


Dear Editor,
We read with interest the article entitled “Biomechanical Stability of the Sacroiliac Joint With Differing Implant Configurations in a Synthetic Model” by Andrew L. Freeman, Joan E. Bechtold, and David W. Polly, published in the International Journal of Spine Surgery in October 2021. First, we thank the authors for this informative in vitro analysis regarding optimal iFuse (SI-BONE, San Jose, CA) implant configuration for minimally invasive sacroiliac joint fusion. We have a few questions about other implant configurations that may achieve greater sacroiliac (SI) stability.
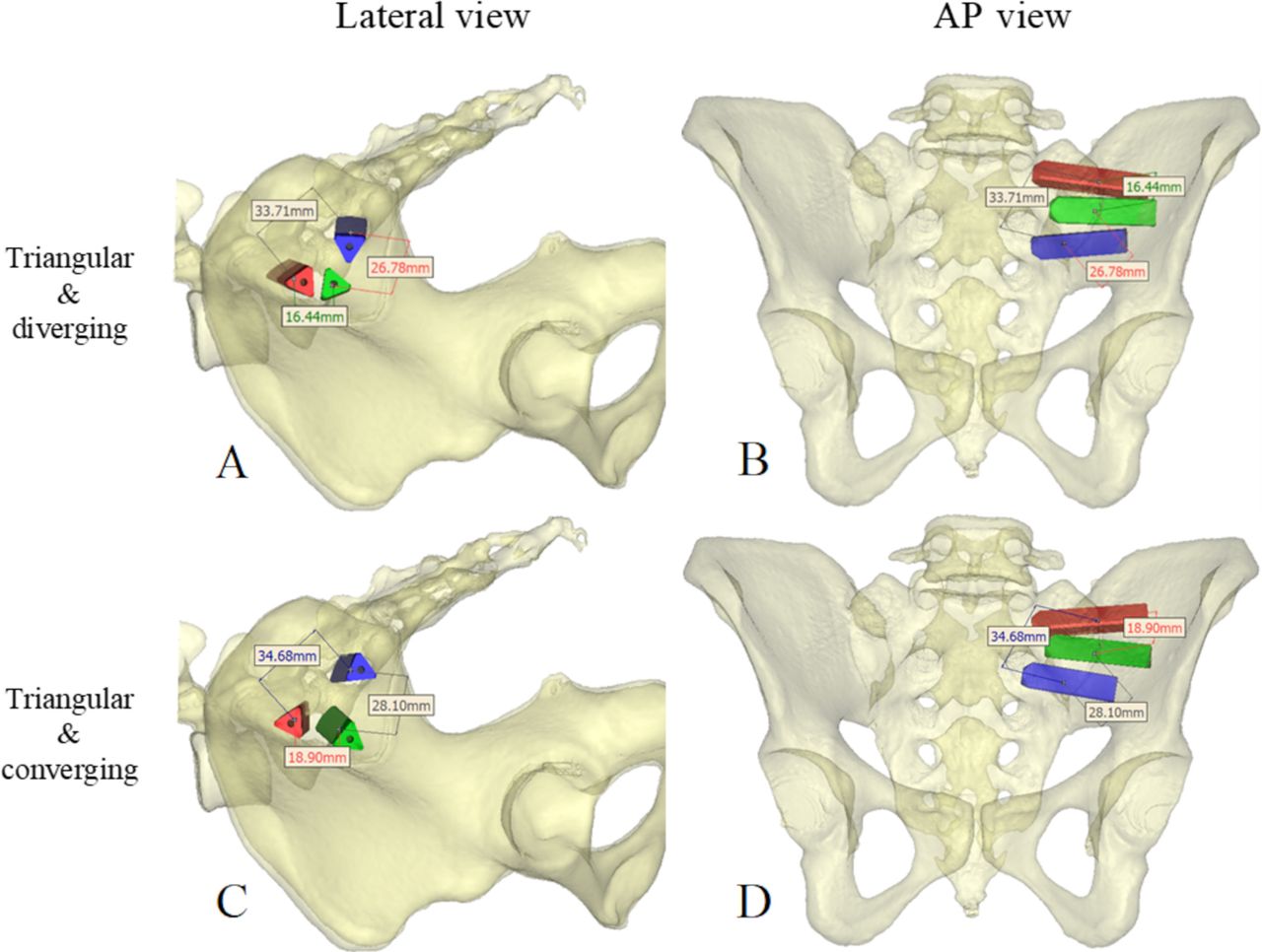
It is an interesting and valuable outcome that implant configurations with more spacing between the implants, a triangular pattern, or an angled (10° diverging) pattern resulted in a lower range of motion compared with the conventional linear configuration. Remarkably, the linear-angled 10° configuration is not superior to the triangular configuration with 22 mm space between implants. This indicates that spacing between the implants is the most essential component for stability. Consequently, combining these 2 patterns and changing the angles to an inward converging configuration might show even more superior outcomes. Unfortunately, this configuration was not described. Figure A and B show a triangular pattern with the peripheral implants placed with a diverging orientation. In Figure C and D, a similar triangular pattern is shown but with the implants placed in a converging transarticular orientation.

Triangular configuration with peripheral implants angled in an outward direction (A and B) and a triangular configuration with implants angled inward (C and D). The distances are measured at the sacroiliac joint gap. The 3-dimensional bone models are based on a computed tomography image and were acquired using Materialise Mimics (Leuven, Belgium). AP, anteroposterior.
In the angled pattern described in the article, the peripheral implants are angled outward, which implies a diverging orientation. However, this will most likely result in a smaller implant depth for the first implant due to the sacrum’s converging shape, while longer implant depths are proven to result in a more stable arthrodesis.1 To obtain the most medial possible implant placement, that is, placing the implants as far as possible into the sacrum, it could be interesting to investigate a triangular implant pattern with a converging orientation to create a transarticular implant configuration. Such configuration can only safely be accomplished by using intraoperative guidance, such as intraoperative navigation as applied by Cleveland et al.2 Previous studies by Lindsey et al1 and Soriano-Baron et al3 have demonstrated that a transarticular configuration reduces motion compared with an inline orientation. Furthermore, could it be that the combination of the triangular pattern with a converging orientation would create more spacing between the implants at the height of the SI joint gap? Although the theoretically lower bone density of the sacrum may have an adverse effect on a converging configuration, spacing between implants and implant depth is probably a more important component for a stable SI arthrodesis. As the authors have demonstrated, more spacing results in the most optimal outcome, that is, less range of motion. When, as we simulated, the implants are placed in a triangular pattern with a converging orientation instead of the diverging orientation, the spacing between implants at the level of the SI joint increases (see Figure). Furthermore, the implants were placed slightly deeper into the sacrum with the converging configuration. Therefore, we believe that a triangular and converging configuration can result in an even more stable SI arthrodesis.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this letter.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures All authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.