


Abstract
Background Computer-assisted spinal navigation allows for real time localization of surgical instruments in multiple views. Its use decreases radiation exposure and clears the surgical field of the C-arm fluoroscope. Despite these advantages, spinal navigation has yet to gain general acceptance among spine surgeons. The purpose of this study is to survey spine surgeons about their opinions on the strengths and weaknesses of spinal navigation.
Methods Spine surgeons from the membership of the Spine Arthroplasty Society (SAS) and the Society for Minimally Invasive Spine Surgery (SMISS) were surveyed regarding their current use of spinal navigation and their perceptions of the strengths and weaknesses of spinal navigation (N = 147). Responses were analyzed using 2-sided chi-square tests.
Results Most spine surgeons (63.4%) have only superficial experience with spinal navigation, and 76.2% of surgeons rarely use spinal navigation in their cases. Spine surgeons have the most experience with virtual fluoroscopy spinal navigation systems (35.9%). Surgeons considered longer operating times (63.5%), increased cost (48.3%), lack of necessity (40.7%), unreliable navigation accuracy (37.9%), and too many intraoperative glitches (35.2%) to be the major weaknesses of spinal navigation.
Surgeons considered decreased radiation exposure to the surgeon (76.1%), increased screw placement accuracy (65.7%), decreased radiation exposure to the patient (41.8%), and keeping the C-arm away from the operating field (29.1%) to be the greatest advantages of spinal navigation. Among the types of procedures surgeons believe are most likely to benefit from spinal navigation are minimally invasive instrumentation and fusion (72.5%) and complex open deformity (55.6%).
Conclusion Most spine surgeons have only superficial experience in spinal navigation. The most commonly selected weaknesses of spinal navigation are increased operative time, cost, and lack of necessity. Increased fluoroscopy and MIS use in the future may shift focus from weaknesses to the strengths of spinal navigation, including decreased radiation exposure and elimination of the C-arm from the operative field.
INTRODUCTION
Computer-assisted spinal navigation describes a closely related group of technologies that merge preoperative or intraoperative images with 3D localization of surgical instruments in real time. Originally modified from intracranial frameless stereotaxy, spinal navigation allows for multiplanar views of instruments in relation to anatomy. Its touted advantages include decreased radiation exposure to the patient and the surgical team,1 increased accuracy in most situations,1–4 elimination of the need for cumbersome protective gowns, and clearance of the surgical field from the C-arm fluoroscope.
Despite these advantages, spinal navigation has yet to gain general acceptance among spine surgeons. This lack of acceptance has been noted in the spinal navigation literature and has been attributed to a substantial learning curve, increased operative time, added complexity and added cost, as well as unique flaws within each navigation system.5–7 In a prior survey of surgeons regarding spinal navigation, Schroder and Wassman8 found that 53% of German neurosurgery departments have access to spinal navigation, but further lines of inquiry regarding the use of spinal navigation and additional perceptions of spinal navigation were not explored.
The purpose of this study is to survey spine surgeons about their use of spinal navigation, as well as their opinions on the strengths and weaknesses of spinal navigation to better understand the current status of computer-assisted navigation in the realm of spine surgery.
MATERIALS AND METHODS
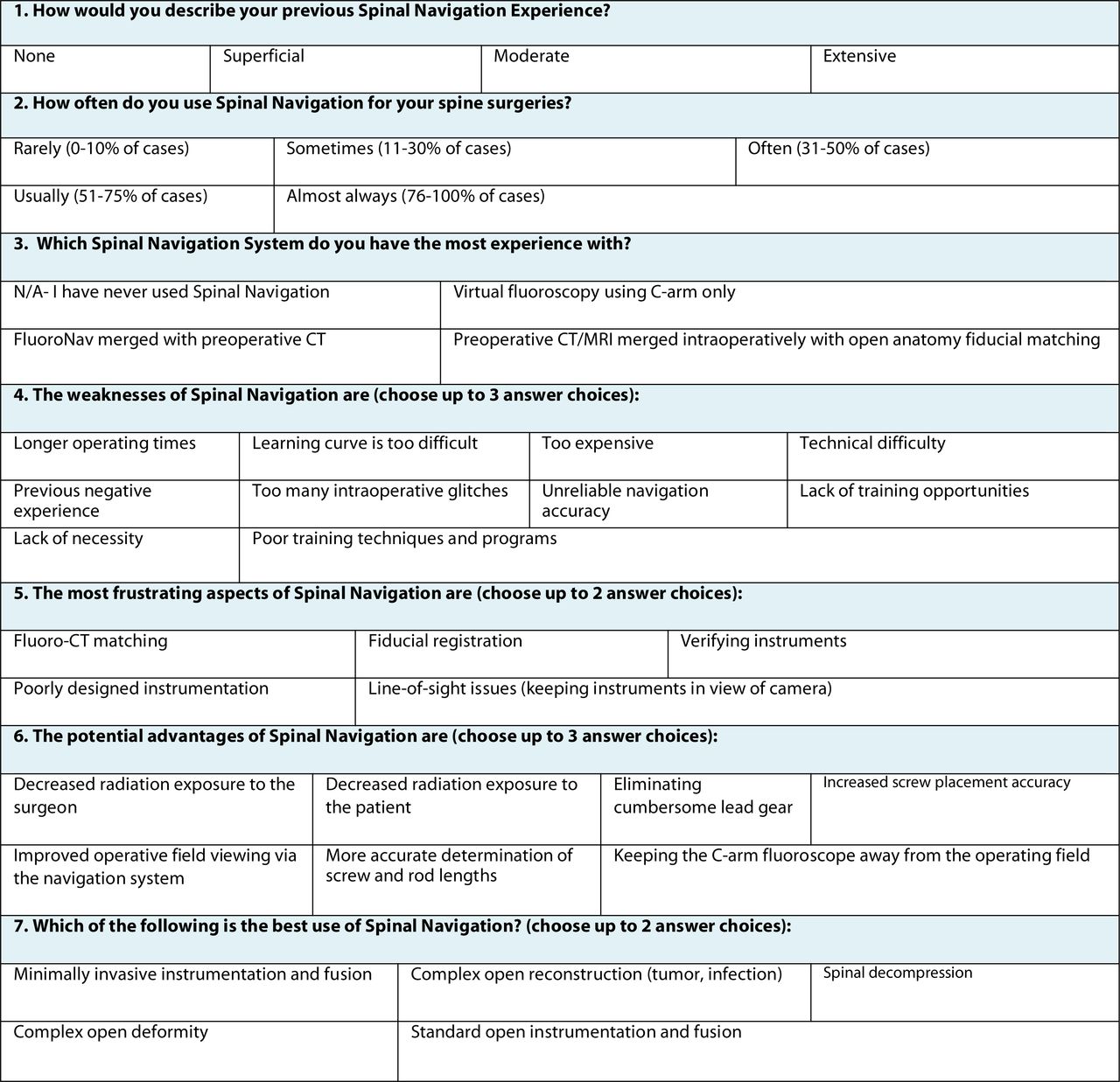
We constructed a survey regarding surgeons’ beliefs about the strengths and weaknesses of spinal navigation (Figure 1). Eight-hundred and two surveys were distributed to the email addresses of the membership of the Spine Arthroplasty Society (SAS) and the Society for Minimally Invasive Spine Surgery (SMISS) through a web-based survey administrator surveymonkey.com (Portland, Oregon). One-hundred and forty-seven (18.3%) responses were returned and analyzed (N = 147).

Survey of Spinal Navigation.
Statistical Methods
Survey data were analyzed where applicable using SPSS v.15.0 (SPSS, Chicago, Illinois) and a 2-sided chisquare test. A probability level of P < .05 was considered statistically significant when comparing groups.
RESULTS
To assess the current state of spinal navigation use among spine surgeons, respondents were asked to rate their experience with spinal navigation using a multiple choice format. Among the spine surgeons responding to the survey, 19.3% had no experience with spinal navigation, 44.1% had superficial experience, 24.1% had moderate experience, and only 12.4% had extensive experience with spinal navigation.
The respondents were then asked how often they use spinal navigation in their surgeries according to 4 ranges of frequency of use. Most (76.2%) spine surgeons indicated they use spinal navigation rarely (in less than 10% of their cases), 14.9% use spinal navigation sometimes (11—30% of cases), 3% use navigation often (31—50% of cases), and 2% almost always (76—100% of cases) use spinal navigation during their spine surgeries.
When surveyed on which spinal navigation system the respondents had the most experience with, 35.9% of spine surgeons had the most experience with virtual fluoroscopy using C-arm only, followed by 21.4% who selected FluoroNav (Medtronic, Inc., Minneapolis, Minnesota) merged with preoperative CT, and 15.2% who selected preoperative CT/MRI merged intraoperatively with open anatomy fiducial matching. The remaining respondents (27.6%) had not previously used spinal navigation.
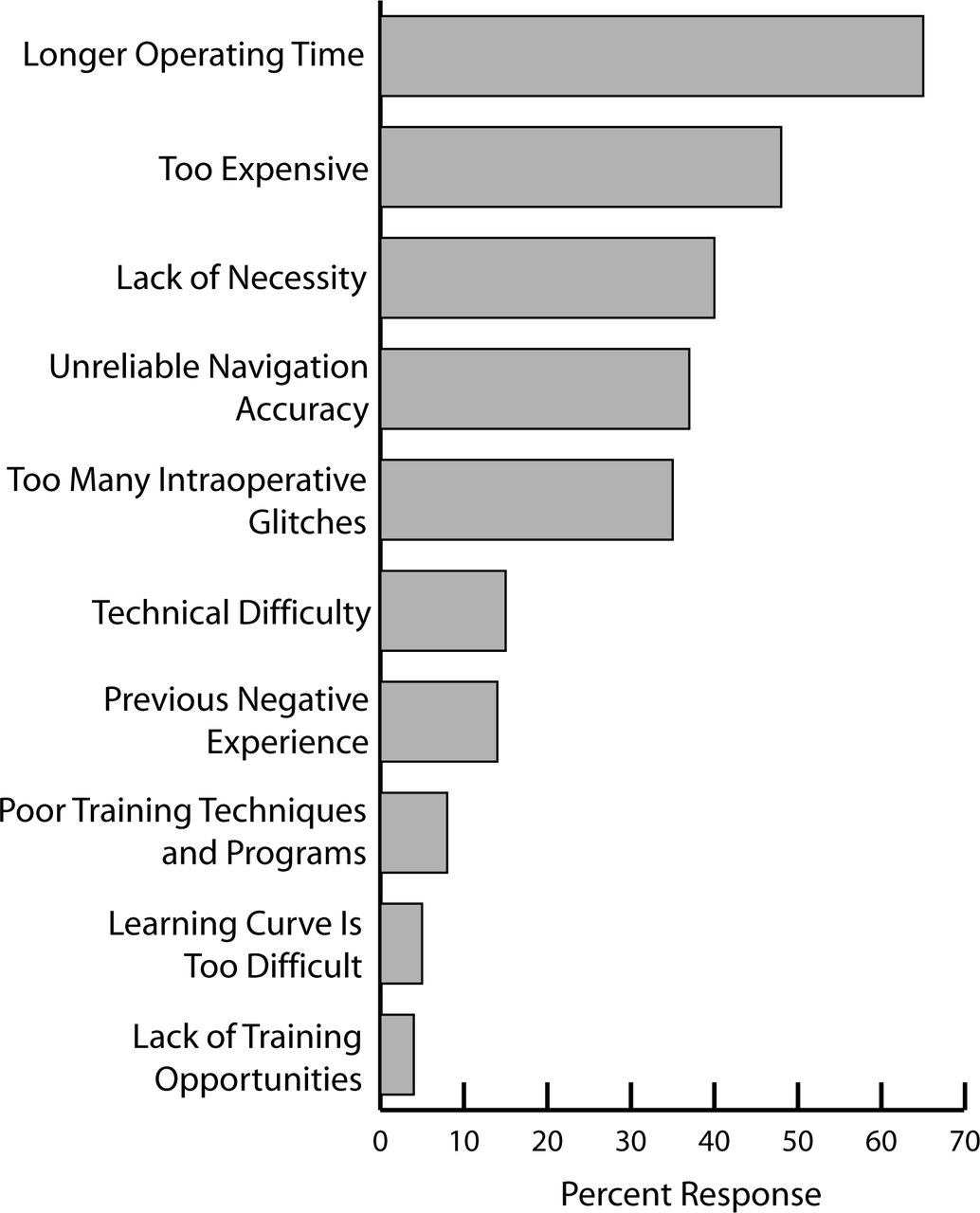
When asked to select major weaknesses of spinal navigation from a list of possible responses, surgeons considered longer operating times (63.5%), increased cost (48.3%), lack of necessity (40.7%), unreliable navigation accuracy (37.9%), and too many intraoperative glitches (35.2%) to be the major weaknesses (Figure 2). These perceptions of the weaknesses of spinal navigation varied among respondents with differing practice demographics and navigation experience. When responses were stratified by spinal navigation experience, surgeons with more experience were more critical about the intraoperative glitches of spinal navigation, as 55.6% of surgeons with extensive experience selected intraoperative glitches as a major weakness compared to 14.3% of surgeons with no spinal navigation experience (P = .031). Surgeons with greater spinal navigation experience were also more likely to select unreliable navigation accuracy as a weakness (44%) than surgeons without spinal navigation experience (28.5%), but the difference was not statistically significant. Surgeons who rarely use fluoroscopy considered lack of necessity more of a weakness (66.7%) than surgeons who almost always use fluoroscopy (27.7%) (P = .037).

The weaknesses of spinal navigation are (choose up to 3 answer choices).
Very few respondents felt that the lack of training opportunities (5.5%), a difficult learning curve (6.2%), or poor training techniques and programs (6.9%) were major weaknesses of spinal navigation (Figure 2).
Surgeons were then asked to select which aspects of spinal navigation (from a list of possible responses) they found most frustrating. Fiducial registration was the most widely selected response (50.4%), followed by line-of-sight issues (48.9%).
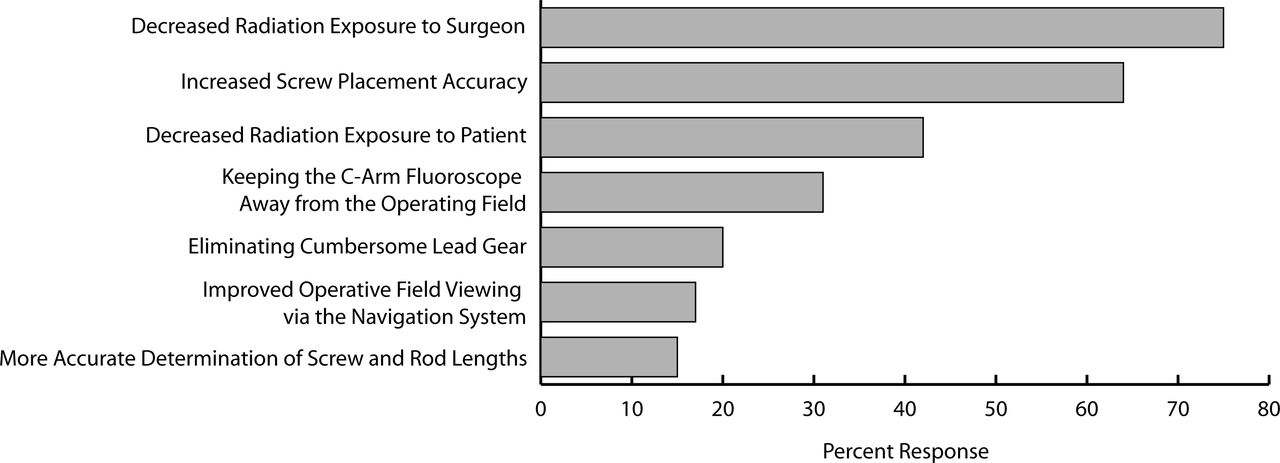
When surveyed on the advantages of spinal navigation, surgeons considered decreased radiation exposure to the surgeon (76.1%), increased screw placement accuracy (65.7%), decreased radiation exposure to the patient (41.8%), and keeping the C-arm away from the operating field (29.1%) to be the greatest advantages of spinal navigation (Figure 3).

The potential advantages of spinal navigation are (choose up to 3 answer choices).
Differences in perceptions of strengths of spinal navigation were found among surgeons based on levels of experience with spinal navigation. As surgeons’ experience with navigation increased, a greater proportion believed that decreased radiation exposure to the surgeon and keeping the C-arm away from the operating field were important advantages. Among surgeons with extensive navigation experience, 94.4% considered decreased radiation exposure to the surgeon an advantage, whereas only 57.1% of surgeons with no spinal navigation experience considered decreased radiation exposure an advantage (P = .018), but all groups considered decreased radiation exposure to be an important strength. More strikingly, 61.1% of surgeons with extensive spinal navigation selected the elimination of the C-arm fluoroscope from the operative field as an advantage as opposed to 3.6% of surgeons with no navigation experience (P < .001).
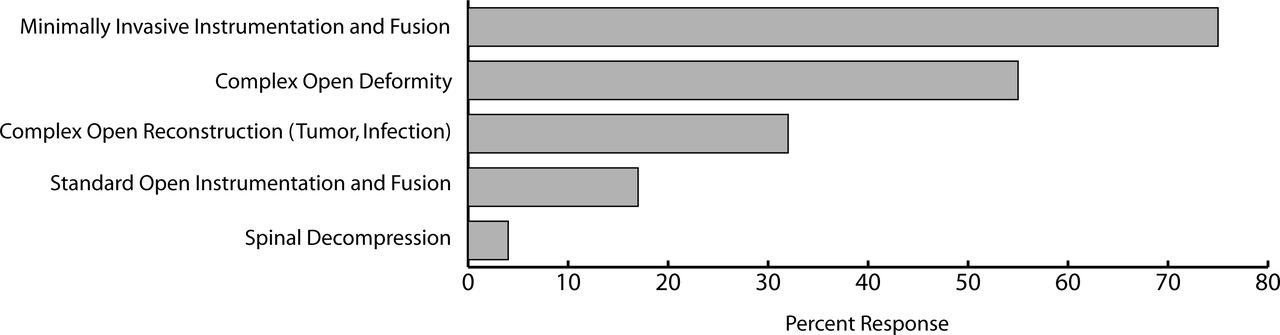
Among the types of procedures most likely to benefit from spinal navigation are minimally invasive instrumentation and fusion (72.5%), complex open deformity (55.6%), complex open reconstruction (tumor, infection) (30.3%), and standard open instrumentation and fusion (16.2%) (Figure 4).

Which of the following is the best use of spinal navigation? (choose up to 2 answer choices).
DISCUSSION
Confirming the common, but previously undocumented, perception that spinal navigation is not commonly used by spine surgeons, our survey found that most spine surgeons have only superficial experience in spinal navigation, and more than 75% of surgeons rarely used spinal navigation in their surgeries. The most frequently used system is virtual fluoroscopy using C-arm only. Thus, despite ongoing improvements in technology and recent increases in the use of fluoroscopy and MIS, spinal navigation remains infrequently used in everyday practice.
The most commonly cited reasons that spinal navigation is poorly utilized were increased operative time, cost, lack of necessity, unreliable accuracy, and intraoperative glitches. Interestingly, the most frequently selected weakness, longer operative times, may be a misconception, based on recent studies. Sasso and Garrido9 showed that spinal navigation using FluoroNav technology, at worst, did not affect operative time and, at best, decreased total case time by an average of 40 minutes. In the setting of preoperative CT merged with open anatomy fiducial registration, Papadopoulos et al.10 demonstrated that single multi-level registration at the beginning of the procedure could save time with no sacrifice of accuracy in contrast to repetitive single-level registration, thus minimizing increases in operative time. Therefore, future studies should focus on bridging the gap between the evidence of existing studies and surgeons’ perceptions of longer operative time with spinal navigation.
The perceptions regarding spinal navigation accuracy are complex. In our survey, we found that unreliable accuracy was the fourth most commonly selected weakness and increased accuracy was the second most frequently selected advantage of spinal navigation, indicating that surgeons are conflicted as to whether they trust the accuracy of navigation. This ambiguity is somewhat reflected in the literature, although most studies demonstrate improved accuracy of spinal navigation as compared to conventional techniques.1–4 However, at least one study demonstrated spinal navigation inaccuracy in the setting of thoracic pedicle screw insertion using FluoroNav with a single reference point.11 Accuracy remains a significant concern as our survey showed that more surgeons with greater spinal navigation experience selected unreliable accuracy as a weakness, suggesting that concerns with accuracy are not alleviated with increased navigation experience.
Although issues related to training, technical difficulty, and learning curve are commonly presumed to be major barriers to the acceptance of spinal navigation, we found surgeons did not select them as major weaknesses in the survey. While such issues are likely to exist, especially among surgeons with less spinal navigation experience, it appears that surgeons consider other disadvantages to be more pressing. These findings differ from the results of an earlier survey12 assessing surgeons’ perceptions of minimally invasive surgery. In the previous survey regarding minimally invasive spine surgery, surgeons selected the difficult learning curve and issues related to training and technical difficulty as major obstacles to the adoption of minimally invasive surgery. These types of issues are easily addressed with improved training protocols and programs. However, our survey results indicate that barriers to adoption of spinal navigation are not due to a difficult learning curve nor to a lack of training opportunities. The barriers to adoption of navigation are more intrinsic to the technology itself, including intraoperative glitches, unreliable accuracy, frustrations with fiducial registration, and line-of-sight issues. These findings suggest that significant improvements in the technology will be required to improve the adoption rate of spinal navigation.
Regarding the advantages of spinal navigation, surgeons indicated they were likely to use spinal navigation because it decreases radiation exposure, increases accuracy, and eliminates the C-arm from the operating field. Selection by 76.1% of the response “decreased radiation exposure” highlights a major occupational hazard of spine surgery that can be mitigated in part by the use of spinal navigation technology. This advantage becomes more evident with increased use as surgeons with extensive navigation experience almost unanimously considered decreased radiation exposure a strength of navigation technology.
In addition, 29.1% of surveyed surgeons with more navigation experience felt that keeping the C-arm out of the operative field was a major advantage. Elimination of the C-arm from the operative field can prevent the surgeon from assuming uncomfortable positions to reach the operative target, as well as allow a second surgeon to assist from the opposite side. It is interesting to note that very few of the surgeons with no navigation experience believed that keeping the C-arm out of the field was a major strength, suggesting that without having experienced the operative room free of the C-arm, the surgeon without spinal navigation experience may not appreciate the advantages of the improved ergonomics. Among the spine surgeries selected as best uses of spinal navigation, there was the common thread of procedures that typically require instrumentation and/or large amounts of fluoroscopy. We anticipate an increased use of minimally invasive techniques in the near future, which in turn will increase dependence on intraoperative fluoroscopy and instrumentation.
CONCLUSION
Increased fluoroscopy use will lead to greater emphasis on issues related to increased radiation exposure and ergonomic comfort of the surgeon. The application of spinal navigation may address these issues, especially the key occupational safety issue related to prolonged, chronic radiation exposure due to intraoperative fluoroscopy. Some perceptions of the weaknesses of navigation may be misconceptions, especially those related to increased operative time. However, significant obstacles remain, including expense and continuing concerns about accuracy and intraoperative glitches. Addressing these issues should be a major goal in the continuing effort to encourage the use of spinal navigation in everyday clinical practice.
- Received May 30, 2008.
- Accepted July 9, 2008.
- Copyright SAS - Spine Arthroplasty Society 2008
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dr. Regev and the Department of Orthopaedic Surgery at the University of California, San Diego received an educational grant from Medtronic Spine and Biologics (Memphis, Tennessee).
Dr. Kim is a consultant for Medtronic Navigation (Louisville, Colorado)
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.