


ABSTRACT
Background: Endoscopic techniques are well accepted as surgical technique for decompression of lumbar lateral recess stenosis (LRS). It is uncertain if there is a difference in clinical outcome for decompression alone (DA) or decompression with partial discectomy (DPD) for the treatment of LRS.
Methods: All files of patients who underwent an endoscopic procedure for lumbar LRS were identified from a prospectively collected database. Preoperative magnetic resonance imaging and endoscopic video were analyzed with special focus on the technique of nerve root decompression. Clinical outcome was assessed via a personal examination, a standardized questionnaire including the numeric rating scale (NRS) for leg and back pain, the Oswestry disability index (ODI), and the modified MacNab criteria to assess functional outcome and clinical success.
Results: Sixty-six patients were identified of which 57 attended for evaluation (86.4%). DA was performed in 15 (26.3%) patients and DPD in 42 patients (73.7%). The mean follow-up was 45.0 months (range: 16–82 months). Fifty-two patients reported to be free of leg pain (91.1%), 42 patients had no noticeable back pain (73.7%), 49 patients had full muscle strength (85.9%), and 48 patients had no sensory disturbance (84.2%). The mean NRS for leg pain was 1, the mean NRS for back pain was 2, mean ODI was 16% (range: 0%–60%). Clinical success was noted in 49 patients (85.9%) and it was significantly higher for patients following DPD (P = .024). The overall repeat procedure rate was 12% with reoperation rate at the index segment in 10.5% of cases. There were no significant differences with respect to leg and back pain, ODI, and reoperation between both groups.
Conclusion: Microendoscopic DPD of LRS achieves a 92% clinical success rate which is significantly higher compared to 67% clinical success achieved by DA. There was no significant difference for the rate of reoperation, leg and back pain, and ODI.
Level of Evidence: 4.
- decompression
- discectomy
- endoscopy
- lateral recess stenosis
- lumbar spine
- minimally invasive surgery
- tubular retractor
INTRODUCTION
The degenerative process of the lumbar spine is natural while aging. Degenerative changes of the disc, the facet joint, and the ligamentum flavum are frequently seen in people over the age of 65 years.1 The overall incidence for lumbar spinal stenosis (LSS) in the Western world is up to 5.7%. In asymptomatic subjects over 60 years of age a LSS is seen on the magnetic resonance imaging (MRI) scan in 21%.2 Accordingly, LSS is one of the most common indications for surgery in patients older than 60 years.3
LSS can occur on the central canal, the nerve root canal, or both. The nerve root canal can be divided in 3 regions: the lateral recess, the neuroforamen, and the extraforaminal part. The lateral recess is confined by several anatomical landmarks. The anterior border is formed by the annulus of the disc and the posterior border is formed by the facet joint.4
A stenosis of the lateral recess might be the cause for neurogenic claudication and radicular symptoms such as pain or sensorimotor deficits.5 The underlying pathology might be a hypertrophic facet joint with hypertrophic ligamentum flavum, a disc bulge, a disc protrusion, or a disc herniation. Once conservative treatment has failed to relief symptoms surgery is recommended for patients.6,7 The goal of surgery is to decompress the nerve root beginning from its origin along its course in the lateral recess by preserving spinal stability. A multitude of different surgical techniques have been reported to achieve adequate decompression of the LSS and lumbar lateral recess stenosis (LRS) varying from open to microscopic to tubular endoscopic to shear endoscopic techniques.8–14
Full endoscopic and tubular endoscopic procedures have been developed to reduce approach-related trauma and both techniques have been applied with great success for the treatment of lumbar disc herniation, central canal stenosis, and synovial cyst resection.15–23 Endoscopic techniques are well established for the treatment of degenerative disorders of the lumbar spine.
However, surgical treatment of LRS is controversial and there is no consensus on the answer to the question of whether stand-alone decompression is sufficient. The purpose of the present work was to compare the midterm clinical outcome in patients who underwent endoscopic decompression alone (DA) and endoscopic decompression with partial discectomy (DPD) for LRS.
METHODS
Patient Population and Clinical Evaluation
A prospectively collected database of endoscopic spine procedures was searched for patients who underwent monosegmental decompression of unilateral lumbar lateral recess stenosis.
Inclusion criteria for this study were the following: no previous lumbar spine surgery, a detailed surgical report that described the technique of LRS decompression, a preoperative MRI that confirms the finding of a LRS, complete endoscopic video recording of the procedure, a complete set of preoperative and postoperative evaluations including a detailed neurological examination, and a minimum follow-up of 12 months.
Retrospectively, all patients' files were reviewed with respect to clinical outcome. The video recording was analyzed with special focuses on the surgical technique for decompression (DA versus DPD), the mobility of the dura and exiting nerve root, and the presence of epidural adhesive tissue.
Two groups were created (DA and DPD) and compared with respect to their clinical outcome. A personal neurological examination and a standardized questionnaire were conducted which included the assessment of pain level for leg and back pain, Oswestry disability index (ODI)24 and functional outcome according to modified MacNab criteria.25 Clinical success was defined as excellent and good result according to MacNab criteria (Table 1).
Modified MacNab criteria.
Study design was approved by a local ethical committee (IRB number: 149/17) and patient consent was obtained.
Surgical Technique and Selection Process for DA and DPD
All procedures were performed under general anesthesia. The patient was placed in a prone position and the diseased segment was identified via a spinal tap needle and lateral fluoroscopy. A paramedian skin incision and opening of the fascia was followed by dilation of the paraspinal muscles. An appropriate sized tubular retractor was inserted with a trajectory perpendicular to the lamina and fixed in its position via a holding arm. A high-definition endoscope was then inserted in to the tubular retractor and fixed in its position. From this moment on the entire procedure was performed under continuous endoscopic visualization in bimanual microsurgical fashion.
In all procedures the EasyGO spine system (Karl Storz Company, Tuttlingen, Germany) was used. A detailed account of the surgical technique for endoscopic decompression has been reported in detail elsewhere.17,26,27 Once the exiting nerve root was identified decompression continued towards the neuroforamen until no nerve root compression was evident.
In case of DA, presence of adhesive epidural tissue which would impede a complete mobilization of the nerve root required performing further dissection and resection of adhesive scare tissue. The decompression was sufficient once the nerve root was completely mobile and there was no sign of compression or adhesive tissue circumferential to the nerve root, which was inspected via a nerve hook.
DPD was performed once the surgeon could not easily probe the ventral aspect of the nerve root and once there was still tension on the exiting nerve root. DPD was performed using sharp instruments such as a knife to open the posterior longitudinal ligament. This was followed by resection of the annulus and disc material via grasping forceps.
Preoperative MRI Evaluation
A disc bulge was considered a protrusion of more than 25% of the disc circumference, patients with this finding were allocated to group 1 (see Figure 1). A disc protrusion was defined as when the disc material extends beyond its normal margin and the margin of the vertebra but involves less than 25% of the disc circumference, patients with this finding were allocated to group 2 (see Figures 2 and 3). An extrusion of a disc material was defined as the displaced disc material not being in continuity with the disc space. Patients with mediolateral subligamentous dis herniation were allocated to group 3, and in case of partial extrusion of the disc material they were allocated to group 4 (see Figure 4).28,29

(a) Sagittal T2-weighted magnetic resonance image (MRI) showing a disc bulge (white arrows) at the levels of L3/4 and L4/5. (b) Axial T2-weighted MRI of the segment L3/4 showing a disc bulge (dashed line) with consecutive left-sided lateral recess stenosis and a slight facet joint effusion on the left side (arrowheads).
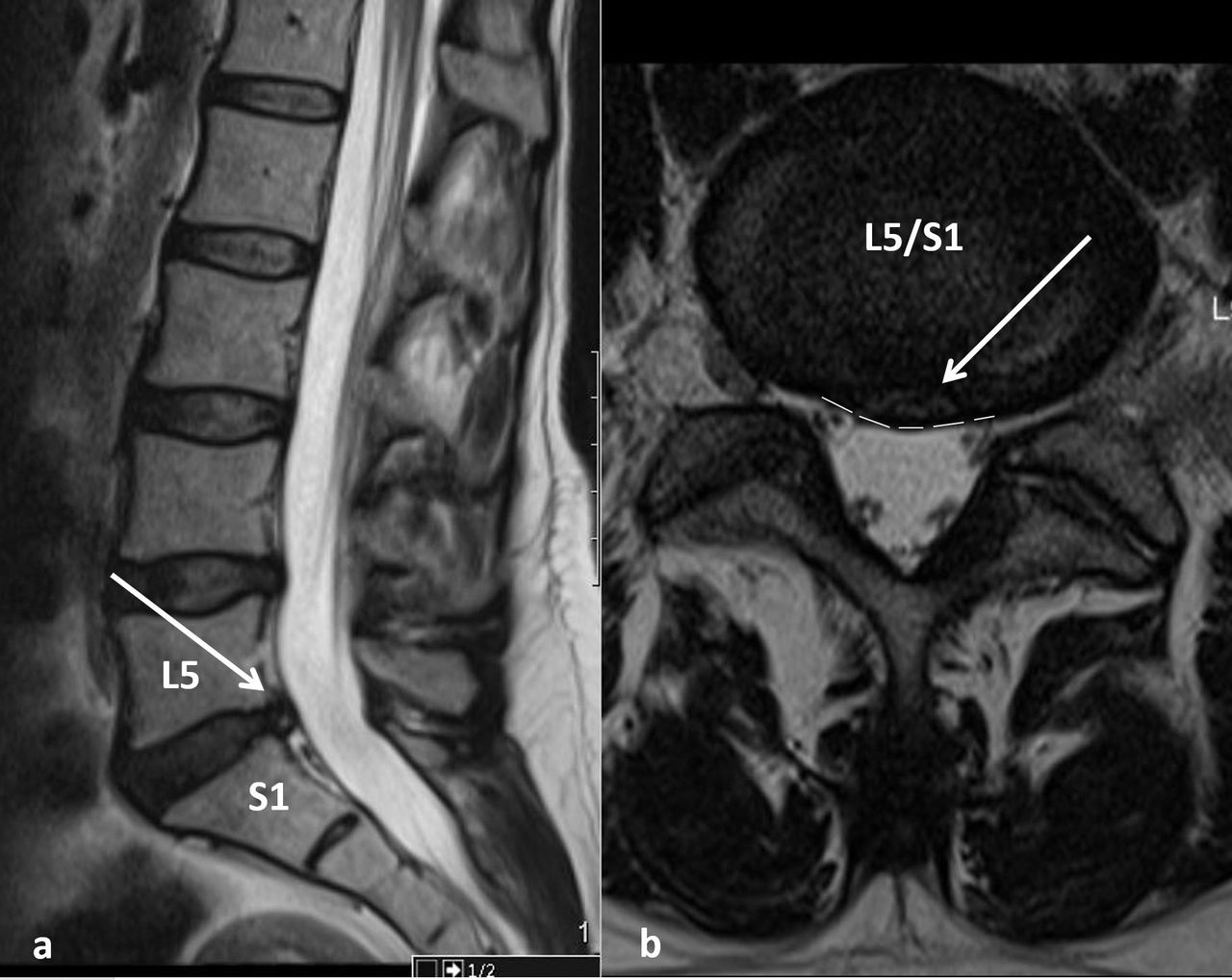
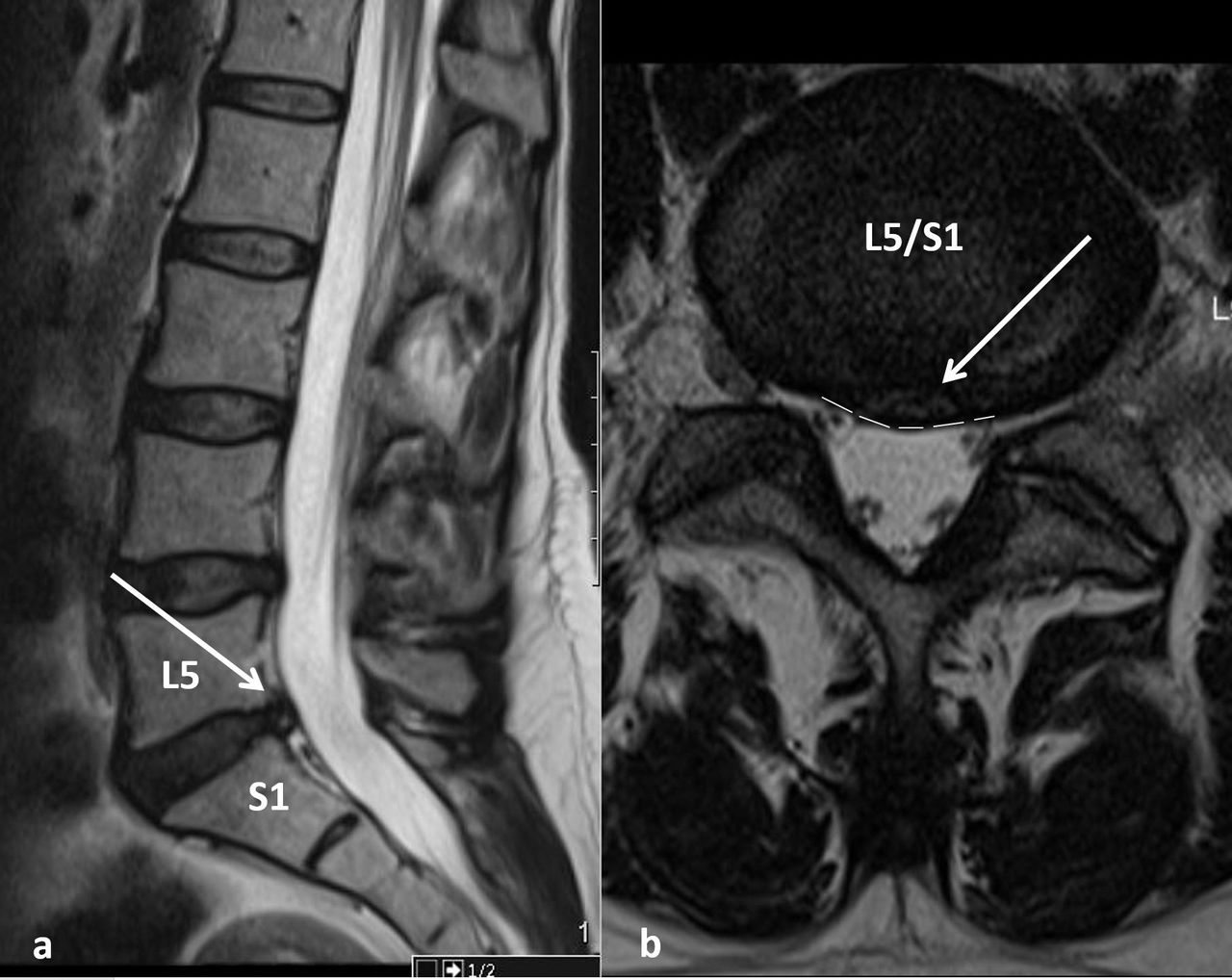
(a) Sagittal T2-weighted magnetic resonance image (MRI)showing a disc protrusion (white arrow) at the level of L5/S1. (b) Axial T2-weighted MRI of the level L5/S1 showing a central (dashed line) disc protrusion (white arrow) with left-sided lateral recess stenosis.

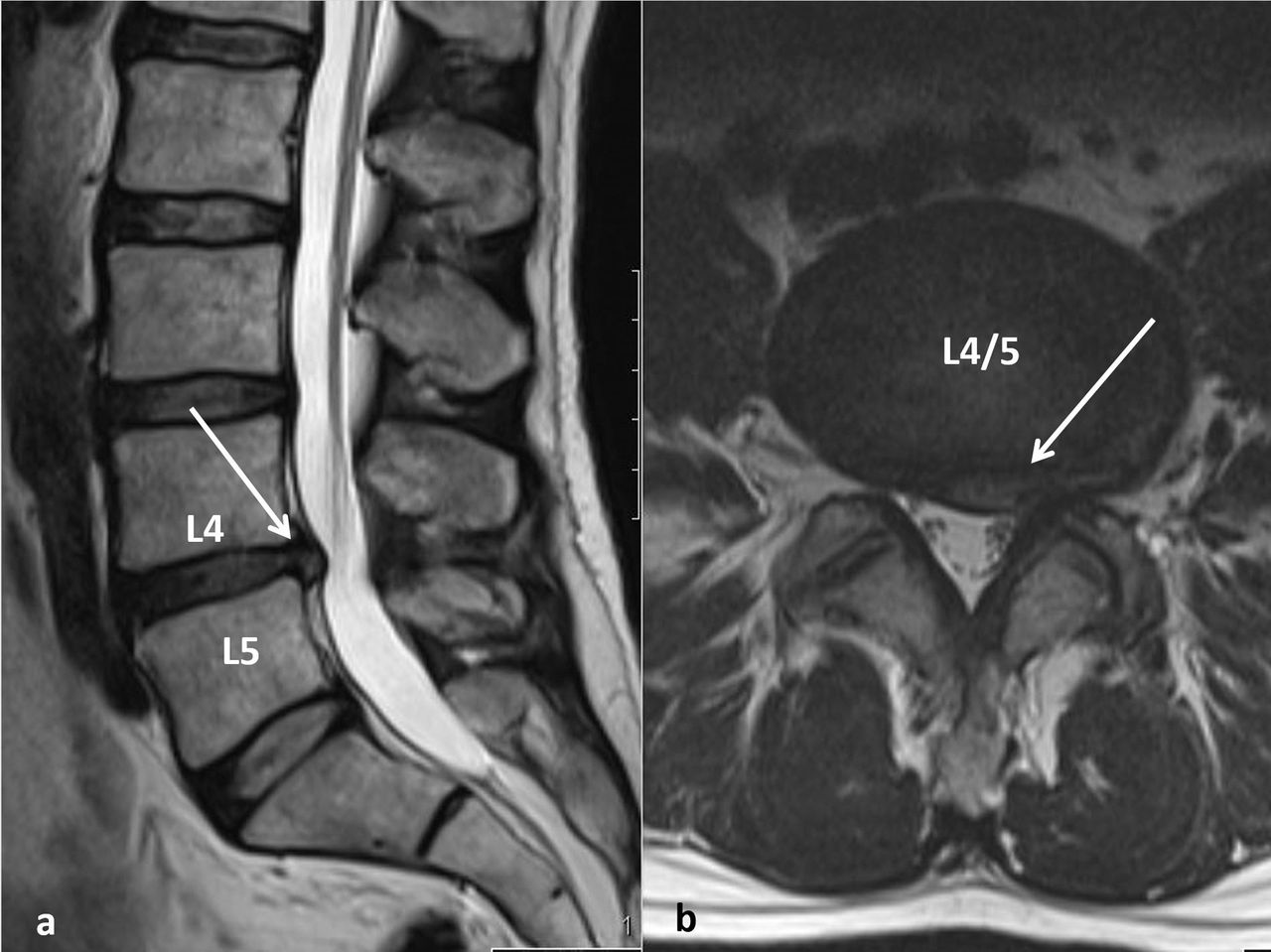
(a) Sagittal T2-weighted magnetic resonance image (MRI) showing a disc protrusion (white arrow) at the level of L4/5. (b) Axial T2-weighted MRI of the level L5/S1 showing a subligamentous mediolateral disc protrusion (white arrow) with left-sided lateral recess stenosis.

(a, c) Sagittal T2-weighted magnetic resonance images (MRIs) showing an extruded disc fragment (white arrow) caudal to the L4/5 disc space. (b, d) Axial T2-weighted MRIs of the level L4/5 showing a hypertrophic ligamentum flavum (white arrow) and a central subligamentous disc protrusion (white arrowhead) with an extruded fragment and left-sided lateral recess stenosis.
Hypertrophy of the facet joint and ligamentum flavum with compression of the dura and nerve root, and facet joint effusion were assessed (see Figures 1 and 4). Furthermore, disc degeneration was assessed graded according to Pfirrmann et al.30
Statistical Methods
The SPSS statistical software package (SPSS version 25, IBM, Chicago, Illinois) was used for statistical analysis of the data. Two groups were created according to the performed surgical technique (DA and DPD) and clinical outcome, as well as repeated procedures, were compared.
We used 2-sided Fisher exact test to compare relative frequencies of a binary outcome between 2 independent groups. A Wilcoxon test was used to compare nonparametric paired sample tests. Any P values given were 2-sided; P < .05 was assumed to be sufficient to indicate statistical significance.
RESULTS
Patient Characteristics and Intraoperative Findings
Between 2011 and 2017, 66 patients (42 male and 24 female) who met the inclusion criteria were identified from the database. The mean age at endoscopic procedure was 56.2 years (range: 33–82 years).
One patient underwent surgery at L2/3, 4 patients at L3/4, 32 patients at L4/5, and 29 patients at L5/S1. The mean duration of symptoms prior to endoscopic procedure was 19 months (range: 1–240 months). Four patients reported to have symptoms since more than 10 years. Fifty-five procedures were performed using a 19-mm tubular retractor and 11 procedures were performed using a 15-mm tubular retractor. A total of 4 different surgeons were involved the procedures. Three among those were trained by the senior author of the manuscript, who has performed the majority of cases. Each surgeon had substantial (>1000 procedures) experience in microsurgical lumbar spine surgery.
Intraoperatively in one case a switch from a 15-mm to a 19-mm tubular retractor was performed due to limited instrument angulation caused by obesity. In 60 cases adhesive epidural tissue that limited the mobility of the exiting nerve root and thecal sac was identified intraoperatively.
In 20 cases DA was performed and in 46 cases DPD was performed; a detailed compilation of the 2 groups with respect to patient characteristics, MRI findings, and clinical outcome is shown on Table 2.
Patient characteristics, MRI findings, and clinical outcome.
There was no conversion to open surgery and no technical complication occurred with the endoscopic system. The mean surgical time was 61 minutes (range: 25–129 minutes). An incidental dural tear was noted in seven cases (10.6%). In all cases the dural tear was repaired using an autologous muscle graft and a fibrin-sealed collagen sponge and all patients were mobilized on the day of surgery.31
Clinical Findings: Preoperative, Postoperative, and Final Follow-Up
Preoperative
The primary indication for surgical treatment was failure of conservative treatment for radiculopathy, which was the cause for restricted quality of life.
Fifty-six patients had radicular leg pain (84.8%), the mean pain intensity was 6 on the numeric rating scale (NRS; range: 1–10). In 34 patients a paresis (51.5%) was documented. Fifty-four patients had back pain (81.8%) with a mean intensity of 6 on the NRS (range: 2–10) and among those 4 patients had a history of chronic back pain (more than 10 years). The mean ODI was 24.2% (range: 0%–46%).
The degree of paresis was 4/5 in 17 patients, 3/5 in 15 patients, and 2/5 in 2 patients. In 25 patients a sensory deficit (37.8%) was noted.
Postoperative
All patients were mobilized at the day of surgery. The median hospitalization was 4 days. At discharge 28 patients reported to be free of leg pain (42.4%), 37 patients reported an improvement of their leg pain (56.1%), and 1 patient reported a worsening of his preoperative leg pain. The mean leg pain intensity improved to 1.4 (range: 0–8) on the NRS. Forty-two patients reported an improvement of back pain (63.6%), while 22 patients reported to be free of back pain (33.3%), and 2 patient reported unchanged back pain. The mean back pain intensity on the NRS was 1.8 (range: 0–9), and mean ODI improved to 10.2% (range: 0%–36%).
At discharge, in 45 patients full motor strength (68.2%) was documented, in 19 patients an improvement of motor strength was noted (28.8%), and in 2 patients no improvement was noted (3.0%).
No postoperative wound healing problems or wound infection were noted. None of the 7 patients with intraoperative dural tear reported any kind of discomfort which could be related to the cerebrospinal fluid leak or development of a pseudomeningocele.
Final Follow-Up
The mean follow-up was 45.0 months (range: 16–86 months) at which 57 patients (86.4% follow-up rate) were evaluated. Nine patients (13.6%) were lost to final follow-up evaluation. Two patients died due to causes unrelated to endoscopic procedure 11 and 26 months after the procedure. Seven patients could not be reached by telephone.
Fifty-two patients reported to be free of leg pain (91.1%); the mean leg pain intensity on the NRS was 0.9 (range: 0–7). Forty-two patients reported to be free noticeable back pain (73.7%); the mean back pain intensity was 2.0 (range: 0–8), and the mean ODI was 16% (range: 0%–60%). Forty-nine patients had full muscle strength (85.9%), and 48 patients reported to have no sensory disturbance (84.2%).
According to the MacNab criteria 49 patients had excellent or good results (85.9%) and 50 patients reported to have no limitation in their daily activity (87.7%). Forty-four patients reported to participate in sports activity regularly (77.2%); 4 patients reported the daily intake of pain medication (7.0%).
Repeat Procedure
In 7 cases (12.2%) a repeat procedure was performed. Those procedures were related to either recurrent disc herniation or progress of degenerative changes with delayed instability in 1 case (1.7%).
One patient underwent transforaminal lumbar interbody fusion (TLIF) due to the increased mechanical low back pain 6 months after initial endoscopic procedure
One patient developed radicular pain on the contralateral side and decompression was performed at the same level for LRS 3 years after the initial procedure.
One patient underwent microsurgical decompression of central LSS in the adjacent segment 16 months after the initial procedure.
One patient developed radicular pain caused by a disc herniation at the previously decompressed (DA) level and underwent endoscopic discectomy 2 years after the initial procedure.
One patient underwent a percutaneous endoscopic lumbar discectomy for resection of a recurrent extraforaminal disc herniation 6 years after the initial procedure.
One patient underwent microsurgical resection of a recurrent disc herniation 11 months after the initial procedure.
One patient underwent microsurgical resection of a recurrent disc herniation 4 months after the initial procedure.
Preoperative MRI Evaluation
According to the preoperative MRI scan 16 patients were assigned to group 1, 19 patients were assigned to group 2, 14 patients were assigned to group 3, and 17 patients were assigned to group 4. Hypertrophy of the facet joint with compression of the spinal canal and dura was noted in 45 cases. Facet joint effusion on the affected side was noted in 14 patients.
Disc degeneration of grade 2 according to Pfirrmann et al30 was noted in 2 patients, of grade 3 in 9 patients, of grade 4 in 39 patients, and of grade 5 in 16 patients.
The rate of clinical success according to MacNab in group 1 was 73%, in group 2 it was 79%, and in groups 3 and 4 it was 100%.
Statistical Analysis
Postoperative results were as follows:
Mean leg pain intensity was 1.3 in the DPD and 1.6 in the DA group, which was not significantly different (P = .483).
Mean back pain intensity was 1.7 in the DPD and 1.6 in the DA group, which was not significantly different (P = .400).
Mean ODI was 20.2 in the DPD and 17.8 in the DA group, which was not significantly different (P = .480).
Final follow-up results were as follows:
Mean leg pain intensity was 0.7 in the DPD and 1.3 in the DA group, which was not significantly different (P = .118).
Mean back pain intensity was 1.5 in the DPD and 2.6 in the DA group, which was not significantly different (P = .115).
Mean ODI was 16.0 in the DPD and 20.0 in the DA group, which was not significantly different (P = .258).
The clinical success rate was 92% in the DPD group and 67% in the DA group, which was not significantly different (Fisher exact test, P = .024).
There was no statistically significant difference in the rate of repeated procedure between the DPD and DA groups (Fisher exact test, P = .365).
DISCUSSION
LSS is a disorder that emerges at the end of a natural degenerative process. The degeneration of the disc with loss of disc height, consecutive hypertrophy of the facet joints, and thickening of the ligamentum flavum are frequently observed on patients over the age of 65 years.32 The nerve root passes the lateral recess and any degenerative disorder such as disc bulge, disc protrusion, disc herniation, facet joint hypertrophy, synovial facet joint, or hypertrophy of the ligamentum flavum can cause as stenosis of the lateral recess and a compression of the nerve root.32–34 In the past decades, spine surgeons had the ambition to get a better understanding of how to perform decompression of lumbar canal stenosis and satisfactory results for various surgical techniques have been reported.20,35–38 Even though the actual technique for decompression might have a limited influence on the long-term clinical outcome, there are 2 aspects which have become a focus for decompression of LSS and LRS.
These aspects are the surgical approach and the amount of facet joint resection. Minimally invasive techniques have been developed to preserve the posterior elements with the approach and reduce trauma to muscle and soft tissue. This results in lower levels of systemic inflammatory parameters, lower postoperative pain levels requiring less intake of analgesics, earlier mobilization, and faster return to work.15,16,19,39–45 Basically there are 2 different endoscopic techniques, the so-called “full endoscopic” technique, which is performed under continuous irrigation in single-handed fashion using special instruments,46,47 and the tubular-assisted “microendoscopic” technique, which is performed in bimanual fashion using standard microsurgical instruments.15,48 The spectrum of indications for full endoscopic techniques has enlarged from discectomy towards the treatment of LSS and LRS due to technical advancements in optics, instruments, and drills, and this particular surgery might be performed via a contralateral, interlaminar, or transforaminal approach.8,9,47,49,50 A significant reduction in leg pain as well as clinical success rates ranging from 75.0% to 92.3% depending on the approach and the event of previous surgery have been reported for full endoscopic procedures.8–11,22,47,49–60
However, one major concern regarding the full endoscopic technique is the prolonged learning curve and the limited option to manage intraoperative complication such as dural tears or dissection of adhesive epidural tissue.49,61–63 In contrast to the full endoscopic technique the microendoscopic decompression of LRS is solely performed via an interlaminar approach. The application of microsurgical instruments allows for decompression of the nerve root, dissection of adhesive epidural tissue, and partial discectomy, if necessary. A very steep learning curve has been reported for the microendoscopic technique, which has been used in the present study.64 However, with the microendoscopic technique, endoscopic dural repair can be performed without conversion to open surgery and the number of procedures to reach the asymptote is smaller compared to full endoscopic techniques.26,64,65 The interlaminar approach risks harming the facet joints. To prevent the progression of postoperative spinal instability and achieve successful clinical outcome it is recommended to preserve the facet joints as much as possible.66–68 It has been reported that preservation of the ipsilateral facet joints is difficult to achieve via a unilateral approach. A reduction rate of facet size from 6% to 22.6% has been reported.40,69,70 Therefore some authors recommend performing a contralateral approach for decompression of LRS. Several advantages have been stated, such as sparing of the facet joint, better visualization of the neuroforamen, and undercutting of the contralateral ligamentum flavum and superior articular process.9,58,71,72
Even though no postoperative computed tomography or MRI scan was performed regularly in the present study the review of the endoscopic video material revealed that resection of the medial third up to two-thirds of the facet joint was indeed performed to perform adequate decompression. Some authors believe that ipsilateral decompression and resection of the facet joint might accelerate the spinal deformity and leads to instability.70,73 In the present series there was 1 patient with a long history of chronic low back pain (1.7%) who underwent a TLIF procedure due to increased mechanical low back pain. It should be stated that the DA in this patients was performed due to the onset of a foot-drop paresis and that this patient initially refused to undergo the TLIF procedure. In addition of all the aforementioned approach-related advantages, the authors also would like mention some limitations. At first the dissection and resection of adhesive epidural tissue, which is often located ventrolateral to the origin of the nerve root and the underlying disc space, is limited via a contralateral and transforaminal approach. Furthermore, the feasibility to perform a partial discectomy and to dissect the dura and the exiting nerve root of the osseous structures and the disc space is limited. Finally, the distance from the skin level to the lateral recess via a contralateral approach is longer compared to the ipsilateral approach and therefore the instrument handling might be limited, especially if it comes to difficult steps of the procedure such as dissection of scar tissue and repair or closure of a dural tear.
The rate of clinical success following contralateral approach has been reported to vary from 92% to 95% within a mean follow-up of about 13 months58,71; a success rate of 92% has been reported for an ipsilateral transforaminal approach with a mean follow-up of 34 months,74 which is higher compared to the overall clinical success of 86.6% of the present study. However, the follow-up of the present study was longer compared to the aforementioned studies.
The number of studies which assessed the clinical outcome after tubular or endoscopic decompression of LRS is limited. The ODI of the present study (ie 16%) is in range of the ODI values reported in the literature review: 10% to 25%. This indicates that partial resection of the ipsilateral facet joint via a tubular approach has no significant influence on the ODI at follow-up.
It has been reported that stand-alone decompression is effective for the treatment of LRS caused by calcified disc herniation. The rate of clinical success has been reported to be up to 90.9% with 5 years of follow-up and none of the patients with stand-alone decompression required a revision procedure.75 This success rate is considerably higher compared to the rate of 66.7% in the present study. In contrast, in the present study 92% of patients who underwent decompression and partial discectomy reported clinical success according to MacNab criteria. However, other patient-reported outcome parameters such as leg pain, back pain, and ODI did not show a statistically significant difference.
Furthermore, it is difficult to identify which aspect might have caused this difference in clinical outcome. In the authors' experience sufficient decompression of the nerve root is the key for clinical success. In the present series the mean duration of clinical symptoms was 19 months. The presence of epidural adhesive tissue with consecutive fixation of the nerve root is frequently observed in patients with a long duration of preoperative symptoms. The origin of this tissue is mainly caused by the resorption process of disc fragments or disc protrusion. The endoscopic visualization allows for ideal illumination of the surgical field as well as identification and differentiation of the dura, the disc, and adhesive tissue.27 In cases with previously diagnosed subligamentous disc protrusion it might be difficult to sufficiently decompress and mobilize the nerve root via decompression alone. In those cases, partial discectomy was performed to completely release the dura and the origin of the nerve root at the level of the disc space. If necessary, this dissection should be continued into the neuroforamen. Some spinal surgeons might argue that such aggressive decompression might result in acceleration of spinal instability or recurrent disc herniation and an increased repeated procedure rate. The MRI evaluation revealed that 83% of discs showed progressive degeneration prior to endoscopic procedure, which might have an impact on the development of recurrent disc herniation as well. Three among those patients who underwent DPD required a revision procedure for recurrent disc herniation (6.8%) and none of those patients developed mechanical low back pain. Therefore, the authors believe that it is worth performing extensive decompression and mobilization of the nerve root including a partial discectomy if necessary.
Limitations
There are limitations to this study which necessitate discussion. It is not possible to control the subtleties of surgeon-driven patient selection and intraoperative technique. It has been reported that based on MRI assessment studies the foraminal area and foraminal diameter significantly changes from supine to upright position.76 It is therefore conceivable that nerve root compression might change in prone position, which could influence the intraoperative decision process for performing DPD or DA alone. All surgeons involved in the present study had substantial experience in microsurgical lumbar spine surgery and all were trained at the senior author's institution. We assume that the bias of surgical experience had minimal influence on the results of the present study. However, there is no reliable score to objectively evaluate the mobility of the nerve root and amount of nerve root decompression that can be applied intraoperatively. Therefore, each surgeon might assess the mobility of the nerve root, which is the key factor in this study, slightly differently. In addition to these potential confounders there was also observed variability in follow-up times for each patient. The results demonstrated that ODI increased over time, as well as intensity of leg and back pain changes. In order to overcome some of these limitations, further prospective and potentially randomized studies with a larger cohort will be needed.
CONCLUSION
The results of the present study demonstrate that endoscopic decompression of LRS is a safe technique and offers a high rate of clinical success. DPD achieves a clinical success rate of up to 92%. In the present series of patients, the rate of recurrent disc herniation was 6.8% and the rate of delayed spinal instability was 1.7% within 45 months.
Footnotes
Disclosures and COI: The authors declare that they have no conflict of interest. J. Oertel acts as a consultant for the Karl Storz company.This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
- 1 .↵
- 2 .↵
- 3 .↵
- 4 .↵
- 5 .↵
- 6 .↵
- 7 .↵
- 8 .↵
- 9 .↵
- 10 .
- 11 .↵
- 12 .
- 13 .
- 14 .↵
- 15 .↵
- 16 .↵
- 17 .↵
- 18 .
- 19 .↵
- 20 .↵
- 21 .
- 22 .↵
- 23 .↵
- 24 .↵
- 25 .↵
- 26 .↵
- 27 .↵
- 28 .↵
- 29 .↵
- 30 .↵
- 31 .↵
- 32 .↵
- 33 .
- 34 .↵
- 35 .↵
- 36 .
- 37 .
- 38 .↵
- 39 .↵
- 40 .↵
- 41 .
- 42 .
- 43 .
- 44 .
- 45 .↵
- 46 .↵
- 47 .↵
- 48 .↵
- 49 .↵
- 50 .↵
- 51 .
- 52 .
- 53 .
- 54 .
- 55 .
- 56 .
- 57 .
- 58 .↵
- 59 .
- 60 .↵
- 61 .↵
- 62 .
- 63 .↵
- 64 .↵
- 65 .↵
- 66 .↵
- 67 .
- 68 .↵
- 69 .↵
- 70 .↵
- 71 .↵
- 72 .↵
- 73 .↵
- 74 .↵
- 75 .↵
- 76 .↵
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.