


ABSTRACT
Background: Cervical laminoplasty is an established and effective surgical treatment for neurologic dysfunction associated with cervical myelopathy. “Dome laminotomies” involve undercutting the laminae adjacent to the laminoplasty levels to decompress and prevent spinal cord kinking on the lamina edges. The technique allows for a decrease in the number of instrumented laminae, smaller surgical exposure, and preservation of muscular attachments at the top of C2 and C7. We investigated whether dome laminotomies are associated with satisfactory neurologic and pain outcome.
Methods: This study involved a retrospective review of consecutive patients treated at a single institution between November 2015 and September 2018. The patients underwent a C3–C6 laminoplasty with dome laminotomies of the caudal edge of C2 and the cranial edge of C7 lamina. Postoperative evaluations of pain, myelopathy symptoms, and complications occurred at early (mean, ∼2 months) and late (mean, ∼15 months) time points.
Results: Twenty-one patients were enrolled (mean age, 62 years). Mean axial pain score improved significantly at both the early (P = .02) and late (P = .045) postoperative evaluations compared with the mean baseline pain score. A total of 92% of patients experienced resolution of baseline hand dysfunction at the early postoperative follow-up, and 84% maintained it at the late follow-up. Two-thirds of patients experienced (late) significant improvement (P < 0.05) in baseline balance impairment. Postoperative response rates for urinary dysfunction were 58% (early) and 42% (late). There were no wound complications, late neurologic deterioration, kyphosis, or C5 palsy.
Conclusions: C3–C6 laminoplasty with C2 and C7 dome laminotomies was safe, well tolerated, and associated with satisfactory early and late improved neurologic function and decreased pain.
INTRODUCTION
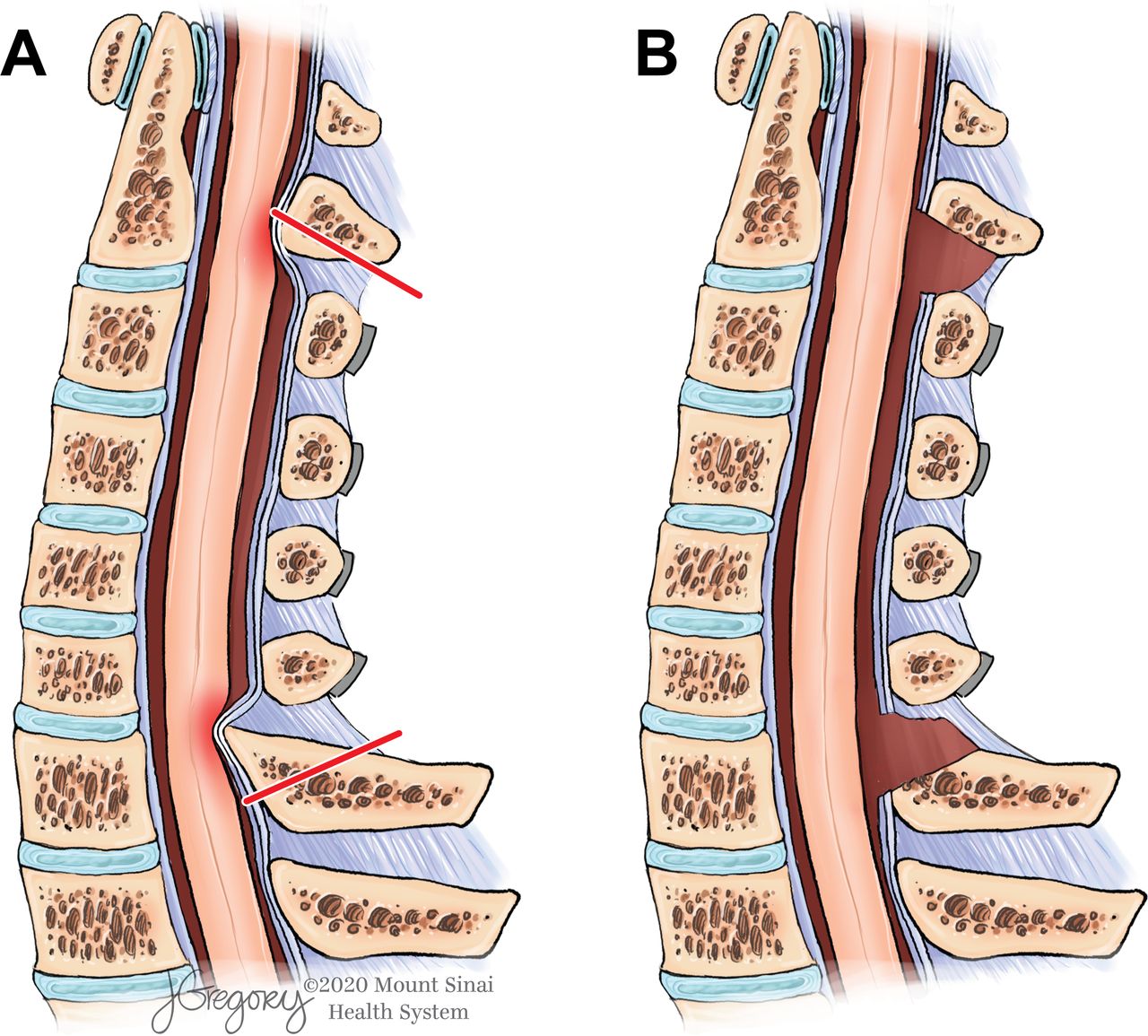
Cervical spondylotic myelopathy causes decreased hand dexterity, urinary dysfunction, and/or gait instability.1 Cervical laminoplasty is a common neurosurgical technique for the treatment of cervical stenosis causing cervical spondylotic myelopathy.2 Limiting the laminoplasty levels by not including the C2 and C7 shortens the operative time, decreases operative exposure, and preserves important muscle attachments.3 It has been described to undercut the C2 and C7 laminae to limit the laminoplasty levels and avoid inadequate decompression.4,5 The purpose of the dome laminectomy is to directly decompress and prevent static or dynamic kinking of the spinal cord after its expected, postdecompression dorsal migration (Figure 1). We undertook to evaluate whether the technique of performing dome laminotomies at adjacent segments is associated with satisfactory neurologic outcomes and decreased postoperative pain.

(A) A sagittal, midline view of the cervical spine following a C3–C6 laminoplasty without dome laminotomies. The dorsal migration of the spinal cord following the decompressive effect of the laminoplasty at the C3–C6 levels leads to kinking and compression (red-shaded areas) of the spinal cord by the caudal edge of the C2 lamina and the cranial edge of the C7 lamina. The kinking can be static and/or dynamic. Adding C2 and C7 laminotomies, defined by the red lines, leads to an improved decompression, which is depicted in panel B. (B) The additional decompression afforded by the dome laminotomies prevents any spinal cord kinking. Illustration by Jill K. Gregory, used with permission of ©Mount Sinai Health System.
METHODS
Patients
The study examined consecutive patients who underwent a C3–C6 laminoplasty with dome laminotomies at C2 and C7. Dome laminotomy is defined as the undercutting (bilateral laminotomies, more extensive on the ventral aspect of the laminae) of the caudal (or “trailing”) edge of C2, or the cranial (or “leading”) edge of C7 laminae. The patients were operated on by the senior author at a single institution between November 2015 and September 2018. The study was approved by the institution's Investigational Review Board, and waiver of the consent process was obtained.
Indications for Surgery
The indications for surgery were cervical myelopathy with/without radiculopathy due to cervical stenosis or mild forms of ossification of posterior longitudinal ligament that respected the K-line rule.6 The presence of baseline cervical kyphosis >13° on standing lateral X-ray, spondylolisthesis between C2 and C7 (defined as >2 mm of anterolisthesis) on neutral lateral X-ray, or the presence of cervical instability in any cervical level was a contraindication. The instability was defined as dynamic sagittal plane translation of more than 3.5 mm, or sagittal plane rotation of more than 20° on flexion-extension X-rays.7 The presence of severe pain (more than numeric rating scale 8/10) was a contraindication, unless this was felt to be related to upper cervical radiculopathy, which can be addressed with foraminotomies.
Parameters
The main outcome measures were neck pain (numeric rating scale) and neurologic outcome. The neurologic outcome was assessed qualitatively by patient-reported changes in the severity of functional impairment domains of cervical myelopathy: hand dexterity/balance/urinary dysfunction. Hand dysfunction and balance impairment (including gait instability) were graded by patient subjective report only, and they were characterized as absent, stable, improved, or worsened at the measured study time points. Urinary dysfunction included urinary symptoms associated with neurogenic bladder, and in women, urinary frequency that did not require catheterization. The secondary outcomes were surgery-related complications and the development of cervical deformity or instability on postoperative imaging. The data were collected retrospectively. Descriptive statistics were used and comparisons were made using unpaired Student t-test and Fisher exact test and a prespecified cutoff level for significance of P < .05.
Surgical Technique
The operative technique is standardized as follows. Standard endotracheal intubation and induction of general anesthesia was performed while maintaining spinal precautions. Baseline motor evoked potentials, somatosensory evoked potentials, and electromyography recordings were obtained. Gardner-Wells tongs were applied. The patient was positioned prone on the Jackson table with a foamy face mask under the face, which was supported on a rigid, radiolucent head frame. Neuromonitoring was repeated after flipping the patient, and then after applying 10 lb of traction. A lateral X-ray was obtained for incision localization. We exposed the spinous process and lamina of C3 down to C6 as well as the caudal edge of the C2 spinous process and lamina, and the cranial edge of the C7 spinous process and lamina. The exposure was extended laterally to the junction of the lamina and lateral mass on the “hinge” side of the laminoplasty. On the opening side of the laminoplasty, the exposure was extended to the lateral one third of the lateral masses while preserving the facet capsules. The opening trough was done on the side that was more symptomatic, given that a more extensive decompression of the spinal canal was achieved on the side of the opening trough. In cases in which the symptoms were equal in severity on both sides, we selected the dominant hand side for the opening trough. A 3-mm matchstick drill bit was then used to drill the cranial edge of the C7 lamina and base of the C7 spinous process. We then drilled a full-thickness trough at the junction of the lamina and lateral mass on the opening trough side. Foraminotomies were performed at this phase if they were indicated. We then drilled on the caudal edge of the C2 lamina and base of the C2 spinous process. We then performed a partial-thickness trough at the junction of the laminae and lateral masses on the hinge side. A small upgoing curette was used to release the ligamentum flavum connecting the undersurface of the laminae to the lateral masses on the open trough side.
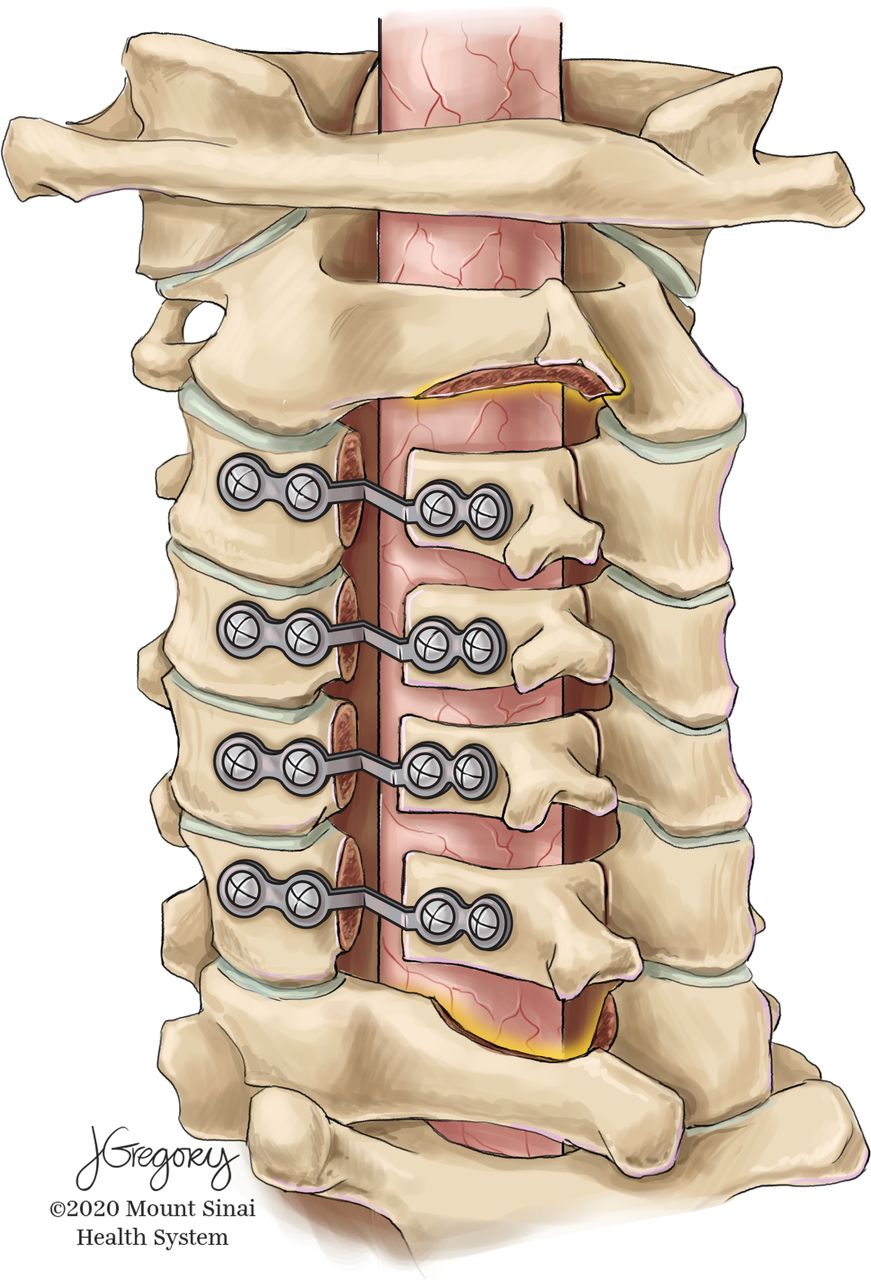
We gently uplifted the C6 lamina by taking advantage of the elastic properties of the bone. Special caution was taken to avoid fracturing the lamina at the hinge trough area. We then inserted an 8-mm laminoplasty plate, which was secured with 2 miniscrews, 5 mm in length, on the lamina and same number/size of screws on the lateral mass. The same process was repeated for C5, C4, and C3. Kerrison rongeurs were used to resect the ligamentum flavum at the C2–C3 and C6–C7 levels. The adequacy of this resection was confirmed by inspection and palpation of the dorsal epidural space with a Woodson elevator. Standard wound irrigation and hemostasis was performed. Then, we placed 2 medium subfascial Hemovac drains. The muscle, fascia, and deep subcutaneous layers were reapproximated and closed with Vicryl-0s. The dermis was closed with Vicryl 2-0s, and a Monocryl 3-0 was run in a subcuticular fashion. Figure 2 shows the bony anatomy at the completion of the operation.
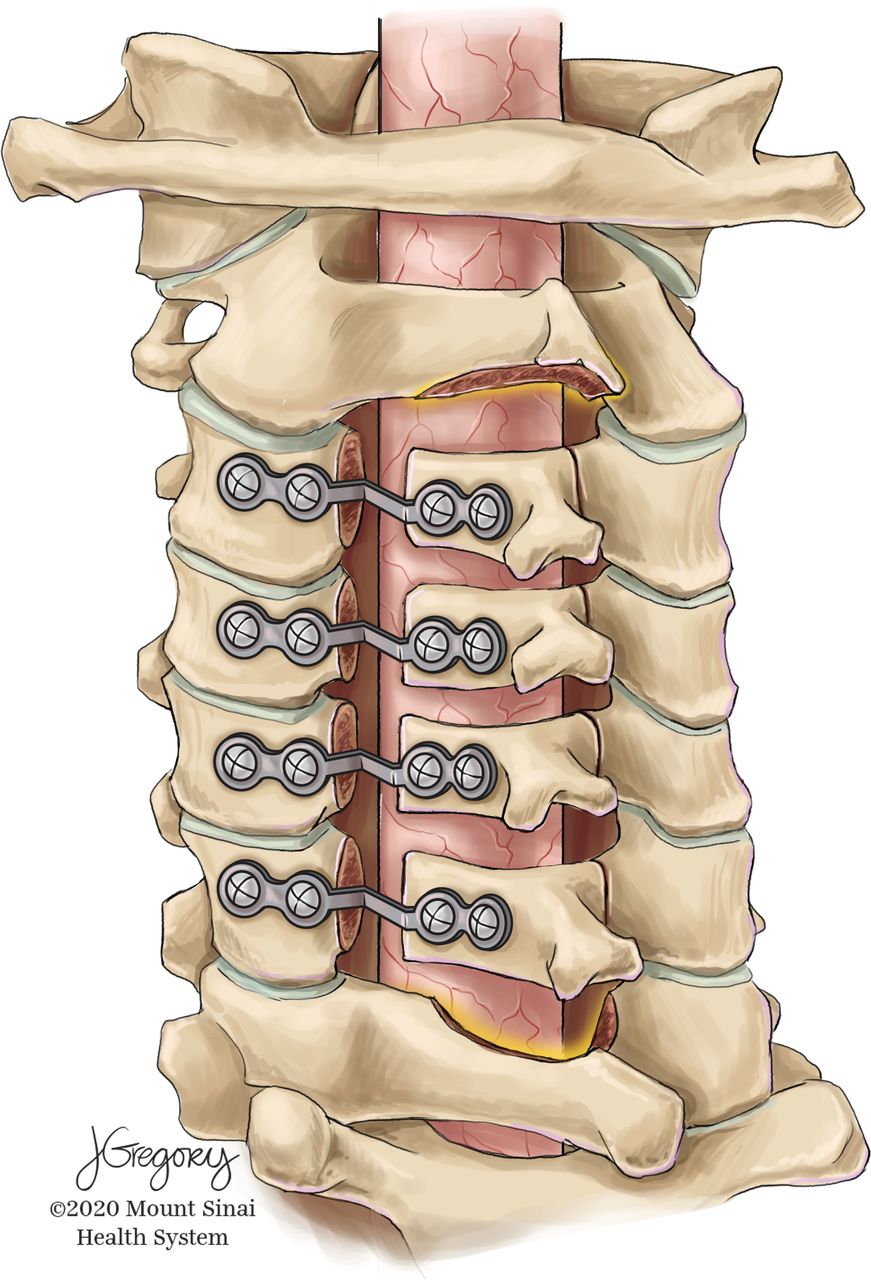
A dorsolateral view of the osseous structures at the completion of C3–C6 laminoplasty and C2/C7 dome laminotomies. Illustration by Jill K. Gregory, used with permission of ©Mount Sinai Health System.
RESULTS
Baseline Clinical Characteristics
A total of 21 consecutive patients (15 men and 6 women) having a mean ± SD age of 62.2 ± 10.4 years met the criteria for inclusion. Early and longer-term (“late”) postoperative follow-up clinical evaluation(s) occurred at a mean ± SD of 2.0 ± 1.5 months and 14.9 ± 13.1 months, respectively. The baseline clinical characteristics of the study patients are shown in Table 1. All patients had CSM; 2 of them also had radiographic evidence for mild OPLL.
Baseline clinical characteristics in the study patients.
Axial Pain
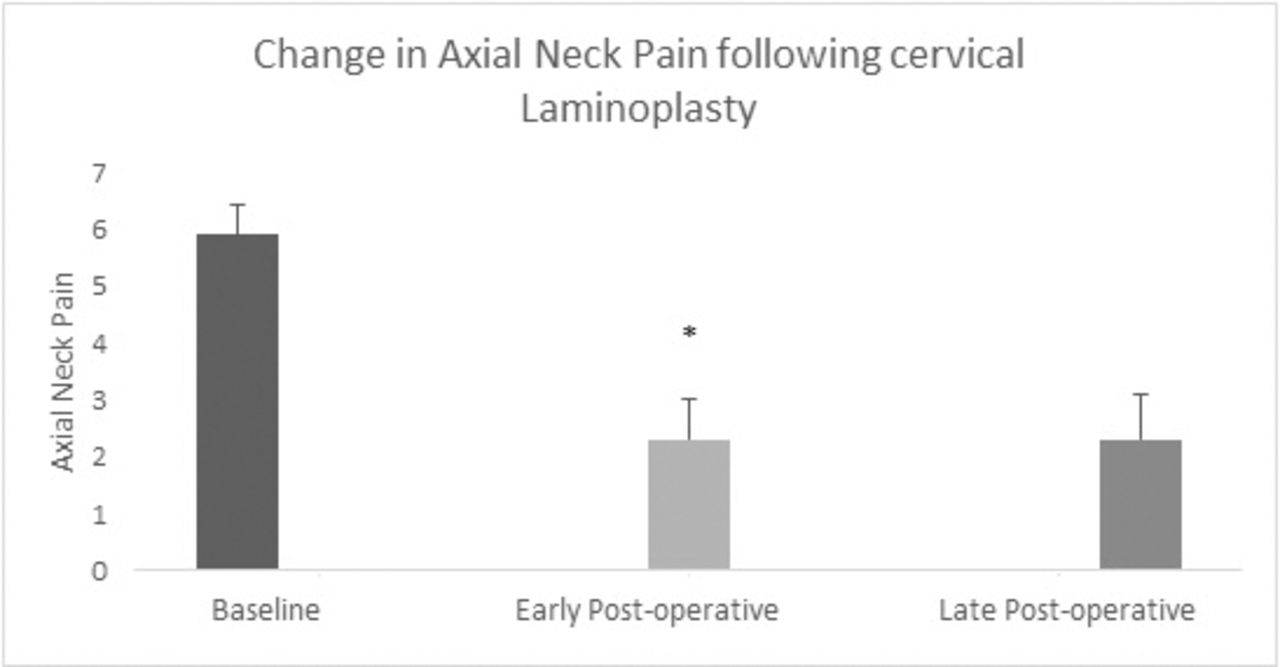
A total of 10 of 21 patients (48%) in our study group reported baseline neck pain preoperatively, including 7 of 21 (33%) having mild, 2 of 21 (4.7%) having moderate, and 1 of 21 (9.5%) having severe pain (Figure 3). In the early postoperative period, 11 of 21 patients (52%) had no axial neck pain and that is unchanged compared with the baseline percentage of patients with no pain (Figure 3). The proportion of patients reporting mild pain increased slightly to 9 of 21 (43%) from 7 of 21 (33%) preoperatively. This was because of 1 patient whose severe preoperative pain decreased significantly and 1 patient (pain-free at baseline) who experienced the new onset of mild postoperative pain. Only 1 patient reported moderately severe axial neck pain preoperatively; the pain had resolved in the early postoperative period, and it had not recurred by 15 months postoperatively (Figure 3). In 2 patients with severe preoperative axial pain, pain substantially improved in 1 patient and persisted early and at the 15-month visit in the second patient (Figure 3). There was no significant difference in the categories of no pain, mild, moderate, or severe pain during the postoperative follow-up period (Table 2). We next compared mean pain scores in patients evaluated at the baseline, early, and late postoperative periods. Patient self-reports of pain severity ranged from 1 to 5 (mild), 6 to 7 (moderate), and 8 to 10 (severe). Mean axial neck pain score improved significantly at both the early (P = .02) and late (P = .045) postoperative evaluations compared with mean baseline pain score (Figure 4).

Axial pain before and after C3–C6 laminoplasty with dome laminotomy. Results are proportions of patients with no, mild, moderate, or severe pain. Baseline and early postoperative visit (n = 21): mean, 2.9 months; late postoperative visit (n = 16): mean, 14.9 months.
Change in axial neck pain severity around the time of cervical laminoplasty.a

Change in mean axial pain score at early and late postoperative time points. There was a significant reduction in the mean pain score at both the early and late postoperative examinations compared with mean baseline pain score. *P < .05 compared to baseline mean axial pain.
Neurologic Function
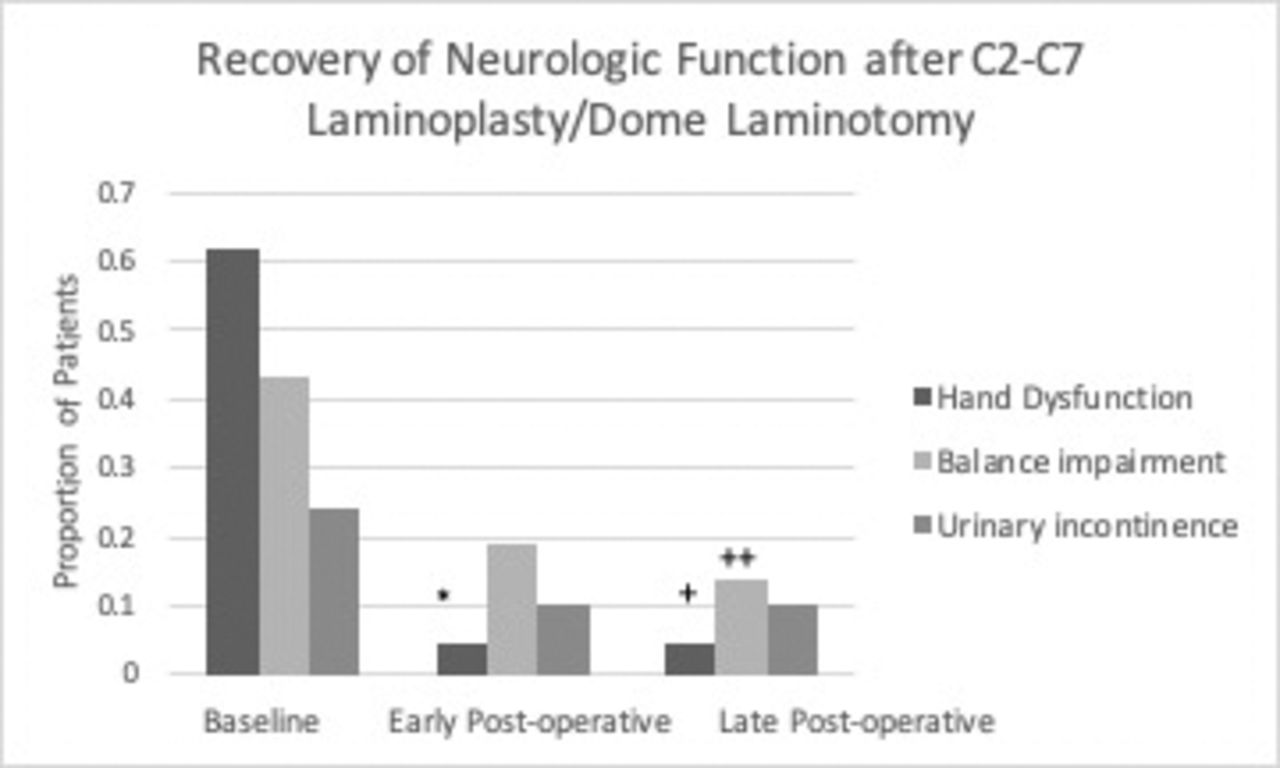
Baseline hand dysfunction improved significantly at the early and later postoperative time periods. The early response rate, (ie, proportion of patients who improved) was 92% (P = .0001) and the late response rate was 84% (P = .001; Figure 5). Balance impairment improved significantly at the late postoperative evaluation (67% response rate, P = .04), and there was a trend of improvement in balance function at the early postoperative time point (57% response rate, P = .06; Figure 5). Urinary dysfunction improved at the early (58% response rate) and late (42% response rate) postoperative evaluations; however, the results did not reach a statistically significant level, possibly because of the small numbers of affected patients (Figure 5). Only 5 of 21 patients (24%; 3 women and 2 men) experienced urinary dysfunction preoperatively. All 3 women experienced postoperative improvement in urinary symptoms, but 2 men continued to experience neurogenic bladder symptoms postoperatively, that is, a total 3 of 21 patients (14%) improved. The “urinary dysfunction response rate” represents the proportion of patients who improved postoperatively divided by the proportion of preoperatively affected patients, or 14%/24% = 58%.

Recovery of neurologic function following C3–C6 laminoplasty with dome laminotomy. There was a significant improvement in hand function at the early and late examinations, and balance impairment improved significantly at the late examination. *P = .0001; +P = .001; ++P < .05 compared to baseline proportion.
Complications
There was no occurrence of wound complication, C5 palsy, or late neurologic deterioration. In 1 patient, there was a new, stable 3-mm anterolisthesis C7 on T1 on postoperative radiographic evaluation which was not associated with any symptoms.
DISCUSSION
The study provides information about the efficacy and safety profile of our nuanced laminoplasty technique. As a retrospective study, there is no inherent control group for direct comparison. However, our profile appears satisfactory, and the study results allow for an indirect comparison with other variations of the technique from the published literature.
New postoperative axial pain (1 of 21; 4.8%) was an uncommon occurrence in our study, in close agreement with the results of Hosono et al8 following C3–C6 laminoplasty without dome laminotomies. The similar pain outcome between the 2 studies suggests that addition of dome laminotomy at C2 and C7 does not alter the favorable pain outcome of C3–C6 laminoplasty (Figure 6). Riew et al3 conducted a systematic review and found evidence that C2 procedures that spare the semispinalis cervicis muscle were associated with a lower incidence of postoperative axial pain. In the present study, the addition of C2 dome laminotomy adhered to the principle of preserving the C2 muscle insertion.

(A) Preoperative sagittal T2 magnetic resonance image which revealed degenerative, superimposed on congenital stenosis with anterior-posterior diameter as low as 4.4 mm. (B) Decompressed C2–C3 level. (C) Decompressed C6–C7 level.
In the current study, zero patients experienced C5 palsy, which compares favorably with prior reports reporting an incidence of postoperative C5 palsy of 8% following C3–C6 laminoplasty without dome laminotomy.3 Faster operative time and shorter wound length of C3–C6 (vs C3–C7) laminoplasty have been cited8 as likely contributing to low incidence of wound complications.
The prevalence of urinary dysfunction in our study (24%) was not substantially higher than the prevalence of clinically relevant urinary symptoms (18%) previously reported among men and women patients (mean age, 58 years) undergoing elective cervical spine surgery.11 Myelopathy (vs no myelopathy) was previously associated with a nearly 3-fold higher rate of baseline clinical urinary dysfunction (30 % vs 11%) in the same study of cervical spine surgery patients reported by Lieberman et al.11 It is possible that postoperative improvement in urinary symptoms experienced by some patients may have been due in part to relief of spinal cord compression. Still, urinary dysfunction among women is quite common,12 and its underlying etiology may be multifactorial.
Another advantage of dome laminotomy is the prevention of impingement of the cord by the cranial edge of C7 lamina due to dorsal expansion of the dura in the decompressed area. This impingement has been described by Hosono et al8 in the C3/C6 laminoplasty approach, where they did not perform C7 dome laminotomy. Although late neurologic deterioration was not observed in any of our patients, Sakuara et al9 reported late neurologic deterioration at the caudal segment in 3 of 137 patients (2.2%) 16–60 months after C3–C6 laminoplasty. Longer-term follow-up in a larger group of patients may be required to exclude the possibility of late neurologic deterioration following C3–C6 laminoplasty with C7 dome laminotomy. The expected risk is minimized by virtue of the C7 dome laminotomy's increase in the anterior-posterior diameter of the spinal canal at the cranial aspect of C7 lamina (Figure 7).
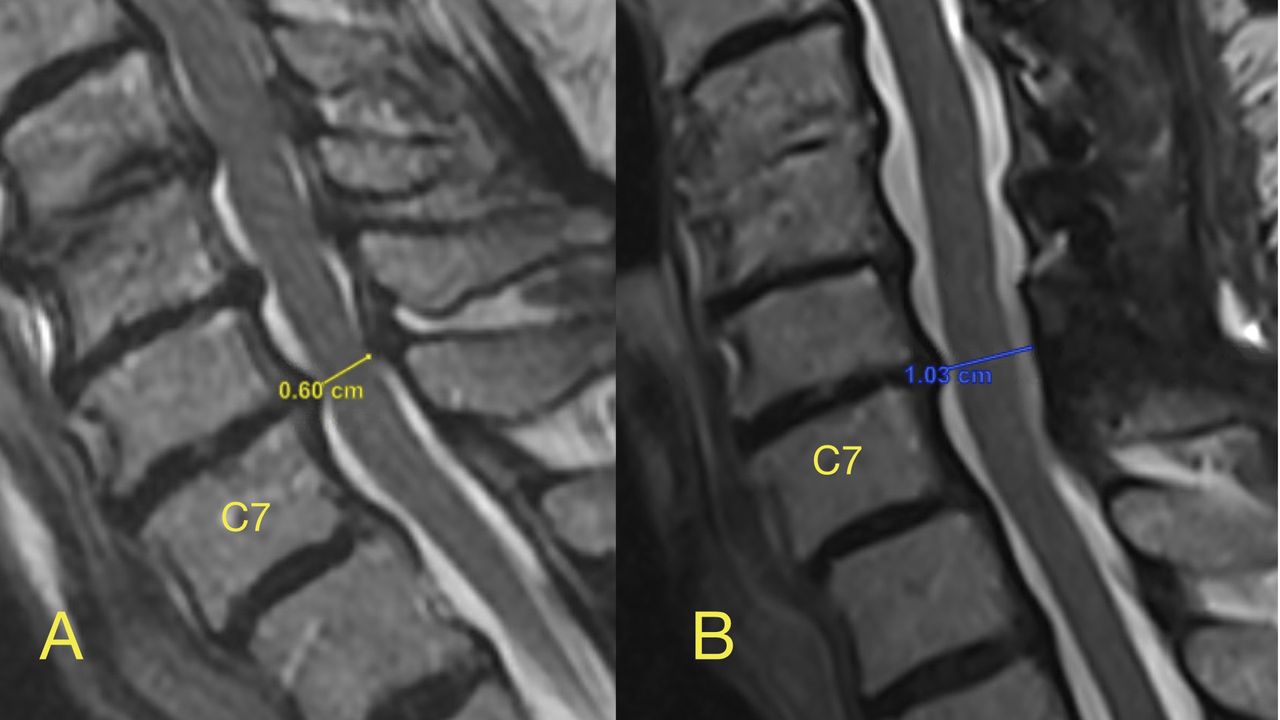
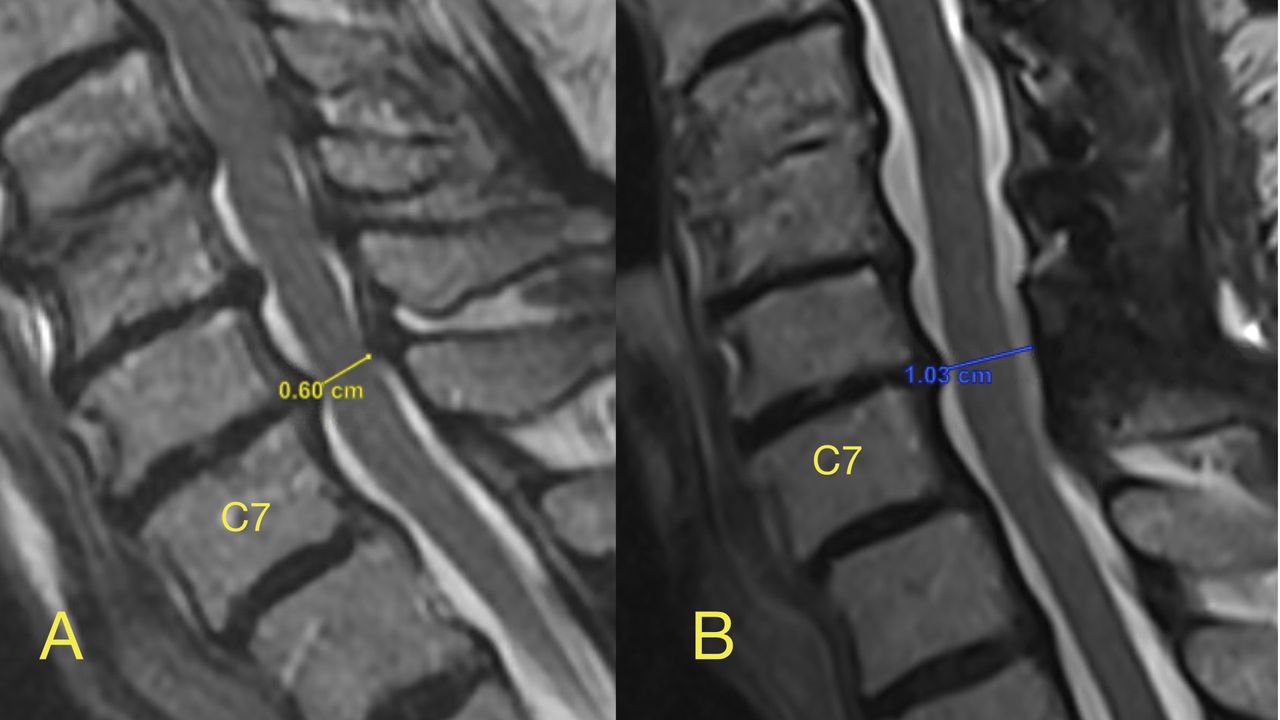
(A) Preoperative stenosis at the C6–C7 level with an AP diameter of the spinal canal of only 6 mm. (B) Image was obtained after a fall experienced 10 months after surgery which was associated with subjective weakness. It shows an increase in AP diameter of the spinal canal to 10.3 mm with adequate decompression of the spinal cord at the C6–C7 level. Of note, the patient had a stable mild spondylolisthesis at C7–T1 that remained unaltered postoperatively.
Mesfin et al4 reported on 34 patients treated with C3 laminectomy including modified C7 undercuts in patients who required it. C3 laminoplasty was avoided, with the belief that it contributes to postoperative axial pain. However, the present results demonstrating a low occurrence rate of postoperative axial pain associated with C3 laminoplasty suggest that the C3 laminectomy (used in their study) is possibly not necessary. The main criticism against C3 laminectomy is the disruption of the posterior tension band at the proximal end of the operated spine levels, which could theoretically contribute to delayed instability.
Sakaura et al9 reported long-term results following C3–C6 laminoplasty sparing muscles attached to the C2 and C7 spinous processes. They found that axial pain continued to decrease and neurologic function was preserved long-term, in general agreement with the results from our study. Sakaura et al10 reported zero occurrence of postoperative kyphotic deformity, consistent with the results in our study.
Lee et al5 found that at both 6-month and 1-year follow-up, patients who had been treated with C3 laminectomy experienced significantly lower mean pain than the patients treated with C3 laminoplasty. These results probably suggest the need for definitive decompression at C2–C3 vs C3 laminoplasty alone. We achieved definitive decompression through C2 undercut with C3–C6 laminoplasty. Our data that early and late axial pain decreased by ∼58% agree with the findings of Lee et al5 that mean postoperative axial pain scores decreased by 55%–63% in the C3 laminectomy cohort. Given the similar outcomes, it appears preferable to maintain the integrity of the posterior tension band by performing a C3 laminoplasty with C2 undercut rather than C3 laminectomy.
Performing dome laminotomies does not require special equipment or any new skill set. The favorable results reported here include cases from the very beginning of the learning curve (Figure 8), suggesting no compromise on the safety or efficacy of the technique.

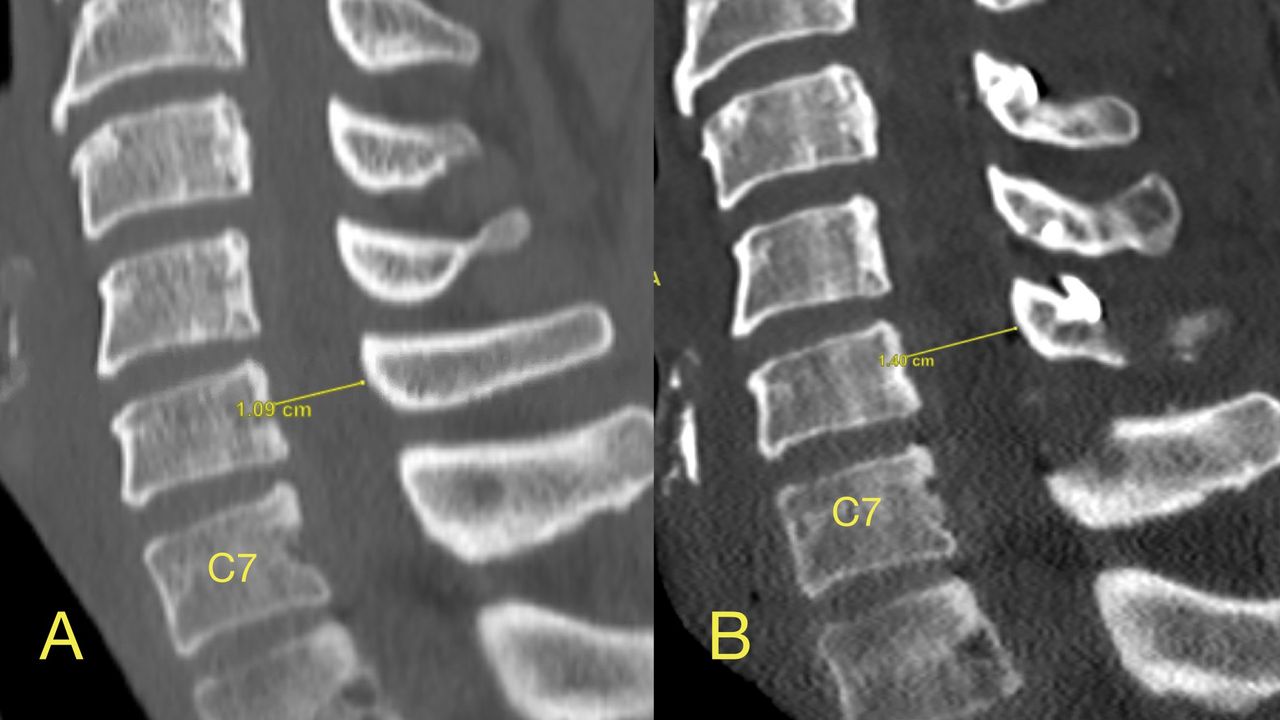
(A) Preoperative sagittal CT. At the C6 level the AP diameter of the osseous spinal canal is 10 mm. (B) The dome laminotomy at C7 as well as the enlargement of the AP diameter of the osseous spinal canal to 14 mm. This is a case relatively early in this case series. The amount of bony resection was relatively more extensive in patients operated on later in the series.
CONCLUSIONS
In summary, C3–C6 laminoplasty that includes C2 and C7 dome laminotomies was associated with satisfactory improvement in neurologic function (hand function, balance, urinary dysfunction) and long-term control of axial neck pain without significant early or late postoperative complications.
Footnotes
Disclosures and COI: The authors report no multiplicity of interest that could affect the objectivity of the presented results. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The study was approved by the institution's Investigational Review Board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.