


Abstract
Background No-profile anterior cervical discectomy and fusion (ACDF) devices are commonplace in spinal surgery. Contained within the intervertebral margins, these devices diminish risks associated with anterior cervical plating, while also marginalizing cage migration and subsidence. However, these devices have been limited in their scope of implant material. Accordingly, a no-profile ACDF (npACDF) device supporting a machined allograft implant body with a connected load-sharing fixation interface was developed. However, it is not established in the literature whether the device supports early mechanical stability and subsequent boney fusion. The objective of this study was to assess this device in both the clinical and preclinical settings.
Methods Biomechanical Analysis: Twenty-four functional spinal units (FSUs) were divided into 4 groups (n = 6). Each group would receive a single construct: (1) npACDF device with connected polyetheretherketone (PEEK) body, (2) npACDF with connected allograft body, (3) npACDF (allograft body) with nonconnected fixation plate, and (4) standard ACDF plate and PEEK interbody cage. FSUs were subjected to pure moment loading (flexion/extension, lateral bending, and axial rotation) via a kinematic test machine in their intact state and then following instrumentation. Vertebral motion was recorded and range-of-motion (ROM) reduction, relative to intact, was calculated.
Clinical Case Series: Ten patients receiving single-level ACDF with the npACDF allograft (connected) device for the treatment of persistent cervical radiculopathy or myelopathy were retrospectively reviewed at 12 months. Radiographic and patient reported outcomes were reported.
Results No differences in ROM existed between the npACDF constructs (P ≥ 0.99). Standard ACDF achieved more ROM reduction than the npACDF constructs in all directions (P ≥ 0.04). All subjects achieved fusion at 12 months.
Conclusions The npACDF allograft device supported less motion reduction in comparison to traditional plating; however, case series data suggest the device provides clinically effective stability resulting in quality radiographic fusion and pain improvement.
Clinical Relevance This report provides both clinical and preclinical insight into a device which offers alternative design features to traditional continuous/rigid ACDF device designs.
Level of Evidence 4.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is a well-established and efficacious intervention when treating pain secondary to degeneration, trauma, and instability of the cervical spine. First described by Cloward, and Robinson and Smith in the 1950s, ACDF technique and philosophy have evolved markedly in recent decades.1,2 While the end-stage goals of neural element decompression and segmental stabilization in pursuit of arthrodesis remain largely unchanged with ACDF, considerable innovation has occurred in attempts to diminish the hardware footprint and optimize the fusion environment.3
Of particular note has been the development and emergence of integrated fixation (“no-profile” and “zero-profile”) ACDF devices. Contained entirely within the intervertebral margins, these devices decrease operative demand (ie, decreased operative time and intraoperative blood loss) and postoperative risk of dysphagia while also marginalizing disc height loss in comparison to stand-alone (cage only) techniques.4,5 However, these devices do possess their own inherent limitations, which can include localized endplate contact areas (ie, fixed angle screws) and narrow scope of implant materials (ie, not allograft compatible).
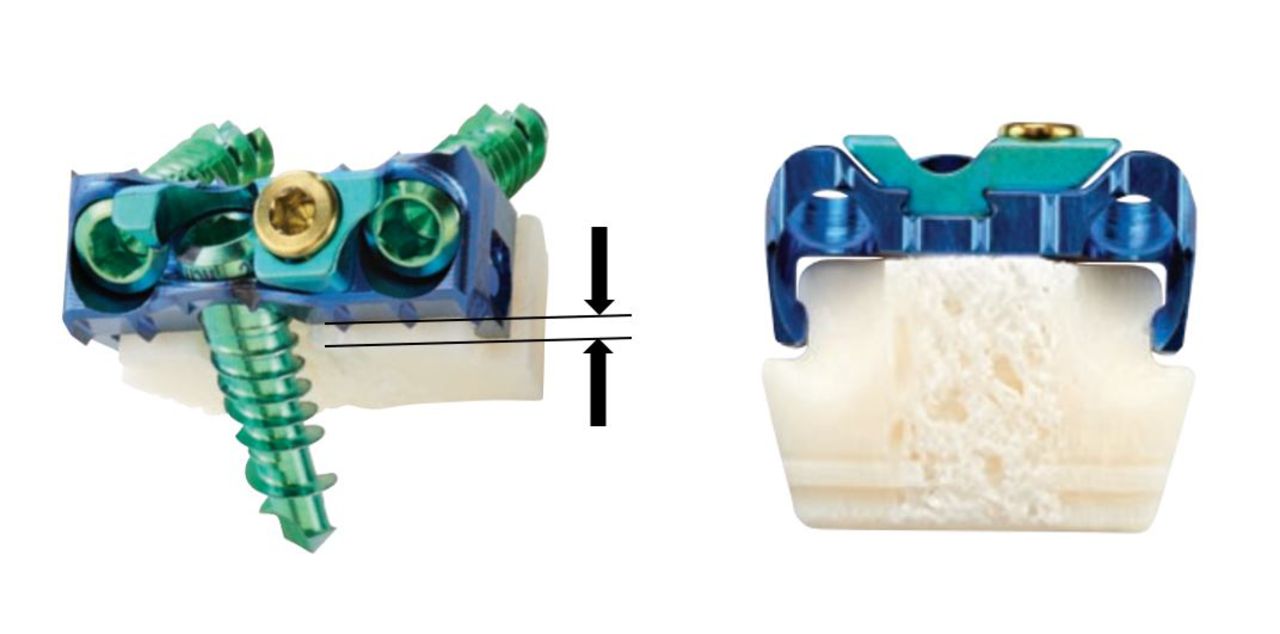
Accordingly, efforts have been made to introduce an integrated and modular ACDF device capable of supporting a machined allograft (corticocancellous, no graft slot) implant body and load-sharing fixation interface (Figure 1). By allowing the implant body to sit slightly pronounced (axially) from the fixation plate, it is intended that the implant face experiences less stress-shielding and more uniform physiological loading (Figure 1). The design differs from traditional no-profile ACDF (npACDF) devices that traditionally possess a continuous (affixed) plate and body design with identical plate and body height. While it is believed that these alternative features may lend to a more optimal fusion environment, it is not yet understood in the literature whether the device provides sufficient early stability in support of mechanical correction and subsequent pain reduction. The objective of this study was to (1) biomechanically (in vitro) assess segmental range-of-motion (ROM) reduction with the connected allograft device in comparison to traditional techniques and (2) clinically evaluate device performance in single-level degenerative patients via a retrospective case series. To date, no study has characterized the aforementioned allograft ACDF device in a preclinical or clinical setting.
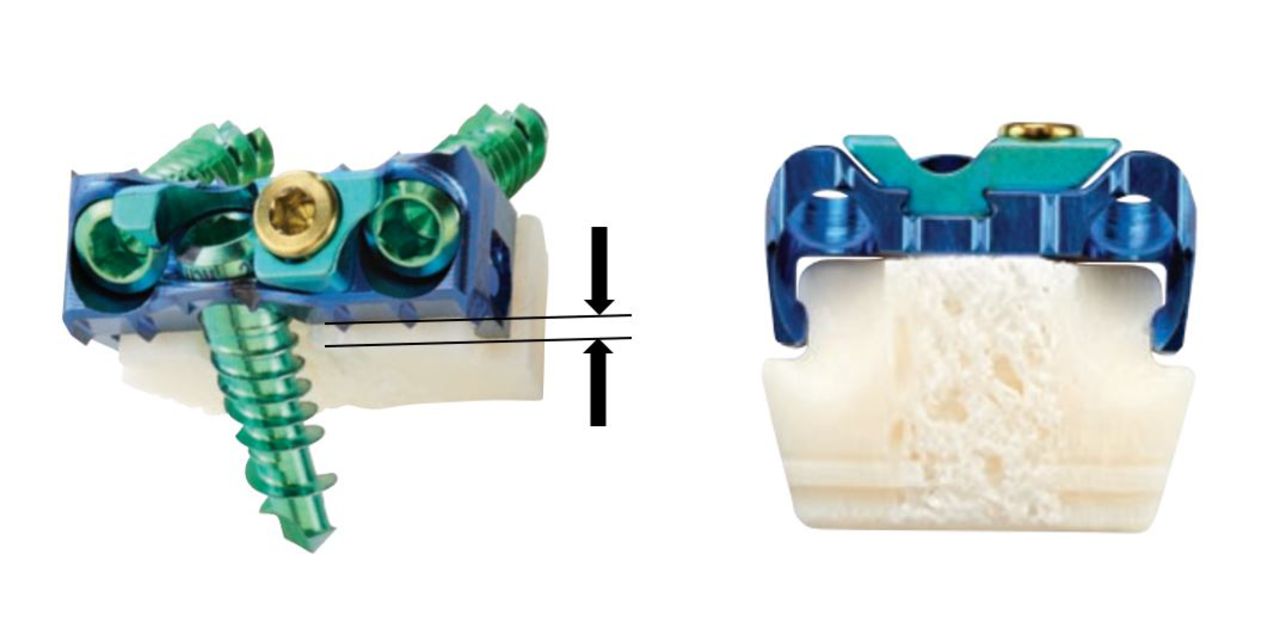
No-profile integrated fixation anterior cervical discectomy and fusion device demonstrating pronounced implant body height relative to plate height (left) and independently connected (nonaffixed) implant body (right).
MATERIALS AND METHODS
Biomechanical Analysis
Specimen Prep
Fifteen (n = 15) fresh-frozen human cadaveric spine specimens were obtained (mean age: 59.4 ± 10.7 years). Each spine was thawed at room temperature, and the cervicothoracic specimens were dissected out. Specimens were then carefully dissected such that the C4-5 and C6-7 motion segments could be isolated. Ligamentous structures were maintained. Residual musculature and adipose tissue were removed. Any specimens exhibiting previous surgery or anatomical discrepancy were excluded. Bone mineral density (BMD) evaluations were performed by dual-energy x-ray absorptiometry scans. The terminal ends of each specimen were potted for subsequent test apparatus attachment using standard drywall screws placed in the vertebral bodies and anchored within high-strength resin (Smooth-Cast 300, Smooth-On; Easton, PA, USA). Of note, terminal C3 and C8 vertebral bodies were left intact such that they could be completely submerged within the potting resin. This allows for less specimen manipulation during preparation and greater surface area for resin adherence. No segmental motion was possible at these levels given full submergence of vertebral body and disc space in the resin. The specimens were sealed in plastic bags and maintained frozen at –20°C until approximately 12 h before testing, at which time they were thawed at room temperature (~25oC). Prior to testing, specimens were divided into 4 equal groups (n = 6). Mean BMD values for each group were comparable (0.8 ± 0.1 g/cm2), and no group shared more than 3 segments from the same donor. Prior to device instrumentation and testing, specimens were instrumented with optoelectronic triad markers in each vertebral body. Marker screw placement was performed such that construct screw trajectories would be uninhibited. The vertebral bodies were assumed to be rigid.
Specimen Instrumentation and Testing
Each specimen would be subjected to pure moment loading; first in its native intact condition, then following a standard anterior discectomy and fixation with one of the following 4 iterations:
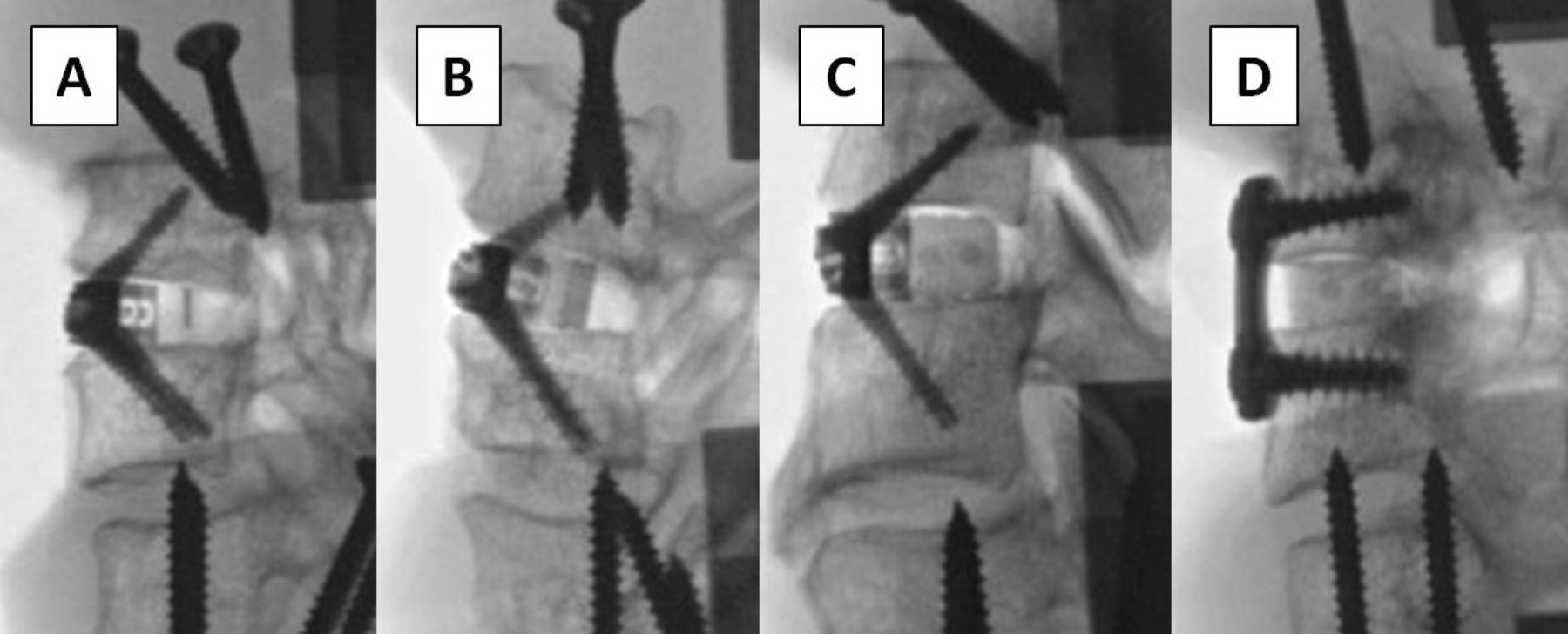
npACDF device with connected polyetheretherketone (PEEK) implant body (“no profile plate [NPP] + cPEEK”) (n = 6) (Figure 2A)
npACDF device with connected allograft implant body (“NPP+ cAllograft”) (n = 6) (Figure 2B)
npACDF device with nonconnected allograft implant body (“NPP + ncAllograft”) (n = 6) (Figure 2C)
Standard anterior ACDF plate and PEEK interbody cage (“TP+ Allograft Cage”) (n = 6) (Figure 2D)
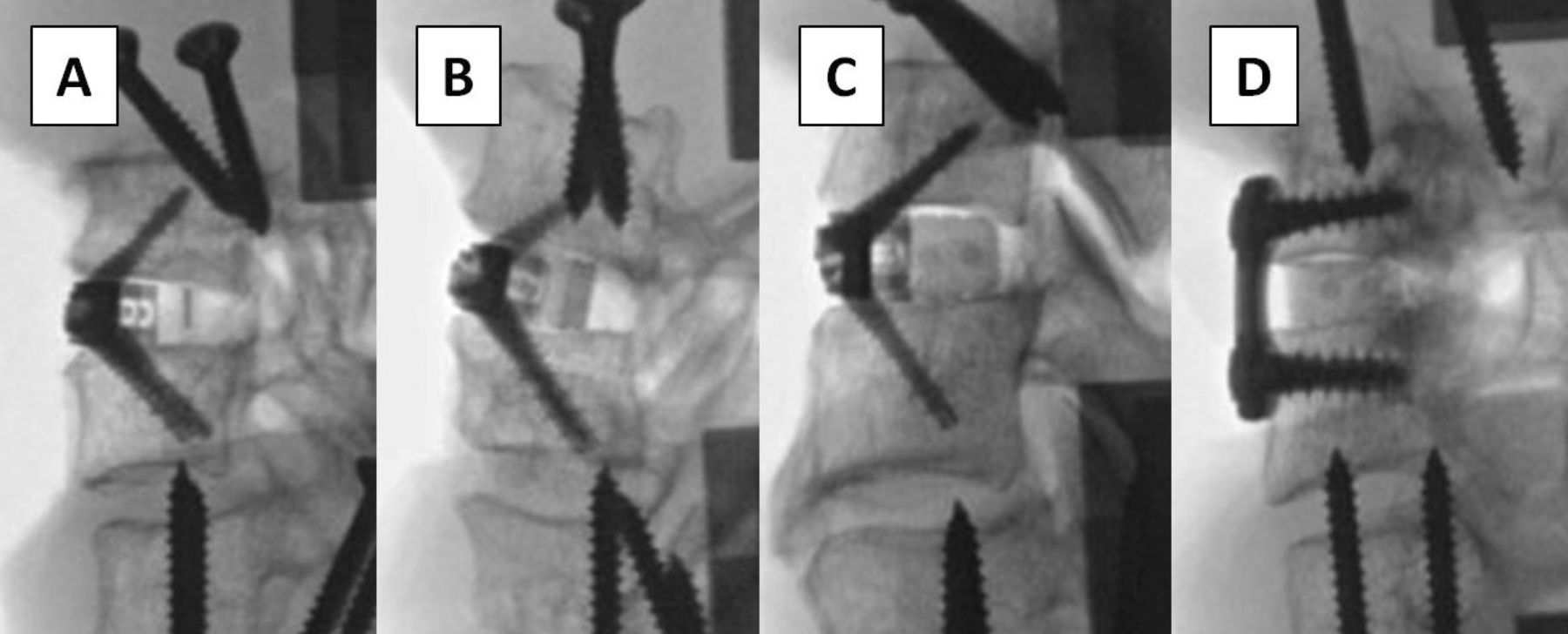
Fluoroscopic images of instrumented test specimens. (A) No-profile anterior cervical discectomy and fusion (npACDF) device with connected polyetheretherketone (PEEK) implant body. (B) npACDF device with connected allograft implant body. (C) npACDF device with nonconnected allograft implant body. (D) Standard anterior ACDF plate and PEEK interbody cage.
All procedures and instrumentation were performed under fluoroscopic guidance by a board certified, fellowship-trained, spine surgeon in a clinically representative manor. All implants were selected specific to specimen anatomy. An anterior annulotomy sized to the width of the interbody device was created, and the disc space was thoroughly denucleated. When necessary, the surgeon removed bone from the anterior endplate to reduce endplate concavity using a high speed burr. Implant trials were used to determine the appropriate device size, and new implants were then implanted into each specimen. The interbody devices were gently tapped into place, and the integrated screws were inserted (if applicable).
A six degree-of-freedom kinematic testing machine (MTS 858 Mini Bionix, MTS Systems, Eden Prairie, MN, USA) was used to apply nonconstraining, nondestructive, pure moment loading in the 3 principal motion directions. Specimens were mounted within the test apparatus at the terminal pots. The caudal pot attachment afforded translation in the X-Y plane via a translating table. A maximum loading moment of ±2.5 Nm was applied in flexion/extension (FE), left/right lateral bending (LB), and axial rotation (AR) at a rate of 0.25 Nm/s for 3 cycles. The selection of a ±2.5 Nm loading moment was consistent with Wilke et al recommendations for cervical segments below C1-2.6 Smaller loading moments are often seen utilized in ACDF biomechanics studies; however, these studies are traditionally taking repeated measures on the same specimen, creating concern for specimen compromise. A compressive follower load was not used; this was done to assess device performance within a “worst” case environment. Furthermore, as demonstrated by Dreischarf et al, nonoptimized follower paths and poorly defined starting conditions can diminish the comparability of studies.7
Three-dimensional motion of each vertebral body was recorded, in all cycles, using an optoelectronic motion measurement system (MX F20 cameras, Vicon, Oxford, UK). Each optoelectronic triad maker was coupled to its respective level to establish a local coordinate system. Additionally, 2 optoelectronic markers were rigidly attached to the static test frame to define the +X and +Y axis’s, and subsequently the +Z axis. Data acquired during the third test cycle were used for statistical analyses, as recommended by Wilke et al.6 Euler angle calculations were performed in the R y, R z, R x order to quantify specimen ROM. ROM reduction relative to intact conditions was subsequently determined.
Statistical Analysis
Iterative instrumented ROM was normalized to intact conditions and pairwise comparisons were then performed between respective conditions using an ordinary 1-way analysis of variance (ANOVA) with Bonferroni’s correction for multiple comparisons. Significance was established at P < 0.05.
Clinical Case Series
A retrospective review (n = 10) of prospectively collected data was performed at a single institution. Institutional review board (IRB) approval was obtained (Western IRB, Puyallup, WA, USA), and informed consent was obtained from all study participants. All patients received single-level ACDF with the connected allograft ACDF device for the treatment of persistent cervical radiculopathy or myelopathy. Patients were excluded from the study if they had symptomatic cervical pathology involving multiple levels or other pathology not isolated to the cervical spine. Further exclusion criteria included prior cervical spine surgery and participation in a worker’s compensation program.
Patients underwent follow-up evaluation at approximately 2 weeks, 6 weeks, 12 weeks, 6 months, and 12 months postoperatively. Patient reported visual analog scale (VAS) and neck disability index (NDI) scores were collected. Any complications and secondary surgical interventions were also reported. At 12 months, plain lateral FE radiographs were obtained and evaluated by an independent radiologist for evidence of fusion. As previously reported by Park et al, fusion was assessed by examination of trabecular continuity, bone bridging across the disc space at the anterior and/or posterior cortex, and a hazy interface between the cage and the vertebral endplate.8 If there was less than 2 degrees of motion at the fusion site or less than 2 mm gap in the interspinous distance on the flexion and extension radiographs, stability was assumed. Subsidence was defined as a greater than 3 mm reduction in the interbody height on the immediate postoperative and 1 year follow-up radiographs or when the cage had clearly penetrated the vertebral endplate.9 Statistical analyses were not performed due to the small sample size.
RESULTS
Biomechanical Analysis
ROM outcomes are summarized in Tables 1 and 2 and Figures 3–5.

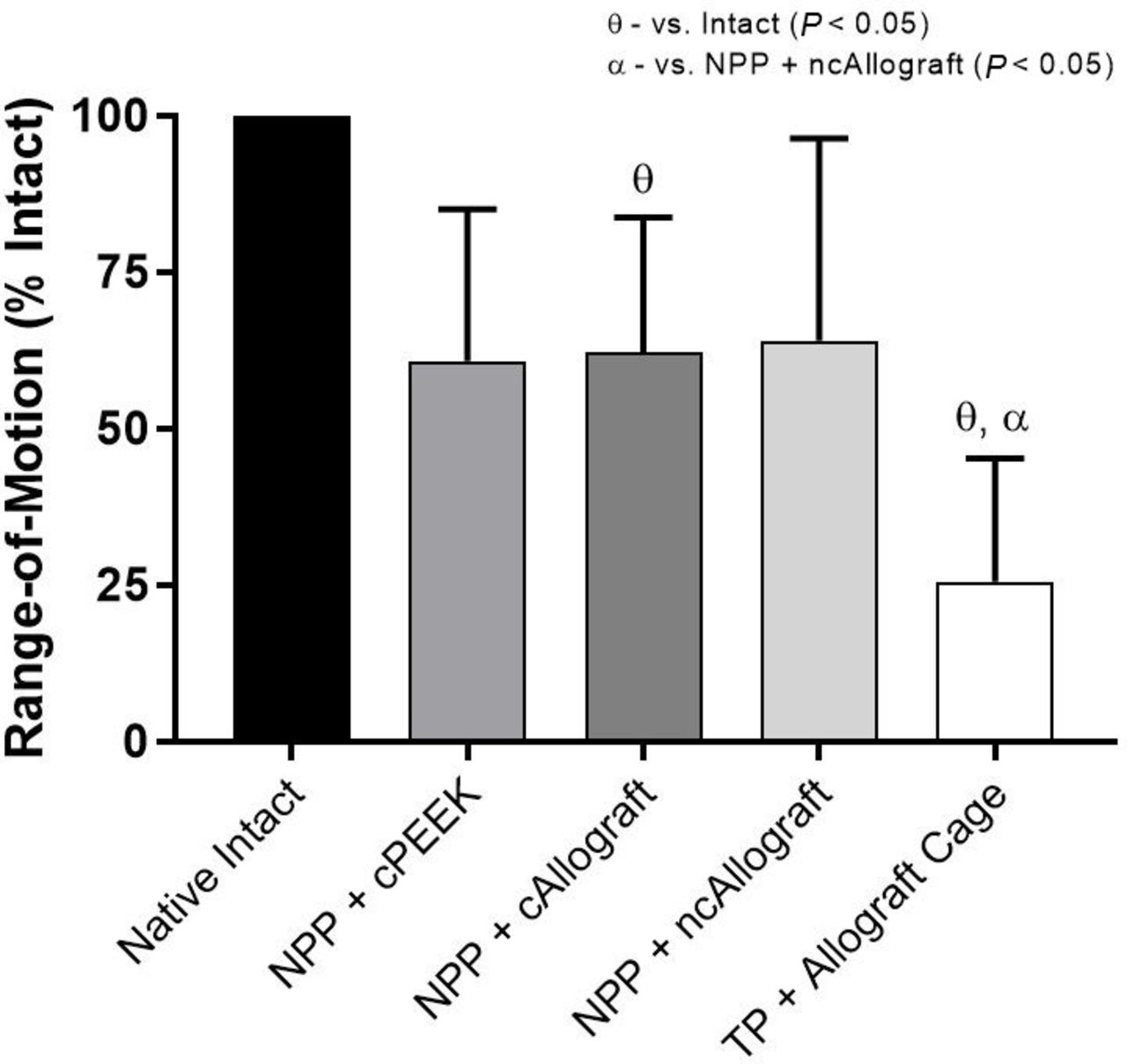
Mean range-of-motion (ROM), relative to intact conditions, when loaded in flexion/extension under a pure moment of ±2.5 Nm. Bars represent the mean, and error bars are SD. Symbols denote significant differences (P < 0.05) between groups according to an ordinary 1-way analysis of variance with Bonferonni’s correction for multiple comparisons; PEEK, polyetheretherketone.

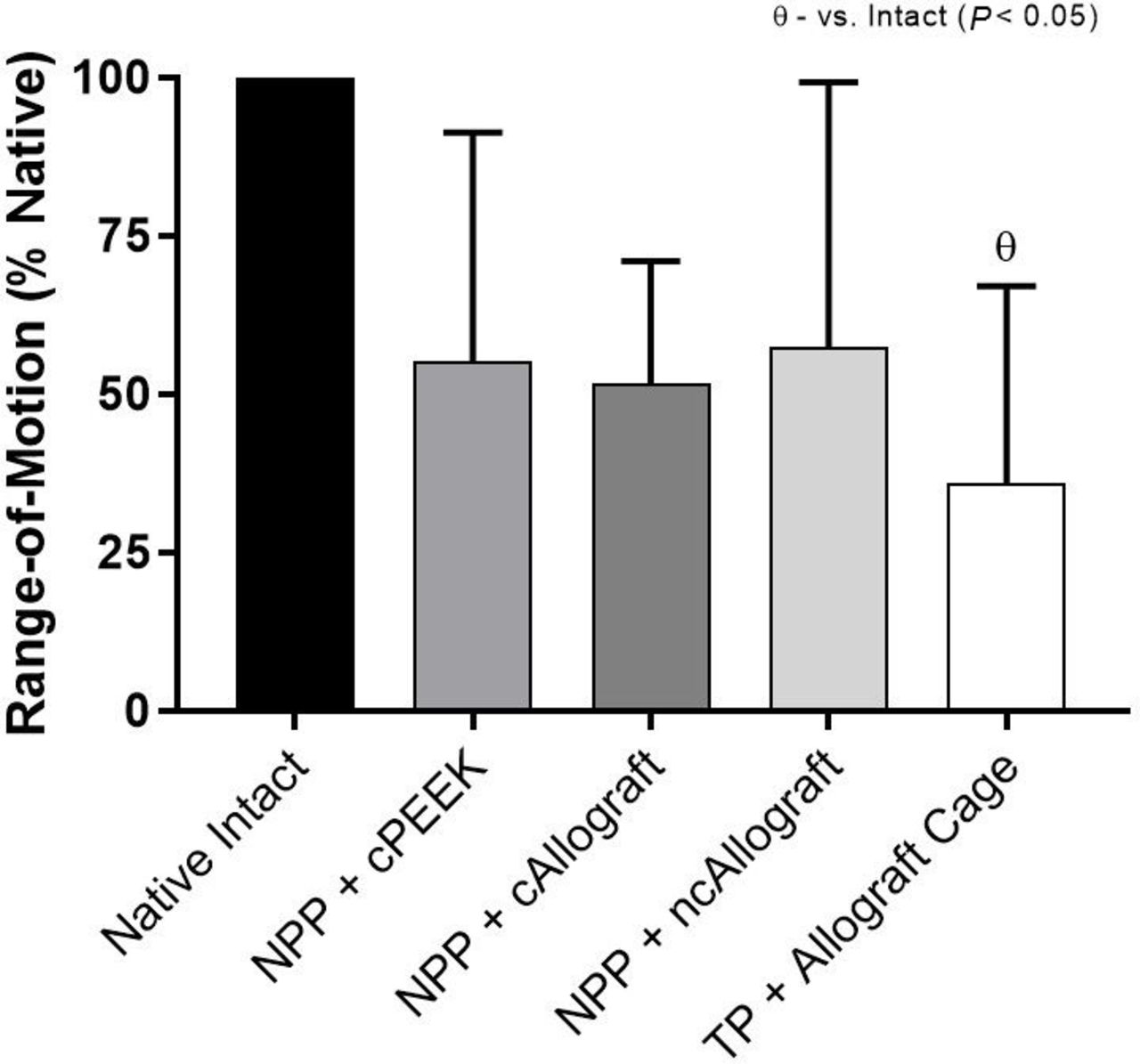
Mean range-of-motion, relative to intact conditions, when loaded in lateral bending under a pure moment of ±2.5 Nm. Bars represent the mean, and error bars are SD. Symbols denote significant differences (P < 0.05) between groups according to an ordinary 1-way analysis of variance with Bonferonni’s correction for multiple comparisons; PEEK, polyetheretherketone.

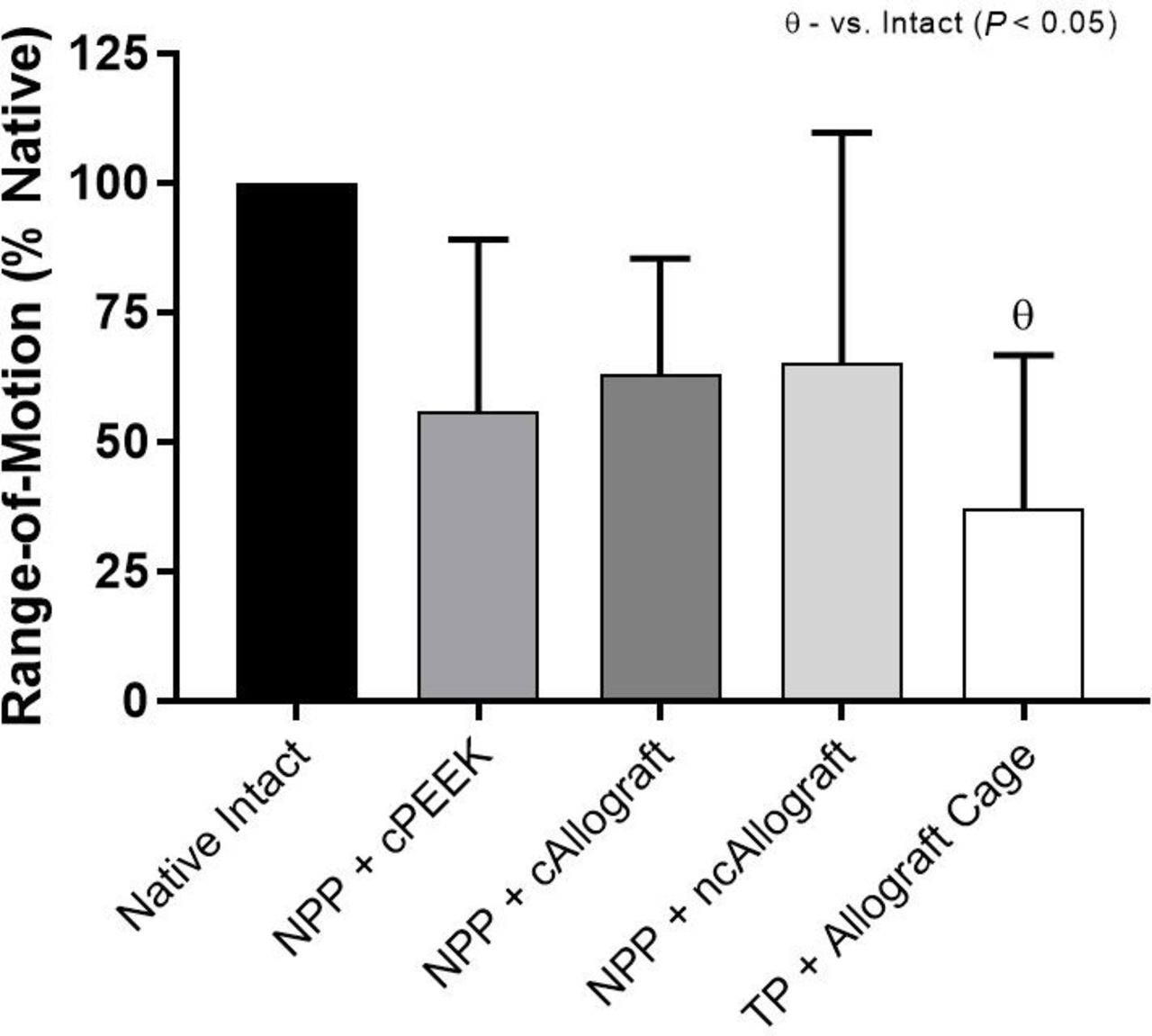
Mean range-of-motion, relative to intact conditions, when loaded in axial rotation under a pure moment of ±2.5 Nm. Bars represent the mean, and error bars are SD. Symbols denote significant differences (P < 0.05) between groups according to an ordinary 1-way analysis of variance with Bonferonni’s correction for multiple comparisons; PEEK, polyetheretherketone.
Raw range-of-motion (ROM) outcomes (degrees).
Normalized (to intact) range-of-motion (ROM) outcomes.
Flexion/Extension
All constructs supported greater than 35% motion reduction from the intact condition; however, only NPP + cAllograft (P = 0.04) and TP + Allograft Cage (P < 0.01) reached significance (Figure 3). No significant differences existed between the no-profile constructs (P ≥ 0.99). TP + Allograft Cage achieved significance over NPP + ncAllograft (P = 0.04) but not NPP + cAllograft (P = 0.06) and NPP+ cPEEK (P = 0.09).
Lateral Bending
All constructs supported greater than 42% motion reduction from the intact condition; however, only TP + Allograft Cage (P < 0.01) reached significance (Figure 4). No significant differences existed between the no-profile constructs (P ≥ 0.99) or in comparison of TP + Allograft Cage with the no-profile constructs (P ≥ 0.71).
Axial Rotation
All constructs supported greater than 34% motion reduction from the intact condition; however, only TP + Allograft Cage (P < 0.01) reached significance (Figure 5). No significant differences existed between the no-profile constructs (P ≥ 0.98) or in comparison of TP + Allograft Cage with the no-profile constructs (P ≥ 0.49).
Clinical Case Series
Patient demographics and outcomes are summarized in Table 3. No intraoperative or postoperative complications (device or procedure related) were observed in any patient. Furthermore, no secondary surgical interventions were performed in relation to the device or procedure.
Patient demographics.
DISCUSSION
A current drawback of integrated npACDF devices is the absence of an allograft implant body option. While direct affixation between implant body and the anterior plate is readily possible with materials such titanium and PEEK, the incorporation of allograft remains challenging given manufacturing and regulatory limitations. Accordingly, a connected npACDF device has been developed in which an allograft implant body is fit to the fixation plate without continuous mechanical locking/affixation. While this helps address the current limitation of allograft usage in npACDF modalities, the noncontinuous design is also believed to improve load sharing/distribution capabilities of the implant body. However, it remains unknown whether the unique fitting/connecting design and variable angle screw features may decrease early mechanical stability and/or potentially predispose the implant to subsidence. The goal of this study was 2-fold: (1) assess in vitro biomechanical stability of the connected no-profile allograft device and 2) characterize initial clinical and radiographic outcomes with the device.
Biomechanical Outcomes
Outcomes observed across the no-profile iterations, including the nonconnected allograft construct, were undifferentiating (P ≥ 0.98). Mean normalized ROM reduction ranged from 36.0% to 39.2% in FE, 43.7% to 48.3% in LB, and 34.8% to 44.2% in AR. Despite what appeared to be pronounced reductions (≥34%) from native intact conditions in all principle directions, only the connected allograft construct achieved significance in FE (P = 0.04). However, such similarities between the nonconnected and connected allograft constructs is particularly notable, as it indicates that fitting of the anterior plate to the implant body provides little, if none/less, added stability. The implication of this finding isn’t entirely explicit; however, it does provoke several mechanical and clinical considerations: (1) When fitted, is micro-motion or translation permitted at the plate/body interface such that the connected design actually holds no further stabilizing implication? (2) When not fitted/connected, does the increased distance (although modest) between plate and implant body induce a moment arm that may improve stability? (3) Could the unconnected no-profile technique allow surgeons to place the cage further posterior without concern for screw angulation obstruction or need for traditional anterior plating? (4) Does the unconnected technique come with any additional risk of subsidence or cage migration?
It is challenging to come to definitive conclusions around the first consideration, which is to what extent the fitted plate/body interface has structural stabilizing implications. However, while no study to date has assessed a connected or fitted integrated ACDF device; multiple studies have examined differences between no-profile devices possessing fixed angle and variable angle screws. While these comparisons are certainly not directly correlating to this study, they do introduce the question as to whether less device rigidity results in less segmental stability. Reis et al assessing the stability of a 2-screw (variable angle) integrated ACDF device, reported mean ROM reductions of 49% (flexion), 44% (extension), 29% (LB), and 44% (AR), of which the outcomes in extension and AR were significantly less (P ≤ 0.01) than those demonstrated with a 4-screw (fixed angle) integrated device in the same study.10 Similarly, Wojewnik et al also comparing the same 2-screw (variable angle) and 4-screw (fixed angle) ACDF devices, noted markedly more ROM reduction with the latter.11 ROM reduction outcomes observed with the 2-screw device were 45.0% (FE), 67.5% (LB), and 47.7% (AR), while outcomes with the 4-screw device were 75.3% (FE), 84.5% (LB), and 77.3% (AR), respectively. Delineating the exact reason why ROM reduction is less with the variable angle devices is confounded by differences in number of screws; however, it can be asserted that nonconstrained screws introduce less stability than those that are fixed. However, a key consideration of ROM reduction is the clinical implication. If clinically meaningful reduction (ie, supports fusion, improved patient reported outcomes) is achieved, relative reduction is of less consequence. As substantiated by Dong et al, fusion rates between no-profile and traditional plated ACDF are not significantly different, despite plated constructs supporting greater relative ROM reduction.4 Furthermore, Dong et al demonstrated that patient reported outcomes scores (ie, NDI, VAS) were also not significantly different between no-profile and traditional plated ACDF techniques.4 These trends bring into question whether a clinically meaningful threshold for segmental ROM exists, after which point outcomes are not further influenced. For example, Tian et al, comparing cervical disc replacement to traditional ACDF, found that segmental ROM was significantly reduced postoperatively in ACDF, while arthroplasty patients experienced a nonsignificant change in ROM from preoperative to 6-month follow-up (mean 6-month ROM: 6.6o ± 4.1o).12 Despite this difference in ROM between techniques, follow-up Japanese Orthopaedic Association and NDI scores were not significantly differing.12 In the current study, all construct iterations permitted <4o of motion following instrumentation (in all motion planes). Extrapolation between preclinical and clinical performance is not appropriate; however, it emphasizes a need for corroborative clinical evidence to understand the clinical significance of raw ROM and ROM reduction.
Again, while extrapolation of outcomes in the current study is challenging, they do indicate that a less constrained device can result in less overall stability. Accordingly, the fitted design of the device examined in this study, coupled with variable angle screws, may explain ROM reductions that trend lower than those reported in the literature with other no-profile integrated devices. Furthermore, it also suggests that while the fitted design lends to a continuous device, the load sharing interface may not possess any additional structural benefit; however, it aids in maintaining device placement and permits physiological loading of the implant body.
As for future implications of using a no-profile plate with an independent interbody cage, further characterization is needed to determine the impact plate-to-cage distance may have on stability, as well as risk of subsidence or migration. As noted previously, if used effectively with proper consideration of mechanical factors, the no-profile plate may afford more posterior placement of the interbody cage without concern of limiting screw trajectories. Furthermore, this may also permit broader usage of interbody cage types while still leveraging a no-profile fixation technique. At best, this study has shown for the first time that an independent no-profile plate can support pronounced ROM reduction from intact conditions, presenting as a differentiated technique in the ACDF surgical space.
Clinical Outcomes
The literature abounds with reports substantiating the perioperative (ie, decreased rates of dysphagia) and long-term radiographic benefits (ie, decreased rates of adjacent level ossification) of no-profile integrated ACDF devices in comparison to traditional plated constructs. However, as this study has shown, as well as many others, no-profile devices typically provide less initial segmental stability, particularly in FE, which often raises concerns about adequate sagittal maintenance/correction and interbody fusion potential. While several studies have shown that when utilized in the proper patient these devices can provide advantageous correction and fusion, integrated no-profile devices, as with any ACDF technique, are far from a one-size-fits-all modality and should be adopted in a progressive and conservative fashion.4
The aim of the clinical analysis performed within this study was to capture initial outcomes with the connected allograft device in single-level degenerative subjects, with a focus on both clinical and radiographic maintenance/improvement out to 12 months. At 12 months, all patients demonstrated interbody fusion, with 1 patient (10%) exhibiting subsidence. These outcomes coincide with the ACDF literature at-large, as a meta-analysis by Fraser and Härtl et al reported single-level ACDF fusion at 97.1%, while a systematic review of ACDF subsidence rates by Karikari et al reported a mean subsidence rate (irrespective of criteria) of 31.4% in plated patients.13,14 Extrapolation of outcomes in the current study for comparative purposes is limited by the small sample size; however, the trends observed do encourage the idea that despite the less pronounced ROM reduction observed in the biomechanical analysis, robust mechanical and fusion outcomes were achieved by just 12 months.
Additional npACDF device literature has also substantiated this dynamic in which lesser baseline stability has not correlated with diminished radiographic (ie, fusion and subsidence) outcomes in comparison to traditional plated ACDF. A meta-analysis by Dong et al, assessing comparative studies of no-profile vs traditional ACDF constructs, reported no significant differences in fusion rate between cohorts (P = 0.76).4 However, the same meta-analysis substantiated the no-profile technique in exhibiting significantly less operative time (P < 0.01) and blood loss (P < 0.01), as well as less significantly less dysphagia early postoperatively (≤6 weeks; P < 0.01) and at last follow-up (P < 0.01). Nemoto et al, comparing a two-screw npACDF device vs traditional plated ACDF, reported no difference in 24-month subsidence rates (16.7% vs 13.6 %; P = 0.71), as well as change in sagittal segmental alignment (P = 0.15) and sagittal alignment of the cervical spine (P = 0.12).15 Similarly, Shin et al, comparing no-profile vs traditional plated ACDF, found no significant relationship in subsidence rate (50% vs 45%; P = 0.76) at last follow-up (range: 12–15 months).16 Mean change in segmental kyphotic angle (P = 0.06) and overall kyphotic angle (P = 0.12) were also not significantly differing between groups. Again, extrapolation of current study outcomes to the literature at-large is limited by the sample size; however, consistency in trends supports and warrants furthered data collection with the connected no-profile allograft technique.
Study Limitations
Limitations of the biomechanical assessment included use of a single individual specimen (FSU) for each test iteration. This was done to ensure uncompromised bone quality due to performing multiple fixations on the same vertebral body. However, a repeated measures analysis was not possible. The effects of this limitation were marginalized as much as possible by ensuring consistent bone quality across all specimens and using a randomized allocation sequence in determining groups. Small sample size (n = 6/iteration) is a limitation of this study. While this is consistent with the minimum recommendation of Wilke et al, it does bring into question the power of the statistical analyses.6 Normalization of iterative ROM to intact conditions was performed to reduce variability, as recommended by Wilke et al.6 However, mean raw data outcomes (Table 1) have been provided to give full context to device performance. Additionally, the specimen model did not account for degenerative changes or instability. While this was done to ensure consistency across specimens, future work may be warranted in which these variables are incorporated.
Limitations of the clinical case series included the small sample size, lack of a comparative cohort, and short follow-up period. Longer follow-up will be telling in characterizing adjacent segment disease and outcome longevity. However, the purpose of the case series was to provide descriptive anecdotal evidence in support of the biomechanical analysis, as well as to encourage a conservative and small-scale introduction of a connected allograft ACDF technique. Outcomes should be considered accordingly.
CONCLUSION
An npACDF device possessing an allograft implant body and connected implant interface may offer capabilities not yet leveraged within the npACDF surgical space. As with other npACDF devices, the connected device does not match mechanical stability of a traditional plate construct; however, reduction in ROM appears clinically robust, as it supported advantageous radiographic fusion and subsidence rates through 12 months, as demonstrated in the clinical case series. Further biomechanical assessment of the connected device with the no-profile plate not connected to the implant body is warranted it understanding its utility. Additionally, larger, long-term follow-up of the current clinical outcomes cohort is needed to adequately compare outcomes to the literature at-large.
Footnotes
Funding This study was funded by Zimmer Biomet Spine.
Financial Disclosures and Conflicting Interests Zimmer Biomet Spine (funding source) manufactures one or more of the devices examined in this study. One author (AG) is a salaried employee (research scientist) of the funding source. Two employees (CF, GK) were previously salaried employees of the funding source, but no longer hold a financial relationship with the funding source. Two authors (NS, CY) have received travel & lodging fees from the funding source, related to business purposes. One author (RD) has received royalties, consulting fees, and travel & lodging fees from the funding source. All hands-on testing and data collection were performed at a facility independent of the funding source. Compensation for said work was not contingent on device performance and/or study outcome.
Disclosure The authors report no financial disclosures related to this article.
IRB Approval IRB Approval was obtained from Western IRB (Puyallup, WA, USA)
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.