


Abstract
Background The presacral retroperitoneal approach to an axial lumbar interbody fusion (ALIF) is a percutaneous, minimally invasive technique for interbody fusion at L5-S1 that has not been extensively studied, particularly with respect to long-term outcomes.
Objective The authors describe clinical and radiographic outcomes at 1-year follow-up for 50 consecutive patients who underwent the presacral ALIF.
Methods Our patients included 24 males and 26 females who underwent the presacral ALIF procedure for interbody fusion at L5-S1. Indications included mechanical back pain and radiculopathy. Thirty-seven patients had disc degeneration at L5-S1, 7 had previously undergone a discectomy, and 6 had spondylolisthesis. A 2-level L4-S1 fusion was performed with a transforaminal lumbar interbody fusion at L4-5 in 15 patients. AxiaLIF was performed as a stand-alone procedure in 5 patients and supplemented with pedicle screws in 45 patients. Pre- and postoperative visual analog scale (VAS) and Oswestry Disability Index (ODI) scores were evaluated and complications were tracked. Fusion was evaluated by an independent neuro-radiologist.
Results At 1-year follow-up, VAS and ODI scores had significantly improved by 49% and 50%, respectively, versus preoperative scores. By high-resolution computer tomography (CT) scans, fusion was achieved in 44 (88%) patients, developing bone occurred in 5 (10%), and 1 (2%) patient had pseudoarthrosis. One patient suffered a major operative complication–a bowel perforation with a pre-sacral abscess that resolved with treatment.
Conclusion Our initial 50 patients who underwent presacral ALIF showed clinical improvement and fusion rates comparable with other interbody fusion techniques; its safety was reflected by low complication rates. Its efficacy in future patients will continue to be monitored, and will be reported in a 2-year follow-up study of fusion.
Lumbar interbody fusion is indicated for a variety of clinical conditions, including degenerative disc disease, spinal trauma, infection, and spinal deformity. Interbody fusion accomplishes the goal of achieving stability of the spine, and maintenance of coronal and sagittal balance by placing the graft near the central axis of rotation.1, 2 The four major access corridors for lumbar interbody fusion include the posterior lumbar interbody fusion (PLIF), transforami-nal lumbar interbody fusion (TLIF), anterior lumbar interbody fusion (ALIF), and extreme lateral trans-psoas lumbar interbody fusion (XLIF).
The PLIF technique described by Cloward et al3, 4 permits dorsal access to the spine for both decompression and fusion. Its potential drawbacks include exposure and retraction of the dural sac and exiting nerve roots bilaterally that can lead to nerve root injury and spinal fluid leakage.5, 6 The PLIF can be performed as an open or minimally invasive technique.5, 7–9 The TLIF was described by Harms in the 1980s as an open procedure6, 10–12 and later became more popular as a minimally invasive procedure with the introduction of percutaneous pedicle screw systems.13–17 In comparison with PLIF, the TLIF provides unilateral exposure with less retraction of the dural sac and nerve roots.
The ALIF, especially the retroperitoneal mini-open version, is one of the most often performed interbody fusion procedures.18–21 It offers a wide exposure of the disc yet allows complete avoidance of the dural sac and neural elements. Disadvantages of the ALIF include higher rates of exposure complications, potential need for a vascular surgeon, and pain caused by muscular disruption of the abdominal wall.2, 13, 15, 22–26 Although the laparoscopic transperitoneal ALIF enjoyed brief popularity,27–29 high complication rates and technical difficulties led to its decline.25, 27, 30 The XLIF, a recently introduced mini-open approach, uses a lateral corridor that requires partial mobilization of the psoas muscle.31, 32 The roots of the lumbar plexus, especially at L4-5, are at risk in this approach and the L5-S1 interspace is inaccessible with the XLIF.
The presacral retroperitoneal approach to axial lumbar interbody fusion ALIF is a minimally invasive technique that uses a new access corridor for interbody fusion at L5-S1.33, 34 In this procedure, the L5-S1 interspace and disc is accessed percutaneously by development of the fatty plane of the presacral space. Yet, little has been reported about the clinical effectiveness of this approach, especially in long-term follow-up. In this retrospective review, we report our clinical and radiographic results at 1-year follow-up in a cohort of 50 patients who underwent axial ALIF using AxiaLIF (TranS1, Wilmington, NC) for L5-S1 inter-body fusion.
Materials and methods
A retrospective medical chart and radiographic review was performed for 55 patients who underwent the presacral ALIF procedure between June 2005 and May 2006 at The Christ Hospital, Cincinnati, OH with approval by the Institutional Review Board. Five patients with incomplete data at 1-year follow-up were excluded from the study. Mean patient age was 45 years (range, 16-78), including 24 males (average, 46; range, 26-78 years) and 26 females (average, 44; range, 16-68 years). Patients included 15 smokers, 29 nonsmokers, and 6 patients with an unknown smoking history. Among the 50 patients, 37 suffered from degenerative disc disease, 6 had spondylolisthesis, and 7 had undergone previous discectomy. Conservative therapy had failed in all patients. Patients were operated on by 2 surgeons: first (40) and second (10).
Data obtained from the medical charts included patient age, sex, and history of smoking, and dates of service. Office charts and operative reports were reviewed for indications for surgery, operative time, estimated blood loss, levels of fusion and instrumentation, type of instrumentation, type of bone graft used, additional procedures performed, and any intra- and postoperative complications. We defined major complications as any condition that required unscheduled return to the operating room or prolonged hospital stay and considered all other complications minor.
On plain x-rays, we defined fusion as <1.5-mm translation and <3° of motion on flexion-extension films at L5-S1 level. All x-rays were digitalized and measured by using eFILM version 2.01 software (Merge Healthcare, Milwaukee, WI). We devised a classification of fusion status using thin-section, high-resolution, multi-planar CT scans (Table 1). Fusion status was assessed by an independent neuroradiologist using x-ray and CT scans performed 1 year postoperatively.
Fusion criteria on 3-mm high-resolution CT scan reconstructions in coronal and sagittal planes (with permission from Mayfield Clinic)
Clinical outcomes were derived from the VAS and ODI questionnaires that patients completed during their office visits at the preoperative evaluation and at 3-, 6-, and 12-month follow-up visits. The t test was used for continuous data and χ2 test was used for noncontinuous data (P < .05 statistical significance).
Presacral ALIF: operative technique
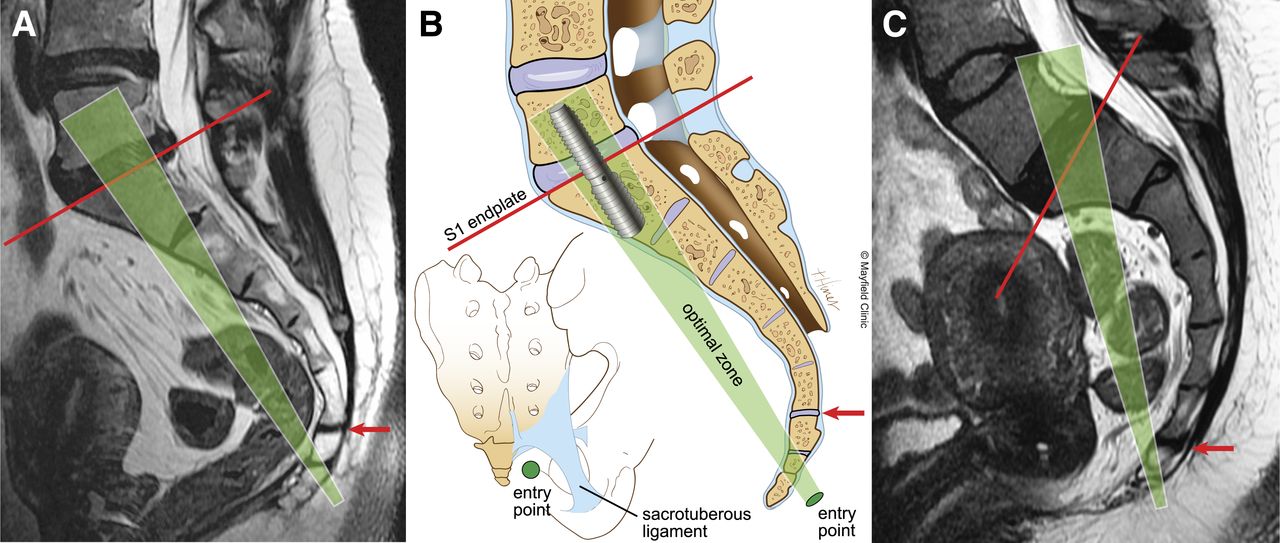
Preoperative evaluation: In addition to routine preoperative studies to determine the indications for L5-S1 fusion, midsag-ittal T1- and T2-weighted MRI images of the sacrum and coccyx were performed to rule out a vascular anomaly or tumor.25, 26, 35 Evaluation of the sagittal curve of the sacrum is necessary to confirm the feasibility of the approach (Fig. 1). The presacral ALIF is contraindicated in certain situations. First, in the occasional patient with an exaggerated sacral curve or C-shaped sacrum, the trajectory of the intended interbody screw may project posteriorly into the spinal canal behind the L5 vertebral body. Second, deformed anatomy from healed fractures may also interfere with proper trajectory generation. Third, patients with a transitional syndrome may not be candidates.36 Lastly, patients with a history of significant inflammatory bowel disease or prior surgical disruption of the pre-sacral space are not candidates. Surgical scarring renders the rectum immobile and at risk for laceration during the approach. Careful preoperative evaluation of the trajectory and vascular anatomy is mandatory.
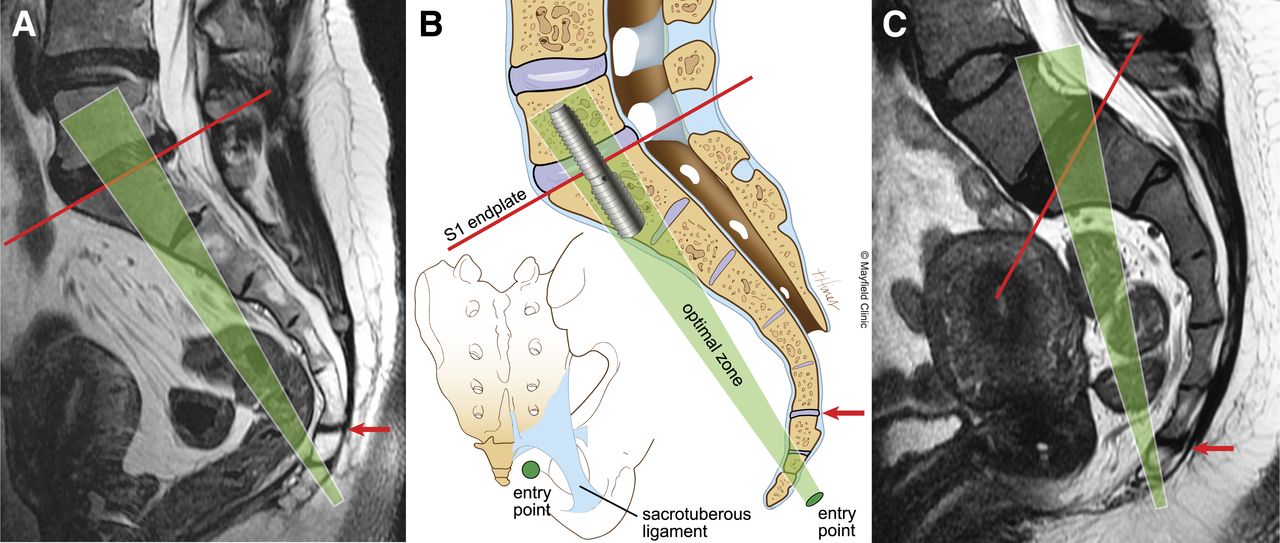
Preoperative evaluation of the sacrum and coccyx for the presacral ALIF procedure. To assess the feasibility of the approach, a line is drawn on the midsagittal MR scan from the probe entry point below the sacrococcygeal joint (red arrow) to the midpoint of the S1 endplate (red line). The optimal trajectory zone (green shaded area) for placement of the implant should be perpendicular to and centered at the midpoint of the superior endplate of S1. MR scan (A) and illustration (B) shows an ideal trajectory for insertion of the screw into the L5-S1 vertebrae. Illustration of the posterior view of the sacrum shows the probe entry point lateral to the coccyx and inferior to the attachments of the sacrospinous and sacrotuberous ligaments. MR scan (C) shows an excessive curvature of the sacrum and coccyx that would result in screw placement at an acute angle to the superior endplate of S1, which is biomechanically suboptimal, and in violation of the spinal canal. This procedure is contraindicated in these patients (with permission from Mayfield Clinic).
Surgical technique
The night before surgery, the patient completes a bowel preparation. At surgery, the patient is positioned prone with maintenance of lordosis and the legs spread. Insertion of a Foley catheter into the rectum will allow air to be injected during the procedure for visualization of the rectum. After the surgeon makes a small incision (15-18 mm) lateral to the tip of the coccyx, a blunt probe is passed through the pre-sacral space using guidance by bi-planar fluoroscopy. The guide probe is gently passed along the anterior cortex of the sacrum and in the midline at all times to an entry point usually close to the S1-2 junction. This is determined by mapping an anticipated trajectory into the L5 vertebral body from an anticipated sacral entry point.
Once the trajectory is chosen, a sharp beveled pin is then driven into the L5-S1 interspace. Using a series of dilators, the surgeon creates a 10 mm opening into the sacrum through which a 10 mm channel is drilled into the L5-S1 disc. The autograft is harvested from this channel for later implantation into the disc space. A series of upward- and downward-directed looped nitinol cutting blades are inserted sequentially into the disc space. After these cutters are rotated around the axis of insertion to morselize the disc material, they are directed against the endplates to denude the cartilage and sharply abrade the bony endplates in preparation for fusion. The disc material is evacuated with a series of wire brushes. Irrigation of the disc space with antibiotic solution helps to evacuate additional debris. Injection of Isovue-370 (Bracco Diagnostics, Inc., Princeton, NJ) into the disc space produces a discogram that documents the volume of evacuated nucleus pulposus. The disc space is then packed with grafting materials of the surgeon's choice. In this study, we used rhBMP2 (InFuse, Medtronic, Memphis, TN) in 46 patients and Actifuse (Apateck, London, England) or Vitoss (Orthovita, Malvern, PA) synthetic calcium phosphate in addition to rhBMP2 in 44 patients. A small amount (3-5 cc) of harvested autograft from the sacrum was used in all patients.
After drilling a channel into L5, the surgeon selects the optimal length of the interbody screw (TranS1, Wilmington, NC). The amount of distraction across the disc space desired determines the thread count at each of the 2 ends of the screw. A larger exchange cannula is placed over the 10 mm working channel for insertion of the screw. As the screw is inserted, the differential thread count creates a reverse Herbert screw effect that leads to disc space distraction, restoration of disc height, and opening of the L5-S1 neurofora-mena. The cannula is removed and the wound is then closed tightly with subcutaneous sutures. If desired, air or contrast injection into the Foley catheter before its removal confirms the integrity of the rectum.
Results
Of the 50 patients who underwent the presacral ALIF procedure, 45 had supplemental percutaneous pedicle screw instrumentation posteriorly at L5-S1 and 5 were standalone. Fifteen patients underwent fusion at L4-5 using the TLIF approach that was combined with the presacral ALIF at L5-S1 and percutaneous pedicle screw instrumentation from L4-S1. Five patients underwent a presacral ALIF at L5-S1 alone without any supplemental posterior fixation (an off-label use of the interbody screw). In all patients, Pathfinder percutaneous pedicle screws (Abbott Spine, Austin, TX) were used for posterior fixation (FDA clearance requires use of posterior fixation with pedicle or facet screws to supplement the screw). There was no significant difference in the fusion rates among smokers and nonsmokers (χ2 test, P > .05). Hospital stay ranged from 0 to 38 days (mean, 2.5 days).
Operative data and complications
Operating time averaged 194 (range, 45-330) minutes and blood loss averaged 218 ml (Table 2). Three patients underwent bilateral decompressive laminectomy and facetectomy and 3 patients underwent unilateral foraminotomy to directly decompress neural elements (total 6 posterior decompressions). Two patients later returned for surgery to undergo decompression of persistent symptomatic nerve roots.
Mean intraoperative blood loss and operative times as noted from anesthetist's chart were significantly lower in stand-alone procedures when compared with procedures supplemented by either pedicle screw fixation or TLIF procedure at another level. Although few patients underwent the procedure alone, morbidity associated with this procedure was substantially lower
One (2%) patient, a 26-year-old man, developed a major complication related to the presacral ALIF—a posterior rectal perforation and pre-sacral abscess. A high-grade fever developed on the third postoperative day followed by drainage of purulent material through the wound. Contrast injection in the bowl disclosed the perforation in the posterior wall of the rectum, which was then treated with open drainage, a diversionary colostomy, and intravenous antibiotics. The patient completely recovered and the colostomy was later reversed. In evaluating this complication, we discovered that the patient had not disclosed a history of multiple peri-rectal abscesses. He was very thin and had virtually no pre-sacral fat; air contrast was not injected into the rectum during surgery. When the guide probe was advanced along the sacrum, more than the usual amount of resistance was encountered that likely represented the point of injury to an immobile rectal wall.
One (2%) patient returned to surgery for revision of a pseudoarthrosis. No device failures, device removals, neurological or vascular complications occurred in this series.
Of 2 minor postoperative complications, 1 patient had wound drainage at pedicle screw insertion site 1 week after surgery that resolved with antibiotics, and 1 patient had prolonged ileus that resolved by conservative treatment.
Clinical outcomes
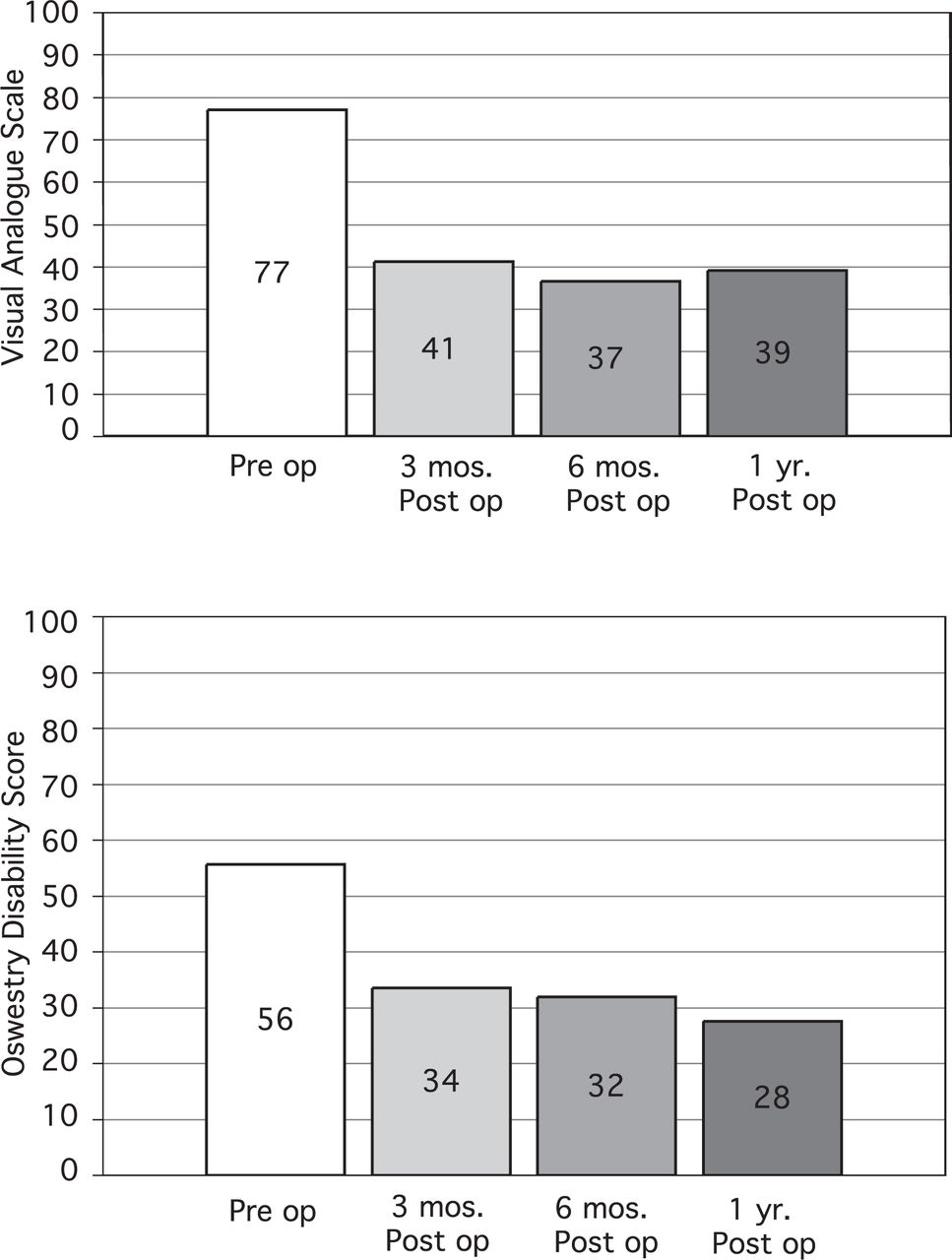
Clinical outcomes were measured by VAS and ODI scores (Fig. 2). The VAS and ODI data were unavailable for 2 patients from the beginning and for 6 patients at 1-year follow-up. VAS score averaged 77 mm preoperatively and significantly decreased to 39 mm at 1-year follow-up (49% improvement, paired t test, P < .0001). ODI score averaged 56 preoperatively and significantly decreased to 28 at 1-year follow-up (50% improvement, paired t test, P < .0001). The U.S. Food and Drug Administration considers a 20 mm decline on the VAS scale and a 15% reduction on the ODI scale as a clinically significant improvement.37, 38 In3patients, VAS and ODI scores had deteriorated at 1-year follow-up

Bar graphs of the pre- and postoperative Visual Analog Scale (A) and Oswestry Disability Index (B) scores. At 1-year follow up, VAS improved 49% and ODI improved 50% (statistically significant P < .0001) (with permission from Mayfield Clinic).
Radiographic outcomes
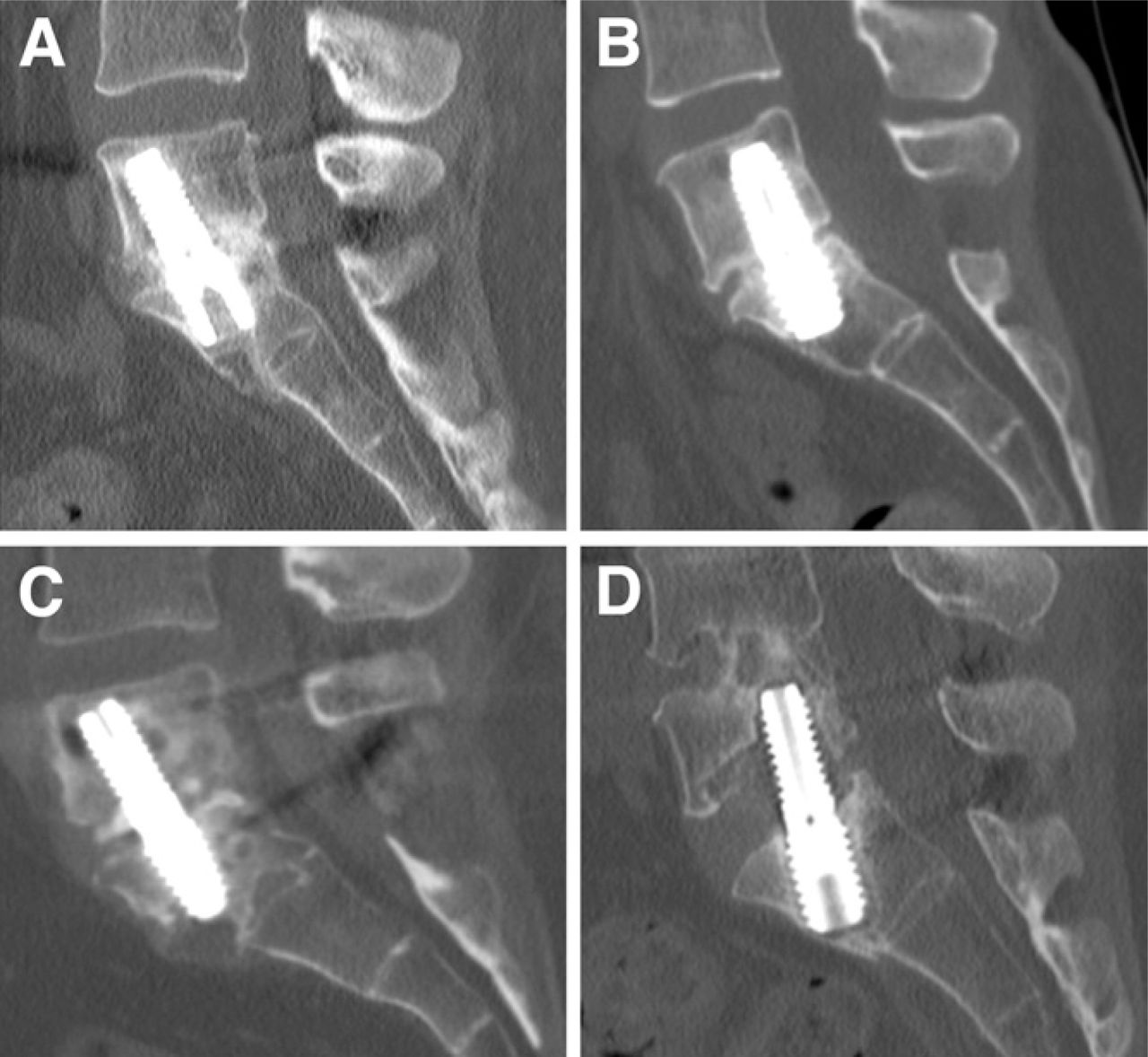
At 1-year follow-up, all 50 patients underwent lateral flexion extension lumbar spine films and CT scans. All 50 patients had fusion at L5-S1, as judged by plain radio-graphic criteria. On CT scan, fusion grade, according to our classification (Table 1), averaged 1.65, with 44 (88%) patients demonstrating fusion. Of the 50 patients, 25 (50%) had Grade I, advanced fusion (Fig. 3,A), 19 (38%) patients had Grade II fusion (Fig. 3,B), 5 (10%) patients had Grade III fusion categorized by developing bone (Fig. 3, C), and 1 (2%) patient had frank pseudoarthrosis (fusion Grade V) that required revision surgery (Figure 3,D). In this latter patient, CT scan demonstrated a halo around the interbody screw and both S1 pedicle screws. At the time of procedure at L5-S1, he had also undergone a TLIF at L4-5 and had demonstrated fusion in the L4-5 interspace. After undergoing surgical revision posteriorly, he was provided a bone stimulator. The interbody screw was not revised. At 1-year follow-up in the 5 patients with Grade III category of developing bone, 4 were asymptomatic (average, VAS 3.3 and ODI 32) and 1 was symptomatic (VAS 8 and ODI 64).
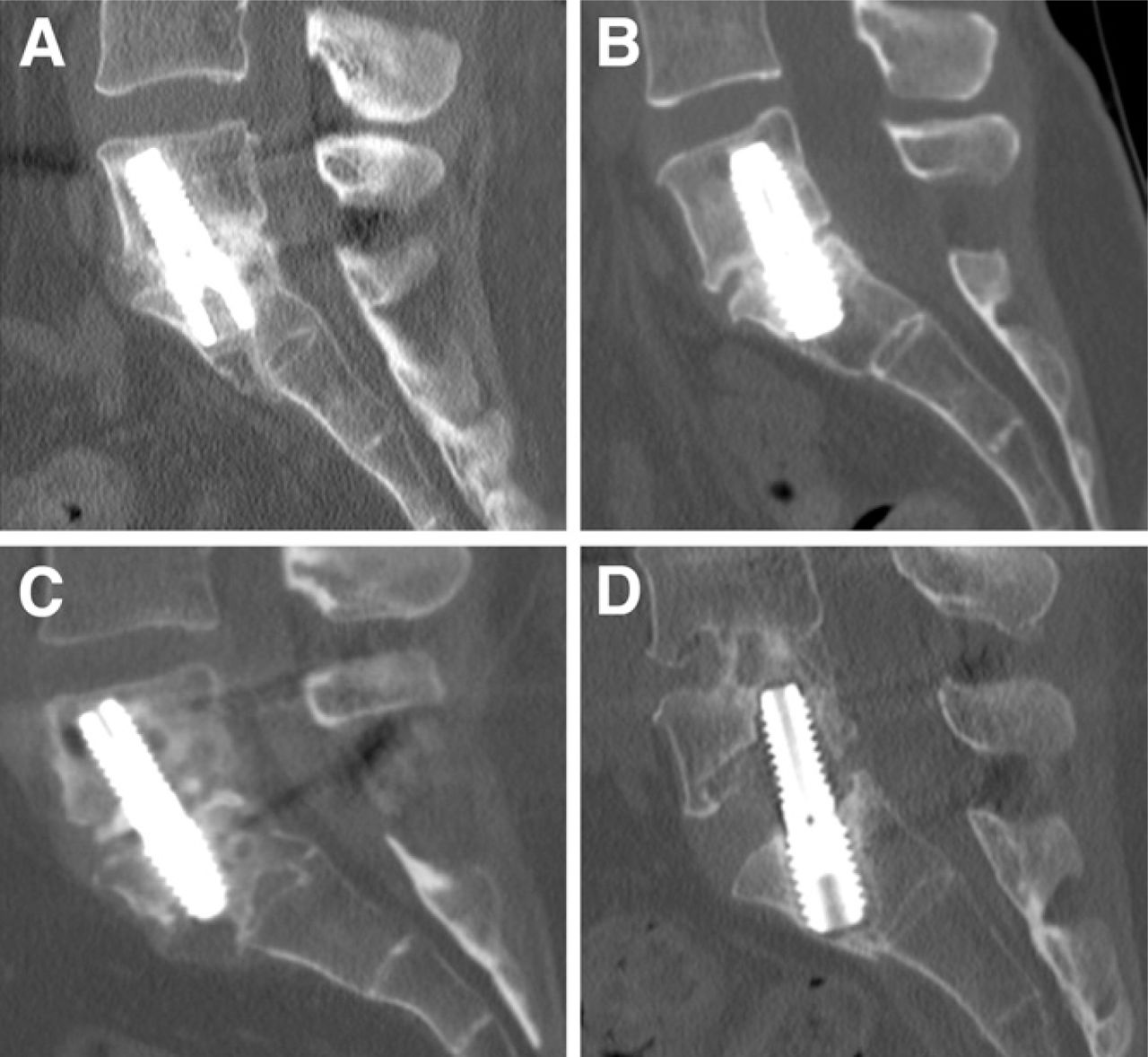
Postoperative fusion grades for the procedure depicted on 1-year postoperative CT scans. (A) Grade I shows continuous bridging bone extending from the L5 to the S1 endplate and occupying >50% of available space for fusion. (B) Grade II has bridging bone extending from the L5 to the S1 endplate and occupying < 50% of available space for fusion. (C) Grade III has developing bone with presence of bone connected to either L5 or S1 endplate without bridging. (D) Grade V is a pseudoarthrosis (with permission from Mayfield Clinic).
Discussion
The presacral retroperitoneal ALIF was introduced in the U.S. after FDA clearance was obtained in late 2004 for L5-S1 interbody fusion.33, 34 Using the avascular presacral space for axial entry into the spine, the surgeon operates through a 10 mm channel and relies entirely on fluoroscopic imaging, never directly viewing the operative field. The approach, methods of discectomy, placement of grafting material, and interbody screw are novel techniques. In our initial review of 50 patients who underwent fusion at L5-S1, the presacral ALIF provided a new access corridor to the spine that we call the axial corridor.
Anatomic and cadaver studies have demonstrated that the presacral space is devoid of muscles, neural elements, and any significant vasculature. These findings then confirmed the approach could be performed safely, so that removal of the nucleus and endplate preparation would be adequate. A thorough discectomy could be accomplished with complete preservation of the annulus.33, 39 Biomechani-cal studies of the TranS1 construct demonstrated superior fixation across the L5-S1 disc space compared with other interbody constructs.40
Our 50-patient cohort represents the largest series with 1-year follow-up after the presacral ALIF. Validation of this new minimally invasive operation for fusion of L5-S1 must include improvement in clinical outcomes, safety of approach, and the equivalency of fusion outcomes compared with other commonly used techniques. Clinically, our patients demonstrated a significant 50% improvement in VAS and ODI scores at follow-up versus preoperative scores and a 2% rate of approach-related complications. More important, by interpretation of fusion based on CT finding, 88% of the patients demonstrated fusion at 1 year, 10% demonstrated developing bone, and 1 (2%) patient had pseudoar-throsis.
Clinical outcomes
The variable thread count design of the screw examined in this study provides the option of distraction of the disc space when it is inserted. Restoration of disc height can relieve nerve root irritation or compression by indirect decompression and stabilization provided by this screw. However, careful evaluation of the patient is needed to determine if the disc space can be distracted, and if the distraction will be adequate to relieve neural compression. When nerve root compression occurs as a result of a large or free disc herniation, severe, compressive facet arthropathy, or central stenosis, direct surgical decompression of the root posteriorly may be needed. In the present study, 6 patients not only underwent a presacral ALIF but a direct decompressive surgery with a minimally invasive cylindrical tube (Access retractor; Abbott Spine, Austin, TX), because the root compression seemed to be so significant that distraction alone would be insufficient for relief. Two patients also later returned to undergo additional decompression. One patient underwent L5 root decompression for persistent root pain that resolved after the second stage decompression and stabilization with pedicle screws unilaterally; she originally underwent a stand-alone presacral ALIF procedure. During consultation in planning the operation, the option of adding a posterior decompression at the time of the presacral ALIF was presented; however, it seemed her mild radiculopathy would resolve after the presacral ALIF procedure. After opting to undergo the stand-alone approach, her radiculopaty did not resolve. The second patient developed recurrent root pain that had initially resolved after the procedure with posterior pedicle screw fixation for a Grade I spondylolysis. In the remaining 42 procedures, all patients with any degree of root symptoms resolved satisfactorily with the stabilization and distraction after undergoing the presacral ALIF. The 5 patients who underwent a stand-alone presacral ALIF (an off-label use without posterior fixation) had degenerative disc disease without significant instability or root entrapment. Estimated blood loss and mean operative time (with its associated exposure to anesthesia) were significantly less in these 5 patients when compared with those who underwent this fusion plus an additional posterior procedure (Table 2). However, complication rates, fusion rates, and VAS and ODI scores did not differ between the 2 groups. Although this 5 patient group is small, these first results hint that the presacral ALIF itself is associated with significantly lower morbidity and may alone be effective in select patients
Among the 50 patients, VAS and ODI scores at 1-year follow-up were improved in 47 patients versus preoperative scores. Of 3 patients with no improvement, 1 had a pseudo-arthrosis, 1 had a definite fusion defined by CT criteria, and 1 had developing bone by CT but continued heavy smoking, which raised our concern that it would become pseudoar-throsis. Statistically, significant improvement in VAS (50%) and ODI (49%) scores reflect the clinical success achieved with this procedure in the entire group.
Complications of presacral ALIF
The pre-sacral space is devoid of muscle, neural, and significant vascular structures. The presacral fat pad usually measures 1 to 2 cm in thickness. Blunt finger dissection along the distal anterior sacrum can be used to create working space by displacing the rectum away from the sacrum. Through this tissue, the blunt probe is slowly advanced with a twisting motion, maintaining gentle contact with the tip of the guide probe against the anterior sacrum at all times. The rectum can be visualized with air injection during the procedure. The probe should never be advanced forcefully if resistance is encountered. Using these guidelines allows the surgeon to safely advance the probe to the sacral entry point, passing by the rectum. Care should be exercised in very thin patients who may have little or no presacral fat because of the proximity of the rectum to the sacrum. The surgical procedure is easier to perform in patients with a thicker fat pad, which displaces the rectum away from the sacrum.
During surgery, a suspected rectal injury can be diagnosed by contrast injection (Gastrografin; Bracco Diagnostics) into the rectum. When injury is suspected, intraoperative evaluation by a colorectal surgeon can lead to immediate treatment and possible avoidance of a colostomy. The rectal injury that occurred in the present study developed in 1 patient early in our experience and was undetected at the time of surgery. We had failed to identify a history of previous anorectal abscess and, secondarily, a very thin presacral space at the level of the sacro-coccygeal junction. After the abscess was drained on postoperative day 4, the patient used a diversionary colostomy for the next 3 months and the disc space remained clear of infection. However, as a result of this case, patients with any history of local surgery, inflammation, radiation treatment, trauma, or infection are now excluded. In addition, all patients considered candidates for presacral ALIF preoperatively undergo mid-sagittal MRI evaluation of the sacrum and coccyx to exclude those with anomalous anatomy. Since modification of technique and careful screening, no further rectal injuries have occurred after more than 200 additional procedures performed at our institution.
Considering possible vascular complications associated with this approach, the presacral artery that crosses the L5-S1 disc space is a consideration, because it is routinely visible in open ALIF procedures. The size of this vessel decreases quickly below the disc space at L5-S1. At the S1-2 level (the usual sacral entry point for the presacral ALIF), this vessel is small if present at all.41, 42 In 50 patients, no known incidents of vascular injury were documented. In considering use of this minimally invasive ALIF, careful evaluation of the preoperative studies, a special sequence MRI, or a CT angiogram can be helpful in the detection of any anomalous or large vessels at the sacral entry point. Back bleeding, which can occur into the presacral space from the drilled sacral channel, occasionally creates the appearance of a hematoma on postoperative CT. However, none of the patients underwent re-exploration for a suspected vascular injury or a postoperative hematoma. The neuroforamina are widely spaced in the sacrum and should be easily avoided during the approach. In our series, we have had no neurological injuries, device failures, or device removals.
Approach complications with PLIF, TLIF, ALIF and XLIF
Approach complications with other interbody fusion procedures are related to injury risk to nearby anatomic structures. The main disadvantage of the PLIF is the possibility of significant bilateral retraction on the dural sac and nerve roots, which can result in CSF tears, dysesthetic nerve root pain syndromes, nerve root injury, and bilateral epidural fibrosis.15
A TLIF can be performed without exposing more than the ipsilateral foramen (although bilateral decompression can be performed if needed). Exposure and retraction on the dural sac are minimal compared with PLIF. Nonetheless, TLIF still poses risks associated with dysesthetic pain syndromes from neuropractic injuries, dural tears, and CSF leaks. In a series of 74 patients, Villavicencio et al25 reported 4.5% incidence of CSF leak and 12% incidence of neural injuries, although some were attributed to misplaced pedicle screws. TLIF can sometimes be difficult to perform at the L5-S1 level in patients with a steep sacral inclination, overhanging iliac crests, and deep position of the disc; therefore, an alternative approach to the L5-S1 interbody, such as presacral ALIF, can be advantageous.
Disadvantages of ALIF include muscular disruption of the abdominal wall, retraction of the iliac vessels (especially at L4-5), and need for a vascular exposure surgeon. Additionally, inherent destabilization associated with this procedure is caused by the resection of the anterior longitudinal ligament and wide resection of annulus. Retraction of the great vessels leads to the risk of deep venous thrombosis and vascular injury and retrograde ejaculation from probable hypogastric plexus injury.23, 24, 30 In a large prospective study of 279 patients who underwent ALIF, Burkus et al19 reported a total exposure complication rate of 9.3%, including a 7.9% incidence of vascular complications and 1.4% incidence of permanent retrograde ejaculation. In a retrospective review, Rajaraman et al24reported a 38.3% incidence of general surgery-related complications in 60 patients after ret-roperitoneal ALIF. Laparoscopic ALIF is an attempt at minimally invasive fusion, but has been largely abandoned because of high complication rates. In a review of the literature on laparoscopic ALIF at L5-S1, Inamasu and Guiot reported complication rates that ranged from 3 to 34%.27
The XLIF fusion procedure was recently introduced as a mini-open approach from levels L1-2 to L4-5 and cannot be performed at L5-S1.32 Monitoring of the descending nerves of the lumbar plexus is recommended as a standard part of the procedure. In a series of 21 patients who underwent this endoscopic approach, 30% experienced transient groin/ thigh paresthesias.31
As the current procedure accesses the L5-S1 level through the anterior spine, it more closely resembles an ALIF approach than the PLIF or TLIF that use a posterior approach to the spine. In the current study, the complication rate of 2% compares favorably with many reports of higher complication rates in the ALIF literature.
Fusion comparisons
As the criteria for the interbody fusion vary in the literature, comparisons of fusion rates are difficult. A number of studies have reported fusion results base solely on plain radiographs. In a 1987 review by Steffee and Sitkowski41 of the PLIF procedure, and a 1981 retrospective review by Cloward3 of 100 patients who underwent the PLIF, plain film evaluation (without flexion-extension views) was used to assess fusion. In a 1995 report, Mathews et al29 noted that all 6 patients who underwent laparoscopic ALIF had fusion on the basis of lack of motion on lateral flexion-extension views. Of interest, the authors noted that CT scans were not used to assess fusion because of concern of radiation exposure. In a 1998 report on fusion in 947 patients operated on in a multicenter prospective trial using BAK cages, Kuslich et al20 defined fusion as <3° of angular motion on plain films. More recently, Salehi et al12 reported a fusion rate of 91.6% in 24 patients who underwent the TLIF procedure. Fusion evaluated on plain x-rays was defined by absence of halo around the screws, presence of bilateral continuous trabecular bone bridge between fused segments on the anteroposterior x-rays, and lack of motion on lateral flexion extension x-rays. In 2005, Schwender et al17 reported a 100% fusion rate in 49 patients who underwent TLIF. Fusion was defined by the presence of trabecular bony bridging, <3° motion on flexion/extension views, and intact hardware; however, the authors did not specify the imaging study used in the assessment of fusion.
During the last decade when the value of CT technology was realized in the evaluation of fusion, the authors of the present study used high-resolution CT scan to more precisely assess fusion status than could be provided by plain radiographs. In 1997, Mayer43 reported a 100% fusion rate in 25 patients who had an ALIF approach. Using sagittal CT reconstructions, the authors defined fusion as continuous, uninterrupted cancellous bone bridging the intervertebral space from one vertebral body to the other. While we cannot overemphasize the obvious importance of eliminating author bias in evaluation of fusion, few studies have enlisted independent radiologists to interpret such results. In a 2002 multicenter trial for a large number of patients, Burkus et al18 concisely defined fusion as translation of <3mmand angulation of <5° with absence of radiolucent lines around the implant as indicated fusion on plain films. Fusion results were identified on the basis of continuous trabecular bone on CT by independent radiologists. At 12 months, fusion was noted in 96.9% of study patients (LT cages and Infuse) and 92.5% of the control group 92.5% (LT cages and autogenous iliac crest graft). In a 2005 study of 74 patients who underwent TLIF with Infuse, Villavicenio et al25 reported a 1-year fusion rate of 100%; the authors defined fusion as <5° in angular motion of flexion-extension x-rays, and an independent radiologist assessed the evidence of bridging trabecular bone on CT scans.
In our study, an independent neuroradiologist evaluated the fusion results from both plain x-rays and high-resolution CT scans. Fusion was interpreted using plain radiographs by a digital assessment program. Of 50 patients, 44 (88%) showed fusion on CT scan, 5 (10%) showed developing bone at 1 year, and 1 patient had pseudoarthrosis (2%). With high-resolution CT scans, developing fusion can be seen as mass of bone attached to an endplate but incompletely bridging the disc space. Our concept of developing bone (Table 1) has not been reported previously in assessment of fusion. We identified the patient who will likely progress to fusion as evidenced by CT studies as having developing bone, no motion on flexion extension x-ray, and significant improvement of VAS and ODI scores at 1 year. In the 5 patients with developing bone on 1-year follow-up CT scan, 4 were asymptomatic; they showed no motion on flexion-extension films and had significant improvement in VAS and ODI scores reflecting clinically developing fusion. However, the fifth patient with evidence of developing bone on CT may progress to pseudo-arthrosis, because her preoperative pain was unrelieved and she resumed heavy smoking after surgery; VAS and ODI scores showed no improvement.
Use of plain film interpretation of fusion has been the historical standard and only radiographic technique before the development of high-resolution reconstructed CT images. Advantages of plain films for fusion evaluation are ease to performance and access, cost effectiveness, and lower levels of radiation than CT. However, lack of measurable motion by flexion-extension films cannot provide direct assessment of fusion and can overestimate actual fusion rate as seen in this study. In the present series, 1-year fusion rates were interpreted as 100% of patients by plain film and 88% of patients by CT. Therefore, in interpreting reports of fusion rates published, one should consider which methodology was used and how fusion was defined. On the basis of our literature review, we found that modalities to assess the extent of fusion are not equivalent. Realizing this limitation, we propose a classification of fusion criteria based on high-resolution CT scans. Although x-rays were used, it is cautioned that these findings may overestimate the extent of fusion.
In the only other series of AxiaLIF patients published to date, Pimenta et al34 reported an 82% fusion rate with autograft at the end of a 1-year pilot study of 18 patients. Using the methodology of fusion evaluation outlined in Table 1, we noted that our fusion results are comparable with rates described with other interbody fusion techniques in the literature.
Conclusions
The presacral ALIF is a new, minimally invasive technique for fusion at L5-S1 that accesses the spine via what we call the axial corridor. In this study of 50 patients, its safety and 1-year fusion rates compared favorably with other interbody fusion techniques as reported in the literature. Its effectiveness is reflected in improved clinical outcome scores, low complication rates, and excellent fusion rates at the end of 1-year follow-up. The proposed classification of fusion using high-resolution CT may more accurately assess the extent of fusion than x-ray films. Additional long-term follow-up (minimum 2 years) will help to define the efficacy of this minimally invasive spine fusion, specifically for complication rates and fusion outcomes.
Disclosure
William D. Tobler is a consultant and recipient of research grants from TranS1 Inc. and Zimmer Spine, and is a stockholder in TranS1 Inc. Robert Bohinski and Viral Jain have no financial disclosures. Mark E Myers is the independent neuro-radiologist who was compensated for his time to evaluate the results in this study, and has no affiliations with the authors or TranS1 Inc.
- © 2010 Published by Elsevier Inc. on behalf of SAS - The International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.