


Abstract
Objectives Vitamin D plays a major role in bone metabolism, regulating calcium and phosphorus homeostasis, along with bone growth and remodeling processes. The objective of the present study was to assess the effect of vitamin D deficiency on clinical outcomes following elective spinal fusion surgery by conducting a meta-analysis on the relevant literature.
Methods Studies included in this analysis involved patients older than 18 years who underwent elective spinal fusion surgery. The number of patients as well as visual analog scale (VAS) and Oswestry Disability Index (ODI) in groups with and without vitamin D deficiency were required to be reported in eligible studies. Of the 179 articles identified, 7 met the inclusion criteria and were included in the analysis.
Results Seven studies, including 1188 patients, reported the relationship between vitamin D deficiency and clinical outcomes in patients undergoing elective spinal fusion surgery. Five studies reported VAS as a primary outcome. The combined results using a random-effects model showed reduction in VAS after elective spinal fusion surgery in group with vitamin D deficiency, but no statistically significant association was identified between vitamin D deficiency and VAS. ODI was assessed and reported as an outcome measure in 5 of the included studies. The combined results showed an increase in ODI following elective spinal fusion surgery in the vitamin D-deficient group compared to the group with normal levels of vitamin D. In addition, a significant association was observed between ODI and vitamin D deficiency.
Conclusions Vitamin D deficiency may negatively affect the postoperative outcomes in elective spinal fusion surgery. Preoperative optimization of vitamin D levels would seem appropriate. Future high-quality studies are highly warranted to evaluate this.
Clinical Relevance This meta-analysis demonstrated a significant association between vitamin D deficiency and postoperative ODI scores in patients undergoing elective spinal fusion surgery.
Level of Evidence 2.
- vitamin D deficiency
- Oswestry Disability Index
- visual analog scale
- systematic review
- meta-analysis
- spinal fusion
- bone metabolism
INTRODUCTION
Vitamin D plays a major role in bone metabolism, regulating calcium and phosphorus homeostasis, along with bone growth and remodeling processes via osteoblasts and osteoclasts, respectively. In addition, it contributes to neuromuscular and immune function, modulation of cell growth, and reduction of inflammation. The physiologically active form of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)2D), is primarily responsible for these effects. However, this form cannot be easily assessed, so the more stable precursor 25(OH)2D is assessed instead as a proxy, with a level below 20 ng/mL being regarded as vitamin D deficiency. The key risk factors for vitamin D deficiency are advanced age, reduced skin pigmentation, low sunshine exposure, increased anthropometry, and malabsorption among others.1
Vitamin D deficiency is common among patients undergoing elective spine surgery. However, adequate amounts of vitamin D are required for normal bone metabolism and postsurgical healing processes.2–5 Therefore, vitamin D deficiency is thought to have major implications for immediate and long-term postoperative spinal outcomes.4,6 Despite the biological plausibility of this hypothesis, the majority of studies that have examined the association between vitamin D deficiency and postoperative outcomes in elective spinal fusion surgery have been crucially limited by their modest sample size, thereby resulting in a degree of discord within the field. The objective of the present study was to assess the effect of vitamin D deficiency on clinical outcomes following elective spinal fusion surgery by conducting a meta-analysis of the relevant current literature.
METHODS
Search Strategy
This study was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist. PubMed/MEDLINE, Scopus, Embase, and Google Scholar search was conducted to identify the relevant studies written in English from inception to July 2020. Keywords used for search were: “spinal fusion” OR “spinal surgery” OR “spinal fusion surgery” OR “posterior spinal surgery” OR “anterior spinal surgery” OR “lumbar spinal surgery” OR “thoracic spinal surgery” OR “cervical spinal surgery” OR “cervical fusion” OR “lumbar fusion” OR “thoracic fusion” AND “vitamin D” OR “ergocalciferols” OR “vitamin D deficiency” OR “cholecalciferol” OR “calcifediol,” OR “25-hydroxyvitamin D.”
Eligibility Criteria
Studies included in this analysis included patients older than 18 years who underwent elective spinal fusion surgery. Assessment of data regarding the number of patients, as well as visual analog scale (VAS) and Oswestry Disability Index (ODI) scores in groups with and without vitamin D deficiency, was required to be reported in eligible studies. All articles were assessed by two independent reviewers. Finally, notes, commentaries, conference papers, letters, and reviews were all excluded in the present design.
Data Extraction
The following data were extracted from the eligible studies: first author, year of publication, country, sample size, age, gender, duration of study, procedure type, pathology, mean, and standard deviation of predefined outcome parameters following surgery.
Quality Assessment
For the quality assessment of studies, the Newcastle-Ottawa Scale (NOS) was applied.7,8 Each study received a score using the following criteria: selection of study samples, intergroup comparability, and ascertainment of the outcome of interest.
Statistical Methods
Median or mean vitamin D in each category was assumed as the corresponding dose of that category. DerSimonian and Laird random-effects model was used to combine mean differences.9 Cochran Q test and I 2 statistic were used to assess heterogeneity among included studies. The publication bias among studies was determined using funnel plot, as well as Egger’s and Begg’s weighted regression analyses. All statistical analyses were performed using STATA 14.0 statistical software (Stata Corporation, College Station, Texas, USA).
RESULTS
Search Results
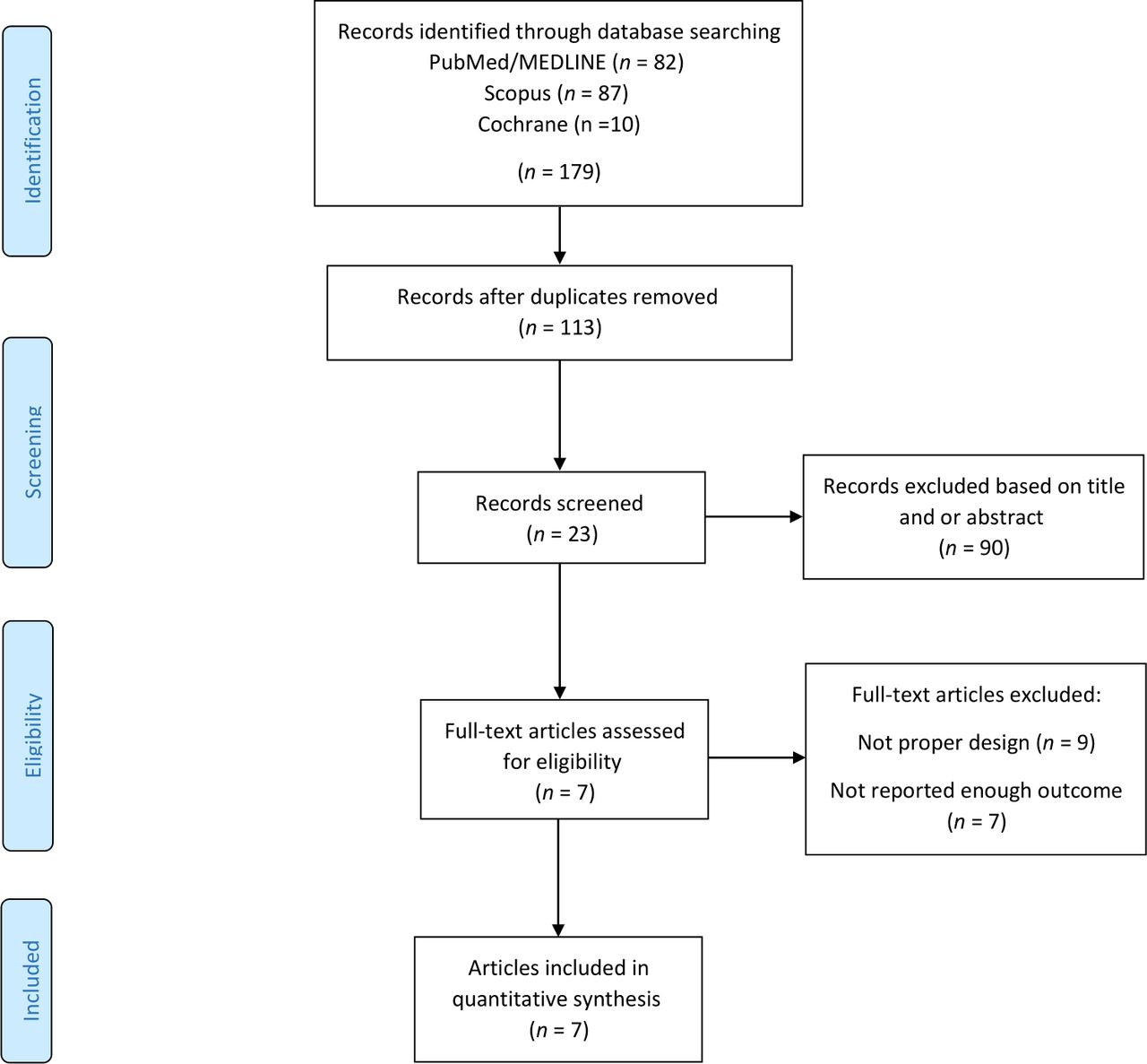
Our initial comprehensive search identified 179 articles. After removing 66 duplicates, 113 articles remained for primary screening. Subsequently, 90 studies were excluded by title and abstract screening, while the remaining 23 were evaluated thoroughly by full text assessment. Finally, 7 articles remained for analysis according to our defined inclusion criteria.2,5,10–13 Figure 1 demonstrates the systematic search and exclusion protocol.
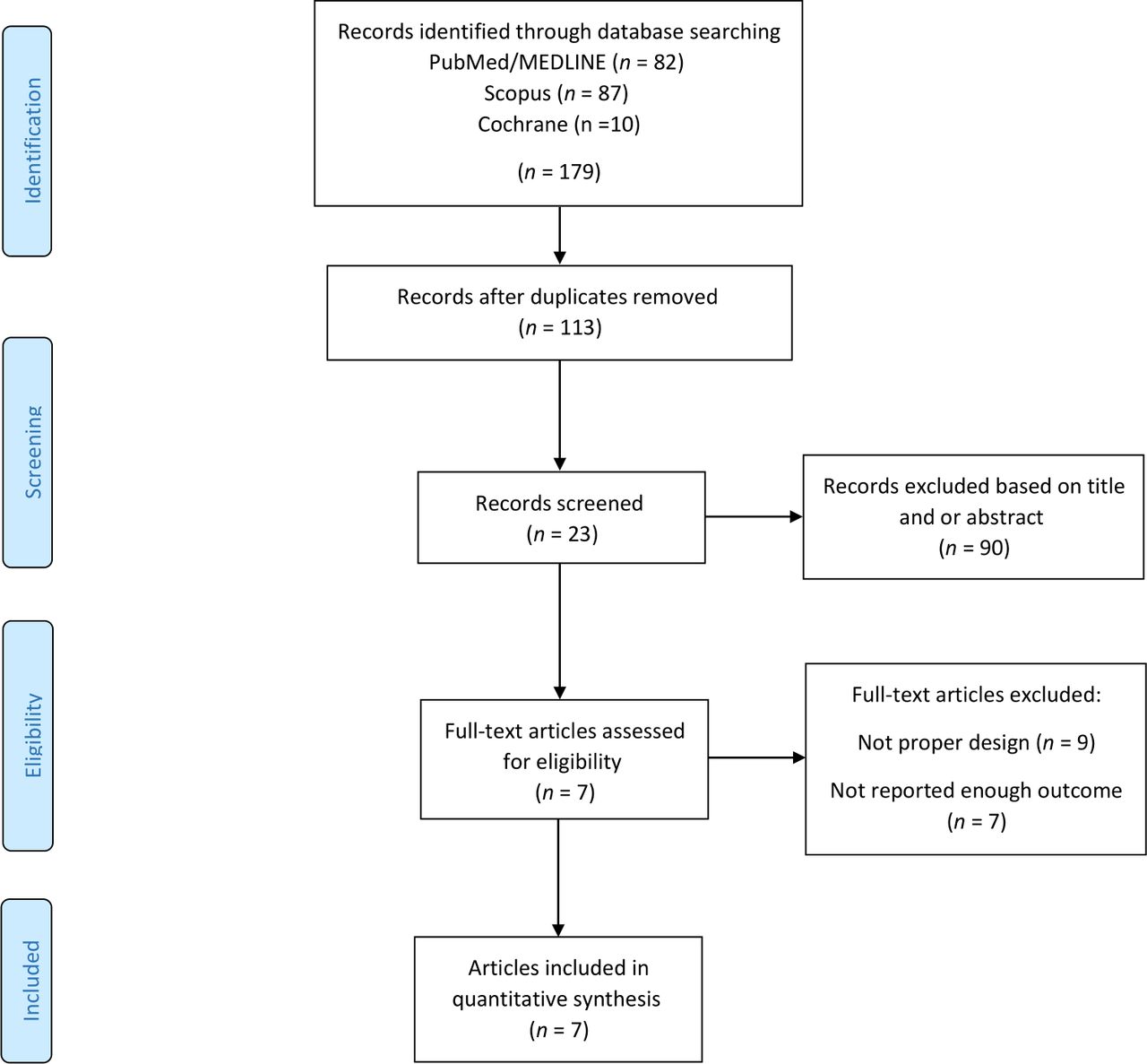
Flow chart of included studies.
Study Characteristics
The characteristics of 7 included cohort studies are outlined in Table 1. The total sample size was 1188 participants and studies published from 2012 to 2020. Four of these studies were conducted in the United States,2,5,12,13 and 3 other studies in Brazil,11 Korea,10 and China.14 Duration of the studies included ranged from 12 to 24 months. One article was conducted solely on female participants, while the rest were conducted with participants of both genders. Among the studies assessed, 514 participants (43.3%) were men and 674 were women (56.7%). The most common surgical indication was degenerative pathology (n = 929, 77.9%). The study populations were divided into two categories based on their serum vitamin D level: deficient (<20 ng/mL) and not deficient (>20 ng/mL).
Characteristics of included studies.
Quality of Studies
Quality of studies assessed based on NOS: 4 for selection, 1 for comparability, and 3 for outcome. In section of comparability, yes considered for adjustment for confounding/bias ≥3 and no ≤3 of 7 articles, just 2 studies did not meet the high quality (Table 2).
Quality of cohort studies assessed based on modified Newcastle-Ottawa scaling.
Meta-Analysis
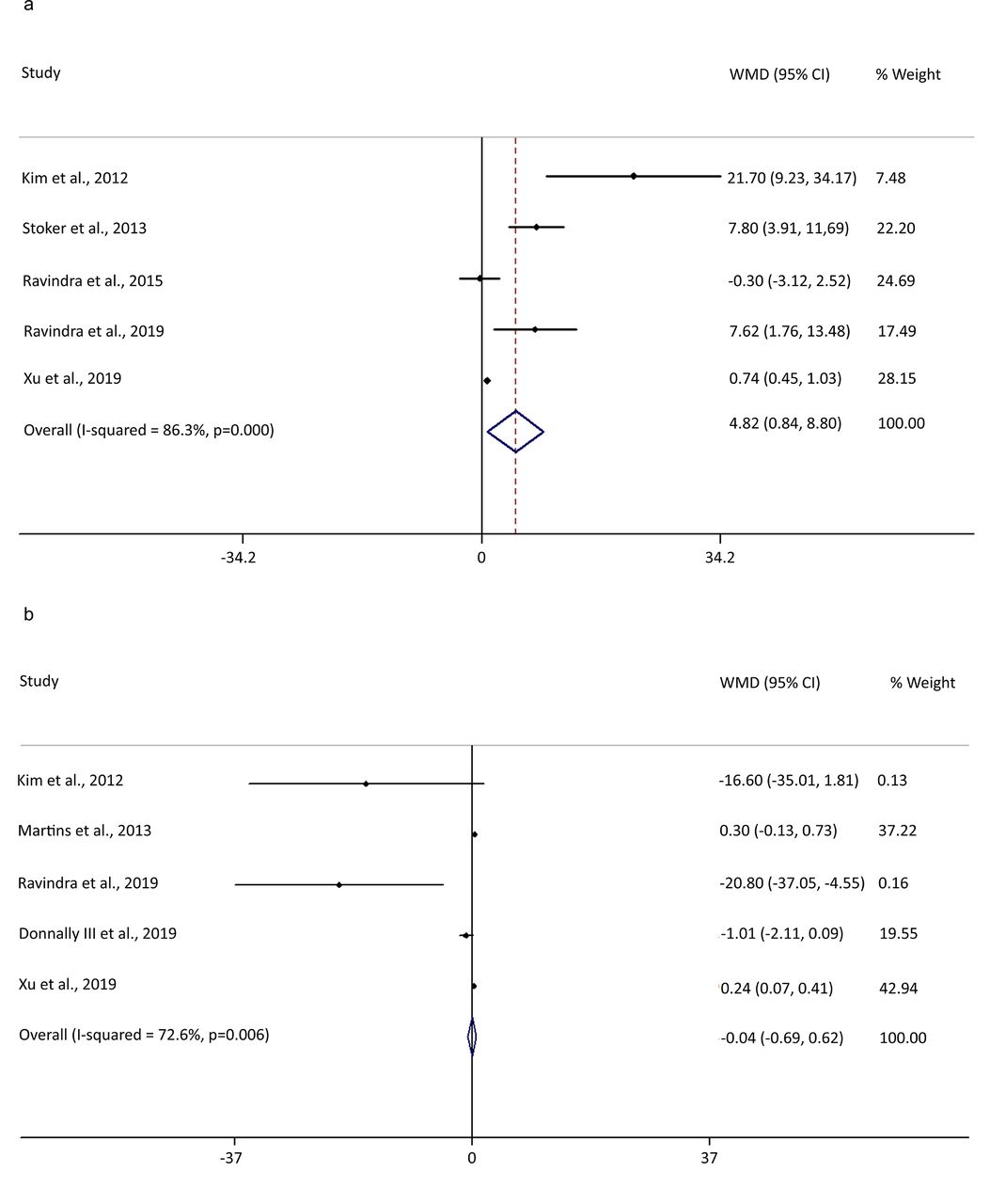
Seven studies, including 1188 patients, reported the relationship between vitamin D deficiency and clinical outcomes on patients undergoing elective spinal fusion surgery. Five studies reported VAS as a primary outcome. The combined results using a random-effects model show −0.04 (95% CI: −0.69, 0.62; I 2 = 72%) reduction in VAS after elective spinal fusion surgery in group with vitamin D deficiency, but no statistically significant association was identified between vitamin D deficiency and VAS. ODI was assessed and reported as an outcome measure in 5 of the included studies. The combined results showed a 4.82 (95% CI: 0.84, 8.80; I 2 = 86%) increase in ODI following elective spinal fusion surgery in the vitamin D-deficient group compared to the group with normal levels of vitamin D. In addition, a significant association was observed between ODI and vitamin D deficiency (Figure 2).

Meta-analysis of the vitamin D deficiency effect on (A) visual analog scale and (B) Oswestry Disability Index. Weights are from random effects analysis. WMD, weighted mean difference.
Publication Bias
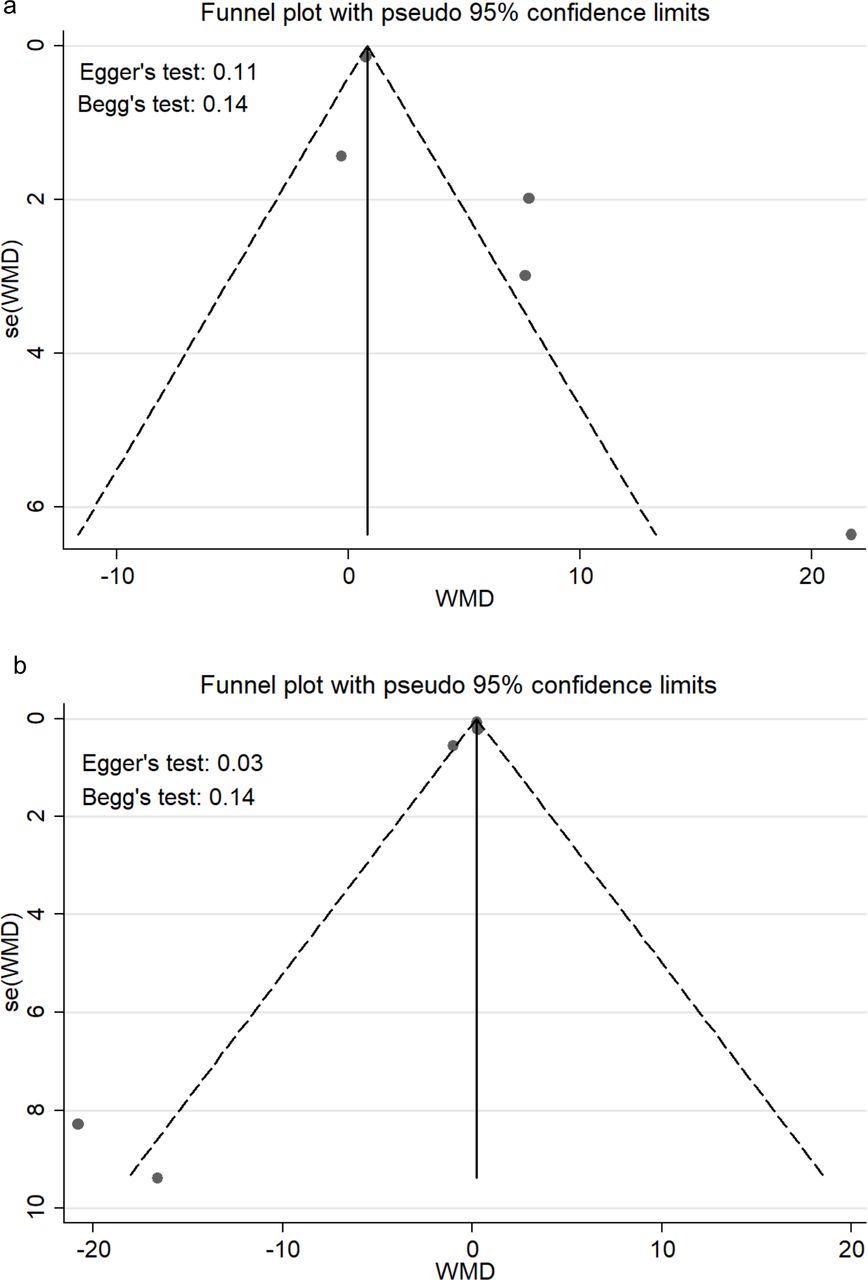
Publication bias, as evaluated by the Egger’s and Begg’s tests, did not reveal any publication bias for VAS (P = 0.03 and 0.14) and ODI (P = 0.11 and 0.14), respectively (Figure 3). In addition, no asymmetry was detected between included studies.

Funnel plot to assess publication bias on (A) visual analog scale and (B) Oswestry Disability Index. se(WMD), standard error (weighted mean difference); WMD, weighted mean difference.
DISCUSSION
This meta-analysis of 7 studies supports the fact that vitamin D deficiency is correlated with poor patient-reported outcomes after elective spinal fusion surgery. Outcome measures that have been utilized for evaluating patient postoperative status and quality of life include ODI, EuroQoL 5-dimension (EQ-5D), Neck Disability Index (NDI), VAS, and Scoliosis Research Society-22.2,5,6,10–12 However, solely ODI and VAS were considered as endpoints in the present study due to their ubiquity in the aforementioned studies. Although a significant association was observed between ODI and vitamin D deficiency, there was no such relationship identified for VAS.
From a total of 1142 patients with reported vitamin D status (one study did not report the number of patients with abnormal vitamin D status), 445 patients (38.9%) had vitamin D deficiency in the present meta-analysis. The prevalence of vitamin D deficiency in patients undergoing instrumented spine surgery has been relatively high in previous studies.2,5,15 According to Stoker et al, 27% and 57% of patients undergoing spinal fusion were vitamin D-deficient and insufficient, respectively, in a cohort of 313 patients.5 Another prospective study showed 30% and approximately 70% of patients undergoing elective spine surgery had vitamin D deficiency and insufficiency, respectively.2 Schmidt et al in a recent retrospective study found that the prevalence of vitamin D deficiency and insufficiency was 36.8% and 73.6% among 144 patients undergoing spinal surgery, respectively.15 Various additional risk factors have also been assessed by these studies. For example, increasing body mass index, NDI, ODI, and a lack of vitamin D supplementation were all defined as risk factors for deficiency by Stoker and colleagues.5 In the study by Ravindra et al, vitamin D deficiency was found to be associated with male gender, age 40–60 years, body mass index >40, lack of vitamin D supplementation, and an existing diagnosis of diabetes. However, they identified no correlation between patient clinical status, as measured by NDI and ODI, and vitamin D deficiency.2
Data related to correlation between vitamin D deficiency and postoperative outcomes have lacked congruency among the studies. Kim et al demonstrated significantly worse postoperative outcomes, as assessed by EuroQoL 5-dimension and ODI, in vitamin D-deficient individuals relative to the control cohort.10 Moreover, a previous observational study found a significant association between vitamin D inadequacy and lower NDI following fusion surgery for cervical spondylotic myelopathy.12 Similarly, Xu et al demonstrated a significantly better clinical outcome at 3 months after the procedure, according to the VAS and ODI, in a cohort of 360 patients who underwent elective posterior lumbar spinal fusion.14 This investigation included patients with degenerative pathology while those with other indications such as trauma, tumor, and infection were excluded from the study. By contrast, Martins et al showed no significant difference between vitamin D-deficient and nondeficient group in terms of quality of life indices including Scoliosis Research Society-22, ODI, and VAS, 1 year postoperatively.11 However, this study is crucially limited by the heterogeneity of the pathologies (degenerative, trauma, tumor, infection, and deformity) and types of spinal surgeries studied. In addition to heterogeneity, this study had a relatively small sample size in comparison to other studies. Consequently, there is discord among the available data mainly because of different populations that have been studied and dissimilarities in methodology, and this warrants further investigation through high-quality randomized controlled trials.
Nevertheless, the present meta-analysis found a significant correlation between vitamin D deficiency and ODI (an increase of 4.82 in the vitamin D deficiency group). Regarding minimal clinically important difference (MCID) of the ODI, previous studies have shown varying results.16–19 Copay et al found an MCID of 12.8 for ODI 1 year after surgery in a cohort of 454 patients who underwent lumbar spinal surgery.18 Monticone et al showed that MCID for ODI is 9.5 (sensitivity 76% and specificity 63%) using the anchor-based methods in a cohort of 179 patients with subacute and chronic back pain.17 In another retrospective study of a cohort of 240 patients who underwent spinal deformity surgery, the MCID of ODI was 11.19 The difference of ODI (4.82) between the 2 groups was statistically significant in the present meta-analysis; yet, it was less than its MCID, according to previous studies.
Although most prior studies have assessed postoperative functional outcomes such as VAS, ODI, and NDI as the outcome measure, the effects of vitamin D deficiency on spinal fusion or nonunion have been less investigated. Due mainly to the effects of various variables such as demographics, vitamin D supplementation, procedure type, graft type, and follow-up time, functional outcome measures may be subject to variation. Thus, the use of fusion-related outcomes is a more accurate strategy in evaluating the relationship between vitamin D deficiency and postoperative outcomes. However, merely a limited number of studies have evaluated the association between vitamin D level and fusion rate.6,13,20,21 Donnally et al found no significant correlation between the pre- and postoperative vitamin D levels and rates of pseudarthrosis or revision surgery after the lumbar spinal fusion surgery.13 On the contrary, Ravindra et al showed a significantly longer time to fusion in patients with vitamin D deficiency who underwent elective spinal fusion.6 They also performed a multivariate logistic regression, which was controlled for many possible confounding variables, and found that vitamin D deficiency is an independent predictor of pseudarthrosis within a period of 12 months. Xu et al, in a retrospective study on 44 patients who underwent posterior transforaminal lumbar interbody fusion, also demonstrated a significantly higher fusion rate in patients who received vitamin D supplementation according to imaging findings at 6 months postoperatively.21 In the investigation performed by Schofferman et al on 47 patients with pseudarthrosis, no significant correlation was found between metabolic bone abnormalities and nonunion after lumbar spinal fusion surgery.20 Nonetheless, currently, data are insufficient to draw firm conclusions concerning the direct effects of vitamin D deficiency or its supplementation on spinal fusion and postoperative pseudarthrosis. Hence, future research should focus on how vitamin D levels affect spinal fusion directly through imaging outcomes, which are more informative than functional outcome measures, while addressing the limitations associated with previous studies. On the other hand, prior studies have shown that vitamin D might be involved in the nociception process directly through various mechanisms, including sensory neuron excitability modulation and inflammatory cytokines’ reduction in addition to its effects on bone mineral density and fusion.22–27 However, due to the lack of high-quality studies, current evidence is inconclusive on this potential effect of vitamin D deficiency.28
Follow-up period is one of the most common limitations of prior studies, particularly those that assessed the impact of vitamin D deficiency upon postoperative complications such as pseudarthrosis, instrumentation failure, and revision surgery. Prior reports have shown that pseudarthrosis is the most common reason for revision surgery >12 months postoperatively among patients undergoing elective spinal procedures.29–31 Therefore, future studies must prioritize the long-term evaluation of patients. Additionally, determined risk factors for vitamin D deficiency should be appropriately adjusted for in future studies. As an example, in Kim et al study, the authors divulge that they could not control the patients’ vitamin D intake in the postoperative period.10 Similarly, Ravindra and colleagues found that preoperative vitamin D supplementation details were subject to recall bias.2 Of the studies assessed herein, 7 studies were prospective and observational in design, but there were no randomized controlled trials. In order to understand the relationship between vitamin D status and surgical outcomes, as well as the preventative role of vitamin D supplementation in patients undergoing elective spinal fusion surgery, appropriately designed randomized controlled trials are of central importance.
Limitations
Before this meta-analysis, Kerezoudis et al had previously performed a systematic review in 2016 on vitamin D deficiency and its association with postoperative outcomes after spinal fusion surgery.32 To our knowledge, however, our study is the first meta-analysis investigating the proposed correlation between vitamin D status and postoperative surgical outcomes in patients undergoing elective spinal fusion surgery. In addition to quantitative analysis, our study involves more recent studies that have not been assessed in the previous review. There are a number of notable limitations to the present analysis, including the small number of studies available, the lack of randomized controlled trials, and absence of control groups within the assessed studies. In addition, heterogeneity was observed among the studies, including participant demographics and risk factors, as well as surgical characteristics and outcome measures. Moreover, the relatively small sample sizes and atypical nature of the certain cohorts in the included studies make the analysis and extrapolation more challenging. Finally, only a few studies assessed the time to fusion, revision surgery, and postoperative surgical complications, in addition to patient-reported outcomes. Therefore, we could not evaluate the effect of vitamin D deficiency on fusion in the present meta-analysis. Reduction of the effect of various demographic confounders in studies is the main advantage of assessing the postoperative complications and fusion directly since VAS and ODI are subject to confounding in such a heterogeneous population of patients. However, there is a paucity of evidence in this regard, and future studies are highly warranted to evaluate the effect of vitamin D deficiency on pseudarthrosis and fusion directly.
CONCLUSIONS
In conclusion, our study results showed that vitamin D deficiency is associated with a negative impact upon postoperative clinical outcomes in patients undergoing elective spinal fusion surgery and preoperative optimization of vitamin D levels might be an effective strategy in this regard. However, there is a need for further high-quality studies to provide more pieces of evidence in this regard.
Footnotes
Funding This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
Ethics Approval The Shahid Beheshti University of Medical Sciences’ institutional review board approved the present study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.