


Abstract
Background Opioids are a mainstay for pain control in patients undergoing lumbar spine surgery but are associated with a high risk of dependence and significant adverse effects. Efforts continue to be made to utilize non-narcotic agents such as regional nerve block for pain control as part of a multimodal analgesia regimen. Recently, transversus abdominis plane (TAP) blocks have proven beneficial for patients undergoing lumbar fusion procedures. The purpose of this study is to evaluate the efficacy of TAP blocks for postoperative pain control and the effect on opioid consumption and hospital length of stay (LOS) in patients undergoing anterior lumbar interbody fusion (ALIF).
Methods A retrospective review of patients undergoing elective ALIF included collection of data on demographics, LOS, pain scores using visual analog scale (VAS), opioid consumption using morphine milligram equivalents (MME) from postoperative day (POD) 0 to 5, and any complications. Patients who underwent primary ALIF or ALIF with concomitant posterolateral lumbar fusion were included.
Results A total of 99 patients met inclusion criteria; 47 had a preoperative TAP block and 52 did not. Demographic data and number of levels fused were equally distributed between the groups. The TAP group had significantly lower MME consumption postoperatively during POD 0 to 2 and 0 to 5. VAS pain scores were lower for TAP block patients on POD 3 and 4; otherwise, there was no significant difference. LOS and complication rates were not significantly different. A multiple regression analysis found male sex to be a predictor of increased postoperative MME, while age and TAP block were significant predictors of decreased MME.
Conclusions The use of TAP block for patients undergoing ALIF was associated with less cumulative MME consumption in the immediate postoperative period. TAP block may be an effective tool for reducing postoperative opioid consumption in patients undergoing ALIF.
Clinical Relevance The data in this study provide clinical relevance supporting the use of TAP blocks for patients undergoing ALIF procedures.
Level of Evidence 3.
- transversus abdominis plane block
- opioids
- anterior lumbar interbody fusion
- lateral lumbar interbody fusion
Introduction
Lumbar interbody fusion is associated with significant postoperative pain that often requires high doses of opioids for analgesia.1 Recent studies have brought attention to the importance of multimodal analgesia (MMA) regimens to decrease narcotic consumption and the adverse effects associated with their use.2 Development and research on MMA protocols have become central during the current opioid epidemic to decrease reliance on opioids for postoperative pain control.2 Regional anesthesia in the form of fascial plane blocks has recently gained attention in the spine surgery literature as part of these MMA protocols.3–5
Transversus abdominis plane (TAP) blocks are a form of regional anesthesia that may be useful in controlling pain for surgeries involving abdominal-based incisions, although its use in lumbar spine surgery is not yet well established. TAP blocks have been traditionally reserved to provide regional anesthesia in general, gynecologic, and urologic specialty procedures involving the anterior and lateral abdominal wall.6 A recent study by Reisener et al found decreased opioid consumption and hospital length of stay (LOS) without significant difference in pain scores when comparing patients who received a TAP block vs those who did not.7
This study retrospectively reviewed a consecutive cohort of patients undergoing elective, primary anterior lumbar interbody fusion (ALIF). The primary outcome was to compare inpatient postoperative opioid consumption. Secondary outcomes were to compare postoperative pain scores and hospital LOS. Patients who underwent staged posterior lumbar fusion (PLF) with instrumentation on the same day as ALIF were also included and analyzed separately. Postoperative opioid consumption was measured using morphine milligram equivalents (MME), postoperative pain was assessed via the visual analog scale (VAS), and LOS was measured in days. Other measured outcomes included complications from the TAP block, rate of revision surgery, and VAS at 2- to 4-week, 2- to 3-month, 6-month, and 1-year follow-up.
The use of TAP blocks for postoperative pain control at the author’s institution has been associated with favorable empirical results. The authors hypothesized that the use of TAP blocks for regional anesthesia in the setting of ALIF would result in reduced postoperative narcotic consumption and improved postoperative pain scores without a significant effect on perioperative complications or LOS.
Methods
This retrospective medical record review study involving human participants was in accordance with the ethical standard of the Institutional and National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (institutional review board) of the authors’ institution approved this study. Informed consent was waived.
Data Collection
A retrospective review of 150 consecutive patients undergoing elective ALIF, with or without a staged instrumented PLF on the same day of surgery, from July 2019 to August 2020 was conducted. Any patient undergoing revision spine surgery with previous instrumentation was excluded. Patients were also excluded if they were younger than 18 or older than 90 years, had surgery for spine trauma or neoplasms, or had an allergy to any component of the local anesthetic used for a TAP block. These criteria resulted in a total of 99 patients being included in the analysis. Patients who received a preoperative TAP block were identified as the case group, and those who did not were designated as the control group. Demographic data collected through an electronic medical record review included age, sex, body mass index (BMI), tobacco use history, surgical history, drug abuse history, current or prior enrollment in pain management, type of surgery, and number of levels involved in the fusion. The primary outcome of interest was total opioid consumption calculated through MME from POD 0 to 5. Additionally, MME from the day of surgery (postoperatively) until POD 2 (POD 0–2) were calculated. Secondary outcomes collected included LOS, VAS pain scores (0–10 scale), and any complications from the TAP block. Patients were excluded if they had any thoracic involvement of their fusion, were younger than 18 years, had a previous lumbar fusion surgery, had a history of spinal trauma or neoplasm, or had an allergy to any component of the local anesthetic used for a TAP block.
TAP Block
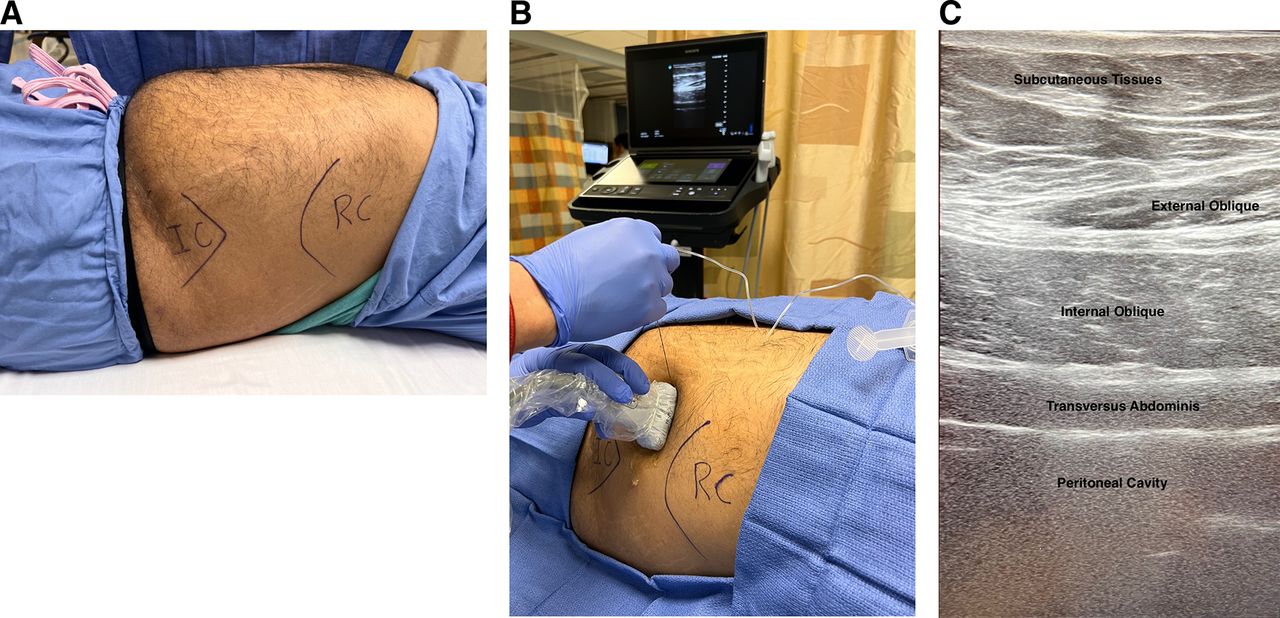
All TAP blocks were performed preoperatively by a qualified anesthesiologist and on the ipsilateral side of the planned surgical incision. Based on patient comfort, they are positioned either supine or in the lateral decubitus position. An ultrasound probe is placed at the midclavicular line in between the anterior superior iliac spine and subcostal margin to obtain a view of the abdominal wall layers (Figure 1). A 22G echogenic needle is advanced under ultrasound guidance until the tip is between the internal oblique and transversus abdominis muscles. At our institution, either 0.5% bupivacaine or a bupivacaine liposomal injectable suspension is used. Dosage is usually between 25 and 30 mL.
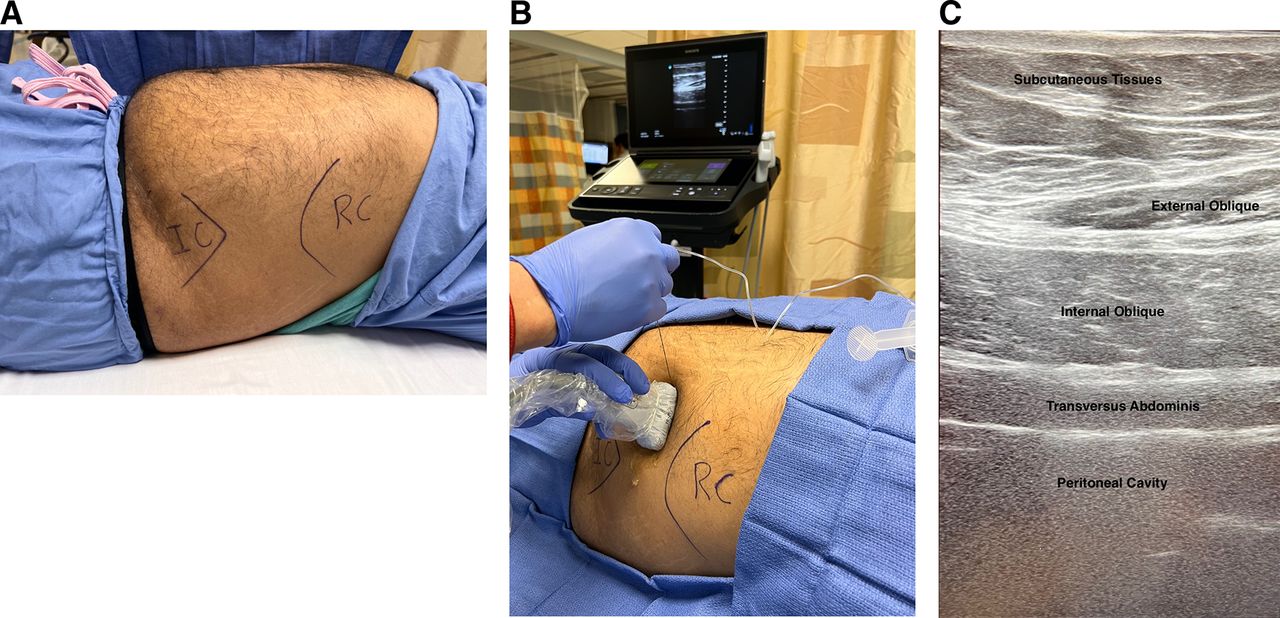
(A) Patient is placed supine for the transversus abdominis plane (TAP) procedure. Skin is marked for level of rib cage (RC) and iliac crest (IC). (B) TAP procedure performed with ultrasound guidance through the lateral abdominal wall using a 21G × 100-mm needle. (C) Lateral abdominal wall layers demonstrated with ultrasound image. Layers are labeled from superficial (superior) to deep (inferior).
Surgical Approach and Procedure
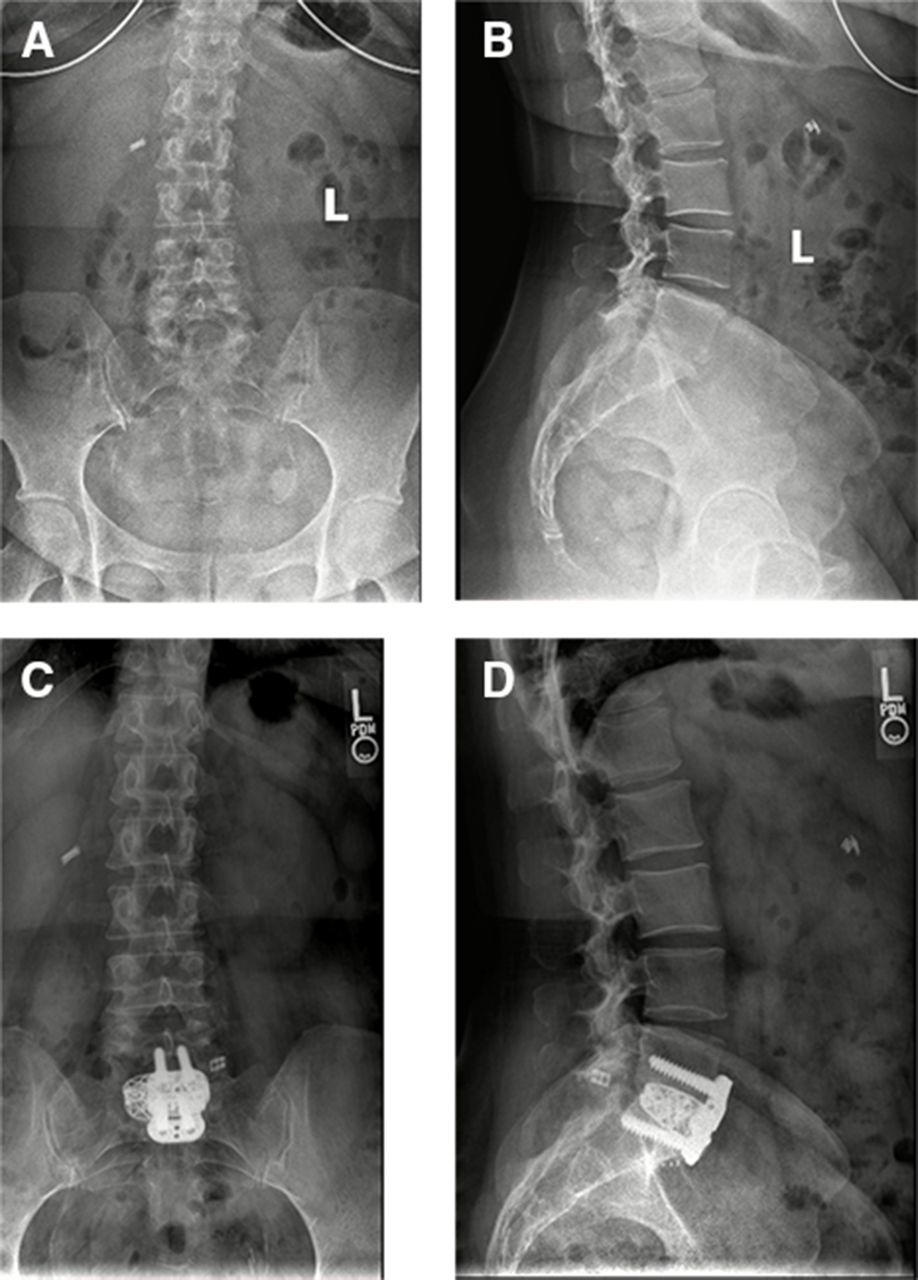
Patients were either placed supine for a vertical pararectal approach or in the lateral decubitus for a more oblique lumbar interbody fusion approach. A muscle-sparing approach was utilized in all patients to access the desired operative levels. For instrumentation, all patients had anterior plating in addition to placement of an interbody graft (Figure 2). None of the patients included in this retrospective review had neuromonitoring during the surgery, either in the form of somatosensory-evoked potentials or motor-evoked potentials.
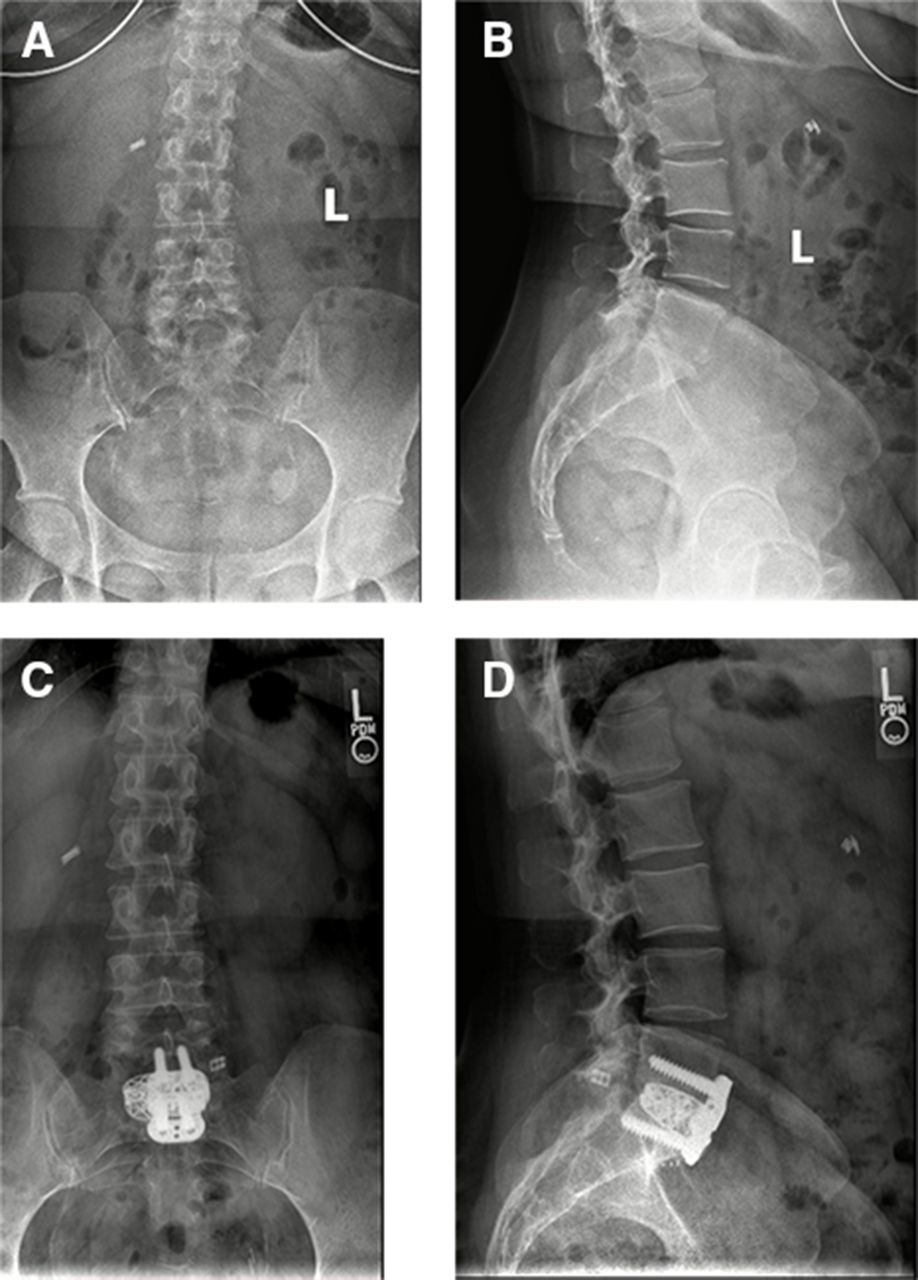
Preoperative and postoperative lumbar x-ray images of a 56-year-old patient who underwent an anterior lumbar interbody fusion. (A) Preoperative anterior-posterior (AP), (B) preoperative lateral, (C) postoperative AP, and (D) postoperative lateral views.
Statistical Analysis
Comparative analysis was carried out between all patients who received a perioperative TAP block and those who did not. Subgroup analysis was also carried out between cases and controls who underwent isolated ALIF and those who underwent staged ALIF/PLF.
Statistical analyses were performed with IBM SPSS Statistics version 27.0 (IBM Corporation, Armonk, NY, USA). Tests were conducted 2-tailed and an α level of <0.05 indicated statistical significance. Demographic variables are expressed as frequencies (percentage) for categorical variables and mean ± SD or median (interquartile range [IQR]) for continuous and ordinal variables. Normality was assessed by Shapiro-Wilk test (P > 0.05). Independent samples t test was conducted to determine significant differences in normally distributed variables. Homogeneity of variances was assessed by Levene’s test (P > 0.05). Mann-Whitney U test was conducted to determine significant differences in non-normally distributed and ordinal variables. χ 2 test or Fisher’s exact test was conducted to determine significant differences in categorical variables.
Multiple linear regression was used to determine significant predictors of POD 0 to 2 MME consumption. Age, TAP use, sex, preoperative opioid use, BMI, presence of diabetes, previous pain management, and smoking status were all included in the model. Natural logarithmic transformation was applied to POD 0 to 2 MME consumption to adjust skewness. Linearity was confirmed by partial regression and studentized residuals against the predicted value plots. Durbin-Watson statistic confirmed independence of residuals (2.131). Homoscedasticity was confirmed by a studentized residuals vs unstandardized predicted values plot. Multicollinearity was absent as assessed by tolerance values greater than 0.1. One standardized residual greater than ± 3 SDs and 1 leverage value of 0.2 remained in the analysis. There were no values for Cook’s distance greater than 1.0. P-P plot confirmed normality.
Results
Demographics
Among the 99 total patients, 47 were included in the TAP group and 52 in the control group. Patient characteristics were comparable between groups (Table 1). Patient characteristics were similar in age (median 58.0 vs 64.0 years), sex (men 48.9% vs 59.6%), BMI (mean 30.5 vs 30.5 kg/m²), tobacco history (36.2% vs 44.2%), drug abuse history (4.3% vs 11.5%), previous pain management (40.4% vs 51.9%), number of levels involved in surgery (median 1.0 vs 1.0), and surgery type (ALIF/PLF 63.8% vs 61.5%; ALIF alone 36.2% vs 38.5%).
Summary of patient characteristics.
Primary Outcome Data
Patients who received a TAP block required less daily and cumulative early postoperative MME (Table 2). During POD 0 to 2, the TAP group (median 124.0, IQR 86.4–173.0 MME) consumed significantly less total MME than the control group (median 151.1, IQR 113.0–196.2 MME) (P = 0.036). A similar result was seen for cumulative opioid consumption from POD 0 to 5, with the TAP group (median 190.0, IQR 115.0–262.0 MME) consuming significantly less total MME than the control group (median 240.7, IQR 157.7–345.6) (P = 0.05). VAS pain scores revealed no significant differences except for POD 3 and 4 in which the TAP group reported lower pain scores (Table 3). There were no significant differences in LOS.
Postoperative day opioid consumption and hospital length of stay.
Postoperative day visual analog scale scores.
Subgroup Analysis
Subgroup analysis of patients who underwent only ALIF (without staged PLF) demonstrated that patients who received a TAP block required significantly less MME from POD 0 to 2 (median 99.2, IQR 62.2–182.2 MME) compared with the control group (median 152.5, IQR 112.0–211.5 MME) (P = 0.026). However, improvement in VAS pain scores was not significant, and there was a difference in LOS (Tables 4 and 5).
Anterior lumbar interbody fusion subgroup patient characteristics.
Anterior lumbar interbody fusion subgroup analysis postoperative day opioid consumption and hospital length of stay.
A subgroup analysis of patients who underwent ALIF with staged PLF demonstrated a significant difference in pain scores on POD 3 and 4 and a significantly lower MME consumption on POD 0. There was no difference in LOS.
Predictors of MME Consumption
A multiple linear regression model including the previously outlined variables identified TAP use, male sex, and age as significant predictors of POD 0 to 2 MME consumption (F[8, 88] = 4.304, P < 0.001, adjacent R 2 = 0.216) (Table 6). Men consumed 31.4% more MME, each year increase in age decreased MME consumption by 1.9%, and TAP use decreased MME consumption by 29.9%.
Multiple regression results for logarithmic postoperative day 0 to 2 opioid consumption.
Discussion
The TAP block was originally implemented for use in intra-abdominal general, gynecologic, and urologic surgical procedures involving the anterolateral abdominal wall.6,8 Potential benefits of TAP block include decreased postoperative nausea/vomiting, decreased early postoperative opioid consumption, and reducing time to first opioid administration.9 The original technique was first introduced by Rafi in 2001 and did not utilize ultrasound but rather landmarks and fascial “pop” for localization.10 Since then, its use has become much more frequent, and ultrasound localization has been added.11 Utilization of the TAP block in spine surgery in the setting of ALIF and lateral lumbar interbody fusion, however, is a relatively novel application with limited evidence in the literature.3,12
Previous studies have investigated local anesthetic infiltration with TAP block in the setting of lower abdominal surgery and found lower pain scores at 24 hours postoperatively and increased patient satisfaction.13,14 A small retrospective study found no difference between TAP block and thoracic epidural injection in pain scores with the only reported complications (hypotension and ineffective coverage) occurring in the TAP group.15 A randomized controlled trial of patients undergoing abdominal wall surgery found reduced morphine consumption, decreased pain scores, improved sedation scores, and decreased pain scores all in the first 24 hours postoperatively without TAP block complication.16
Given the broad usage and effectiveness of TAP block for various lower abdominal surgeries, the addition of TAP block to perioperative protocols for ALIF presents a significant opportunity for investigation. The present study demonstrates decreased early postoperative MME consumption in patients receiving a preoperative TAP block prior to undergoing an ALIF. Although no difference was seen in mean VAS pain scores, patients experienced similar pain control with decreased narcotic needs relative to those patients who did not receive a TAP block. No increase in perioperative or overall complications was seen with TAP block use, which is consistent with prior studies in the literature.17 When controlling for confounding variables in the regression analysis, age and TAP block use were the only significant predictors of decreased early postoperative MME consumption in the present study.
The potential benefits of TAP block utilization are accompanied with a considerably low risk of complications. Theoretical risks include systemic toxicity from the anesthetic, intraperitoneal needle penetration, and unintentional fascia iliacus or femoral nerve blockade.17 Ultrasound guidance for TAP block should reduce these potential complications to near zero; however, patients should still be informed of these potential risks during the informed consent process. None of the 47 patients who received the TAP block had a complication from the procedure. Reported contraindications for TAP block are patient refusal, infection of the skin or abdomen near injection sites, or other impediment to the needle insertion site.17 A study investigating difficulty of the TAP procedure based on patient factors was unable to find any difference based on patient age, weight, BMI, length of surgery, intravenous fluid administration, or operative changes.18
To our knowledge, there is only 1 other study that conducted a comparative analysis of the TAP block in the setting of lumbar spine surgery.7 The authors demonstrated very high efficacy and patient acceptance of a perioperative TAP block and saw no adverse events related to its use.12 They compared TAP block with traditional postoperative pain management regimens and found an association between TAP block and decreased LOS, decreased postoperative nausea/vomiting, and decreased opioid consumption in the postanesthesia care unit.7 The group of patients in this study who received TAP blocks were found to be both significantly younger and healthier with regard to American Society of Anesthesiologists classification, representing a possible selection bias. The results of the study by Reisener et al, however, offer complementary findings to the present study in favor of TAP block utilization. Although these early, retrospective studies show promise regarding TAP block implementation for ALIF, prospective, randomized trials are needed to confirm these results. Given the low risk of TAP block complication, however, the authors feel that strong recommendation for regional nerve blockage should be given in the setting of ALIF with proper personnel, equipment, and training.
In regard to ALIF alone vs ALIF with combined PLF, TAP block was not found to be more effective with regard to early postoperative pain control in the combined ALIF/PLF patient cohort. There was no significant difference in MME consumption between those with and without TAP block, indicating that TAP is likely not sufficient as a regional anesthetic to reduce early postoperative opioid use in patients undergoing combined anterior and posterior fusion. Augmentation with an erector spinae plane block, for example, could serve as an adjunct in this group, but this was not investigated in the current study. In those undergoing ALIF alone, however, TAP use was found to have an influential effect on decreased MME.
There are several limitations to the present study. First, the retrospective nature of the data collection places it at risk for selection bias. Although patients were not randomized, the authors attempted to decrease this risk by including a cohort of consecutive patients during a specified time frame with strict inclusion and exclusion criteria. Second, some patients were lost to follow-up after 2 to 4 months postoperatively, which places the results at an increased risk for attrition bias on VAS pain scores at 6 months (57.4% follow-up) and 1 year (38.3% follow-up). Last, there were no standardized criteria for selection of patients who received TAP blocks. The decision to forego the intervention was left at the discretion of the treating spine surgeon, anesthesiologist, and patient preference.
Conclusion
The goal of MMA is to provide adequate analgesia using alternative strategies, such as the TAP block, to decrease reliance on opioids for postoperative pain control. TAP block offers a useful adjunct to control pain in the immediate postoperative period for patients undergoing ALIF. Findings of the present study demonstrate lower MME utilization in patients who received a perioperative TAP block during the early postoperative phase without significant difference in VAS pain scores and no increase in complications. Use of perioperative TAP block in the setting of ALIF may produce similar pain control with less overall daily MME in the early postoperative period and may in turn help patients reduce their risk of the side effects associated with increased opioid use. For patients undergoing ALIF with combined PLF, alternative pain control options should continue to be explored. Prospective randomized controlled trials are needed to further elucidate the benefits of this intervention in patients undergoing lumbar interbody fusion through an anterior or lateral approach.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval University of Tennessee College of Medicine Institutional Review Board approved this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.