


Abstract
Background Minimally invasive surgery (MIS) has benefits over open surgery for lumbar decompression and/or fusion. Published literature on its cost-effectiveness vs open techniques is mixed.
Objective Systematically review the cost-effectiveness of minimally invasive vs open lumbar spinal surgical decompression, fusion, or discectomy using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Methods A systematic electronic search of databases (MEDLINE, Embase, and Cochrane Library) and a manual search from the cost-effectiveness analysis (CEA) database and National Health Service economic evaluation database was conducted. Studies that included adult populations undergoing surgery for degenerative changes in the lumbar spine (stenosis, radiculopathy, and spondylolisthesis) and reported outcomes of costing analysis, CEA, or incremental cost-effectiveness ratio were included.
Results A total of 17 studies were included. Three studies assessed outcomes of MIS vs open discectomy. All 3 reported statistically significant lower total costs in the MIS, compared with the open group, with similar reported gains in quality-adjusted life years (QALYs). Two studies reported cost differences in MIS vs open laminectomy, with significantly lower total costs attributed to the MIS group. Twelve studies reported findings on the relative direct costs of MIS vs open lumbar fusion. Among those, 3 of the 4 studies comparing single-level MIS-transforaminal lumbar interbody fusion (TLIF) and open TLIF reported lower total costs associated with MIS procedures. Six studies reported cost evaluation of single- and 2-level TLIF procedures. Lower total costs were found in the MIS group compared with the open fusion group in all studies except for the subgroup analysis of 2-level fusions in a single study. Three of these 6 studies reported cost-effectiveness (cost/QALY). MIS fusion was found to be more cost-effective than open fusion in all 3 studies.
Conclusion The studies reviewed were of poor to moderate methodological quality. Generally, studies reported a reduced cost associated with MIS vs open surgery and suggested better cost-effectiveness, particularly in MIS vs open single- and 2-level TLIF procedure. Most studies had a high risk of bias. Therefore, this review was unable to conclusively recommend MIS over open surgery from a cost-effectiveness perspective.
Clinical Relevance The incidence of spinal decompressive and fusion surgey and financial constraints on healthcare services continue to increase. This study aims to identify the cost and clinical effectiveness of common approaches to spinal surgery.
Level of Evidence 3a.
- minimally invasive
- minimal access surgery
- lumbar spine
- discectomy
- cost
- cost-utility
- cost-effectiveness
- cost-minimization
- systematic review
- QUALY
- QALY
- quality-adjusted life year
Introduction
Direct and indirect spinal decompression are established surgical treatments of central, lateral recess and foraminal stenosis in the lumbar spine. Central stenosis typically causes neurogenic claudication, although radicular complaints are also possible. Radiculopathy from nerve root impingement can cause pain, weakness, and sensory symptoms.1 The incidence of both conditions is increasing with the aging population. Outcomes have traditionally been measured by pain or patient-reported outcome scores.
Spinal surgery is a significant financial cost for health services.2 The clinical effectiveness of both laminectomy and discectomy has been extensively described in the literature.3,4 Modern budgetary constraints have led to an increased emphasis on value-based health care, but the threshold of treatment cost defined as “cost-effective” can vary across health care systems. The cost-effectiveness of the surgical management of lumbar stenosis and degenerative spondylolisthesis has been demonstrated in several settings, most notably from cost-utility data on decompressive surgery for lumbar disc herniation .5 TLIF was first described with the aim of treating radiculopathy, by achieving decompression and circumferential fusion of 2 or more lumbar vertebrae.6
During open posterior lumbar surgery, the paraspinal muscles are detached from their origin/insertion. In contrast, minimally invasive surgery (MIS) aims to minimize muscle injury by using a paraspinal exposure that seeks to split or dilate the muscles to reduce injury. MIS is hypothesized to be associated with better perioperative outcomes, such as lower blood loss, less surgical site infections, and shortened length of hospital stay.7
Prior work reports medium- and longer-term outcomes of MIS and open approaches.8,9 Since the first description of MIS-TLIF in 2003,10 a number of articles have compared clinical effectiveness following open vs MIS lumbar spinal surgery. However, there is an absence of good quality comparative studies.
The present article aims to systematically review cost-effectiveness studies comparing MIS with open surgical procedures in the lumbar spine. Our key question was whether there was evidence of a difference in cost-effectiveness between MIS and open approaches to surgical decompression, discectomy, and fusion procedures in the lumbar spine.
Methods
Systematic Review and Data Collection
The review of literature was performed using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.11
A systematic electronic literature search was performed using the MEDLINE, Embase, PubMed, and the Cochrane Library (1 September 2020) to identify studies on the cost-effectiveness of open vs minimally invasive lumbar discectomy, decompressions, and/or fusions. Two reviewers (K.E. and U.O.) screened study titles, abstracts, and full text articles to identify appropriate studies (Figure 1).

Study selection flow chart of the results of systematic literature review for identification of included studies.
The cost-effectiveness analysis (CEA) registry database (Tufts Medical Center, Institute for Clinical Research and Health Policy) and the National Health Service economic evaluation database were also manually searched using the following keywords:
Medical subject headings: “minimal access”/“minimally invasive” and “lumbar spine”/“lumbar vertebra” or “fusion”/“surgical procedure”/“decompression”/“laminectomy”/“discectomy”/“diskectomy” and “cost-effectiveness”/“cost-utility”/“cost-benefit”/“QALY”/“QUALY”/“quality adjusted life year”
Potential articles were exported into the Endnote reference manager (Endnote X9, Clarivate Analytics).
Table 1 summarizes the inclusion and exclusion criteria. These were established a priori. Articles were excluded if they were reviews, research methodologies, or did not involve comparison of MIS vs open lumbar spinal surgery.
Summary of inclusion and exclusion criteria.
Definitions
A procedure was considered MIS if it was conducted through a cylindrical soft tissue retractor/sleeve via a muscle dilating approach, through a tube, or endoscopically and described as MIS in the study text.
Outcome Measures
CEA
Cost-utility analysis
Results
Search Results
The electronic database search yielded 454 studies, 72 of which were duplicates). An additional 6 articles were identified by a manual PubMed search. Of these 388 studies, 291 were excluded on citation and abstract review because they failed to meet inclusion criteria. The primary reason for exclusion was a failure to compare direct costs in both the MIS and open surgical groups, or a failure to specify costs or cost-effectiveness data for the conditions of interest. Costing studies were included, even if cost-effectiveness had not been measured. Seventeen studies were selected for final inclusion (Figure 1, Table 2).
Characteristics of included studies.
Study Characteristics
Eight studies (47%) were based on data from retrospective cohorts, 2 (12%) were based on data from decision model analyses, and 7 (41%) were based on prospective cohorts. Of these, only one study was a randomized controlled trial (RCT).13
Length of follow-up ranged from 12 to 60 months but was not reported in 2 (11.8%) of the studies included. All 17 studies assessed the direct cost of MIS vs open surgical management. A total of 1978 patients were analyzed across the included studies (1037 MIS vs 941 open).
Nine studies met the 4 key components for a cost-effectiveness study as described by the US Panel of Cost-Effectiveness in Health and Medicine.29
All 17 studies calculated direct cost, but only 6 (35.2%) reported indirect costs.13,15,17,20,22,27 Age was reported in 14 of the 17 studies (MIS range 37–64 years, open range 42–58 years). Mean age was 53 years in both groups (open and MIS) with no significant difference between the MIS and open groups in any study.
Quality Appraisal and Risk of Bias
The quality of study methodology varied significantly. Risk of bias was assessed using the Dutch Cochrane group checklist. 30(Table 3) All studies in the review were deemed to have clearly defined their outcome assessment, study population, and outcomes. However, all studies (except the RCT) were at high risk of bias due to a lack of double blinding. Three studies were led by the same main author.15,20,22 Study methodology was analyzed using the Quality of Health Economic studies instrument (QHES)31 (Table 4 and Appendix 1). Five studies scored higher than 75 (good) on the QHES scale, while 5 studies scored below 40 (poor) (range 24–79).
Risk of bias assessment.
Study quality assessment—QHES Score.
Appendix 1.
Economic Evaluation of MIS vs Open Surgery in the Lumbar Spine
Discectomy of the Lumbar Spine
Three studies assessed outcomes of MIS vs open discectomy alone.12,13,19 One of these was an RCT from the Netherlands that compared results following MIS (tubular) vs open lumbar discectomy. They reported an 8.8% reduction in total costs in the MIS group compared with the open group and no statistically significant difference in cost-effectiveness (cost per quality adjusted life year) (QALY) ($42,665 [MIS] vs $38,321 [open] [P > 0.05]).13
Cahill et al19 retrospectively reviewed 76 patients undergoing single-level lumbar microdiscectomy in an academic setting (USA). They reported statistically significant lower total costs in the MIS group, compared with the open group with similar reported gain in QALY (clinical effectiveness).
Slotman et al12 analyzed the cost of endoscopic vs open discectomy. They found a significant difference in direct cost between MIS and the open techniques, with a 38.8% reduction (P < 0.01) in direct costs of endoscopic compared with open discectomy.
Hemilaminectomy of the Lumbar Spine
Both costing studies of hemilaminectomy (decompression) for spinal stenosis reported that MIS lumbar decompression had a lower direct cost than open lumbar decompression (19.5% and 60.3% lower) (Table 5).18,20 Interestingly, Parker et al performed a further subgroup analysis on open vs MIS multilevel decompression and found no significant difference in costs or QALY gain (Table 5).20
Summary of economic evaluation.
Fusion of the Lumbar Spine
Twelve studies reported findings on the relative direct costs of MIS vs open lumbar fusion (4 studies evaluated MIS vs open single-level TLIF,15,17,22,27 6 reported single-level and 2-level MIS-TLIF vs single-level and 2-level open TLIF,14,21,24–26,28 and 1 study did not break down the number of levels fused).23 A single study reported posterior lumbar interbody fusion (PLIF) results.16 The quality of methodology varied significantly among these studies, ranging from a QHES of 26 (poor) to 79 (good) (Table 4).
MIS vs Open Single-Level TLIF Procedures
Of the 4 studies evaluating MIS vs open single-level TLIFs, 2 were prospective17,22 and 2 were retrospective CEA.15,27 None of these 4 studies reported a statistically significant difference in clinical effectiveness between MIS and open single-level TLIF. Three of the 4 studies reported a lower total cost of MIS-TLIF compared with that of open TLIF.15,17,22 This reached statistical significance in a single study17 (Table 5). Three of these studies reported a cost/QALY.15,22,27 In 2 of the 3, the total cost was lower in the MIS group than in the open TLIF group.15,22 This was below $100,000/QALY (the acceptability threshold accepted in a number of cost-evaluation studies)32–34 in all studies comparing open and MIS cohorts, except for the open TLIF cohort reported by Parker et al (2012), in which cost/QALY was slightly above this acceptability threshold ($109,090/QALY).22
MIS vs Open 1- and 2-Level TLIF Procedures
Six studies reported cost evaluation of single- and 2-level TLIF procedures.14,21,24–26,28 The quality of the methodology in these studies varied from poor to fair (QHES score: 37–74). Two of these were cost analyses without inclusion of clinical-effectiveness data (1 retrospective and 1 prospective).
Rampersaud et al (2015) published a Canadian retrospective cost-effectiveness study comparing single- and 2-level TLIFs in patients with grade I to II degenerative or isthmic spondylolisthesis (n = 78).25 This study estimated total costs from the perspective of a single national centralized payer. Significantly fewer 2-level TLIF procedures were performed in the MIS group than in the open group, and the baseline Oswestry Disability Index scores were significantly lower in the MIS group than the open TLIF group, indicating some baseline heterogeneity between the groups. This study reported lower total costs, better clinical effectiveness (improvement in QALY), and therefore better cost-effectiveness (lower cost/QALY), in the MIS compared with the open 2-level TLIF groups. The difference in QALY between the 2 groups did not reach statistical significance (MIS 0.113 vs open 0.079, P = 0.08). An incremental cost-effectiveness ratio was not calculated in this case because MIS “dominated” the open TLIF (it was both more clinically effective and less costly than open surgery).
Wang (2011) published an economic evaluation of single- and 2-level open vs MIS-TLIF procedures.16 They found significantly lower costs associated with MIS surgery in the single-level group (n = 59, P = 0.027), but no significant cost difference in 2-level PLIF cases (n = 15, P = 0.07). Maillard et al published a retrospective cost-minimization study from the perspective of direct costs from the provider perspective (France).24 This study found that total costs in the MIS-TLIF group were significantly lower than those in the open TLIF group (21.6%, P < 0.05), with a €1139 hospital “profit” accrued per patient in the MIS group compared with a €620 “loss” per patient in the open group (P = 0.021).24 This profit/loss was calculated from the difference between direct costs and hospital reimbursement. Hospital admission and treatments were classified according to a diagnosis-related group, while reimbursement rates paid to the hospital provider were set by a “rates per activity” system.
The most recent comparative study on the cost-effectiveness of single- and 2-level MIS-TLIF vs open TLIF was published in 2019 by Djurasovic et al.28 Direct costs at 1 year were collected, including costs associated with the index surgical visit and costs associated with readmission. The 33 patients in each cohort (MIS-TLIF and open TLIF) were propensity matched, ensuring equivalence in age, sex, body mass index, diagnosis, American Society of Anesthesiologists class, smoking status, and levels fused.
Variable direct costs at 1 year were $2493 lower in the MIS-TLIF group than in the open TLIF group (mean $15,867 vs $17,612, P = 0.073). There was no difference in implant or biologics cost, but blood utilization, operating room supplies, hospital room and board, pharmacy, laboratory, and physical therapy costs were all significantly lower in the MIS group. Additionally, the mean length of stay was decreased in the MIS-TLIF group (3.21 vs 4.02 days, P = 0.05). No significant difference in EQ-5D or SF-6D gain was seen at 1 year.
MIS vs Open Multilevel TLIF Procedures
A single study included cases of more than 2-level fusions.23 This nonrandomized, retrospectively analyzed cohort included 11 patients managed by open TLIF and 57 by MIS-TLIF. Baseline demographics were similar between the groups. Of the open TLIF cases, 9 (81%) involved more than 2 fused levels, while only 12 of the 57 (21%) cases managed by MIS involved fusion of 2+ levels. This difference in the composition of the MIS and the open groups made direct and meaningful comparison problematic.
Discussion
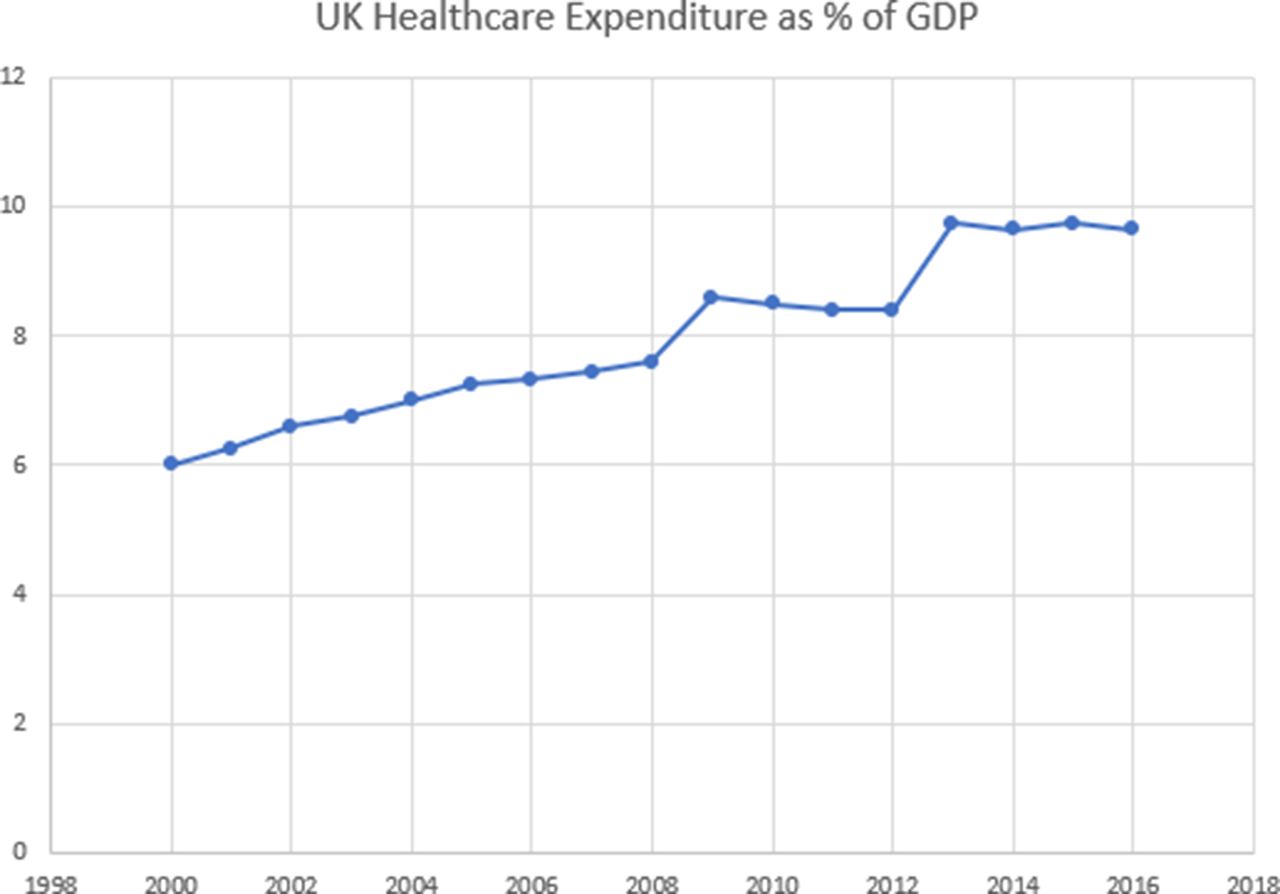
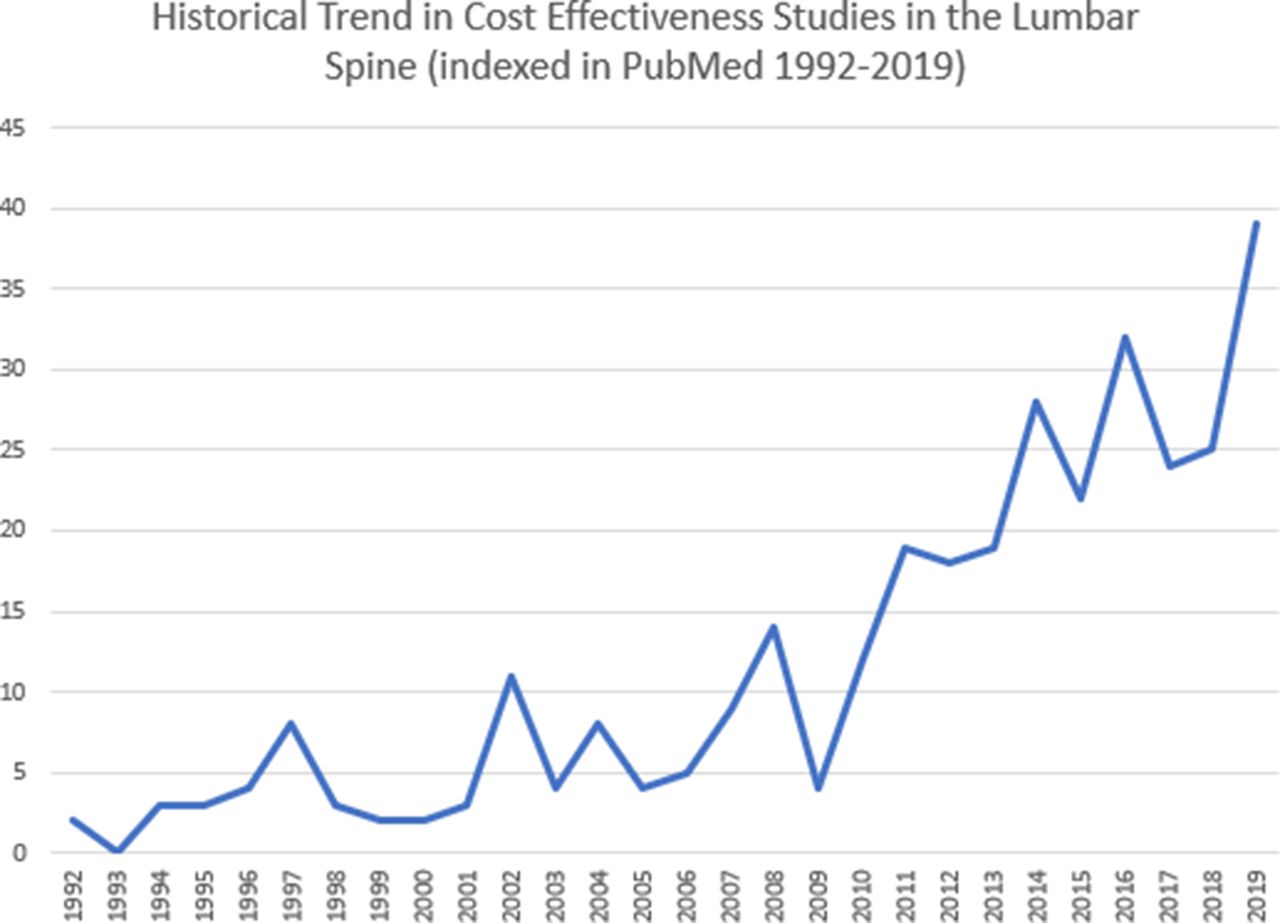
Health demands continue to outstrip health budgets (Figure 2). Studies focused on economic evaluations of health services are increasingly common. The increase in the number of “cost-evaluation studies in the lumbar spine” in the PubMed database highlights this trend (Figure 3).

UK health care spending as a percentage of gross domestic product.
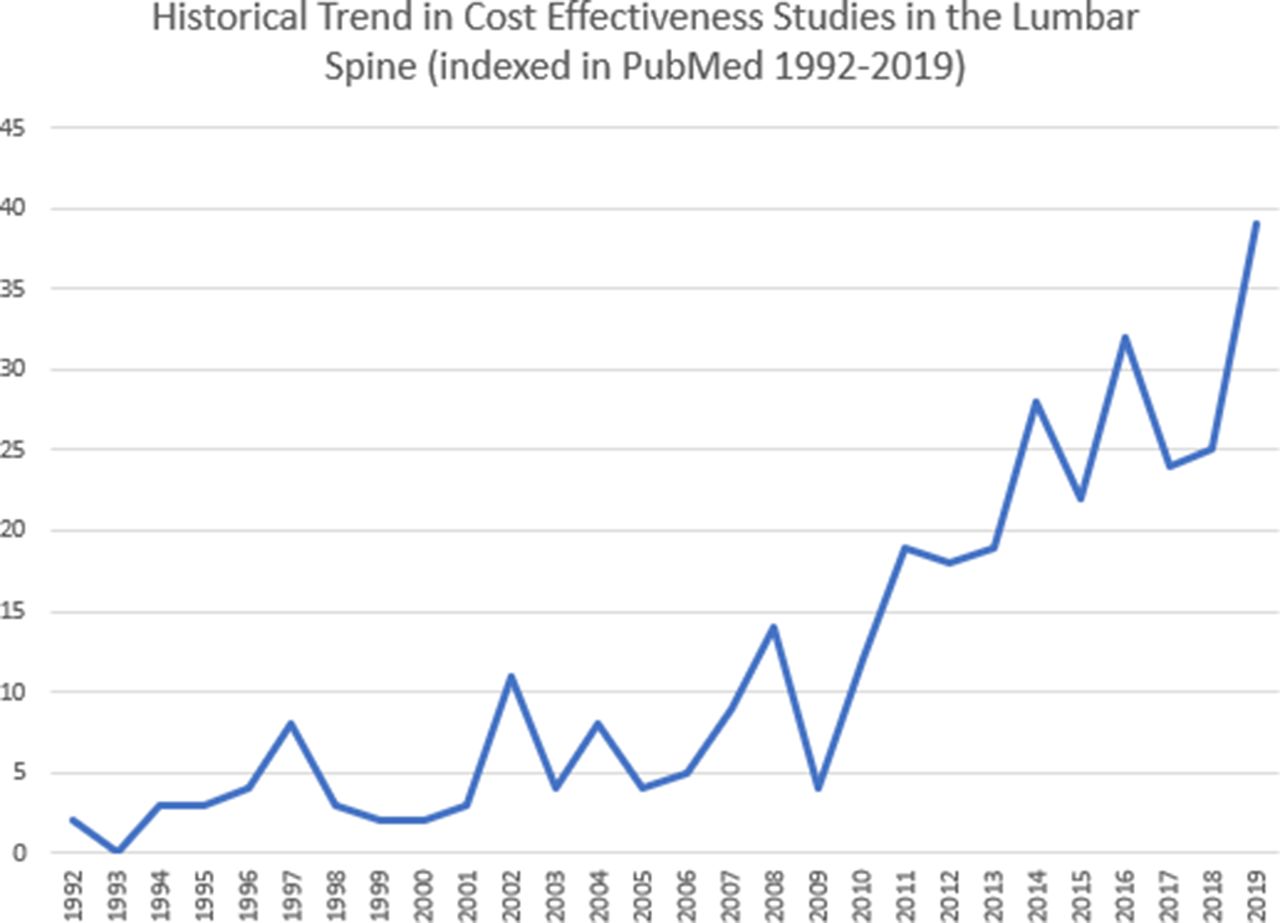
Number of clinical-effectiveness studies in the lumbar spine indexed per year in PubMed (1992–current).
Health care expenditure in the United States currently accounts for over 17% of gross domestic product, and “value-based” health care has been cited as a potential solution for rising health care costs.35 The Patient Protection and Affordable Care Act (2010) will affect the economics of provision of spinal services in the United States, and these changes may filter across to European health markets.36
Cost-utility evaluation of the treatment of lumbar stenosis and degenerative spondylolisthesis supports the cost-effectiveness of the surgical treatment of lumbar stenosis.1,37 The cost-effectiveness of lumbar fusion surgery remains a matter of debate. This systematic review aimed to outline the literature comparing the cost-effectiveness of minimally invasive and open lumbar spinal surgery across a variety of procedures and health care systems.
The studies reviewed outline a cost-effectiveness comparison between MIS and open surgery for lumbar discectomy, laminectomy, and fusion surgery. Overall, the studies sampled found lower total costs associated with MIS procedures, compared with the open group, with similar reported gains in QALY (clinical effectiveness). Three studies assessed outcomes of MIS vs open discectomy alone.12,13,19 Two of the 312,19 reported significantly lower total costs in the MIS, compared with the open group, with similar reported gains in QALY. The other reported a slightly higher total cost associated with MIS when compared with open lumbar discectomy, but this difference did not reach statistical significance.13
Two studies reported cost differences in MIS vs open laminectomy, both found significantly lower total costs and greater cost-effectiveness attributed to the MIS group.18,20 Twelve studies compared total costs and/or cost-effectiveness for open vs MIS lumbar fusion procedures across health care systems from a variety of payer perspectives.14–17,21–28 Lower total costs were found in MIS when compared with open fusion procedures across all the studies sampled except for one.27 Seven studies compared total cost and cost-effectiveness. Six of these found lower total costs and greater cost-effectiveness associated with MIS lumbar fusion than the open group.15,22,24–26,28 Only one of these studies found a higher total cost and lower cost-effectiveness in the MIS group compared with the open single-level fusion group.27 The small difference in both total cost and cost-effectiveness between the 2 groups did not reach statistical significance.
Historical review articles have explored this subject. Lubelski (2014) reviewed 6 economic studies comparing MIS with open procedures in the lumbar spine.9 They reported a similar cost base and clinical effectiveness (QALY gain) for MIS and open lumbar fusion (TLIF/PLIF) and decompression procedures (laminectomy/discectomy). For TLIF specifically, Parker (2014) performed a cost-utility evaluation and reported no difference in QALY between MIS and open procedures and reduced direct costs in MIS.22
Total costs (direct+ indirect) in MIS were less than they were for open surgery in 15 of the 17 studies (88.2%) included in our review (Table 5). While the cost of procedural equipment was higher in MIS cases, length of stay, blood transfusion, and other indirect costs were lower. Parker et al (2013) reported that mean 2-year direct costs (surgery, postoperative doctor visits, medications, injections, and physical therapy) were similar for their MIS and open TLIF groups. However, approximately twice as many workdays were missed after open (vs MIS) TLIF, and this translated into the significant difference in reported indirect cost ($6650).20 The majority of studies included in our review did not include an assessment of indirect costs. If indeed greater indirect costs do result from open lumbar surgery, the actual cost advantage of MIS vs open surgery concluded by the articles in this review could be underestimated.
Goldstein8 focused on the cost-effectiveness of MIS vs open PLIF or TLIF (but excluded discectomy and laminectomy), and found that MIS surgery was associated with a $2106 (5.8%) lower cost for 2-level fusions (vs open), with the cost savings mostly being attributable to lower hospital accommodation fees, operating room, and laboratory costs.8
Vertuani (2015) performed a cost analysis for both MIS and open TLIF using a decision model analysis.26 The study found that operative and equipment costs were higher for MIS, whereas hospitalization and surgical site infection costs were higher for open surgery. Most MIS cost saving was due to the reduction in inpatient stay and less requirement for blood transfusion. Postoperative complications were a relatively small contributor to the total costs for MIS, but a large contributor to the total costs for open surgery, mainly due to a higher rate of surgical site infection.
Study Challenges and Limitations
Attempts to perform a meta-analysis of the studies included in our review were made more challenging by factors such as variability in exchange rates, effects of inflation over different follow-up periods, and different cost perspectives across the studies (eg, societal vs provider vs payer). For these reasons, we did not attempt to pool any costing data from these studies.
One major challenge in cost evaluation of surgical procedures is that variation in health care systems can preclude direct cost comparison. Health care systems also have differing perspectives of the cost per QALY threshold used to define “cost-effectiveness.” Some studies fail to report the perspective of their costing data; for example, “costs” related to charges or reimbursements may bea significantly different in some private health care systems, such as in the United States (we outlined various payer perspectives in Table 5).
The dominance of nonrandomized studies in cost-evaluation analyses increases the risk of bias (only 1 of the 17 studies in our review was based on level 1 evidence).13 Table 4 highlights the wide range of methodological quality between the studies. Studies with weak methodology lack generalizability, and comparison between studies of different methodological quality is a significant challenge. This limitation is clearly illustrated in 2 of the studies in our review. In both cases, the MIS and the open group were not statistically equivalent, which limited the inferences that could be drawn from comparative cost and clinical outcome evaluation.23,25
Privately funded health care systems, such as the United States, create a different incentive base when compared with centrally funded systems such as the United Kingdom. Specialists may oversupply services within a pay per procedure model to maximize earnings. From the patient perspective, the economic theory of “moral hazard” dictates that an individual with comprehensive insurance coverage or a low deductible/copayment is incentivized to “overconsume” health services, when compared with an individual with less comprehensive insurance, a large deductible/copayment, or under the conditions of more stringent rationing in a centrally funded system.
When interpreting cost-utility analyses, choice of utility measure is significant. It is accepted that the interval changes of the EuroQol (ED-5Q) and SF-6D may differ within the same population, and hence these measures are not freely interchangeable. The SF-6D tends to be associated with a smaller effect and would result in a greater cost-utility than if the ED-5Q was used. The utility score is independently affected by the MIS technique and the baseline outcome score; thus, the true effect of MIS on the change in utility score vs other confounders is difficult to quantify.25
Despite the limitations of this review, due to the variations across health care systems and weaknesses in the methodology of the component studies, we have produced a useful outline of the current literature on this increasingly important topic.
Conclusion
We report lower direct costs in MIS compared with open surgery across all 3 of these common forms of lumbar spinal surgery. Our work supports the existing literature28,38–40 in confirming both the cost- and clinical effectiveness of MIS and open lumbar surgery in most cases, and in failing to conclusively find a difference in clinical effectiveness (QALY gain) between the MIS and open surgical groups.5,41
The methodological quality of studies in this review was poor to moderate, and most studies were retrospective rather than prospective. More randomized prospective work is needed to minimize bias and to provide sufficient statistical power to allow firmer conclusions to be made.
Despite increasing interest in this field, definitive conclusions on cost-effectiveness cannot yet be made. Future work should focus on constructing higher-quality clinical trials across a range of health care systems, with consistency of the costing perspective, predetermined costs, and longer-term follow-up to allow more definitive conclusions to be made.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.