


Abstract
Background Postoperative pain management of multilevel lumbar fusion remains challenging. There are few reports of opioid-sparing regional analgesia for spine surgery. We present a novel method for surgeon-placed erector spinae plane (ESP) catheters for multilevel lumbar spine fusion and compare pain- and opioid-related outcomes in a matched cohort who received anesthesiologist-placed ESP blocks.
Methods A retrospective matched pilot study of 18 patients: 6 received intraoperative, bilateral ESP catheters. Tunneled catheters were placed under the intact ESP at the proximal end of the incision. Continuous infusions of ropivacaine (0.2%) were started in the postanesthesia care unit (PACU) after emergence from anesthesia and maintained for 48 hours. Catheter patients were matched 1:2 with 12 patients who received preincision single-shot ESP blocks administered by an anesthesiologist, according to age, gender, American Society of Anesthesiologists class, body mass index, and number of spinal levels fused. All patients were provided opioid intravenous patient-controlled analgesia (IV-PCA). Numeric rating scale pain scores (NRS, 0–10), length of stay (LOS), opioid consumption (oral morphine equivalents, mg), opioid side effects, and complications (motor weakness, local anesthetic toxicity, infection, technical issues, and failure), were compared in the PACU and on the nursing floor.
Results Only 1/6 patients with ESP catheter used opioid IV-PCA, compared with 11/12 who received ESP blocks. There were no differences in total opioid consumption (catheters: 135 ± 141 mg; blocks: 183 ± 112 mg; P = 0.448) or median (interquartile range) LOS (catheters: 73 [50,107] hours; blocks: 90 [72,116] hours, P = 0.708). NRS pain was significantly higher in the PACU after ESP catheters (5.9 ± 1.7) vs ESP blocks (3.3 ± 2.4; P = 0.036), but no differences were found at later timepoints (5.0 ± 1.6 vs 4.3 ± 1.1, respectively; P = 0.383). No catheter-related complications were found.
Conclusion Surgeon-placed ESP catheters represent a simple technique to provide regional analgesia, particularly in centers lacking regional anesthesiology services. Risks, benefits, and efficacy compared to other techniques require prospective study.
Level of Evidence 3.
- erector spinae plane block
- continuous catheter
- erector spinae catheter
- opioid consumption
- pain score
- lumbar spine fusion
- postoperative pain management
- multimodal analgesia
Introduction
As demand for lumbar spinal fusion continues to rise worldwide, interventions that improve patient outcomes and shorten length of stay (LOS) are required.1 Postoperative pain management is based on multimodal analgesic (MMA) regimens, which typically include acetaminophen, discretionary nonsteroidal anti-inflammatory drugs, muscle relaxants, and opioids.2 Historically, there have been limited opportunities to incorporate regional analgesic techniques into MMA regimens. Surgeon-administered local infiltration and epidural analgesia have both been described; however, each has significant limitations, including equivocal benefits on pain scores and opioid consumption, and hypotension and motor/sensory block, respectively.3,4
More recently, single-shot erector spinae plane (ESP) blocks are emerging as an intervention to improve pain and minimize opioid consumption after lumbar spine surgery.5,6 Although promising, to date, there is minimal evidence to support routine use, and widespread clinical adoption may be limited to centers with advanced regional anesthesia resources and expertise. Furthermore, the duration of analgesia of ESP blocks is limited by the local anesthetic used; for spinal procedures with high pain burden, it may be unacceptably short.
Continuous ESP catheter techniques may solve these problems but are associated with challenges of their own: methods to improve placement accuracy and consistency are required, and benefits on pain- and opioid-related outcomes have not been defined in spine surgery population.
Here, we present a novel regional analgesic technique in which intraoperative bilateral ESP catheters were placed by the spine surgeon under direct visualization. We also present the results of a retrospective analysis comparing pain- and opioid-related outcomes in 12 patients who received ESP blocks and were matched 2:1 to 6 patients who received catheters for lumbar spine fusion.
Methods
Patients
The study was a proof-of-concept retrospective comparison of 18 patients presenting for multilevel lumbar fusion. Six patients who received surgeon-placed, bilateral continuous ESP catheters between December 2020 and February 2021 were matched 1:2 with 12 patients who received single-shot ESP blocks between January 2019 and July 2020 administered by an anesthesiologist. From a total of 342 patients who received an ESP block, patients were matched according to age, gender, American Society of Anesthesiologists class, body mass index, and number of spinal levels fused. The study was approved by the institutional review board, and written informed consent was waived. Written permission was obtained for publication of deidentified images.
Erector Spinae Plane Catheters
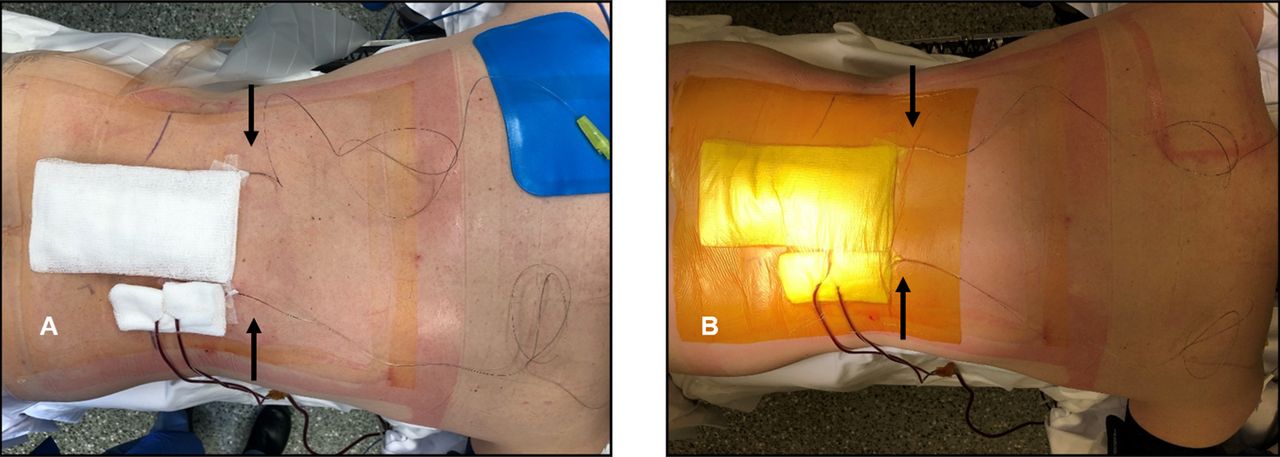
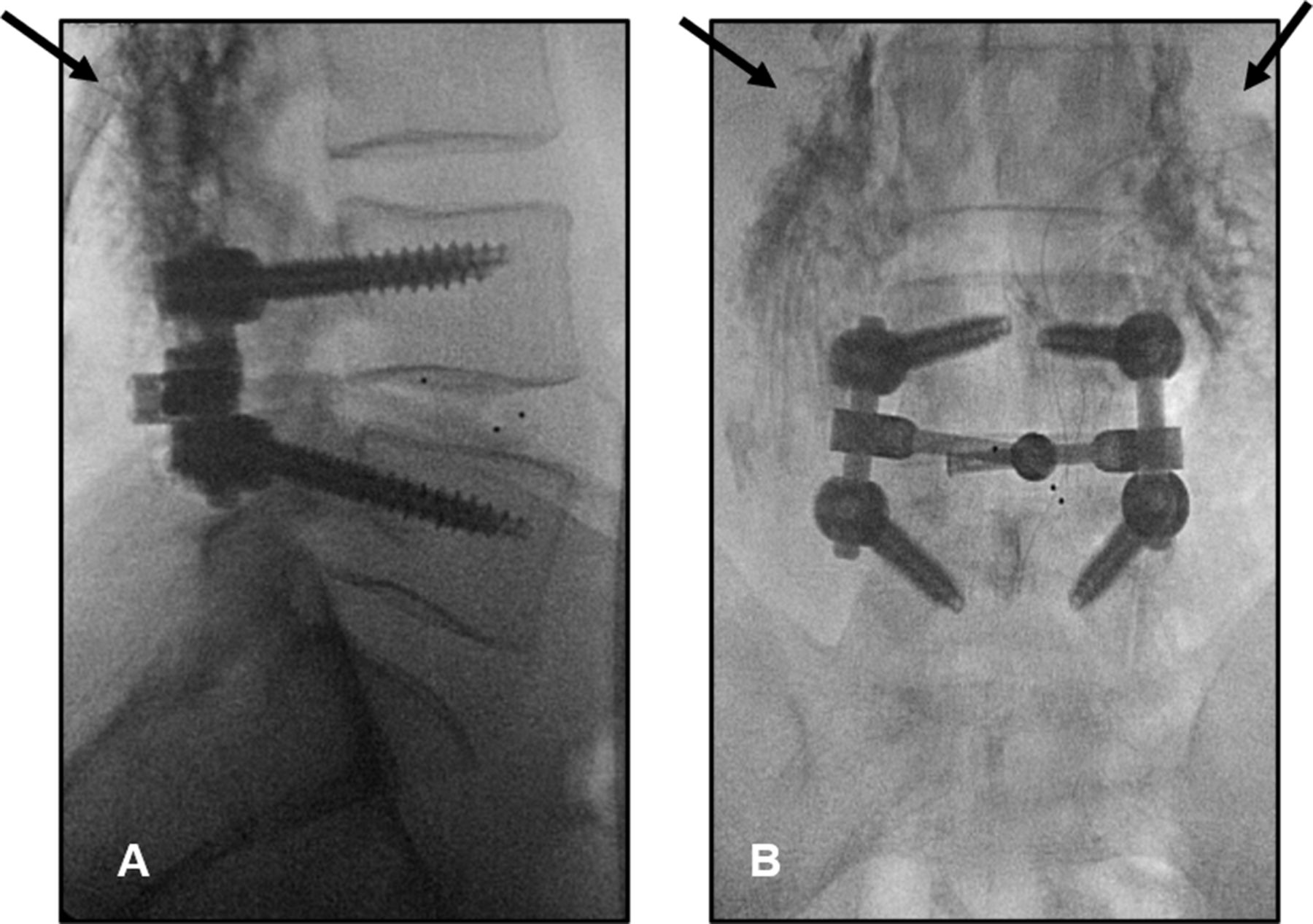
Bilateral ESP catheters were placed by the attending surgeon under direct visualization at the end of the procedure, prior to closure. An introducer needle (Contiplex Tuohy Ultra Nonstimulating Catheter System, 18 Ga/4 in; B. Braun Medical Inc., PA, USA) was used to tunnel the catheters at the proximal end of the surgical field. Each catheter tip was placed under the distal-most portion of the intact ESP, at the tip of the transverse processes (Figure 1). Catheters were secured at the skin with dermabond and steristrips, and surgical dressings were applied (Figure 2). Confirmation of catheter position was confirmed by fluoroscopy (Figure 3).

Position of erector spinae catheter (ESC) relative to surrounding anatomy. The catheter is tunneled and then positioned at the tips of the transverse processes (TP, arrows), with the proximal end placed under the erector spinae muscle (ESM). (A) The image indicates the position of the ESC at the tips of the TPs. (B) The image illustrates the position of the catheter tip. The artist omitted the TPs to enhance visualization of the ESC trajectory.
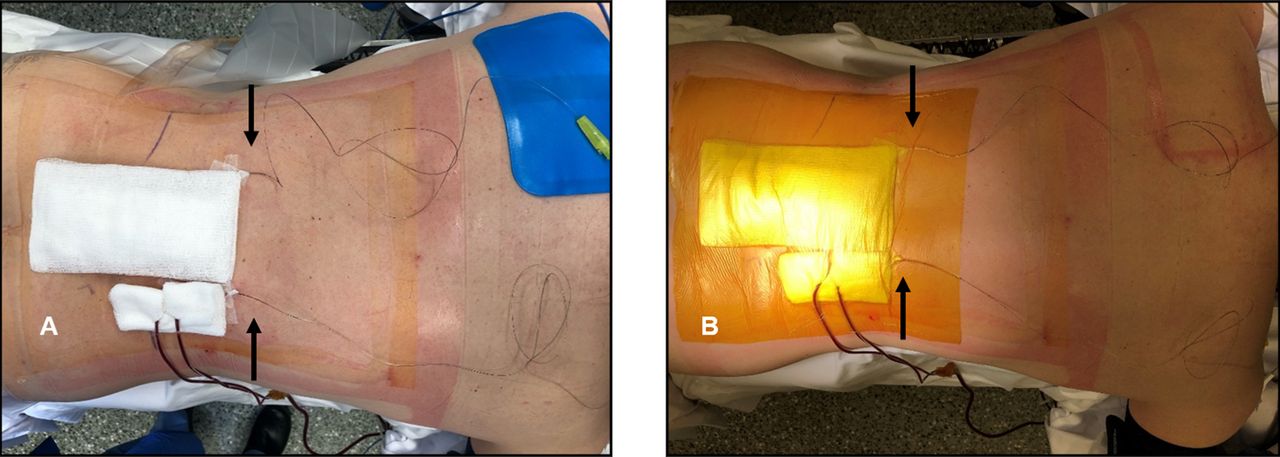
Intraoperative photographs showing location of catheters (arrows) relative to surface landmarks (A) and method to secure catheters under the surgical dressings (B).

Contrast fluorescence radiograph in lateral (A) and anterior-posterior (B) views, demonstrating the spread of dye (arrows) under the erector plane tissue following placement of bilateral erector spinae plane catheters.
In the postanesthesia care unit (PACU), after extubation and recovery from anesthesia, a full motor and sensory examination was performed, and a patient-reported pain score was recorded. Catheters were bolused with 10 mL of 0.2% ropivacaine on each side. Each catheter was attached to a continuous infusion pump with 0.2% ropivacaine analgesia (0.3–0.6 mg/kg/h) for 48 hours. Catheters were managed by the acute pain service and removed by the spine service physician assistant with the dressing change on postoperative day 2.
Anesthetic Details
Patients were cared for under an enhanced recovery pathway for lumbar fusion, as previously described.2 In brief, all patients received general anesthesia with endotracheal intubation and a total intravenous (IV) anesthetic-based regimen (propofol, dexmedetomidine, and ketamine). Our institutional care pathways for spine surgery include intraoperative IV lidocaine.2,7,8 However, lidocaine was omitted in the present study to minimize the risk of local anesthetic toxicity. Standardized, MMA comprising acetaminophen, ketorolac, and oral opioids (titrated to pain scores) was provided. All patients were prescribed hydromorphone intravenous patient-controlled analgesia (IV-PCA) for postoperative care.
Relevant Surgical Details
All patients underwent primary open lumbar interbody fusion with pedicle screw instrumentation and posterolateral bone grafting. All surgeries were performed by fellowship trained orthopedic spine surgeons. The transverse processes of fused levels were exposed and directly visualized bilaterally. The transverse processes, facet joints, and remaining laminae of appropriate levels were decorticated, and autografts and/or allografts were placed on the decorticated bones. Details of included surgeries are presented in Table 1.
Patient demographics and comparisons between bilateral ESP blocks and catheters.
Single-Shot Erector Spinae Plane Blocks
Bilateral ESP blocks were performed with the patient in prone position after induction of general anesthesia, prior to surgical incision. Blocks were performed by the attending anesthesiologist. Ultrasonography was used to identify the appropriate lumbar level. A 10-Hz high-frequency linear probe (FUJIFILM Sonosite, Inc., WA, USA) was placed in parasagittal orientation in the midline to identify the spinous processes. The probe was translated laterally until the tips of the transverse processes were viewed. A 20-Ga 4-in Ultraplex needle (B. Braun Medical Inc., PA, USA) was placed in-plane and advanced in a cranial-to-caudal direction until the tip was under the erector spinae muscle.9 Between 20 and 30 mL, 0.375% bupivacaine with preservative-free dexamethasone (2 mg/30 mL) was injected under visual inspection.
Outcomes
Data on outcomes of interest were extracted from the electronic medical record. Pain scores (numeric rating scale, 0–10) and opioid consumption (oral morphine equivalents, mg) were assessed 8 hourly in the PACU and on the nursing floor. LOS was measured for the PACU and nursing floor. Complications related to the catheters (motor weakness, local anesthetic toxicity, infection, difficulty removing, migration/dislodgment, and failure) and opioid-related side effects (respiratory suppression, postoperative nausea/vomiting, obstipation, uncontrolled pain, confusion/disorientation, and sedation) were assessed by review of notes and medications administered (antiemetics, naloxone, rescue analgesics, dexmedetomidine, and bowel regimen).
Statistical Methods
Descriptive statistics were used. Data are presented as mean (SD) unless one or more the results were skewed, in which case data are presented as median (25%–75% interquartile range). Normality of distribution was determined by using the Shapiro-Wilk test. Testing was performed using Χ 2/Fisher exact test and t test where appropriate. A P value < 0.05 indicated significant differences between groups. As a proof-of-concept study, there was no sample size calculation or formal hypothesis testing.
Results
Eighteen patients were included in the analyses: 6 patients received ESP catheters, and 12 patients received ESP single-shot blocks. There were no significant differences in any measured demographics and surgical variables between the groups (Table 1).
Comparisons of pain scores, opioid consumption, and LOS are presented in Table 2. Numeric rating scale scores were significantly higher in the PACU among patients who received ESP catheters (5.9 ± 1.7) than ESP blocks (3.3 ± 2.4; P = 0.036), but no differences were found at later timepoints. Trends in pain scores over time revealed higher scores in the PACU compared with the nursing floor for patients who received ESP catheters (5.9 ± 1.7 followed by 5.0 ± 1.6; P > 0.05), and lower scores in the PACU compared with the floor for patients who received ESP blocks (3.3 ± 2.4 followed by 4.3 ± 1.1; P > 0.05). These changes were nonsignificant for both ESP blocks and catheters.
Comparison of pain scores, opioid consumption, and length of stay between bilateral ESP blocks and catheters.
There were no differences in total opioid consumption between the groups in the PACU or on the nursing floor (Table 2). Just 1/6 patients in the catheter group used IV-PCA opioid, compared with 11/12 patients in the ESP block group. One patient in the catheter group took no postoperative opioids at all.
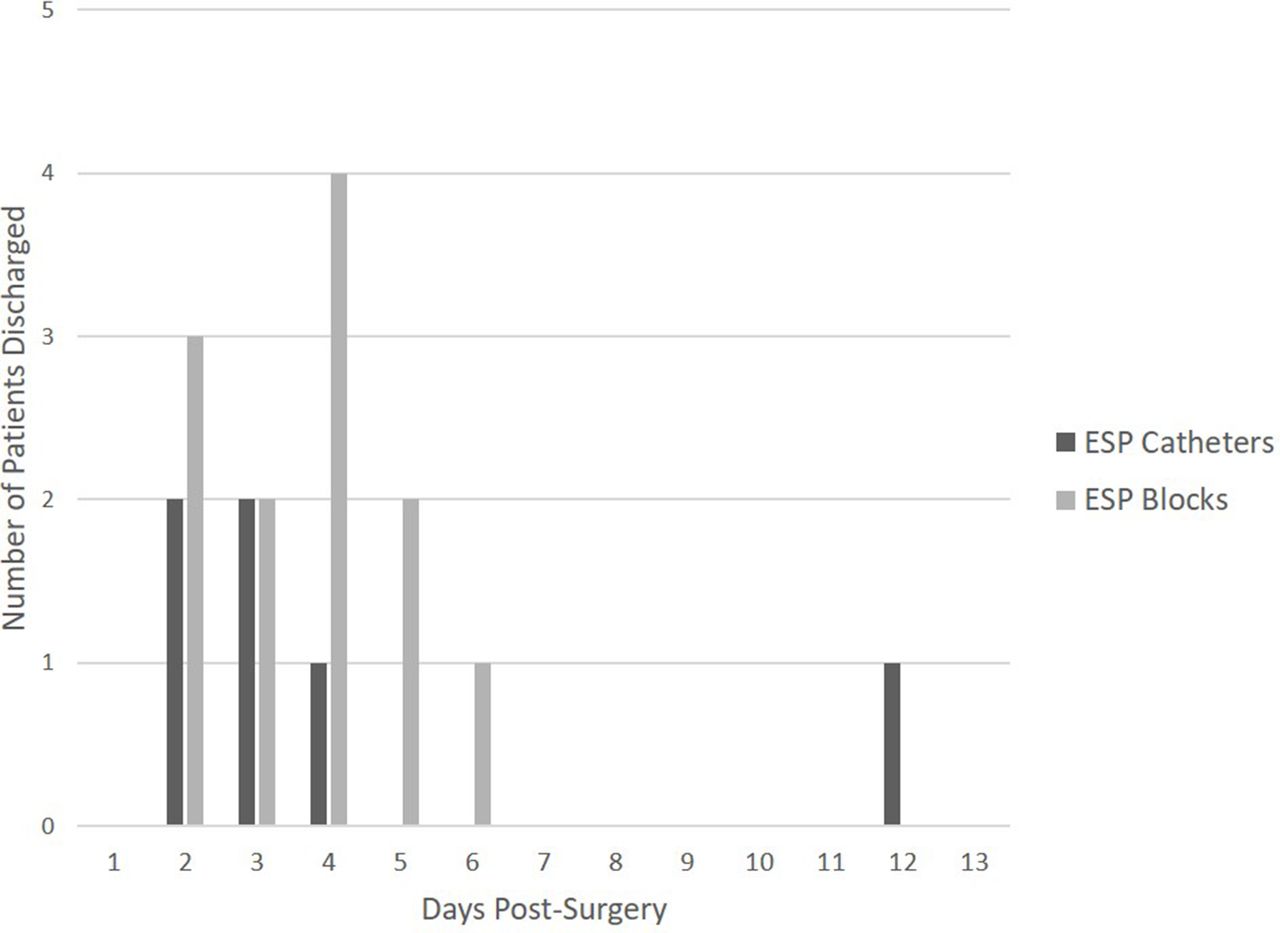
There was no difference in total LOS between patients who received ESP catheters (median [interquartile range] 73 [50, 107] hours) and ESP blocks (90 [72, 116] hours; P > 0.05). Half the patients who received ESP catheters were discharged on or before postoperative day 3, while half the patients who received ESP blocks were discharged on or before postoperative day 4 (Figure 4). One patient in the catheter group had an extended LOS (12 days) for management of complex medical comorbidities while awaiting placement in an acute rehabilitation facility.

Length of stay of patients receiving erector spinae plane (ESP) catheters (dark bars) vs ESP blocks (light bars), by day of discharge.
The only opioid-related side effect found in the ESP block group was confusion/disorientation, reported in 2 patients. There were no prespecified opioid-related side effects or major catheter-related complications found in the catheter group. A single catheter in 1 patient dislodged after 12 hours; the contralateral catheter was maintained. A single patient was ready for discharge after 24 hours, so the catheters were stopped early and removed. Workflow issues were remarkable for one instance (the first catheter patient) where floor nurses were unsure which service (pain service, anesthesiologist on call, or surgical service) to contact for questions and concerns.
Discussion
This retrospective observational study describes a novel method for placing ESP catheters for patients undergoing multilevel spine fusion and compares outcomes to single-shot ESP blocks. We found low pain scores and modest opioid consumption in both groups, and patients who received ESP catheters used significantly less IV opioids than those who received single-shot blocks. However, we found no significant differences in total opioid consumption, pain scores, or LOS between the groups. Although not designed as a safety trial, we did not find any complications attributed to ESP blocks or catheters. The technique for catheter placement was simple to perform and represents an opportunity to offer benefits of regional analgesia for spine surgery patients in centers lacking specialist anesthesia services.
Multilevel spine fusion is among the most painful surgical procedures, with median pain scores on postoperative day 1 of approximately 7.10 Opioids have traditionally formed the basis of analgesic regimens after spine surgery. However, recent trends toward opioid-sparing and opioid-free MMA are emerging in the literature and are touted as important tools to improve short-term recovery after spine surgery and reduce the risk of long-term opioid use and misuse.2,7,8,11,12
Regional analgesic techniques are considered a key component of MMA and enhanced recovery pathways for spine surgery, but opportunities to incorporate blocks in spine care have been limited. In recent years, reports of fascial plane blocks for spine surgery with lateral and/or posterior approaches have been described and associated with benefits on pain- and opioid-related outcomes.5,6,13,14 Chief among these is the ESP block. The ESP block was first described in 2016 for the treatment of thoracic neuropathic pain and has subsequently been successfully used to provide analgesia for a variety of procedures including thoracic, cardiac, breast, and abdominal surgeries.9,15–18 The role and value of the ESP block in spine surgery are not yet established, but at the time of writing, evidence supports the potential of the block to reduce pain and opioid consumption after lumbar decompression and/or fusion.5,6 Despite hundreds of reports of efficacy since its first description in 2016, the mechanism of action of the ESP block remains incompletely understood and heavily debated. The prevailing theory is that multilevel sensory block is achieved by cranial-caudal spread of local anesthetic spread, facilitated by the thoracolumbar fascia. Consistent with this, a recent narrative review of evidence from preclinical, clinical, and cadaveric studies concluded the most consistent, plausible mechanism is via spread to the dorsal rami of spinal nerves at the affected levels.19
Distinct from the question of efficacy, there are several potential drawbacks to single-shot ESP blocks for spine surgery: (1) placement typically requires specialist anesthesiologist services, (2) the duration of analgesia is limited by the local anesthetic selected, and (3) local anesthetic spread and distribution may be disrupted by surgical interruption of the ESP. Each of these disadvantages may be obviated by surgeon-placed ESP catheters. The feasibility and efficacy of surgeon-placed catheters have been suggested in a prior technical report of continuous thoracolumbar dorsal ramus blocks in 3 patients undergoing scoliosis surgery.20 Description of ESP catheters for lumbar surgery is limited to a single case series, in which catheters were placed preincision by the anesthesiologist.21 Consistent with the results reported here, both concluded low pain scores, low opioid consumption, and no complications. However, pain scores and opioid use at all times appear significantly lower in the latter series compared with the results found here.21 Reasons for these discrepancies may include differences in local anesthetics used, the surgeries performed, the number of levels fused, and the other intra- and postoperative MMA agents. Notably, in the present study and in the technical report by Xu et al, continuous infusions were used for postoperative catheter analgesia.20 In contrast, Melvin et al used a bolus-based regimen to deliver local anesthetic.21 Prior reports in other surgical subtypes suggest bolus dosing may be superior to continuous infusion for peripheral nerve catheter analgesia.22
Except for IV opioid use, we found no differences in outcomes of interest between ESP blocks and catheters. However, several notable trends were apparent, which merit further study. Absolute pain scores were lower than reported in the literature in both groups, supporting the value of adding ESP analgesia to MMA for spine surgery.10 Pain scores were significantly higher in the PACU in the catheter group compared with the block group, but not different thereafter. This is potentially explained by our workflow, in which a full motor/sensory examination was performed prior to starting the catheter infusions. Another potential explanation is that blocks were performed prior to surgical incision, and catheters were placed prior to surgical closure. The immediate analgesic benefits of ESP blocks on emergence from anesthesia suggest optimal regimens may include both techniques (specifically, ESP blocks performed prior to surgery and catheters for longer-term analgesia). The subsequent drop in pain scores in the catheter group is consistent with our interpretation that ESP analgesia could be an important MMA adjunct in this population. Finally, although overall LOS was not significantly different between the groups, more of the catheter patients were ready for discharge almost 1 day prior to patients who received single-shot blocks. The potential for shorter LOS may be explained by sparing the requirement for opioid-containing IV-PCA, an effect which has been described after major orthopedic surgery.23
The benefits suggested by ESP blocks and catheters must be weighed against potential risks, and our study was likely too small to assess the incidence of complications. Complications associated with ESP blocks and catheters include vascular injury or inadvertent injection (leading to local anesthetic toxicity), as well as the potential for interference with intraoperative neuromonitoring and the early postoperative examination (should there be spread of local anesthetic to adjacent neuraxial structures). Where performed for thoracic procedures, the risk of pneumothorax is additionally presented. Encouragingly, despite the large number of studies reporting outcomes after ESP blocks for mixed surgical subtypes, there are very few reported complications.15 Prospective studies in spine cohorts consistently report zero complications as secondary outcomes; however, if complications are rare, these small trials may be underpowered to detect them.6,16,21 Consistent with this, the largest retrospective series on this question reported an incidence of 1 complication (pneumothorax) in 684 ESP blocks for spine surgery (or 0.2%), suggesting the relative safety of this technique for patients undergoing spine surgery.24
There are several important limitations to the present study. First, as a retrospective design with small sample size, we did not aim to establish differences in outcomes between ESP blocks and catheters, and we did not include a formal sample size calculation to detect differences in outcomes of interest. Rather, we sought to generate pilot data and demonstrate proof of concept for surgeon-placed catheters to generate hypotheses and power future studies. We did attempt to mitigate the design weakness by matching patients who received block:catheter in a ratio of 2:1. We found no differences in demographic and perioperative variables between the 2 groups, suggesting a reasonable matching process. Second, the study was performed at a specialty orthopedic surgery hospital, with full perioperative pain, regional anesthesia, and ancillary services, limiting the generalizability of our findings. Third, the ESP catheters were visible to patients and providers, which may have affected providers’ behavior and/or patients’ perception and expectations.
Nonetheless, this work raises several provocative questions for future research. The procedure-specific indications for ESP blocks vs catheters and the relative risks and benefits of each are unknown, and direct comparisons of the 2 techniques are required before concluding superiority of one over the other and/or introducing either into routine clinical practice. Comparisons should consider the surgical approach and extent to which the ES plane is violated: in conventional open posterolateral fusion, the ES plane is more exposed compared with minimally invasive techniques with percutaneous pedicle screw placement. These differences may affect the differential spread of local anesthetic and potentially determine the indications for each technique. Prospective studies should also evaluate the role and value of ESP blocks vs catheters on a patient-specific basis. Cohorts to consider include opioid-tolerant patients and those with chronic pain conditions as well as patients undergoing revision surgery. The latter group may benefit more from surgeon-placed catheters than single-shot blocks where scar tissue may impede the spread of local anesthetic into the ES plane. The optimal regimen for ESP catheters also remains unclear, and future studies should assess the dosing, timing, bolus vs continuous infusion regimens, and selection of local anesthetics. Although surgeon-placed catheters may represent a simple intraoperative technique, issues with postoperative management in institutions without acute pain services may be challenging, and these issues (and solutions) should be reported. Future studies should focus on safety and the incidence of complications associated with each technique. In addition to clinical evaluation of the techniques, cost analyses would be valuable. Given the resource-intense nature of these types of regional analgesia-based techniques, costs may be increased with a catheter-based analgesic regimen. Conversely, costs to implement and maintain a catheter service may be offset by savings if LOS is reduced.
Conclusion
We report a simple method to place bilateral ESP catheters under direct visualization and compare outcomes to single-shot ESP blocks. We found low pain scores, modest opioid consumption, and comparable LOS in both groups, without any detected complications. These techniques may offer promise to improve recovery after multilevel spine fusion. Surgeon-placed ESP catheters may be particularly suitable for settings lacking developed regional anesthesia services for particular patients and/or for specific types of spine surgeries.
Acknowledgements
We thank Justas Lauzidas, PhD, from the Department of Anesthesiology, Critical Care & Pain Management at Hospital for Special Surgery for creating the technical illustrations of the erector spinae plane catheter.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was conducted after IRB approval (HSS IRB #2021-0267; PI, EM Soffin).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Continuous erector spinae plane catheters leading to unwanted neuraxial spread after spinal fusion surgery: a report of two cases from a terminated prospective randomized clinical trial
- Continuous erector spinae plane catheters leading to unwanted neuraxial spread after spinal fusion surgery: a report of two cases from a terminated prospective randomized clinical trial