


Abstract
Background Lateral lumbar interbody fusion (LLIF) with posterior screw fusion is a safe and effective treatment for patients suffering from degenerative spine disorders. While LLIF has been shown to restore disc height, decompress neural components, correct sagittal imbalances, and improve pain scores, the approach requires repositioning patients for posterior pedicle fixation, which requires 2 separate surgeries. The evolution of surgical techniques, navigation, and robotics has allowed for a single position approach to LLIF with the patient in the prone position. The purpose of this study was to perform a systematic review and meta-analysis comparing the prone single position (PSP) LLIF approach to the dual position LLIF approach. We hypothesized that PSP LLIF will have a reduced operative time, complication rate, and blood loss compared with the dual position LLIF procedure.
Methods A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. PubMed and Embase databases were searched with key terms: (lateral AND [interbody OR “inter body”] AND lumbar AND fusion) AND (prone OR single). Results were extracted and reviewed by 2 authors (MR and RB) per selection criteria. Patient demographics were extracted from the selected studies, along with surgical, patient-reported, and radiographic outcomes. A meta-analysis was performed using an unstandardized mean difference or log odds ratio with a confidence level of 95%.
Results Fifteen studies were included in the systematic review and 5 studies compared PSP LLIF to dual position LLIF for meta-analysis. PSP LLIF had a reduced operative time and length of stay compared with the dual position approach, although there was no significant reduction in estimated blood loss. Additionally, PSP LLIF improved lumbar lordosis more effectively than dual position LLIF. There was no difference in segmental lordosis or pelvic tilt. There was no difference in intraoperative complications, postoperative complications, or reoperations.
Conclusions PSP LLIF reduces operative time and length of stay, with no relative increase in complications or reoperations compared with the dual position approach. Additionally, PSP LLIF improves lumbar lordosis relative to dual position LLIF, which may improve functional outcomes and reduce the risk of developing adjacent segment disease.
Clinical Relevance The associated operative and postoperative benefits of PSP LLIF may improve long-term outcomes of patients undergoing spinal fusion.
Level of Evidence 1
- Lumbar interbody fusion
- Prone single position fusion
- lateral fusion
- degenerative disc disease
- pedicle screw fixation
Highlights
Key findings: Prone single position (PSP) lateral lumbar interbody fusion (LLIF) reduces operative time and length of stay (LOS) and improves postoperative lumbar lordosis with no relative increase in complications or reoperations compared with the dual position approach.
What is known, and what is new? The PSP LLIF approach offers advantages over the prior dual position LLIF approach. This review confirms these trends with relatively shorter operative time and LOS. Additionally, PSP LLIF can increase postoperative lumbar lordosis due to prone patient positioning, which may improve patient outcomes.
What is the implication, and what should change now? PSP LLIF can be utilized by surgeons to reduce operative time, OR resources, and LOS in patients undergoing lumbar spine fusion.
Introduction
In recent decades, increasing evidence of the long-term benefits of operative fusion procedures to treat degenerative disc disease has catalyzed advancements in the field.1 When combined with a growing elderly population and increased prevalence of degenerative disc disease, it is no surprise that spinal fusion operations across the globe are increasing at a rapid rate.2–5 Surgeons currently can select from a multitude of different approaches to spinal fusion, each with their own advantages and disadvantages. Despite different risk profiles associated with each approach, the literature does not support improved outcomes in 1 approach over the other.4,6,7 Current techniques in spinal fusion surgery include posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, anterior lumbar interbody fusion, oblique lumbar interbody fusion, and lateral lumbar interbody fusion (LLIF).
The advent of minimally invasive surgery and robotic-assisted navigation has allowed the development of minimally invasive techniques that encourage quicker postoperative mobilization and high fusion rates when compared with the traditional anterior and posterior approaches.6,8–10 LLIF utilizes a lateral approach that avoids the vasculature and visceral organ risk associated with anterior access and can be employed through a minimally invasive approach.11 However, 2 major limitations exist in that surgeons must reposition patients from left lateral decubitus to prone for bilateral screw fixation, and any multilevel L5/S1 fixation must be completed by anterior lumbar interbody fusion or transforaminal lumbar interbody fusion, which likewise requires patient repositioning. Several approaches have been proposed to help counteract the limitations of LLIF, 1 of which is the single-position prone approach.
A single position LLIF approach in the lateral decubitus position was recently proposed in 2018, offering several advantages over prior LLIF techniques. The shorter operative time can be attributed to the single position approach, which does not necessitate repositioning during the procedure. This further reduces health care costs, risks associated with the procedure, and complications related to time under anesthesia.12–14 Additionally, operating room (OR) workflow can be optimized with decreased complications and risk of infection resulting from fewer operations, reduced OR traffic, and lack of patient repositioning.11,15
Single position LLIF has also been performed with patients in the prone position, which has the added benefit of low barrier to implementation as many surgeons are already familiar with prone positioning due to experience with posterior lumbar interbody fusion.16 In this approach, both LLIF and posterior screw pedicle fixation are performed with patients prone. There are multiple anatomic changes that occur when the patient is placed in the prone position. As the weight of the abdomen hangs freely from the table it increases natural lordosis, which places the iliopsoas and lumbar plexus in a more posterior position.12 The prone positioning may allow for improved correction of lordosis, optimized anatomy for anterior and posterior vertebral access, and improved ability of the surgeon to perform an osteotomy in cases of severe deformity.11–13,17 In a study that compared the lateral and prone positions, the prone approach was found to add more lateral extension to the psoas muscle and have less patency to the venous structures, while the arteries remained fully open in both positions. Overall, magnetic resolution imaging evaluation showed that the psoas and, therefore, the lumbar plexus and vasculature moved significantly anterior in both positions, though to a lesser extent in prone.18 The retroperitoneal organs also undergo a ventral shift while the patient is prone. Although one may think this eliminates injury risk, preoperative planning is still warranted to prevent injury as the ventral shift of the organs has been found to not be large enough to fully reduce the risk, and many patients still have organs located within the cage corridor while in prone.19 Despite the potential advantages of the prone position, patient outcomes associated with prone LLIF are yet to be fully elucidated in the literature.
The purpose of the present study was to perform a systematic review and meta-analysis of the safety profile and patient outcomes associated with the prone single-position approach to LLIF. We hypothesized that prone single position (PSP) LLIF will reduce operative time, thereby reducing complications and blood loss in patients undergoing spinal fusion.
Materials and Methods
Search Strategy
This systematic review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. PubMed and Embase databases were searched with the following key terms and use of Boolean operators “AND” and “OR”: (lateral AND [interbody OR “inter body”] AND lumbar AND fusion) AND (prone OR single). The search was performed on 24 June 2023. Duplicate studies were removed, and titles and abstracts were screened by 2 independent reviewers (M.R. and B.C.) per the inclusion and exclusion criteria. Following the initial review, full manuscripts were reviewed per selection criteria. Any conflicts following the review were resolved by the authors.
Selection Criteria
Randomized controlled trials comparing PSP LLIF to dual position LLIF approach were included, reporting on metrics such as operative time, intraoperative and postoperative complications, neurological deficit, blood loss, length of hospital stay, readmission rate, adjacent segment disease, subsidence, morbidity/mortality, outcome survey score (visual analog scale [VAS] and Oswestry low back disability questionnaire), rates of fusion, and radiological outcomes were included in the study. Additionally, any observational studies reporting on PSP LLIF were included in the review. Any studies that used alternative procedures or single position left lateral decubitus LLIF were excluded. Animal studies, literature reviews, case reports, letters to the editor, and surgical technique articles were also excluded.
Data Extraction
Each study was extracted and assessed for risk of publication bias using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tool.20 Each study was reviewed for available data by a single author. The following demographic data were collected from each study: number of patients, age, body mass index, sex, number of levels fused, and intervention. Surgical outcomes were also recorded, including operative time, estimated blood loss (EBL), length of stay (LOS), surgical complications, postoperative complications, revision surgery, subsidence, fluoroscopy time, and retractor time. Any patient-reported outcome scores were documented (Oswestry Disability Index [ODI], short form (SF), and VAS). The following radiographic data were collected: sagittal alignment, segmental lordosis (SL), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), and PI-LL mismatch.
Meta-Analysis
A meta-analysis was performed on randomized controlled trials comparing PSP LLIF to traditional LLIF with available mean, SD, or dichotomous variables. All statistical analyses w performed in IBM SPSS (version 29.0.1.0). Operative time, EBL, complications, and reoperations were analyzed in addition to radiographic measurements including LL and SL. For continuous variables (operative time, EBL, LL, and SL), data were assessed as unstandardized mean difference with a confidence level of 95%. For dichotomous variables (complications and reoperations), a Log odds ratio was estimated. χ 2, Q test, and I 2 statistical analyses were performed with P = 0.05 to assess heterogeneity between studies. I 2 values less than 25 were analyzed with a fixed effect model, and values greater than 25 were assessed with a random effect model. Publication bias was assessed with an Egger test with significance set at P < 0.05.
Results
Study Characteristics and Demographics
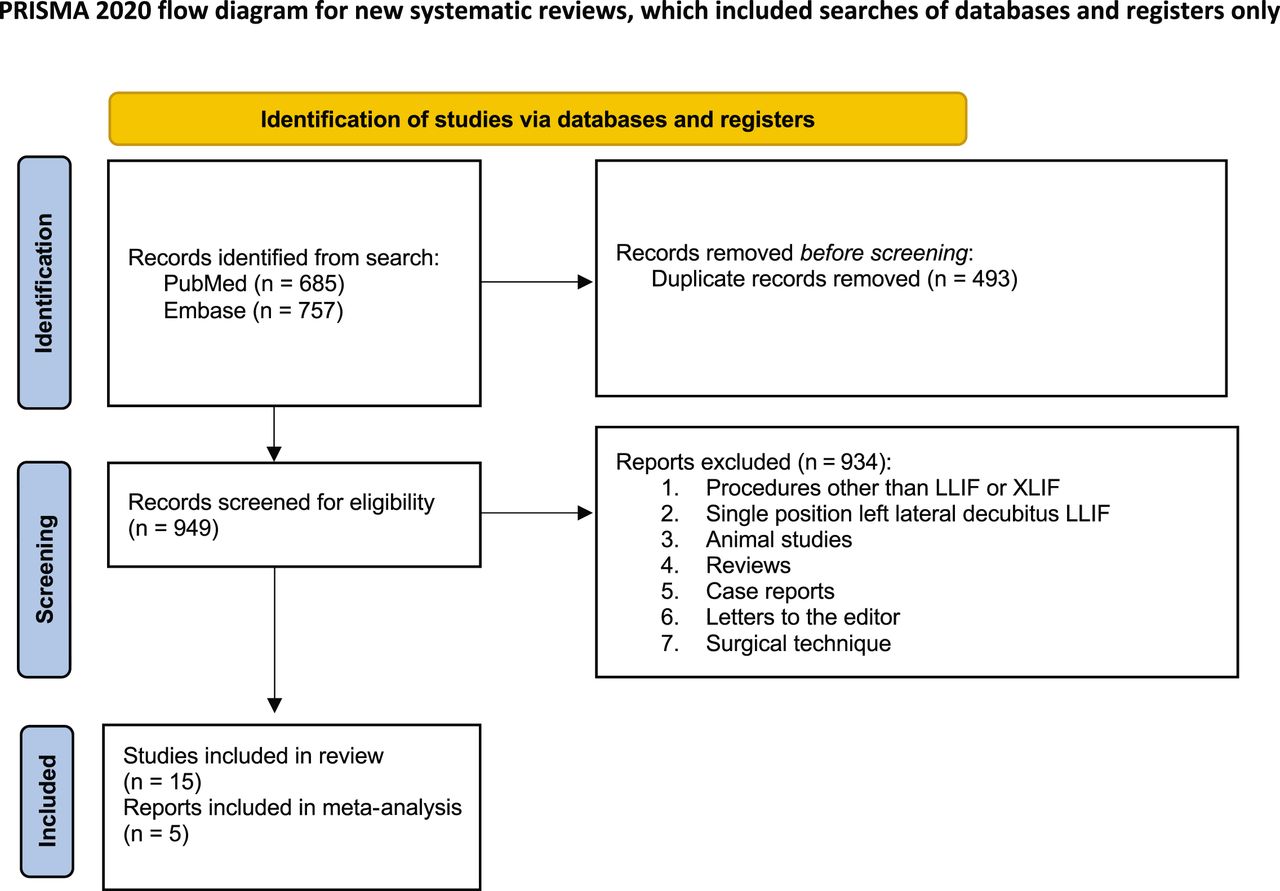
The initial search returned 685 studies from PubMed and 757 from Embase. Four hundred and ninety-three studies were merged as duplicates, leaving a total of 949 studies extracted. Nine hundred and thirty-four studies were deemed irrelevant by the reviewers, leaving a total of 15 studies for analysis (Figure 1). Four studies were retrospective cohort trials14,17,21,22 and 1 study was a randomized controlled trial23 comparing surgical, patient-reported, and radiographic outcomes between PSP LLIF and dual position LLIF. The remaining 10 studies were retrospective medical record reviews and case series with outcomes data associated with PSP LLIF.12,15,16,24–30 The lowest mean patient age was 53.8 years, and the highest was 67.9 years. All studies had a majority of female patients, and the mean body mass index ranged from 26.3 to 33 kg/m2. Three studies reported on only single-level fusions, and the remaining studies varied from an average of 1.07 to 2.3 levels. Study characteristics are summarized in Table 1, and patient demographics are summarized in Table 2.

Query results and study screening process per eligibility criteria conducted in accordance with the PRISMA guidelines. Abbreviations: LLIF, lateral lumbar interbody fusion; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; XLIF, extreme lumbar interbody fusion.
Characteristics and outcomes measures of eligible studies.
Demographic data for each study.
Bias
GRADE was used to assess publication bias in the systematic review. Ten of the studies had a GRADE of low, and 1 study had a GRADE of very low. Four of the studies had a GRADE of moderate. Egger’s test was performed on all meta-analyses, and the results were not significant (P > 0.05).
Operative Outcomes
Twelve studies reported mean operative times, EBL, and LOS ranging from 73.0 to 286.5 minutes, 19.0 to 694.5 mL, and 1.3 to 4.8 days, respectively.12,14–16,16,22–28 Three of these studies compared operative time and EBL of PSP LLIF to dual position LLIF. Buckland et al14 reported a significant reduction in operative time (103 vs 306 min, P < 0.001), while Lamartina and Berjano23 and Soliman et al28 reported a reduction in operative time, although results were not significant (133.8 vs 182.6 minutes, P = 0.08; 294.6 vs 352.7 minutes, P = 0.4). All 3 studies reported no significant difference in EBL between PSP and dual position LLIF (138.5 vs 166.6 mL, P = 0.353; 105 vs 92.9 mL, P = 0.79; 129.5 vs 88.5 mL, P = 0.3).14,22,23 Both Buckland et al and Soliman et al reported a reduction in LOS, although results were not significant (2.62 vs 3.18 days, P = 0.12; 2.7 vs 4.2 days, P = 0.10). Two studies12,15 reported retractor times ranging from 15 to 29.2 seconds, and 3 studies reported radiation dose between 89.8 and 171 mGy12,15,24 and fluoroscopy time between 112 and 267 seconds.12,15,22 In a comparative study of dual position LLIF, Soliman et al reported no significant difference in fluoroscopy time with PSP LLIF (112 vs 131.7 seconds, P = 0.5).22
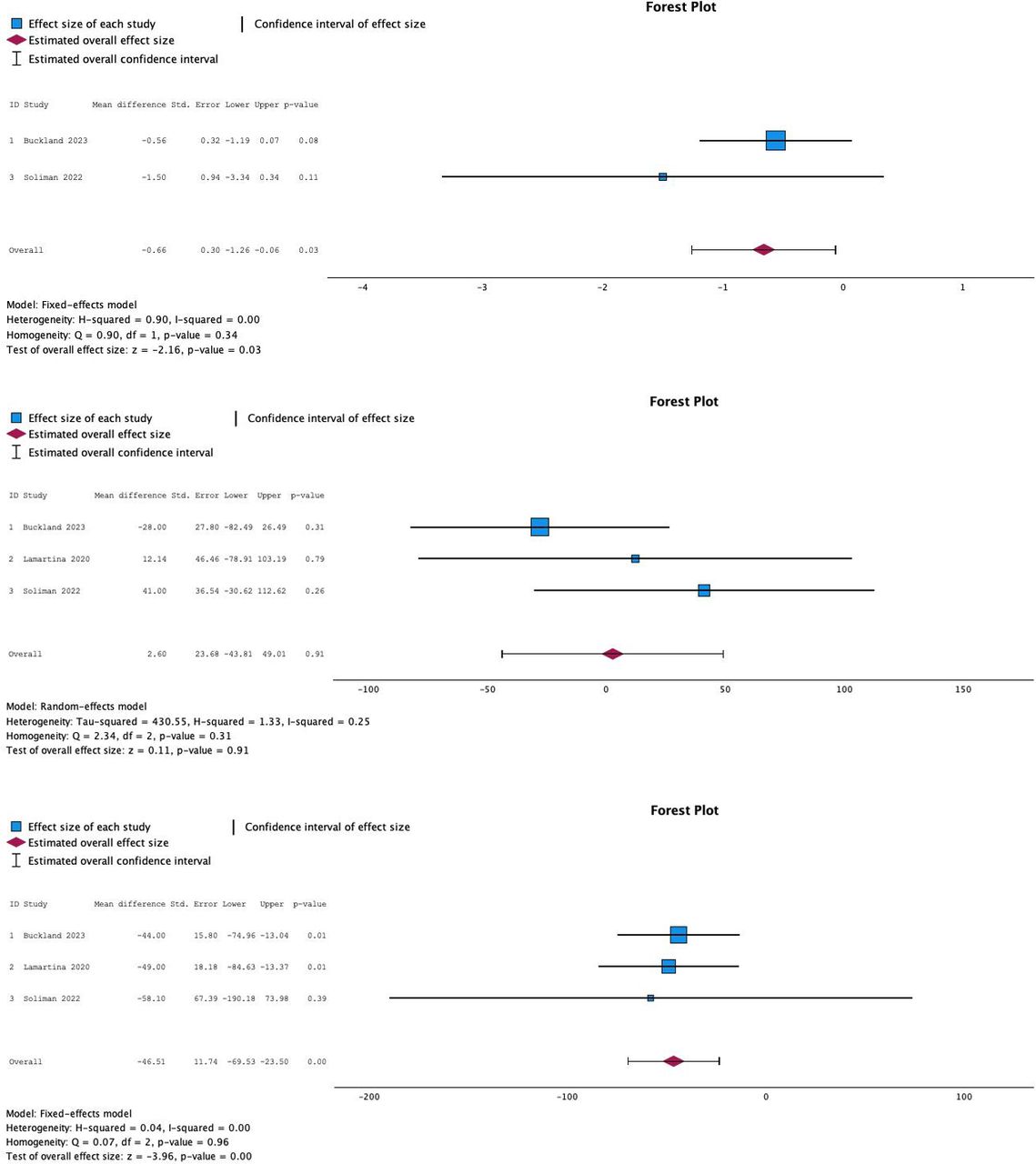
The meta-analysis pooled operative results from 3 comparative studies14,22,23 and found a statistically significant reduction in operative time with PSP LLIF vs dual position LLIF (P < 0.0001). EBL was shown to not be statistically different between groups (P = 0.91). Results from 2 studies14,22 showed a statistically significant reduction in LOS with PSP LLIF (P = 0.03). Figure 2 shows results from the meta-analysis for operative time, EBL, and LOS, respectively.

Forest plots of unstandardized mean differences between operative time (top; P < 0.001), estimated blood loss (middle; P = 0.91), and length of stay (bottom; P = 0.03).
Complications
Eleven studies12,14–16,22–28 reported complications associated with PSP LLIF. The most common intraoperative complications were 16 accounts of anterior longitudinal ligament ruptures across 747 patients. There were additionally 3 cases of subsidence, 4 cases of endplate fracture, 1 iliac vein injury, and 5 accounts of postoperative bleeding. Three studies reported a single occurrence of reoperation across 54 cases.12,22,28 Postoperative complications included 23 accounts of sensorimotor deficits, 5 cases with subsidence, 3 with pulmonary embolism, 1 with infection, 2 with urinary retention, and 1 with psoas hematoma (Figure 3)

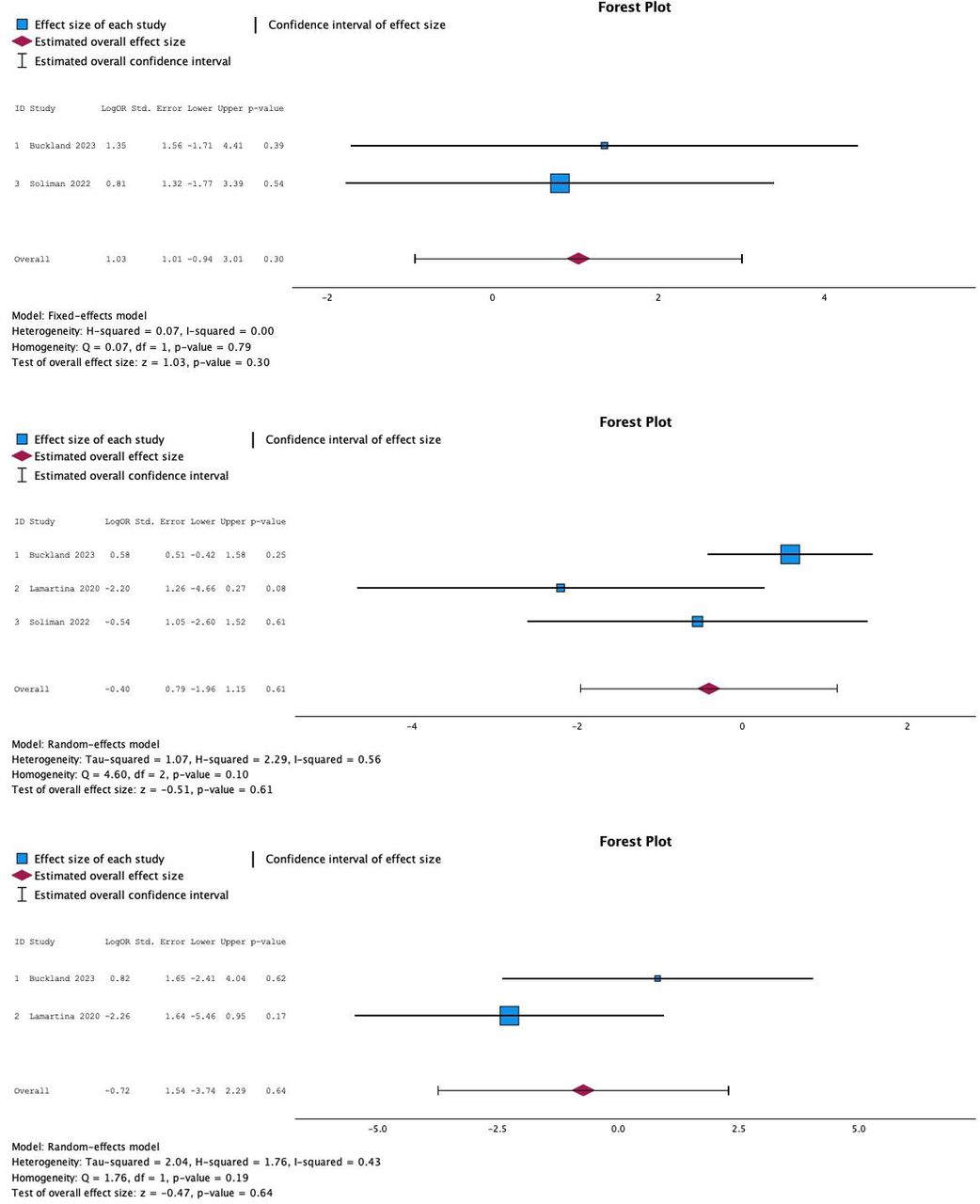
Forest plots of meta-analysis for intraoperative complications (top; P = 0.64), postoperative complications (middle; P = 0.61), and reoperations (bottom; P = 0.31).
Meta-analysis of the 3 comparative studies showed no statistical difference between intraoperative complications, postoperative complications, and reoperations (P = 0.64, P = 0.61, and P = 0.30). Results are shown in Figure 3.
Patient-Reported Outcomes
Seven studies included patient-reported outcomes for PSP LLIF with ODI scores ranging from an improvement in 3.3 to 43.9 with a significant improvement in 6 of the 7 studies.12,15,22–24,30,31 Soliman et al had the longest mean patient follow-up at 11.9 months and reported an improvement in ODI of 22.3 and an improvement in SF-12 of 10.3 (P = 0.002; P = 0.01). Four studies reported significant improvement in VAS back pain scores with a range of 3.7 to 4.5,12,15,24,30 with Diaz-Aguilar reporting the longest follow-up period at a mean of 7 months with an improvement of 4.5. Soliman et al compared patient-reported outcomes (PROs) between PSP LLIF and dual position approach and reported a statistically significant difference in improvement for SF-12 physical component scores (14.8 ± 12.1 vs 4.1 ± 7.6, P = 0.03) and additionally observed an increase in improvement of SF-12 mental component scores and ODI, although results were not significant (6.2 ± 9.3 vs 5.0 ± 10.5, P = 0.8; 12.3 ± 11 vs 4.3 ± 8.9, P = 0.1). Lamartina and Berjano similarly reported an increase in improvements in ODI (43.93 vs 38.3) and the reduction in the numerical rating of back pain (6.99 vs 2).
Radiographic Outcomes
Nine studies analyzed radiographic outcomes for PSP LLIF. Four studies reported SL improvements ranging between 5.1° and 10.1°,17,21,27,30 and 8 studies showed improvements in LL ranging from 1° to 11.5°. Change in pelvic tilt ranged from −0.6° to 3° between 5 studies, and 3 studies observed a PI change from 1.2° to 3°. SVA was analyzed in 4 studies showing changes ranging from 0° to 3.2°,15,17,22,27 and 1 study reported a significant increase in anterior disc height and posterior disc height of 7.4° and 3.3°, respectively.30 Five studies compared radiographic outcomes between PSP LLIF and dual position LLIF. Amaral et al and Walker et al showed a statistically significant increase in SL with the PSP LLIF approach (6.6° ± 6.5° vs 2.6° ± 4.5°, P = 0.03; 5.1° ± 3° vs 2.1° ± 3°, P = 0.03), while Buckland et al showed no significant difference (1.83° ± 3.72° vs 3° ± 5°, P = 0.233). Soliman et al reported a statistically significant improvement in LL (9.9° ± 8.5° vs 3.0° ± 5.0°, P = 0.047), while Buckland et al and Walker et al reported an improvement, although the results were not significant. Walker et al additionally reported no significant differences in SVA, PI, PT, anterior disc height, and posterior disc height. Soliman et al reported a statistically significant increase in PI-LL mismatch (15.6° ± 8.1° vs 3.7° ± 15.7°, P = 0.05), and PT, PI, and SS all did not vary between approaches.
Meta-analysis from the 3 comparative studies14,17,22 showed a significant improvement in LL (P = 0.05). SL was not different between groups (P = 0.28). Two studies17,22 reported PT with no difference between groups (P = 0.93). Results from the meta-analysis are shown in Figure 4.

Results of meta-analysis forest plot for lumbar lordosis (top; P = 0.05), segmental lordosis (middle; P = 0.28), and pelvic tilt (bottom; P = 0.93).
Discussion
The results from the current review and meta-analysis suggest that PSP LLIF reduces operative time and LOS, although there was no significant reduction in EBL. Additionally, PSP LLIF improves LL more effectively than dual position LLIF. The safety profile was comparable between PSP and dual position LLIF with no increase in intraoperative complications, postoperative complications, or reoperations. While a meta-analysis was unable to be conducted on PROs, the current evidence suggests that PSP LLIF improves PROs, and in 1 study, improvement in outcomes measures was increased relative to dual position LLIF.
With the recent technological advances in minimally invasive surgery and robotic-assisted navigation, procedures such as LLIF offer many advantages over traditional anterior or posterior approaches to lumbar interbody fusion.32 The main drawback to LLIF is the requirement to reposition patients; however, the recent development of single position techniques demonstrates promising results. The results from our study suggest that both operative time and LOS are reduced in PSP LLIF compared with dual position approaches; however, there was no associated difference in EBL or complication rates. While it is encouraging that there was no relative increase in complication rates, we hypothesized that EBL and complication rates would be reduced with a significant decrease in operative time and no need to reposition patients. The failure to support this hypothesis could be due to the small sample size of studies or other factors including surgeon familiarity with the single position approach. Soliman et al did compare PROs and reported an improvement relative to the dual position approach. Interestingly, results from our review suggested that PSP LLIF improves LL relative to the dual position approach. This improvement is most likely due to the anatomical benefit of placing patients in the prone position12 and may improve functional outcomes and reduce the incidence of segmental adjacent disc disease over the lateral single position approach. More long-term follow-up studies are required to confirm these trends.
The authors acknowledge that this study comes with limitations. Meta-analysis was performed on the current literature, which lacks a significant number of randomized control studies comparing PSP LLIF to dual position LLIF due to the recent development of this approach. This limited the number of comparisons we were able to make. Additionally, many of the studies were retrospective in nature and had a consequently low GRADE score, which may introduce bias. As more surgeons begin utilizing the PSP lateral approach, future studies can further assess comparisons between single and dual position surgeries.
Conclusions
PSP LLIF leads to reductions in operative time and LOS, with no difference in complications or reoperations compared with the dual position approach. Additionally, patients may experience the added benefit of improved postoperative LL and outcomes scores relative to dual position LLIF.
Footnotes
Funding No funding was received for this study.
Disclosures The authors have no disclosures or conflicts of interest to declare.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.