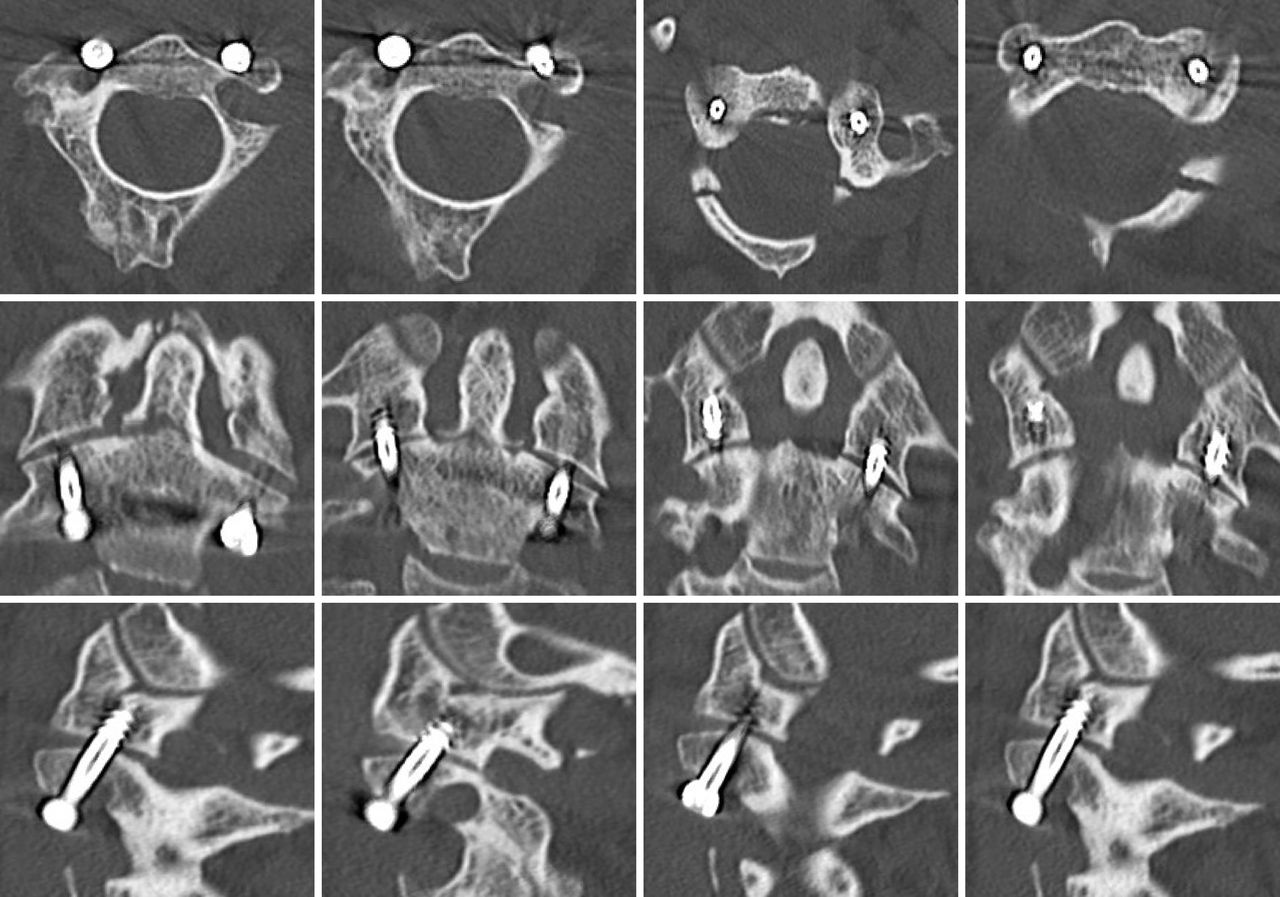
Demonstrating the screw placement of the anterior transarticular screw fixation in a patient suffering from a type II fracture according to the Anderson-D'Alonzo classification.
Statistics
Data were analyzed using SPSS 23.0 (Statistical Package for the Social Sciences, SPSS Inc., Chicago, Illinois) for Windows. For statistical analysis, we performed the Shapiro-Wilk test, the Mann-Whitney U test, and the Kendall tau-b test.
RESULTS
Surgical Results
A thin-sliced CT scan of the cervical spine was performed postoperatively. A good alignment of the fracture and correct screw placement were stated in all patients. In 1 patient, 1 screw had to be repositioned intraoperatively after the 3D fluoroscopy scan. In 1 patient, an additional screw had to be placed laterally, as the initial screw could not be removed because of a damaged tap. In 5 patients, a ventral odontoid screw was placed additionally.
Complications
Neurological examination after surgery revealed no postoperative deficit. However, all patients suffered from swallowing difficulties in the postoperative course without any injury to the esophagus or the trachea. A mild dysphagia according to the score from Bazazs et al22 was observed in 3 patients. A non–ST-segment elevation myocardial infarction was diagnosed during the postoperative course in 2 patients. One patient had to undergo cardiopulmonary resuscitation due to an acute respiratory insufficiency. These events stress out the heavy comorbidities of the patients.
Follow-Up
All patients attended to the follow-up examinations 3 months after surgery. Fracture healing was detected in every case. However, 4 patients complained about newly recognized neck pain 6 to 12 months after surgery. In these cases (4/13, 30.8%), a loosening rim around the screws was diagnosed. Loosening occurred after 9 months on average. A posterior fusion was offered in those cases. One patient refused re-surgery but developed a stable pseudarthrosis 1 year after. One patient died after the first follow-up examination.
DISCUSSION
In atlantoaxial instability, both an anterior and a posterior approach are viable options for stabilization after trauma. Over the past decades, the posterior stabilization techniques of both Grob and Magerl23 and Harms and Melcher24 have been commonly used, combining a high biomechanical stability and a high fusion rate up to 100%.25 Operative techniques employing an anterior approach are anterior odontoid screw fixation or the less commonly used ATSF, first described by Barbour in 1971. The latter seemed to be an effective surgical treatment in atlantoaxial stabilization with similar biomechanical features.16
Sen et al19 published a biomechanical study supporting that ATSF of the atlantoaxial joint is as stable as posterior screw fixation and emphasizing the limited stiffness in flexion-extension movements. Only the dorsal C1/C2 wire cerclage was superior in the movement on the sagittal plane. Lapsiwala et al26 reported similar results in their biomechanical study, showing that anterior and posterior transarticular screw techniques are not significantly different in stiffness unless cable fixation was added to the posterior construct.26 Both Sen et al19 and Lapsiwala et al26 suggested that ATSF is less rigid compared with the surgical techniques from Grob and Magerl23 or Harms and Melcher24 with posterior wiring only in flexion-extension movements. Both Doherty et al7 and Sasso et al28 were able to show that there is no biomechanical difference between the usage of 1 or 2 odontoid screws.
ATSF might bear a couple advantages compared with the posterior approach. The positioning of the patient using a supine position with fixation of the head in extension reduces the risk of spinal cord compression compared with posterior approaches, where the head needs to be fixed in flexion after turning the intubated patient upside down on the operating table. The supine position is preferable in polytrauma patients with sternum or rib fractures, pulmonary contusions, or other injuries or in patients with cardiopulmonary comorbidities. Contrary to the supine position, the prone position alters respiratory dynamics by decreasing respiratory compliance even in nonobese patients.29 Despite the advantages of the positioning, ATSF avoids the risk of trauma to the spinal cord and the C2 roots, and there is no bleeding from the venous plexuses surrounding the vertebral artery or the C2 root. But damage to vertebral arteries, the dural sac, and the spinal cord may be possible due to the trajectory of the K-wire and screws. The anterior approach is less invasive, the duration of the operation is shorter, and the blood loss is less compared with the posterior approaches. Complications associated with anterior approaches are retropharyngeal hematomas, laceration of the pharyngeal and esophageal walls, carotid artery injury, dysphagia, dysphonia, or postoperative problems with airway management.30 Rates of dysphagia after anterior cervical are reported to be up to 60% immediately after surgery and up to 21% after 6 months.31
Ventral stabilization using ATSF with its above-mentioned advantages was chosen in cases of barrel-chested patients, making a transodontoid screw placement somewhat difficult, or in cases of high anesthesiology risks due to severe comorbidities of the patients, seen in the high ASA score. Nevertheless, ventral screw osteosynthesis of the dens with a single screw remains the therapy of choice whenever possible.
Independently of the multiple advantages of ATSF, screw loosening in 4 patients of our cohort shows a nonviable high rate of 30.8%. This rate may be caused by the small number of patients treated, but it still remains an indisputable matter of concern.
A reason for the high rate of screw loosening may be caused by the screws used for stabilization. Different from the screws used for ventral screw osteosynthesis of the dens, the used screws (4.5 mm/24 mm; DePuy Synthes Deutschland) are not self-penetrating. Furthermore, a screw allowing for cement augmentation may be used, leading to better results with respect to long-lasting rigid fixation.
Despite a probable failure of the material, Osti et al32 analyzed failure following ATSF in geriatric patients with type II dens fractures. They were able to show a significant association between failure to heal and age as well as failure to heal and severity of degenerative changes in the atlanto-odontoid joint.
Degenerative changes in the atlanto-odontoid joint have been reported to be 42% in the normal population in the seventh decade and 61% in the eighth decade.33 Similarly, Lakshmanan et al34 found an increased incidence of atlanto-odontoid osteoarthritis in 90% in their geriatric population with type II odontoid fractures and a mean age of 79 years.
There are only a few articles analyzing the success rate of ATSF for different indications. For example, Li et al35 showed in a case series with 8 patients (3 os odontoideum combined with atlantoaxial dislocations, 3 odontoid type II fractures, and 2 atlantoaxial dislocations) good results using the ATSF for younger patients (median age of 41 years). No screw loosening was seen in median follow-up at 16 months.
Polli et al36 also reported a case series with 14 patients (median age of 59.2 years) suffering from Landells type II fracture and atlas transverse ligament disruption, Landells type II + odontoid fracture, and atlas transverse ligament disruption undergoing ATSF with and without odontoid screw placement. They were able to show promising short-term results in patients with atlas fractures after a median follow-up range of 25.9 months.
In addition to those studies, Herren et al37 showed similar results in a case series of 16 patients (8 dens fractures [type II/III] with atlantoaxial dislocation, 8 type II dens fractures with atlas fracture) treated using ATSF. One case of screw loosening was reported after 4 weeks. In 4 cases, penetration of the atlanto-occipital joint was seen. Therefore, complications were seen in 5/16 patients. Follow-up was performed in only 7 cases up to 16 months, showing good results in those patients.37 Josten et al38 recently published a study on the anterior transarticular treatment of 83 patients suffering from an isolated type II dens fracture with a median age of 84.7 years. Forty-seven patients were treated using ATSF and 1 odontoid screw, and 36 patients were treated using ATSF and 2 odontoid screws. The treatment was successful in 65 patients (78.3%); in 15 cases, a screw loosening without clinical relevance was seen, and in 3 cases, a revision surgery (3.6%) had to be performed (2 clinically relevant cases of screw loosening). Compared with the results of Josten et al, our results showed a higher rate of screw loosening (30.8% versus 18.1%). This difference may result from the smaller cohort of patients treated and the different fracture pattern.
In summary, the results of our treatment using ATSF suggest that preoperative selection of the patients (only isolated type II fractures without additional atlas fractures and without signs of severe degenerative changes of the atlanto-odontoid joint) are essential for the postoperative success of this surgical technique. Nevertheless, this technique might be a useful treatment option in elderly multimorbid patients due to shorter operation times and decreased anesthesiology risks and complications. Cement augmentation may be an option to decrease postoperative screw loosening. Furthermore, preoperative evaluation of the level of osteoporosis might be useful to preselect the patients who are suitable for ATSF to increase fusion rates.
The present study has several limitations that must be acknowledged. First, this was a retrospective, nonrandomized study with the associated inherent biases. Only a few patients were evaluated, and the analyzed data were collected from documented electronic records, operative reports, radiological data, and reports of the patients. Furthermore, the follow-up period is relatively short, caused by the retrospective nature of the study and the resulting impracticality of following up on the patients. Therefore, future prospective studies with a longer follow-up are needed to evaluate the success rate of this interesting technique.
CONCLUSIONS
Our data show that the trajectory employed for ATSF of C1/C2 is steeper than for odontoid screw placement, suggesting a more convenient application, especially in patients with short necks and/or high body mass index. However, ATSF seems to have fewer biomechanical properties compared with the dorsal stabilization in cases of C2 fractures but may be an alternative in elderly, multimorbid patients with a high anesthesiologic risk suffering from isolated type II fractures of C2.
APPENDIX EVALUATION OF SAFE ENTRY ZONES FOR ATSF SURGERY
Background
Anterior odontoid screw fixation (AOSF) is an osteosynthetic technique for internal stabilization of unstable odontoid fractures with good fusion rates, low morbidity, and preservation of the atlantoaxial range.39 Finding the screw entry point for screw placement and the trajectory in open surgery might be relatively easy, but using percutaneous approaches, this might be much more challenging without the anatomical landmarks one can use intraoperatively. However, angle of trajectory (AOT) of AOSF is shallower than for anterior transarticular screw fixation (ATSF). Although several reports have described anterior transarticular screw placement techniques,16,18,20,40 there are only a few reports investigating the different trajectories for single16,18,40 or double-facet screws in the literature.20,40–42
Methods To Evaluate Safe Entry Zones
CT scans of the cervical spine from 50 trauma patients (mean age of 51 ± 3 years, range 18–91 years; female n = 20, male n = 30) were analyzed. The images were made by an 18-row multidetector CT scanner (Somatom Definition AS, Siemens Healthcare GmbH) using a rotation time of 500 milliseconds, tube voltage of 100 kV, tube current of 180 mA, and matrix of 512 × 512. Images were reconstructed using a bone window setting (750-HU length, 2300-HU width) into 1-mm-thick slices with a 0.5-mm space between each slice. Afterward, a sagittal, coronal, and axial 3-dimensional reconstruction was performed.
Angulation of the entry trajectories for AOSF and ATSF were assessed as well as bilateral defined distances (Figures A1 and A2) to evaluate safe entry zones for the screws and their passages either into the odontoid process or transarticular through C1/C2.
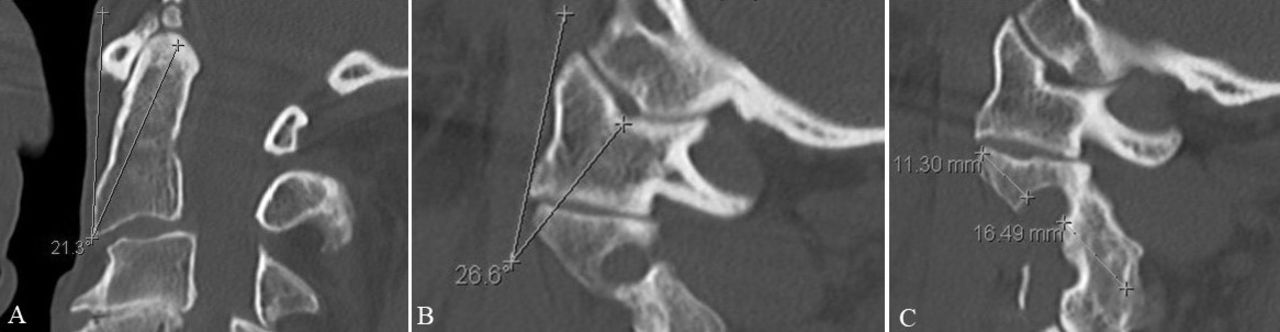
(A) Trajectory for odontoid screw fixation. (B) Trajectory for anterior transarticular screw fixation. (C) Anterior distance from transverse process to vertebral artery and posterior distance from vertebral artery to transverse process.
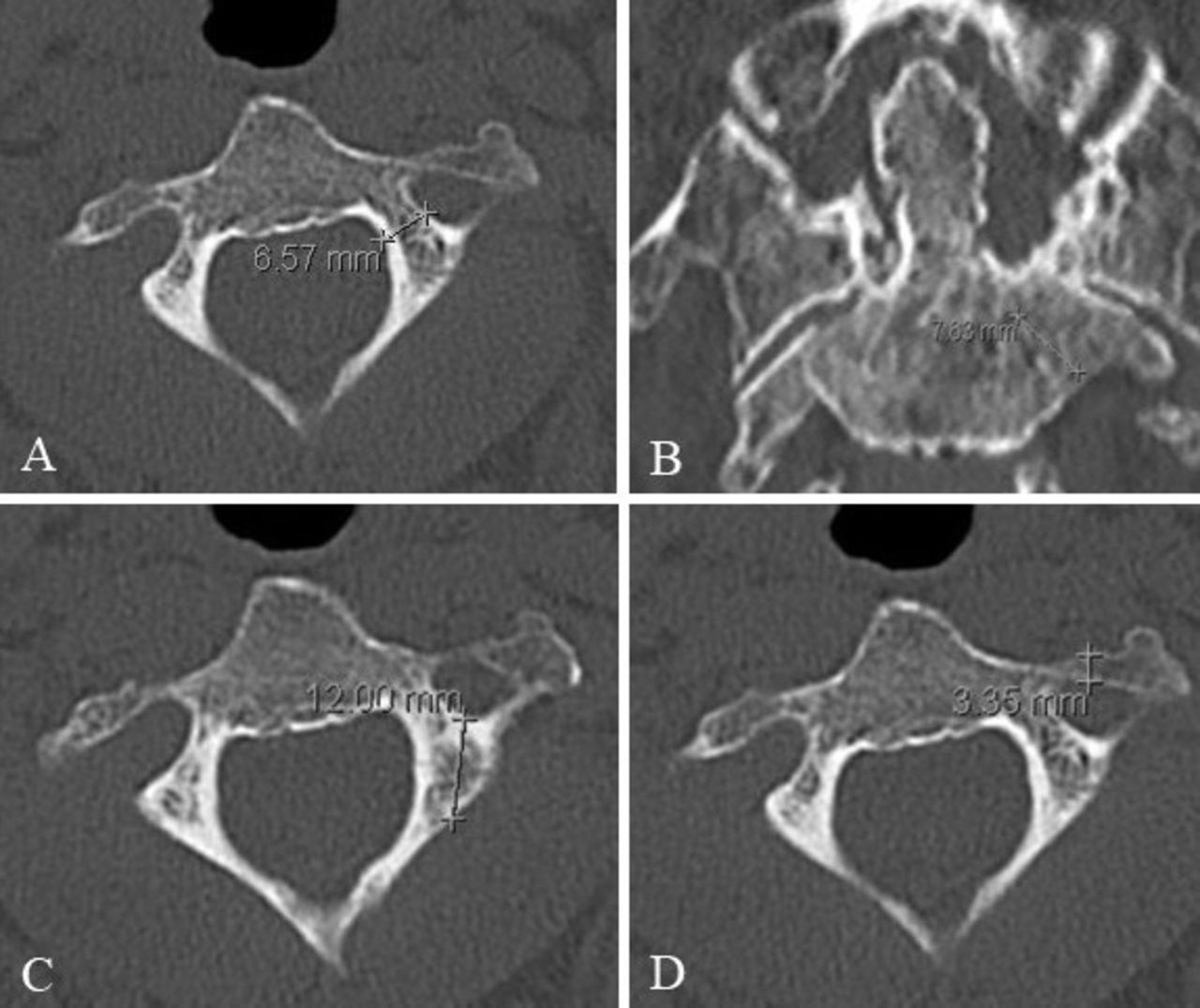
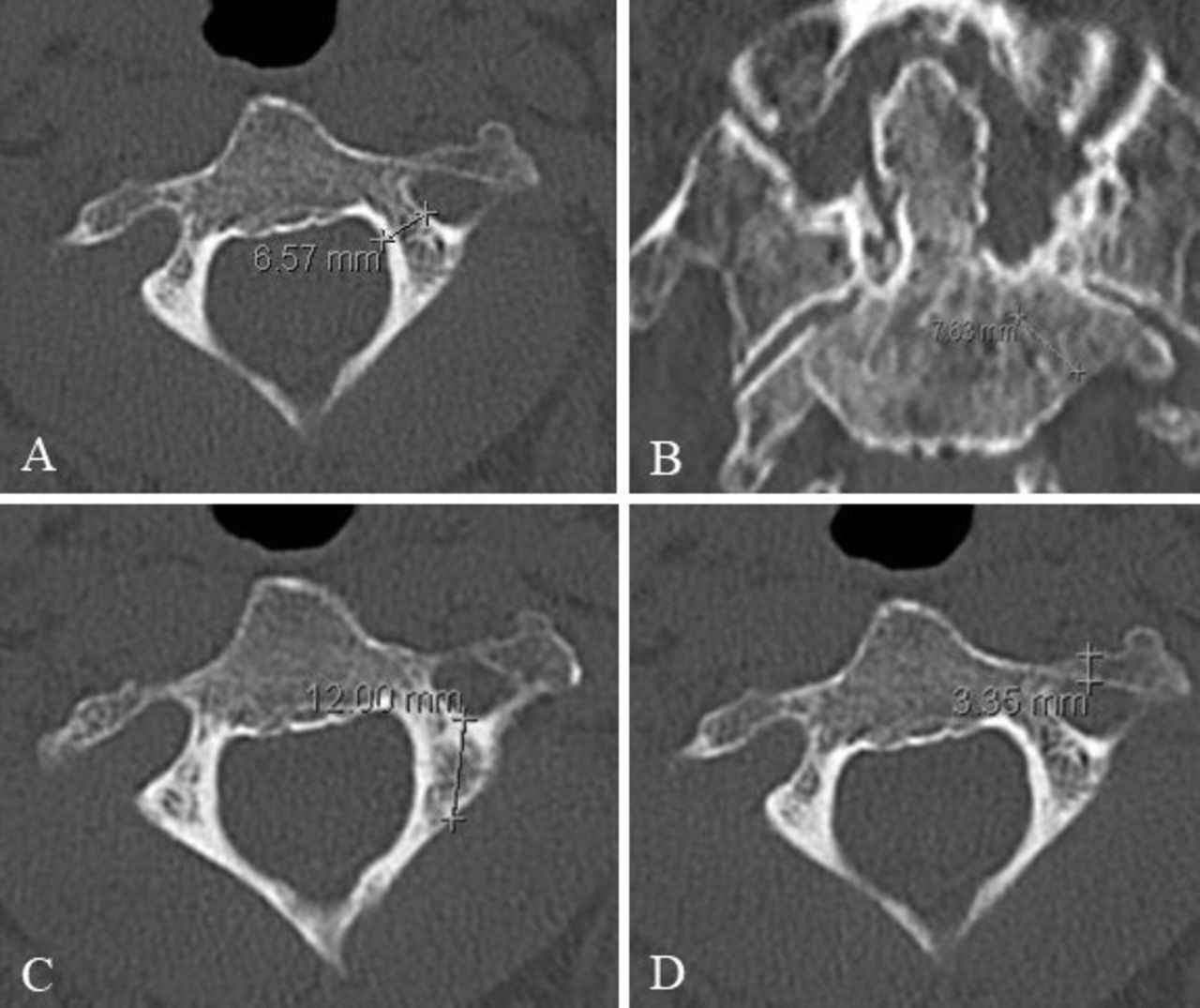
(A) Isthmus C2. (B) Anterior entry zone for placement ATSF. (C) Length of lateral masses. (D) Anterior distance from transverse process to vertebral artery.
Results of Anatomical Analysis
Statistical analysis showed that the AOT for AOSF (24.9° ± 5.85°) is significantly shallower than for ATSF (39.1° ± 6.44° [left] and 40.5° ± 6.79° [right], P = 0.02). Furthermore, in patients >65 years, the AOT for ATSF on both sides was statistically larger than for patients <65 years (42.6° ± 7.55° [left and 44.6° ± 8.08° [right] versus 37.5° ± 5.2° [left] and 38.5 ± −5.1 [right], P = 0.05), whereas the AOT for AOSF was not statistically smaller (26.2° ± 7.2° versus 24.2° ± 5.1° P = 0.29). Besides, there was a statistically significant positive correlation between the age of the patients and the AOT for ATSF (0.24 P = 0.01 [left] and 0.26 P = 0.01 [right]). While the isthmus of C2 was as narrow as 4.1 ± 0.90 mm (left) and 4.2 ± 0.80 mm (right) on average, respectively, the anterior entry zone for screw placement was between 9.7 ± 2.08 mm (left) and 10 ± 2.04 mm (right) with a length of 7.8 ± 1.34 mm (left) and 8 ± 1.43 mm (right) toward the vertebral artery. Length of the lateral masses was approximated with 14.6 ± 1.47 mm (left) and 14.3 ± 1.58 mm (right).
Discussion
However, screw fixation, especially in C1 and C2 fractures, urges for positioning the materials next to vital structures and requires precise adoption of anatomical variation and patterns of bone loss. Safe entry zones and trajectories have been established for the posterior approach.43–45 Trajectories for AOSF and ATSF42 are rarely found in the literature despite the common use of AOSF.
From our data, we could demonstrate that the required angulation of instruments (drill, screwdrivers) for AOSF is significantly shallower than in the approach for ATSF. In patients with a high body mass index, a barrel chest, or a short neck, the latter may be still employed, while AOSF is not feasible due to anatomical conditions.
Conclusions
The safety zones in our series are more favorable for the anterior screw placement with respect to the course of the vertebral artery in comparison with the posterior fixation.
Footnotes
Disclosures and COI: The authors received no funding for this study. The study has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Institutional Review Board (Medical Faculty, University of Duisburg-Essen, Registration number 18-8049-BO). The authors declare that they have no competing interests.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.