


Abstract
Background In patients undergoing spine surgery for renal cell carcinoma (RCC), we sought to: (1) describe patterns of postoperative targeted systemic therapy and radiotherapy (RT), (2) compare perioperative outcomes among those treated with targeted systemic therapy to those without, and (3) evaluate the impact of targeted systemic therapy and/or RT on overall survival (OS) and local recurrence (LR).
Methods A single-institution, retrospective cohort study of patients undergoing spine surgery for metastatic RCC from 2010 to 2021 was undertaken. Treatment groups were RT alone, targeted systemic therapy alone, dual therapy consisting of RT and targeted systemic therapy, and neither therapy. Multivariable Cox regression controlled for age, race, sex, insurance, and preoperative targeted systemic therapy.
Results Forty-nine patients underwent spine surgery for RCC. Postoperatively, 4 patients (8%) received RT alone, 19 (38.8%) targeted systemic therapy alone, 12 (24.5%) dual therapy, and 13 (28.6%) neither. All groups were similar in demographics, preoperative Karnofsky Performance Score (P = 0.372), tumor size (P = 0.413), readmissions (P = 0.884), complications (P = 0.272), Karnofsky Performance Score (P = 0.466), and Modified McCormick Scale (P = 0.980) at last follow-up. Higher 1-year survival was found in dual therapy (83.3%) compared with other therapies. OS was significantly longer in patients with dual therapy compared with other therapies (log-rank; P = 0.010). Multivariate Cox regression (HR = 0.08, 95% CI = 0.02–0.31, P < 0.001) showed longer OS in dual therapy compared with other therapies. Seven patients (14.3%) experienced LR, and a similar time to LR was found between groups (log-rank; P = 0.190).
Conclusion In patients undergoing metastatic spine surgery for RCC, postoperative dual therapy demonstrated significantly higher 1-year survival and OS compared with other therapies.
Clinical Relevance Multidisciplinary management of metastatic RCC is necessary to ensure timely implementation of targeted systemic therapy and RT to improve outcomes.
Level of Evidence 3.
Introduction
Renal cell carcinoma (RCC) is one of the most commonly diagnosed cancers in the United States, with an estimated 76,080 new cases in 2021.1,2 About one-third of patients with RCC progress to metastasis, with 18% to 30% of patients presenting with metastasis at the initial diagnosis.3,4 The lungs are the most common site of metastasis (70%), followed by bony metastasis (32%), 40% of which occurs in the spine.5,6 Although surgery can restore neurological function and spinal stability, appropriate regimens of postoperative radiotherapy (RT), chemotherapy, and targeted systemic therapy are needed to minimize disease progression.7,8
Targeted systemic therapy has greatly improved the prognosis of patients with RCC, specifically tyrosine kinase inhibitors (TKIs) that target vascular endothelial growth factors, such as sunitinib and pazopanib.9 Sunitinib outperformed standard interferon-alpha therapy in progression-free survival and overall survival (OS), as well as objective response rate.10,11 Similarly, pazopanib has shown substantially higher response rates and longer progression-free survival than placebo.12 Targeted systemic therapy represents an efficacious treatment regimen, particularly in patients with advanced disease.13,14 However, patients undergoing spine surgery require considerable recovery to improve their performance status and ambulation. There is a paucity of research evaluating the impact of new targeted systemic therapy in patients undergoing surgery for RCC spinal metastases, particularly when combined with RT.15
Given the lack of studies investigating the efficacy of postoperative targeted systemic therapy, potentially combined with RT, in patients undergoing spine surgery for metastatic RCC, we sought to further investigate this topic. In a cohort of patients undergoing metastatic spine surgery for RCC, the current objectives were to (1) describe patterns of postoperative targeted systemic therapy and RT, (2) compare perioperative outcomes among those treated with targeted systemic therapy to those without, and (3) evaluate the impact of targeted systemic therapy and/or RT on OS and local recurrence (LR).
Materials and Methods
Study Design
A single-institution, multisurgeon, retrospective cohort study was undertaken for patients undergoing metastatic spine surgery from 2010 to 2021. Vanderbilt University Medical Center’s Institutional Review Board (IRB) approval was obtained for this study (IRB#211900). Signed consent for participation was obtained from all patients.
Patient Population
Registry data were obtained for patients who underwent spine surgery for metastatic RCC between 2010 and 2021. Adult patients (aged ≥18 years) with metastatic, extradural RCC to the spine who underwent spine surgery for tumor resection and stabilization were included. Exclusion criteria consisted of pediatric patients (<18 years old), intradural tumors, and non-RCC histology. The date of the last follow-up was extended to the date of death or the date of the last clinical follow-up.
Independent Variable
The primary exposure variable of interest was the choice of postoperative adjuvant treatment received, which was divided into 4 groups: (1) RT alone, (2) targeted systemic therapy alone, (3) dual therapy (which included both RT and targeted systemic therapy), and (4) neither therapy. Targeted systemic therapy included either monoclonal antibodies, such as pembrolizumab, nivolumab, and ipilimumab, or TKIs that target vascular endothelial growth factors, such as sunitinib, pazopanib, cabozantinib, sorafenib, axitinib, and tivozanib.
Additional independent variables included preoperative and operative variables. Preoperative variables included the following demographics: age, sex, body mass index, and comorbidities, as well as the tumor’s primary organ. Operative variables included functional and pain status at presentation, categorized into biological, neurological, and mechanical pain.16 Biological pain refers to pain that arises directly from the tumor itself or from the biological processes associated with tumor growth and invasion, which is typically deep, dull, and poorly localized, often persisting even at rest.16 Neurological pain originates from the compression or infiltration of neural structures by the tumor, leading to nerve root irritation or spinal cord compression, and is described as sharp, shooting, or burning sensations that radiate along the distribution of affected nerves. Mechanical pain often arises from vertebral compression fractures, facet joint arthritis, or instability, is usually aggravated by specific movements or positions, and may be relieved with rest or changes in posture. Mechanical pain often presents as aching, throbbing, or stiffness localized to the affected area.16 All 3 types of pain can coexist. Other variables included tumor size and level, preoperative embolization, type of surgery, total instrumented levels, total decompressed levels, estimated blood loss, intraoperative monitoring changes, operative time, length of stay (LOS), and discharge disposition.
Outcome Variables
The primary outcomes were OS, 1-year survival, and LR. Additional secondary outcomes consisted of functional status as measured by the Karnofsky Performance Scale (KPS), neurological function measured by the Modified McCormick Scale (MMS), complications, readmissions, and reoperations, all at the last follow-up.
Surgical Procedure
The standard approach to extradural, metastatic RCC lesions was consistent with separation surgery, involving spinal cord decompression and long-segment posterior stabilization and fusion.17 Patients were most often taken for a posterior thoracic/lumbar approach, potentially involving a transpedicular approach or costotransversectomy to achieve adequate spinal cord decompression. For cervical lesions, an anterior corpectomy was sometimes needed based on the location and extent of spinal cord compression. The goal of adequate spinal cord decompression was to achieve 2 to 3 mm of separation between the tumor and the spinal cord, in addition to “reconstituting” the circular nature of the thecal sac, to achieve a safe distance from the spinal cord to the tumor for adequate dosing of radiation, stereotactic, or external beam. Intraoperative ultrasonography was often used to evaluate an adequate spinal cord decompression. Anterior column reconstruction was sometimes performed depending on the extent of kyphosis, the presence of a lytic lesion, and surgeon preference. Postoperative RT, whether stereotactic body radiation therapy (SBRT) or external beam radiation therapy, was decided by the treating radiation oncologist.
Statistical Analysis
Descriptive statistics were reported to compare patients with (1) RT alone, (2) targeted systemic therapy alone, (3) dual therapy, and (4) neither therapy. Mean and SD were reported for continuous variables and frequency for categorical variables. One-way analysis of variance test was used to compare continuous and ordinal baseline variables. χ 2 or Fischer’s exact test was used for categorical variables. Kaplan–Meier survival curves were performed, and the log-rank test was calculated for LR and OS. Cox regression was subsequently performed; a forest plot model was created to visualize the following covariates: age, race, sex, insurance, and preoperative targeted systemic therapy. A subanalysis was performed for patients with preoperative dual therapy, postoperative dual therapy, and neither therapy. A P value <0.05 was considered statistically significant. All analyses were performed using R version 4.1.3 (The R Foundation, Vienna, Austria).
Results
Patient Demographics and Preoperative Variables
Of 357 patients undergoing metastatic spinal surgery, 49 patients (13.7%) had metastatic RCC. Median (interquartile range) follow-up time was 542 (200–837) days. Mean age was 59.5 ± 10.0 years, and 33 (67.3%) were men. A total of 15 patients (30.6%) received preoperative, targeted systemic therapy, which consisted of monoclonal antibodies in 3 patients (6.1%), TKIs in 9 (18.4%), and a combination of both in 3 (6.1%; Table 1).
Demographics and preoperative data of patients undergoing spine surgery for metastatic renal cell carcinoma according to postoperative treatment received.
Postoperatively, 4 patients (8%) received RT alone, 19 (38.8%) targeted systemic therapy alone, 12 (24.5%) dual therapy, and 13 (28.6%) neither therapy. In patients receiving RT alone, only 2 patients (50.0%) received SBRT. In patients with dual therapy, 7 (58.3%) received SBRT. Thus, the proportions of SBRT were similar between both groups receiving radiation. With regard to targeted systemic therapy agents used, tyrosine kinase was the most common postoperative, targeted systemic therapy in the targeted systemic therapy alone group (63.2%) and dual therapy group (66.7%). Importantly, only 4 (8.2%) received monoclonal antibodies alone, and 7 (14.3%) received monoclonal antibodies in combination with tyrosine kinase. All treatment groups had comparable demographics. Of note, 45 patients (91.8%) were white, and race was not significantly different between treatment groups. In addition, 6 patients (50.0%) receiving dual therapy had private insurance, and 6 (42.9%) of neither therapy group were uninsured, with no significant difference in insurance type between groups (P = 0.536). No other differences were found in symptom duration (P = 0.477), comorbidities (P = 0.626), and the presence of other organ metastasis (P = 0.083; Table 1).
Perioperative Variables
All treatment groups were similar in types of pain, including mechanical pain (P = 0.426), biological pain (P = 0.255), neurological pain (P = 0.226), motor deficit (P = 0.164), preoperative KPS (P = 0.372), tumor size (P = 0.413), preoperative embolization (P = 0.490), and preoperative RT (P = 0.116). Intraoperatively, no significant differences were found in total decompressed levels (P = 0.341), total instrumented levels (P = 0.389), operative time (P = 0.051), estimated blood loss (P = 0.799), and LOS (P = 0.726; Table 2). Rates of costotransversectomies were similar among all groups (P = 0.365). LOS was higher in the RT group (13.8 ± 16.5 days) yet still not significantly different across groups (P = 0.726).
Perioperative and intraoperative variables of patients undergoing spine surgery for metastatic renal cell carcinoma according to postoperative treatment received.
Postoperatively, 12 patients (24.5%) had complications, 11 (22.4%) were readmitted, and 5 (10.2%) had reoperations at the time of the last follow-up, with no significant discernable differences among the 4 groups (Table 3).
Outcomes of patients by postoperative therapy for metastatic renal cell carcinoma.
OS and Local Recurrence
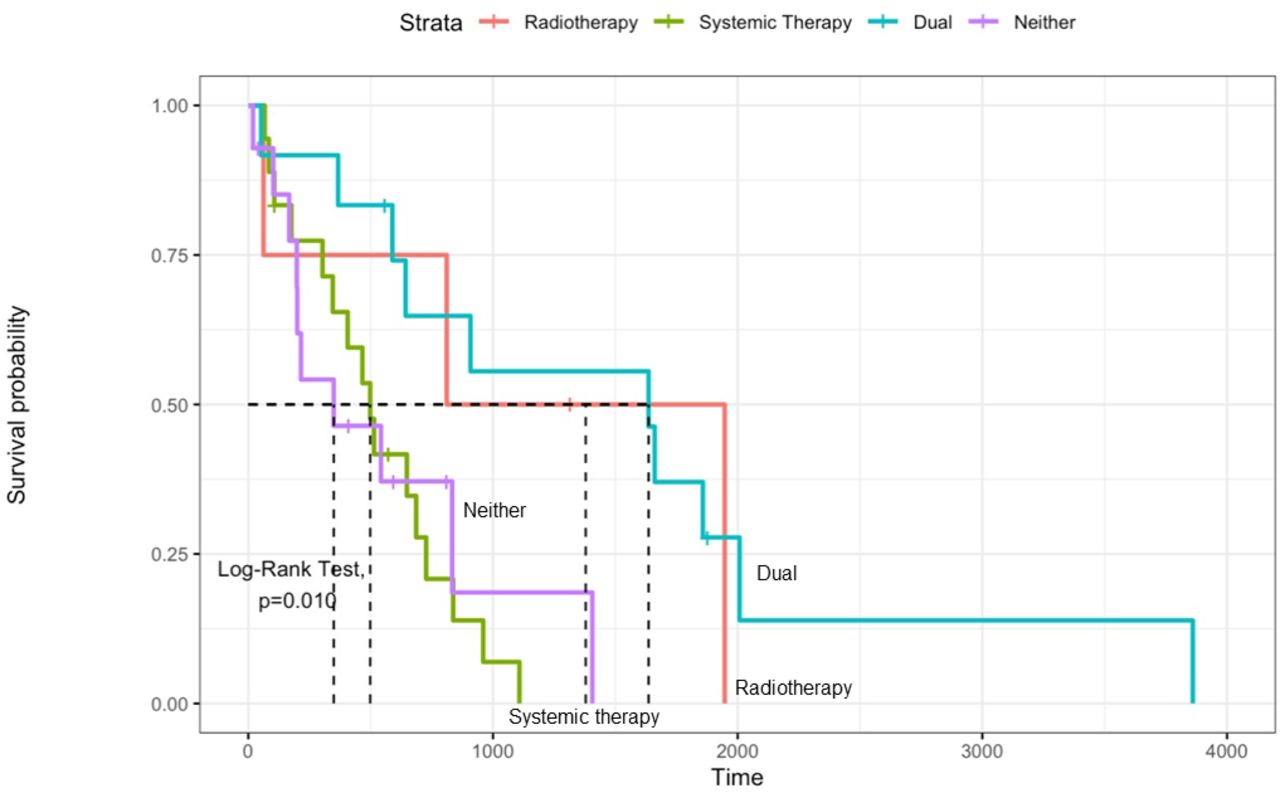
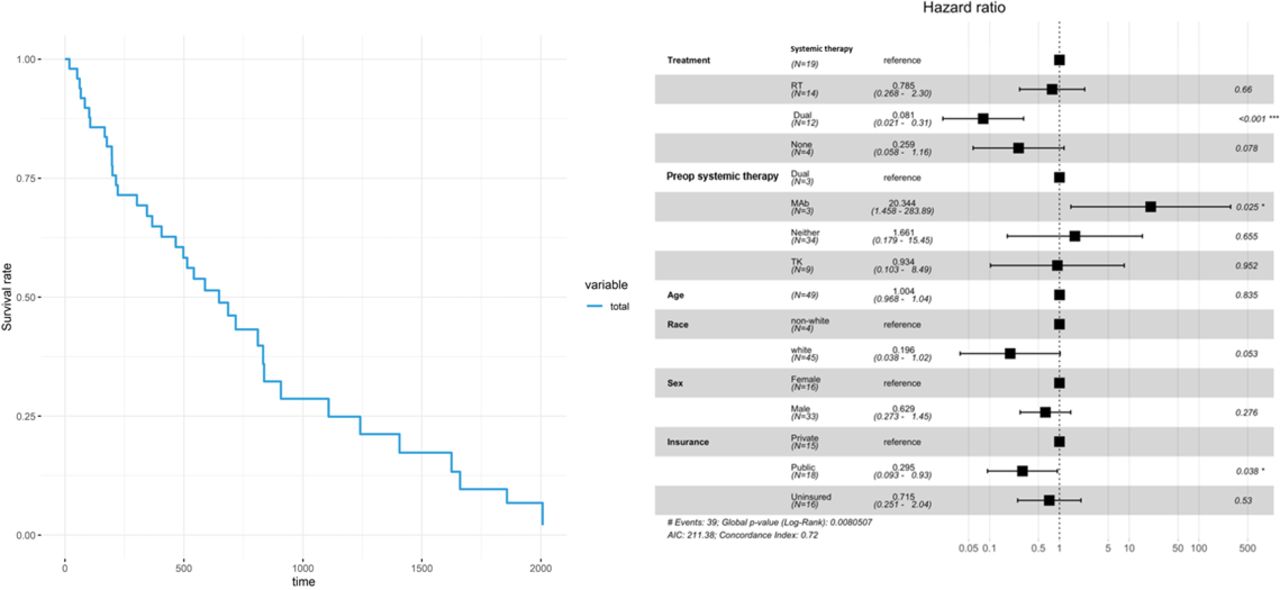
Higher 1-year OS was found in patients undergoing dual therapy (N = 10/12, 83.3%) compared with RT alone (2/4, 50.0%), targeted systemic therapy alone (10/19, 52.6%), and neither (3/14, 21.4%; P = 0.013). At the last follow-up, a total of 39 patients (81.2%) died with a mean time to death of 723.0 ± 752.3 days (Table 3). A longer OS time was found in patients recieving dual therapy compared with targeted systemic therapy alone, RT alone, and neither therapy on survival analysis (log-rank; P = 0.010; Figure 1). Univariate and multivariate Cox regression controlling for age, race, sex, insurance, and preoperative targeted systemic therapy were performed, comparing each therapy to neither therapy. Only dual therapy showed an increased OS on univariate Cox regression (HR = 0.24, 95% CI = 0.08–0.69, P = 0.008) and multivariate Cox regression (HR = 0.08, 95% CI = 0.02–0.31, P < 0.001) but not compared with RT alone or targeted systemic therapy alone (Figure 2).

Kaplan–Meier plot of overall survival.

Cox regression and forest plot of therapy type and overall survival controlling for age, race, sex, insurance, and preoperative targeted systemic therapy.
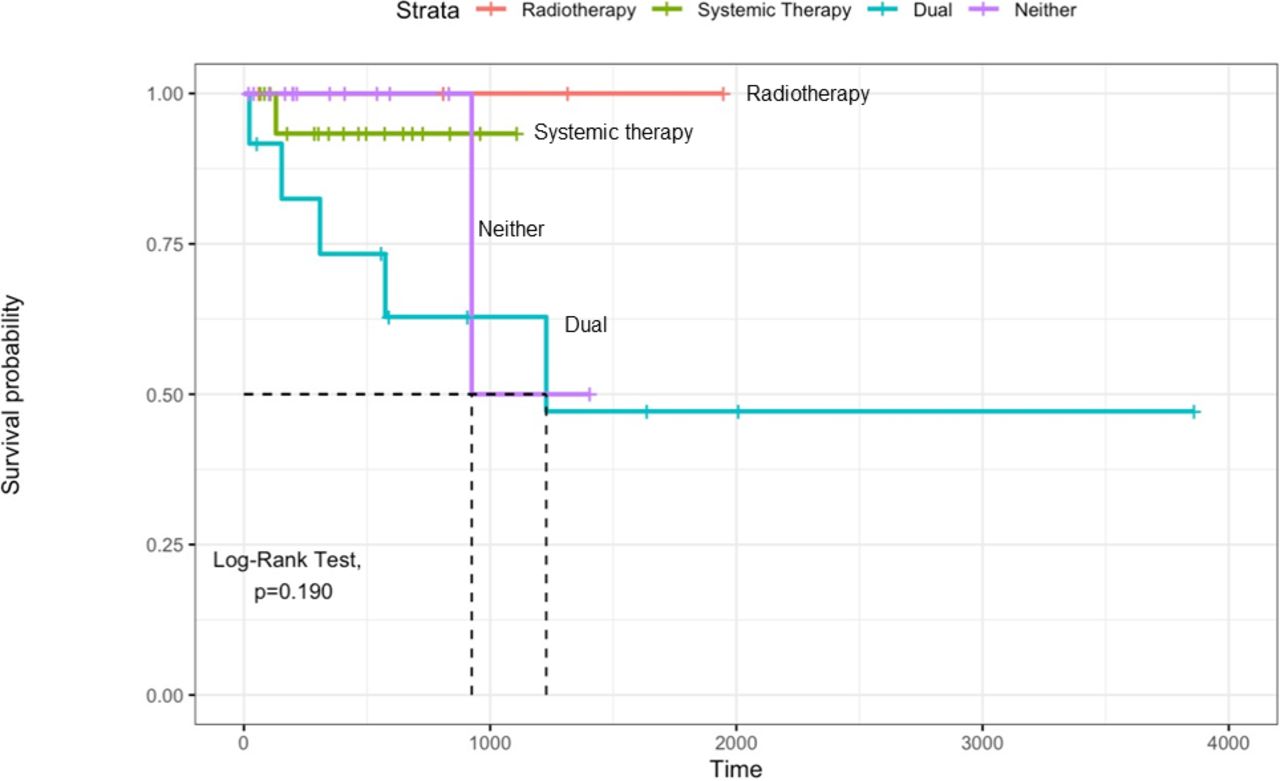
LR was found in 7 patients (14.3%) postoperatively, 5 of which occurred in patients who underwent dual therapy (P = 0.033). However, time to LR did not show any significant difference between the 4 groups on the Kaplan–Meier plot (log-rank; P = 0.190; Figure 3). Due to the low number of LR, multivariate Cox regression analysis was not performed.

Kaplan–Meier plot of local recurrence.
Functional Outcomes
Postoperative KPS (P = 0.252) and MMS (P = 0.346) were similar between all groups and remained nonsignificant at the last follow-up (Table 3). Similarly, KPS and MMS correction did not show a significant difference postoperatively and at the last follow-up.
Representative Case
A case presentation of a 45-year-old man with RCC is illustrated in Figure 4. The patient suffered from a worsening left upper extremity weakness and back pain. The patient had T4 and T7 lesions compressing the spinal cord on sagittal, contrasted T1-weighted magnetic resonance imaging (MRI; Figure 4A), axial T2-weighted MRI at T4 (Figure 4B), and axial T2-weighted MRI at T7 (Figure 4C). The patient then underwent posterior spinal fusion from T2-T9, with bilateral transpedicular decompression at T4 and T7 and tumor debulking, as evident in the lateral and posteroanterior x-rays (Figure 4D,E). Although T7 was causing Bilsky 1C compression, separation was requested by the radiation oncology team.

(A) 45-year-old man with renal cell carcinoma presented with worsening left upper extremity weakness and back pain. The patient had evident T4 and T7 lesions compressing the spinal cord on preoperative sagittal, contrasted T1-weighted magnetic resonance imaging (MRI) (A), axial T2-weighted MRI at T4 (B), and axial T2-weighted MRI at T7 (C). Subsequently, the patient underwent posterior spinal fusion from T2 to T9, multiple posterior column osteotomies, and laminectomy with bilateral transpedicular decompression at T4 and T7 with tumor debulking, as shown on lateral and posteroanterior x-rays (D and E).
Discussion
In patients undergoing metastatic spine surgery for RCC, we sought to investigate the role of targeted systemic therapy and long-term outcomes in patients receiving postoperative RT alone, targeted systemic therapy alone, dual therapy, and neither therapy. Among 49 patients included in the current study, no difference was found regarding readmissions, complications, or KPS and MMS. However, a higher 1-year OS was found in patients undergoing dual therapy compared with RT alone, targeted systemic therapy alone, and neither therapy. Moreover, dual therapy was independently associated with increased OS compared with other therapies or neither therapy, with no significant impact on LR. Despite a relatively small sample size, the current study provides further insights in the postoperative management of patients undergoing spine surgery for RCC metastases.
Although metastatic RCC can be an aggressive disease with poor expected survival, new targeted systemic therapy agents have been shown to improve survival.18 In the setting of spinal cord compression, surgery is often necessary as RCC lesions are radioresistant.19 Separation surgery allows high-dose SBRT to be delivered and also provides definitive stabilization for unstable lesions.17 Newer studies in patients with visceral metastases have shown promising results from newer agents. In 5872 patients with metastatic RCC, Chakiryan et al18 found that dual immunotherapy (ipilimumab plus nivolumab) or a combination of targeted therapy and immunotherapy (axitinib plus pembrolizumab) was significantly associated with improved survival. Other studies have reported similar findings.20–22 These novel agents have yet to be fully explored in a large cohort of patients undergoing metastatic spine surgery for RCC.23,24
Patients undergoing postoperative dual therapy involving both targeted systemic therapy and RT showed an improved OS compared with RT alone, targeted systemic therapy alone, and neither therapy. Recent studies have advocated for SBRT to treat metastatic RCC to the spine for symptomatic treatment and local control; however, outcomes are mixed.25–28 Park et al25 did not find a significant increase in OS with RT or targeted systemic therapy in 44 patients undergoing spine surgery for metastatic RCC. Similarly, in a retrospective study of 267 patients undergoing spine surgery for metastatic RCC, Tatsui et al29 found a significant increase in OS in patients receiving postoperative targeted systemic therapy but not RT. However, no clear distinction between patients receiving dual therapy or each therapy alone was detailed in either of the aforementioned studies.25,29 In parallel, Massaad et al30 performed a retrospective study of 88 patients undergoing spinal surgery for metastatic RCC with postoperative RT and showed that implementing postoperative targeted systemic therapy significantly improved OS. While our study was limited in sample size, the current results reinforce the added benefit of dual therapy on long-term survival.
In this study, TKIs were used in two-thirds of the patients, with only a few patients receiving immune checkpoint inhibitors. These findings are similar to other studies involving patients undergoing spinal surgery for metastatic RCC.25,31,32 However, in light of recent reports demonstrating the higher efficacy of monoclonal antibodies to the traditional tyrosine inhibitors in metastatic RCC,21,24,33–35 future studies should focus on the role of monoclonal antibodies in RCC metastases involving the spine.
While our study focused on the impact of treatment modality on patients’ outcomes and not risk factors for poor outcomes, we found that patients with dual therapy were more likely to have private insurance as compared with patients with neither therapy, who tended to be mostly uninsured. It is worthwhile to note that risk factors associated with decreased OS have been thoroughly documented in the literature in patients undergoing spine surgery for metastatic RCC and included a lower Tokuhashi score, lower KPS, neurological deficit at presentation, lower albumin levels (<3.5 g/L), nonambulatory status, major comorbidities, multiple spinal metastases, other bony metastases, and visceral metastases, among others.30,32,36–38 The insurance differences in our study reveal a potentially important area of future research, which includes social determinants of health outcomes in patients undergoing metastatic spine tumor surgery. Additional topics worthy of study include socioeconomic status, race, ethnicity, and education level.
While spine surgeons work alongside oncologists and radiation oncologists in the care of patients with spinal metastases, these results underscore the role of multidisciplinary management to maintain the highest quality of care and achieve optimal outcomes. SBRT and targeted systemic therapy regimens should be offered as part of the postoperative care to ensure local and systemic control of the disease once the wound has healed at approximately 2 to 3 weeks. Though the current study was not adequately powered to compare systemic therapies, future studies should investigate the impact of specific targeted systemic therapy agents combined with SBRT in patients with spinal metastatic RCC.
The present study contains several limitations that warrant discussion. First, while this study was limited by the relatively small sample size, these findings can be a valuable add-on to the current management of RCC metastatic to the spine. Second, the retrospective nature of our study possesses inherent limitations. As such, future prospective studies should be conducted to validate these results. Third, the single-center nature of this study limits the extrapolation of these findings to a larger population. Fourth, this study is prone to selection bias through the different indications and surgical techniques used. Another selection bias might have originated from the possibility that more aggressive treatment regimens (dual therapy) are likely chosen in patients with a worse prognosis, which might explain the high LR in the dual therapy group. Another reason for the high LR found in the dual therapy group could be the long survival in these patients. Regarding selection bias, factors such as the presence of solitary spine lesions, concurrent systemic disease, patient quality of life, and individualized approaches by different medical oncologists all contributed to the variability in treatment choices at our institution. It is important to acknowledge that our study reflects real-world clinical practice, where treatment decisions are based on a multitude of patient-specific factors and clinical judgment. Furthermore, postoperative RT is influenced by various considerations, including prior radiation, performance status, prognosis, loss to follow-up, insurance issues, and feasibility of radiation techniques such as SBRT. Randomized trials are needed to eliminate this bias. Fifth, given the small sample size, we were unable to control for all factors potentially influencing OS. Accounting for all possible confounders was difficult given the retrospective nature of our study. While we controlled for age, race, sex, insurance, and preoperative targeted systemic therapy, more confounders may be related to the type of surgery performed and disease severity. Sixth, while multiple regimens of targeted systemic therapy exist, we analyzed all targeted systemic therapy regimen as 1 group to increase the sample size. Seventh, the rationale behind the choice of the postoperative treatment regimen could not be depicted in a retrospective medical record review.
Finally, the strength of our study lies in including a control group not receiving any postoperative therapy to delineate the impact of different treatment modalities on long-term outcomes. Despite the retrospective nature of the study from a single institution focusing on a specific histological type (RCC) in spine surgery, we believe that our findings provide valuable insights into the treatment outcomes of RCC metastasis to the spine. While our study may not have the statistical power to draw definitive conclusions, it serves as an initial exploration of the efficacy of postoperative dual therapy in this patient population. Moreover, we think there is value in sharing our own experience, as it was surprising that so few people received dual therapy. Larger studies with a broader sample size are warranted to validate our findings and provide more robust evidence.
Conclusion
In a single-center cohort of patients undergoing spine surgery for metastatic RCC, dual therapy consisting of combined radiation and targeted systemic therapy demonstrated a significant survival benefit at 1 year and longer OS compared with all other postoperative treatment regiments. Taken together, multidisciplinary management of spinal metastatic RCC with targeted systemic therapy and RT is recommended to maximize long-term survival.
Footnotes
Disclosures Dr. Zuckerman reports being an unaffiliated neurotrauma consultant for the National Football League and consultant at Medtronic. Dr. Stephens is a consultant for Nuvasive and Carbofix and receives institutional research support from Nuvasive and Stryker Spine. Dr. Abtahi received an institutional research support from Stryker Spine. There are no other perceived conflicts of interest by any of the listed authors.
Ethics Statement Institutional review board (IRB) approval was obtained for this study (IRB#211900).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.