


Abstract
Background Patients with ankylosing spondylitis (AS) are prone to spinal fractures even after low-energy trauma. Posterior fusion through open surgery has been the standard procedure for spinal fractures in patients with AS. Minimally invasive surgery (MIS) has been proposed as an alternative treatment option. There are few literature reports regarding patients with AS being treated for spinal fractures with MIS. This study aims to present the clinical outcome of a series of patients with AS treated with MIS for spinal fractures.
Methods We included a consecutive series of patients with AS who underwent MIS for thoracolumbar fractures between 2014 and 2021. The median follow-up was 38 (12–75) months. Medical records and radiographs were reviewed, and data on surgery, reoperations, complications, fracture healing, and mortality were recorded.
Results Forty-three patients (39 [91%] men) were included with a median (range) age of 73 (38–89) years. All patients underwent image-guided MIS with screws and rods. Three patients underwent reoperations, all due to wound infections. One patient (2%) died within 30 days and 7 (16%) died within the first year after surgery. Most patients with a radiographic follow-up of 12 months or more (29/30) healed with a bony fusion on computed tomography (97%).
Conclusion Patients with AS and a spinal fracture are at risk of reoperation and have significant mortality during the first year. MIS provides adequate surgical stability for fracture healing with an acceptable number of complications and is an adequate choice in treating AS-related spinal fractures.
Level of Evidence 4
Introduction
Ankylosing spondylitis (AS) is a chronic, seronegative, and systemic inflammatory disease with progressive enthesopathy causing erosion of the joints, discs, and ligaments of the spinal column followed by ossification and autofusion of the spine.1,2 Patients with AS have a high prevalence of extra-articular manifestations (eg, lung fibrosis, emphysema, psoriasis, and osteoporosis) and cardiovascular pathologies.3–6 The prevalence of AS in Sweden has been estimated to be 0.18% to 0.24%, with the highest prevalence in the Northern region.7–9 Autofusion of the spine, in conjunction with secondary osteopenia, leaves patients with AS susceptible to fractures.2,10,11 The fractures are usually unstable because of a long lever arm, and surgical treatment with long constructs is often required to withstand shearing forces across the fracture site.12,13
Posterior fusion through open surgery has been the standard procedure for spinal fractures in patients with AS.13–15 Minimally invasive surgery (MIS) has been proposed as an alternative treatment option that could limit bone fusion because of the absence of bone grafting. There are few literature reports on patients with AS treated for spinal fractures with MIS.16–23 Therefore, this study aims to present clinical outcomes in a series of patients with AS treated with MIS for thoracolumbar spinal fractures.
Materials and Methods
Study Design and Setting
This study is a retrospective cohort study that includes patients with thoracolumbar fractures and AS. The study was conducted at the Department of Orthopedics at Umeå University Hospital between January 2014 and December 2021. Umeå University Hospital is a level 1 trauma center affiliated with Umeå University and has a catchment area for spinal trauma surgery of approximately 900,000 inhabitants.
Data Collection and Follow-Up
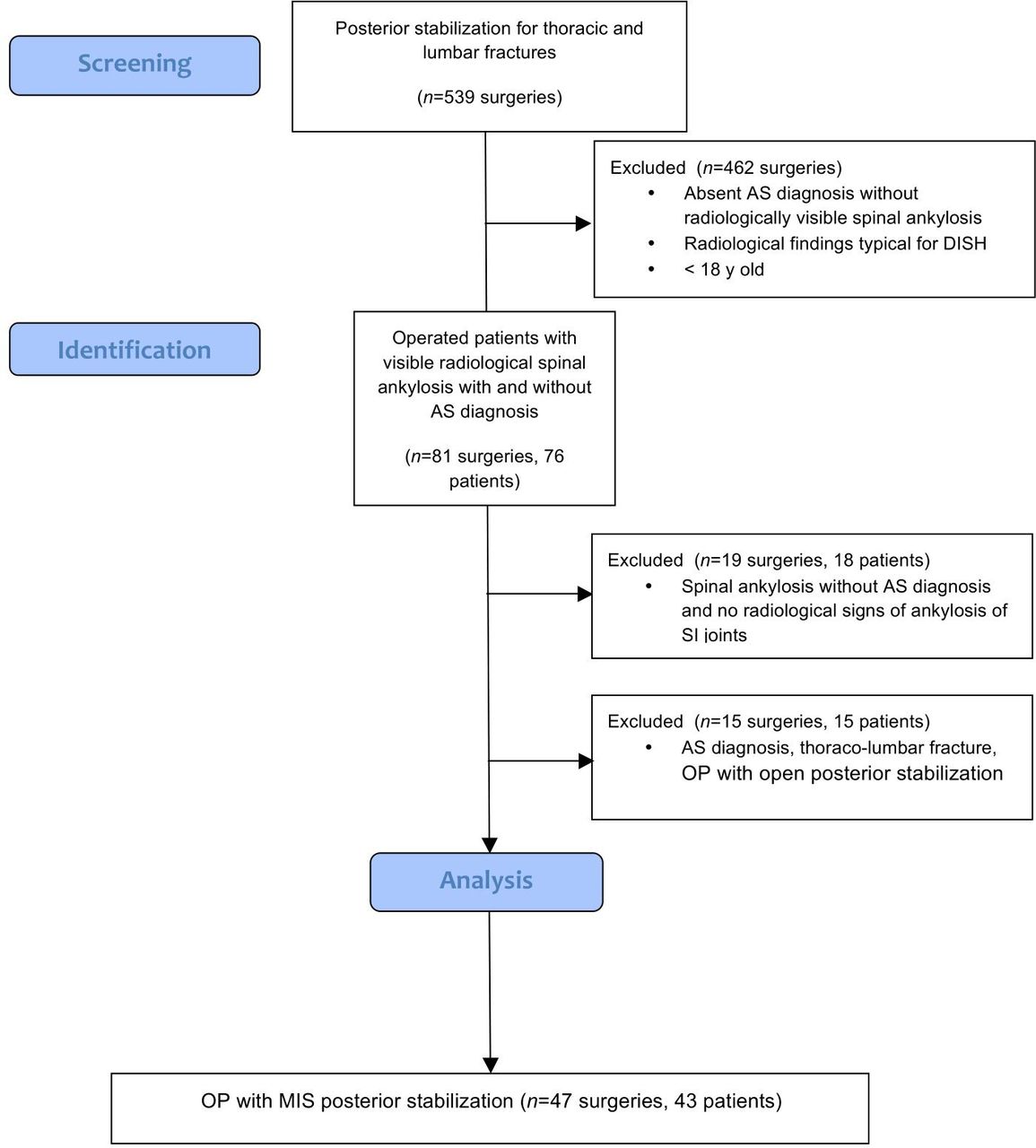
We included a consecutive series of patients older than 18 years who underwent surgery for unstable thoracolumbar fractures due to AS. Patients with type A fractures, treated with open surgery, pathological fractures, osteoporosis, or diffuse idiopathic skeletal hyperostosis (DISH) were excluded.24 For the exclusion of patients with DISH, we used the criteria from Resnick et al that state at least 2 to 3 adjacent vertebrae have to show bony bridges with nearly normal intervertebral discs and without sacroiliac or apophyseal joint fusion.25 Additionally, all patients without previous AS diagnosis, regardless of the presence of ankylosis in the spine, were investigated using New York criteria with radiological evaluation of sacroiliac joints for the presence of ankylosis.26 Patients without a previously documented diagnosis of AS and/or radiological signs of ankylosis of the sacroiliac joints were excluded from the study because of suspicion of DISH changes falsely diagnosed as AS. A flowchart of the selection process is provided in Figure 1.

Flowchart of patients. AS, ankylosing spondylitis; DISH, diffuse idiopathic skeletal hyperostosis; MIS, minimally invasive surgery; SI, sacroiliac.
We used the unique personal identification number given to all permanent residents of Sweden to collect data, including a review of medical records. Patient data included age, sex, American Society of Anesthesiologists classification, cognitive impairment, initial treatment, pre- and postoperative neurological function according to the American Spine Injury Association (ASIA),27 comorbidity, reoperation, and date of death. Reoperation and mortality were recorded until October 2022.
Radiographic Assessment
Anatomical level and fracture classification according to the AO Spine thoracolumbar classification system were obtained through preoperative computed tomography (CT). Magnetic resonance imaging was performed to evaluate the posterior column, intraspinal traumatic compression (hematoma), and instability. Postoperative bone fusion was assessed with CT at the last postoperative follow-up. Fusion was defined as visible bone-bridging callus across the fracture.
Outcome Measurements
Reoperation was defined as undergoing a secondary surgical procedure (eg, failure of fixation with subsequent implant loosening, surgical debridement, antibiotics, and implant retention due to deep postoperative infection). Minor reoperation was defined as the removal of an implant after subsequent healing of the fracture. Bony fusion was defined as visible bridging trabeculations with or without bony remodeling and callus formation across the fracture.
Medical complications were defined according to Lebude et al.28 Neurological deficits were determined using the ASIA score, where only clinically significant sensory and motor deficits were regarded as neurological deficits.27 Significant motor deficits were defined as a reduced function of 1 or more myotomes with an ASIA score of 3/5 or less. Significant sensory deficits were defined as an ASIA score of 1/2 or less in 2 or more dermatomes.
Implant and Surgery
Surgeries were performed under general anesthesia in a prone position on a Jackson table. The chest roll, iliac crest, and thigh support in different shapes and sizes accommodated the kyphotic deformity. Patients with severe thoracolumbar deformities were also positioned on the Jackson table, however, without thigh support with legs hanging in the hammock to adjust for the curvature to minimize the risk of additional extension and translation across the fracture. Antibiotic prophylaxis was given in 3 doses of 2 g of cloxacillin (Ekvacillin, Meda, Sweden) at 0.5 hours before and 2 and 6 hours after the start of surgery. Clindamycin (Dalacin, Pfizer AB, Sweden) was used in patients with anaphylaxis to penicillin in 3 doses of 600 mg at the beginning of surgery and then at 8-hour intervals. In 6 patients, 1 preoperative dose of broad-spectrum antibiotics, either cefuroxime or cefotaxim, was used (Zinacef, GlaxoSmithKline, Sweden and Claforan, Sanofi AB, Sweden) because of suspected pneumonia. Therapy continued with 1 dose every 8 hours daily for 10 days. Thromboprophylaxis with subcutaneous low molecular weight heparin (Fragmin, Pfizer AB, Sweden or Innohep, LEO Pharma, Denmark) was given for 10 days. Under the supervision of a physiotherapist, all ambulatory (ASIA E, D) patients were mobilized to full weight bearing on the first postoperative day. Patients with a neurological deficit (ASIA A, B, C) were referred for neurorehabilitation. Passive mobilization to a sitting position was initiated on the first postoperative day to prevent postoperative complications. All surgeries were performed by a consultant orthopedic surgeon or neurosurgeon specialized in spine surgery.
Minimally Invasive Surgery
For MIS procedures, either Everest (K2M, Leesburg, VA, USA, N = 14) or Longitude II (Medtronic, Minneapolis, MN, USA, N = 29) was used. The first step of the procedure was the attachment of the reference frame to the spinal process at the most caudal vertebrae included in instrumentation. In case instrumentation extended over more than 5 segments, double registration was required. After that, cannulated polyaxial screws were implanted percutaneously with the assistance of guide wires using navigated instruments in combination with O-arm connected to StealthStation (Medtronic, Sofamor Danek, Memphis, TN, USA) in all cases. Intraoperative image acquisition was performed to control the position of the implanted screws. The rods were placed bilaterally, inserted subfascially, and locked. A central decompression was performed in 1 patient with ASIA C. After hemostasis and wound washout, stabs (N = 19) or midline incisions (N = 24) were closed in layers in a watertight fashion. Decortication, bone harvesting, and implantation were not performed in any cases.
Statistics
Descriptive statistics for continuous variables are presented as medians with ranges and categorical data as numbers and percentages. Postoperative survival was estimated using the Kaplan-Meier method with death as an event. The statistical package SPSS for Mac (version 26.0; IBM Corp., Armonk, NY, USA) was applied for statistical analyses.
Ethics
The study complied with the ethical principles of the Helsinki declaration and was approved by the Swedish Ethical Review Authority (DNR 2019-01068 and 2021-06873-02).
Results
Patients and Descriptive Data
In all, 43 patients (39 men and 4 women) were included and 495 were excluded (Figure 1). The median age at the time of surgery was 73 (38–89) years (Table 1). Three patients (7%) presented with neurological deficits; 1 of them suffered from paraplegia years before the trauma. Two patients were classified as ASIA A and 1 as ASIA C but with a Brown-Sequard pattern with a motor deficit in the right leg. The 2 patients with ASIA A did not recover after surgery, whereas the patient with ASIA C recovered completely to ASIA E. The trauma mechanism was low energy in 33 patients and high energy in 10 (Table 2). Median follow-up was 38 (12–75) months. One patient (2%) died within 30 days and 7 (16%) died within the first year after surgery.
Clinical characteristics of patients undergoing minimally invasive surgery for ankylosing spondylitis.
Details on surgery, levels of fixation, and trauma (N = 43).
Fracture Classification
The proximal level of the fracture was most commonly located in the thoracic spine (n = 36); 7 fractures were located only in the lumbar (n = 6) or the lumbar and sacral spine (n = 1). Two patients had a fracture classified as B2; all the other fractures were classified as B3 according to AO/Orthopaedic Trauma Association classification. The most common fracture site was between T9 and L1 vertebrae (n = 31). Two patients (4%) sustained more than 1 fracture.
Surgical Treatment
All patients underwent a posterior approach with pedicle screws and fixation with rods. Three patients underwent more than 1 surgery (2 patients were operated on twice and 1 patient 3 times) because of repetitive trauma and adjacent fractures. The median (range) surgical duration was 140 (80–300) minutes and blood loss was 100 (50–410) mL (Table 2).
Radiographic Assessment
Fusion at 12 months or more with follow-up CT examinations (Figure 2) could be seen in 29 of 30 patients (97%). Only 1 patient showed no visible fusion. This patient had a partial fusion but did not require revision. Four patients canceled the 1-year follow-up CT examination due to no pain, 7 patients died, and 2 patients did not return at the 1-year follow-up.

Preoperative and 1 y postoperative computed tomographic images.
Reoperations
Three patients underwent reoperations because of wound infections (1 superficial and 2 deep infections). Loosening of 2 proximal screws was encountered in 2 patients. Loosening was discovered during the revision of deep wound infection.
Complications
Complications were seen in 11 patients (26%). Systemic postoperative complications occurred in 7 patients (16%), whereas postoperative surgical complications were detected in 4 patients (9%) (Table 3). Five of 7 patients (71%) with systemic complications and 2 of 4 patients (50%) with postoperative surgical complications were classified as having major complications.
Medical and surgical complications.
Discussion
AS patients with a spinal fracture are at risk of reoperation and significant mortality during the first year. We found that MIS is a good choice with adequate surgical stability for fracture healing in the present population. The literature on surgical treatment in AS patients is sparse, with limited studies on MIS in AS patients with a thoracolumbar fracture.16–23,29,30 Most of these studies are case series, including patients with DISH. We excluded all patients with DISH due to different prevalence, pathology, demographic, and mechanical features to focus solely on AS patients.31–36
The combination of a rigid spinal column and osteopenia results in a 10× increased risk of spinal fractures and a higher incidence of neurological deficits compared with non-AS patients.37 Therefore, surgical stabilization with long posterior constructs with screws and rods is recommended to maintain mechanical stability, prevent secondary injury, and enable bony fusion.12,13
The overall complication rate after surgery for spinal fractures in patients with AS varies between 30% and 90%.12,15,38–41 Patients with AS have a high prevalence of cardiovascular pathologies with a significantly increased risk of cardiac-related mortality compared with the general population.4,5,12 Puvanesarajah et al reported significantly higher surgical site infection, transfusion rate, respiratory failure, pneumonia, and acute renal failure in AS patients compared with proportion-matched groups without AS.39 Open surgery is considered a standard procedure for AS patients with thoracolumbar fractures but is associated with significant postoperative morbidity.12,40,42 Open surgery requires considerable exposure and extensive dissection of fascia and muscles, causing injury to the small vessels and nerves surrounding the spinal column.15 Prolonged surgery in a prone position in patients with a high prevalence of comorbidities could adversely affect the risk of postoperative complications.3,6 The rationale for using MIS is that a shorter surgical duration with lesser surgical soft tissue trauma and perioperative blood loss would minimize postoperative pain and facilitate mobilization and fracture healing. The skepticism in using MIS stabilization to treat fractures in AS patients is usually related to 3 issues: radiation exposure, screw misplacement, and risk of pseudarthrosis. MIS fixation in patients with high body index and/or advanced deformity, especially in upper thoracic region, can be technically demanding without the use of navigation. However, all consecutive patients in our study underwent operations with an image-guided technique that provides higher precision of screw placement in spinal surgery and limits exposure to radiation for the surgeon and the operating team.43–45 Recent evidence suggests that MIS provides sufficient fracture stabilization with reduced risk of complications compared with open surgery.17,22
The use of MIS in AS patients seems promising, but previous studies were of level 3 or 4 evidence with a few cases or included a mix of patients with DISH and AS.16,17,23,30 Most patients in our study who underwent radiological follow-up developed bony fusion, despite being treated without bone grafting. The pathophysiology of AS facilitates autofusion by osteoproliferation and ankylosis.1 Several studies support our findings of the high fusion rate in AS patients despite using MIS.17,18 Few of our patients suffered from spinal cord injuries because of the fracture, which is consistent with findings reported by Lukasiewicz et al.38 However, other reports found higher incidences of spinal cord injuries (up to 33%–50%) in cases with AS and thoracic and thoracolumbar fractures.37,40,46,47 We found a 30-day mortality rate of 2% and a 1-year mortality rate of 16%. The 1-year mortality rate has been reported to be between 17% and 56%,12,15,23,41 with in-hospital mortality between 6% and 7%,13,38,40 though mortality rates up to 28% have also been presented.46
Strengths and Limitations
The main limitation of this study relates to the inherited flaws of the retrospective design. Another limitation is the small sample size that prevents statistical analysis from identifying covariates associated with the outcome. Additionally, some clinical factors and details could not be assessed from the medical records and limited completeness of radiologic follow-up with a high rate of loss to follow-up. Despite these limitations, our study is the largest consecutive single-center cohort of patients with AS treated for thoracolumbar fractures with navigated MIS. We investigated a highly selected cohort by excluding all patients with potential DISH to provide reliable data without confounding conditions with possible differences in prevalence, etiology, pathophysiology, skeletal changes, and biomechanics.
Conclusion
Patients with a spinal fracture due to AS are at risk of reoperation and have significant mortality during the first year after injury. Our study shows that MIS provides adequate surgical stability for fracture healing and is a viable alternative to open surgery with less risk of soft tissue injury.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.