


Abstract
Background Osteoporotic compression fractures often progress to neurological impairment and severe pain, which results in restriction of mobility in elderly patients. Conventional open spinal decompression and stabilization in these patients have significant morbidities related to age, surgical approach, and blood loss. This case series evaluates the treatment of osteoporotic compression fractures at the thoracolumbar junction with short-segment stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty using a minimally invasive percutaneous technique.
Methods Eleven patients aged 75 years or older who had osteoporotic vertebral fractures with worsening back pain and neurologic impairment were included in this study. Plain radiographs, magnetic resonance imaging, and computed tomography images of these patients were assessed. These patients underwent minimally invasive percutaneous stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty with or without decompression. Preoperative and postoperative American Spinal Cord Injury Association score, visual analog scale (VAS) score, and Charlson Comorbidity Index were recorded. Cobb angle, spinal alignment, spinal canal encroachment, and anterior vertebral body height were recorded preoperatively and during each follow-up.
Results All patients neurologically recovered, and the VAS score significantly improved from an average of 9 before surgery to 2 immediately after surgery and 1 at final follow-up (P < 0.001). An average, local angle of kyphosis was 15° preoperatively, which decreased to 7° postoperatively (P < 0.01). The average anterior vertebral body height was 11 mm, which increased to 22 mm postoperatively (P < 0.001). No revision was required due to screw loosening or failure of construct.
Conclusion We concluded that patients with osteoporotic vertebral fractures treated with short-segment stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty by minimally invasive percutaneous technique are associated with good clinical outcomes during an average follow-up of 18 months after spinal surgery.
Level of Evidence 4.
- osteoporotic vertebral compression fractures
- cement-augmented fenestrated pedicle screws
- percutaneous stabilization
- vertebroplasty
Introduction
Osteoporosis is currently a major global health issue, one that gets more complicated with a compression fracture of the spine that can severely affect the physical function of elderly patients due to chronic pain and disability. Women and men have a lifetime osteoporotic fracture risk of 40%–50% and 13%–22%, respectively.1 The thoracolumbar region is the foremost location of vertebral fractures.2 About two-thirds of vertebral fractures are asymptomatic, but others are responsible for significant and disabling chronic back pain, disability, kyphotic deformity due to progressive vertebral collapse, painful nonunion, and neurological deficit affecting the function and quality of life of patients.2
The surgical options in these patients with neurological deficits include vertebral column decompression (anterior/posterior) and stabilization. However, considering the age and comorbidities of such patients, these procedures can be rather extensive. Hence, stabilization of the fracture using a minimally invasive technique has been preferred in recent years. Osteoporotic vertebral fractures, if not treated aggressively, will lead to a significant neurologic deficit and nonambulatory status.3–5 Additionally, osteoporotic patients have poor bone quality, which does not provide sufficient strength for common pedicle screws due to low mineral density at the bone-screw interface during internal fixation. Pedicle screw loosening and pullout are the main reasons for internal fixation failure, with an incidence of 0.6%–11%. This can be reduced by improving the pullout strength of the screws.6 Several authors have identified different techniques to increase pullout strength, such as using a thicker and longer screw, improving the design of the screw rod or the screw threads, choosing a proper insertion angle and trajectory, stabilizing the spine with bicortical fixation, and using expandable pedicle screws and bone cement-augmented pedicle screws.2,3,7
The purpose of this study was to evaluate the clinical and radiological outcomes of short-segment minimally invasive percutaneous stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty for the treatment of osteoporotic compression fracture. To the best of our knowledge, published literature in this topic area is lacking.
Materials and Methods
The present study included patients who had osteoporotic vertebral fractures with worsening back pain and neurologic impairment and who underwent minimally invasive stabilization at our institute between January 2016 and December 2019. According to the World Health Organization’s diagnostic criteria, osteoporosis in these patients was diagnosed with a T score of 2.5 from dual-energy x-ray absorptiometry of the lumbar spine.8 Included patients had bone mineral density (BMD) of more than 2.5 SD below the young adult mean (−2.5 SD or less). Patients younger than 75 years , patients with pathological fracture and osteomyelitis, and patients with a near-normal T score for BMD were excluded from the study. Electronic medical records of include patients were evaluated after approval from the ethical committee (IRB No: KDA01276). All patients provided informed consent.
Clinical evaluation was done using visual analog scale (VAS) for pain intensity, and the severity of the neurologic deficits was assessed using American Spinal Cord Injury Association impairment scale. Charlson Comorbidity Index has shown that patients with advanced age are at risk of prolonged hospital stays and postoperative morbidity following an extensive surgical procedure.9 This index was used to assess the medical risk for a more extensive surgery. All patients were nonambulatory due to severe pain and neurologic impairment. For each patient, demographic data, length of stay, and potential complications were also recorded. All patients were evaluated by plain radiographs, computed tomography, and magnetic resonance imaging to determine the morphology of the fracture.
The following parameters were observed to evaluate the correction obtained after the surgical procedure:
Local kyphosis—It was calculated using the Cobb angle between the cranial end plate of the vertebra just proximal to the fracture and the caudal end plate of the vertebra just distal to the fractured vertebrae on lateral plain x-ray films.2,6,10
Retropulsion/Spinal canal encroachment (CE)—The migration of the posterior vertebral elements into the spinal canal was categorized as retropulsion of the vertebral body.1,2,9 Retropulsion further progressed to spinal CE. This was measured as the ratio of the sagittal diameter of the bony fragments into the spinal canal to the sagittal diameter of the spinal canal at one level proximal to the fractured vertebrae. The ratio greater than 25% was considered significant compression leading to varying degrees of neurologic deficits.2,5
Anterior vertebral height (AVH) loss >50%—The AVH of the fractured vertebrae was compared with the normal vertebrae above. This leads to a worsening sagittal profile. The height restored after surgery was also measured.11
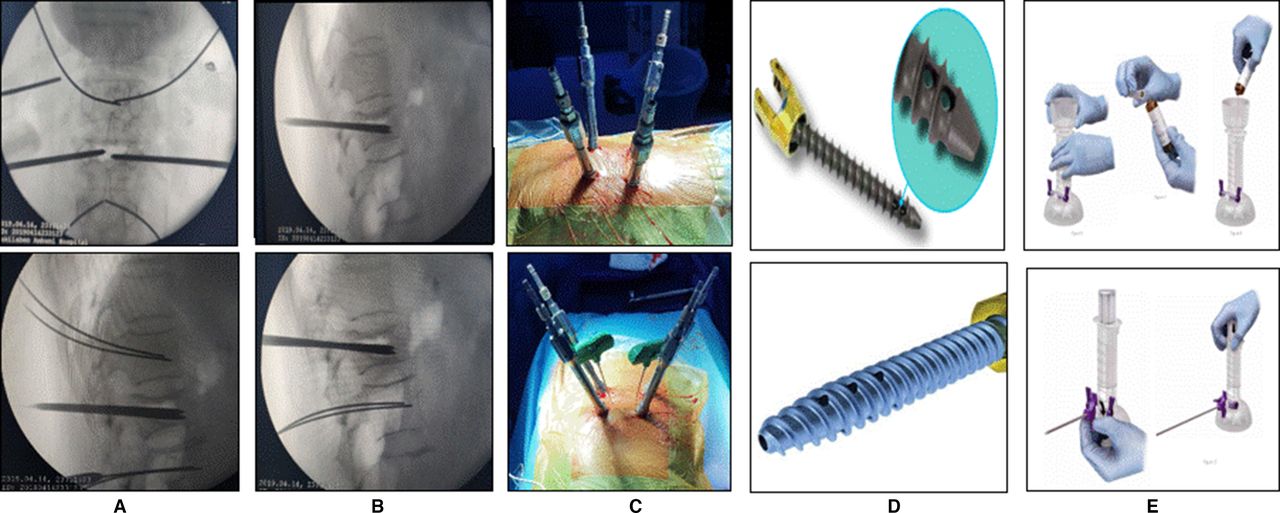
The surgical technique is illustrated in Figure 1. The patient was positioned prone on bolsters. This leads to partial correction of kyphosis and restoration of AVH. First, the pedicles of the affected segment were identified and the skin was marked. The entry points for the percutaneous guide wires were made based on the C arm (Figure 1A). Jamshedi needles were passed into the pedicles after their positions were confirmed on the image intensifier (Figure 1B). Percutaneous fenestrated screws were passed (Figure 1C–D), one level above and one level below the fracture over guide wires. Two vertebroplasty needles were also passed into the fractured vertebra (biportal vertebroplasty). The position of screws and needles was confirmed under C arm. Cement was prepared and loaded into the syringes (Figure 1E). Each fenestrated screw was augmented by 2-mL vertebroplasty cement injected through the connector. Also, about 5–6 mL of vertebroplasty cement was injected into the fractured vertebrae under fluoroscopy until cement reached the posterior one-third of the vertebral body. Once the position of the cement was confirmed, unilateral laminotomy with bilateral (over the top) decompression was done at the level of retropulsion, if necessary. An x-ray lateral view of the vertebrae was performed during the cement injection to observe the distribution of bone cement. Correction of focal kyphosis partially with rods resulted in indirect decompression (Figure 2).

Surgical technique. (A) The entry points for the percutaneous guide wires under C arm. (B) Jamshedi needles were passed into the pedicles at the fractured vertebra. (C, D) Passing of percutaneous fenestrated screws, one level above and one level below the fracture. (E) Cement preparation and filling of syringes.
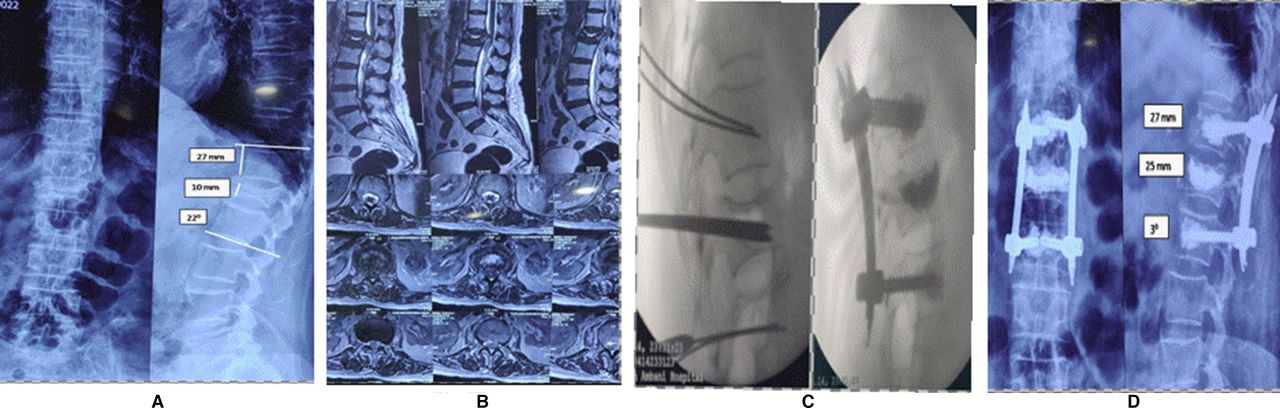
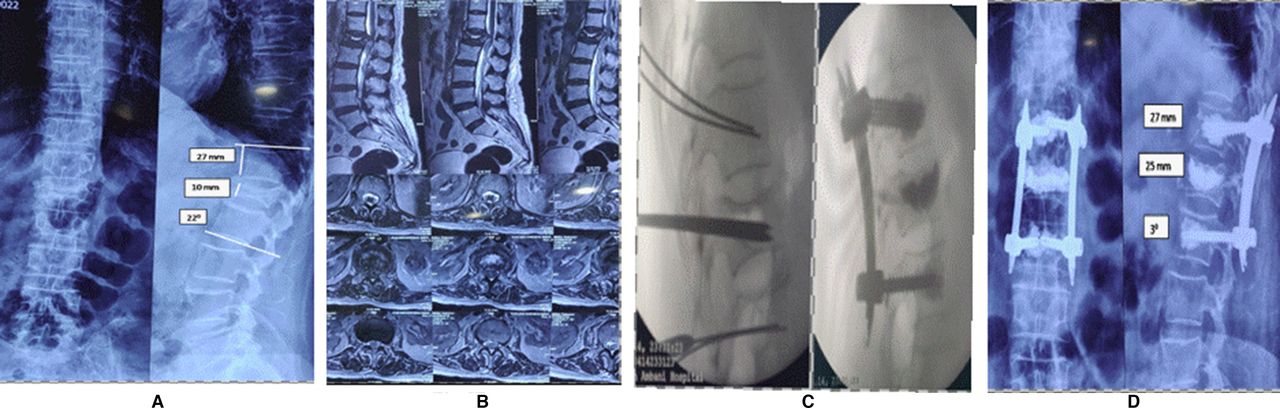
Case 1: A 75 y wheelchair-bound woman with American Spinal Cord Injury Association C neurology with L1 compression fracture. (A, B) Vacuum sign+, local kyphosis of 22°, anterior vertebral height loss of >50%, retropulsion and spinal canal encroachment >25%. (C) Guide wires and biportal vertebroplasty needles placed, and C-arm picture of vertebroplasty and minimally invasive stabilization. (D) Postoperative x-ray of vertebroplasty and minimally invasive stabilization with cement-augmented percutaneous pedicular screws.
The patients were mobilized on postoperative day 1 with braces in the presence of a physiotherapist. Clinical and radiological evaluations were done preoperatively, immediate postoperatively, and at 3-month, 6-month, 1-year, and final follow-up after surgery. Angle of local kyphosis, AVH, and hardware loosening or implant failure were assessed at follow-up.
Statistical Analysis
Comparison of preoperative and postoperative measurements was performed using a paired t test for independent samples. Statistically significant differences were defined at a 95% confidence level. The values were given as mean ± SD. The SPSS software was used for statistical evaluation.
Results
Patient Demographics and Clinical Data
Out of 30 patients, 11 patients who underwent minimally invasive percutaneous technique stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty were included in the study. Electronic medical records of these 11 patients were evaluated clinically as shown in Table 1. The most common level involved was D12 followed by L1. These patients had failed an average conservative trial of 9 weeks (range 8–14 weeks) before they presented to us with neurodeficit. There were 4 men and 7 women with a mean age of 78.5 years (range 75–84 years). The average duration of surgery was 130 minutes (110–180 minutes), and the mean blood loss was 80 mL (range 60–300 mL). The mean follow-up was 18 months (range 12–24 months), and the average hospital stay was 4 days (3–8 days). The average Charlson Comorbidity Index was 6 (range 5–8).
Demographic data and clinical parameters of 11 patients.
Radiological Parameters
Radiological data of 11 patients are shown in Table 2.
Radiological parameters of 11 patients.
Clinical Outcome
There were no reported perioperative complications related to cement injection, such as intraoperative hypoxia, hypotension, pulmonary embolization, myocardial infarction, neurovascular or viscera injury, or death. Three patients had asymptomatic minimal cement extravasation anteriorly, laterally, or in the intraspinal region (Figure 3). The VAS score significantly decreased from a mean preoperative of 9 (range 7–10) to 2 (range, 1–4) immediately after surgery and 1 (range 0–1) at final follow-up (P < 0.001). The average local angle of kyphosis was 15° preoperatively (range 0–30°), which decreased to 7° postoperatively (range 0–15°) (P < 0.001). No loosening of implants or loss of reduction had occurred. The average anterior vertebral body height was 11 mm, which increased to 22 mm postoperatively (P < 0.001). The correction in kyphosis and AVH was stable at a mean follow-up of 18 months.

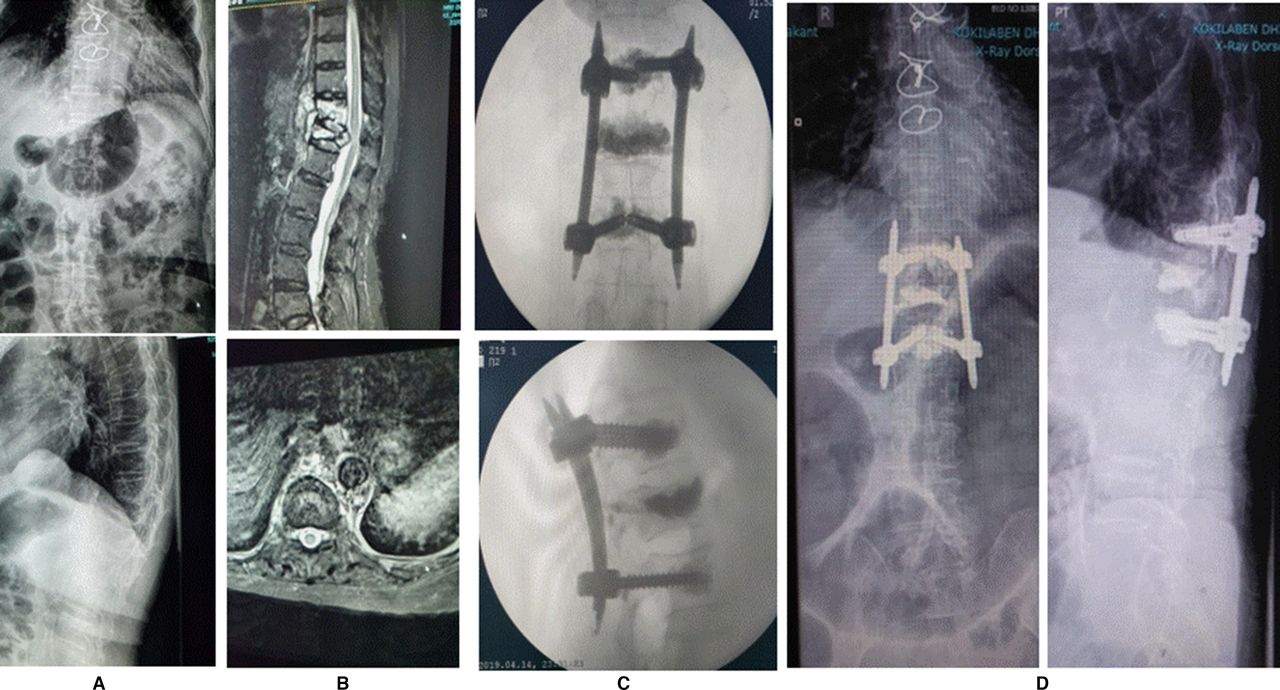
Case 2: An 84 y woman post-cornonary artery bypass grafting status with D12 compression fracture with American Spinal Cord Injury Association C neurology. (A) An x-ray showing D12 compression fracture with collapse. (B) Magnetic resonance imaging showing D12 compression fracture with collapse and retropulsion with D11 edema. (C) C-arm picture of short-segment fixation with vertebroplasty with minimal cement leakage. (D) Postoperative x-ray showing stable short-segment fixation with D12 vertebroplasty.
Discussion
Osteoporotic vertebral fractures often result in debilitating pain, functional decline, and reduced quality of life, necessitating prolonged bedrest and higher risk of complications, which lead to an increase in morbidity and mortality.3,12 Severe osteoporosis was categorized if the patient had a BMD of <2.5 SD below young adult and had one or more osteoporotic fractures.13 Management of severe osteoporotic thoracolumbar junctional fractures remains a challenge for spine surgeons. Thoracolumbar junctional fractures have dynamic instability with hypermobility at the fractured level. This leads to gradual retropulsion of bony fragments into the spinal canal, which causes neurological impairment. To decrease these operative risks, various techniques have been described. In recent years, percutaneous spine surgery has become increasingly popular as it decreases surgical time, blood loss, and infection rates. The objectives of these minimally invasive procedures are to limit muscular damages, decrease postoperative pain, decrease length of stay, and accelerate postoperative recovery. The vertebroplasty technique stabilizes the anterior column and has an analgesic effect, and fixation provides stabilization to the middle and posterior columns.1 However, mechanical failures of implants, chances of pseudarthrosis, and screw pullout or loosening are much higher in patients with poor bone stock due to poor screw interface. To minimize this, fenestrated screws are used with cement augmentation, though one of the limits of these augmented screws is a high risk of cement leakage that may be associated with a nonacceptable neurologic risk.14 Recent development of partially fenestrated screws is one of the solutions to these risks as it allows a cement injection in distal one-third of the screw, increasing the pullout strength with a reduced risk of leakage.15–18 Recent studies have reported satisfactory results for these fenestrated screws in terms of fixation strength and fewer complications.10,11,19,20
In the current study, most of the patients had CE, angular kyphosis, and instability of the middle and posterior column, for whom vertebral column resection and stabilization would be one option in treatment.12,21 Considering the age of the patients and the morbidity of the procedure, we decided to treat with minimally invasive stabilization and anterior column support by vertebroplasty. In this study, the fracture was reduced partially by placing the patient prone on bolsters and partially by proper distraction applied between 2 screws as necessary before vertebroplasty. Hydroxyapatite vertebroplasty cement was used in all patients. If the CE was greater than 50%, then bilateral decompression with unilateral laminotomy was done to preserve the midline structures; however, reconstruction of the anterior spinal column was not attempted. This procedure is less morbid and well tolerated in the elderly population. Correction of kyphosis and fairly good restoration of AVH resulted in indirect decompression and vertebroplasty leading to anterior column support. In the present study, symptomatic relief, functional improvement in terms of VAS, and improvement in neurology were observed after surgery in all the patients. The radiological images on follow-up revealed no implant loosening and no worsening of local kyphosis. None of our patients had any complications, which is in line with M. Abdelaziz’s study.22Amendola et al reported bone cement leakage occurred in 1 patient out of 21 cases, with bone softening treated with a fenestrated pedicle screw augmented with cement, causing transitory nerve root palsy, which was attributed to injecting an excessive amount of cement (>3 mL) and another case of leakage that resulted in an interruption in the screw insertion.23 However, none of our patients had symptomatic cement leakage as fenestrated part of screws located in the anterior one-third of the vertebral body. Amendola et al10 also advised no more than 2 mL of polymethyl methacrylate (PMMA) should be injected under continuous fluoroscopic monitoring, ceasing injection if leakage occurs. This aligns with our study regarding injection amount in the lower thoracic region. However, in the lumbar spine, we injected 2.5 mL with no complications as leakage; this is in line with Folsch et al that results of cement volume should be kept to the smallest volume needed and should not exceed 2.8 mL per pedicle screw.24 This was attributed to the strict adherence to the company recommendation about the cement injection time that never injects the cement before a doughy stage or attainment of spaghetti consistency. The risk of PMMA extravasation ranged between 27% and 74% in various series causing radiculopathy and cord compression in 3.7% and 0.5%, respectively.5,23,25
Our study is consistent with other studies that have shown that PMMA cement augmentation of pedicle screws increases fixation strength in severely osteoporotic bone.26,27 Unlike the traditional midline incision, the Wiltse approach avoids disruption of the supraspinous and interspinous ligaments and evades detachment of muscle from bone. It also provides a more direct approach to the transverse processes, and pedicles ultimately reduce bleeding and postoperative pain.28,29 A similar technique was used by Gu et al and resulted in the following: mean duration of the operation was 82 minutes (range 67–91 minutes), mean blood loss was 77.2 mL (range 61.3–93.1 mL), and mean stay in the hospital was 5.3 days (range 4–7 days).7 The pain intensity level on the VAS dropped significantly from 7.3 ± 1.3 preoperatively to 1.2 ± 0.7 (P < 0.001) immediately after the operation and 0.7 ± 0.7 (P < 0.001) at final follow-up. Our results are almost similar to this study.
Sudo et al retrospectively compared surgical outcomes of anterior decompression and strut graft vs posterior decompression and pedicle screw fixation with vertebroplasty for osteoporotic thoracolumbar vertebral collapse. They observed significantly lower blood loss intraoperatively in the posterior group, and perioperative respiratory complications were found in 34% in the anterior group. In the anterior group, early posterior reinforcement was needed in 20% to 30% of patients with very low bone density due to progression of a kyphotic deformity or screw loosening within 3 months postoperatively.26 In the current study, patients also had 2 or more medical comorbidities, such as diabetes, history of stroke, myocardial infarction, or dementia. The average Charlson Comorbidity Index was 6, suggestive of a risk of prolonged hospital stay and postoperative morbidity, if extensive anteroposterior decompression was attempted due to complications like long-segment fixations with long surgical times and large amounts of blood loss. Sudo et al’s study also supports our decision to perform short-segment instrumentation with vertebroplasty, leading to less surgical time and blood loss resulting in less morbidities postoperatively and early recovery.26 One of the limitations of our study was the retrospective design. A prospective study would be a better and effective way to see the natural progression of osteoporotic fractures leading to instability. Another limitation was the small sample size. We suggest further studies to compare this technique with percutaneous vertebroplasty groups, percutaneous kyphoplasty groups, and nonsurgically treated controls.
Conclusion
Minimally invasive stabilization with or without local decompression and vertebroplasty is well tolerated in the elderly population with encouraging results. We concluded that short-segment stabilization with cement-augmented fenestrated pedicle screws and vertebroplasty by minimally invasive percutaneous technique is a valuable option for patients with osteoporotic vertebral fractures. This technique is associated with good clinical outcomes, early and safe mobilization, less morbidities, and the absence of obvious complications, such as early and late implant failure.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.