


Abstract
Background Ehlers-Danlos syndrome (EDS) is a heterogeneous collection of connective tissue disorders characterized by varying degrees of skin hyperextensibility, joint hypermobility, and tissue fragility. Surgical treatment of EDS patients is complicated by the extreme fragility of their vessels and tissues. The purpose of this case report is to present the management of an EDS patient with debilitating low-back pain.
Methods A 52-year-old woman with a clinical diagnosis of EDS presented with degenerative disc disease at L4-5 that had not been alleviated by previous microdiscectomies. The clinical course, decision-making process, and treatment are discussed in this case report.
Results The patient was referred for genetic evaluation, which classified her with type III EDS, or hypermobility type. We presented the patient with the risks and benefits of fusion versus artificial disc replacement (ADR), particularly with regard to her EDS diagnosis of the hypermobility subtype. Given the patient's lack of extreme spinal hypermobility on examination and the absence of clear contraindications regarding ADR in type III EDS, the decision was made to proceed with ADR. There were no surgical complications, and the patient's low-back pain and radicular symptoms resolved with no evidence of implant migration or hypermobility at 1 year postoperatively.
Conclusions In this case report, the referral to a geneticist and consultation with a vascular surgeon were integral steps in the decision to proceed with surgery. Although the clarified diagnosis of type III EDS did not eliminate the potential risk for vascular compromise during surgery, it placed the patient at lower risk than patients with other subtypes of EDS. Similarly, her lack of extreme hypermobility made us more comfortable with pursuing ADR. Although we emphasize extreme caution when considering surgical treatment, this case report suggests that some patients with less severe forms of EDS may be able to successfully undergo anterior spine surgery, including ADR.
Ehlers-Danlos syndrome (EDS) is a collection of heritable disorders featuring abnormally lax and fragile connective tissue. According to the revised classification system,1 there are 6 different subtypes of EDS: classical (EDS I and II), hypermobility (EDS III), vascular (EDS IV), kyphoscoliosis (EDS VI), arthroclasia (part of EDS VII), and dermatosparaxis (included in EDS VII). EDS patients manifest a variety of clinically challenging problems, including chronic musculoskeletal pain, chronic fatigue, soft-tissue and visceral injury, cardiovascular pathology, skin abnormalities, and neurologic problems.2 Varying degrees of skin hyperextensibility, delayed wound healing, joint hypermobility, atrophic scarring, tissue fragility, and excessive bruising and bleeding may also occur.3 At the molecular level, mutations in the genes that encode collagen and/or collagenrelated proteins are thought to produce the constellation of symptoms present in the subtypes of EDS. Despite advances in genetic testing for specific subtypes of EDS, the phenotypic presentation of any single patient may span 2 or more subtypes of EDS, and often, definitive genetic testing is unavailable.4–8
Spinal anomalies are common across many subtypes of EDS because of ligamentous laxity and bony malformations inherent to the disorder. Cases of spondylolisthesis,9 thoracic scoliosis,10 thoracic kyphosis,10 double-structure scoliosis, 10–13 lumbar scoliosis,14 thoracolumbar junctional kyphosis, 14 and lumbar lordosis12 have been reported in the literature. Importantly, surgical treatment of spinal disorders in patients with EDS can be complicated by the extreme fragility of their vessels and tissues and the tendency for prolonged bleeding after vascular injury. There are various reports of intraoperative and postoperative complications associated with spine surgery in patients with EDS, including avulsion, rupture, and/or thrombosis; these complications are more frequently encountered during anterior approaches. 12–16 A recent case report described the significant blood losses encountered in 3 patients with EDS during anterior spine surgery.14 These patients had injury to the iliac artery, segmental artery, and abdominal aorta with blood losses ranging between 600 mL and 6 L. Vascular injuries associated with spine surgery have also led to significant neurologic consequences, including paraplegia.16 Furthermore, Debnath et al.13 presented a case report of a 20-year-old man in whom quadriparesis developed after 2-stage surgical correction of kyphotic deformity and who ultimately died at 10 months postoperatively due to sepsis and respiratory failure.
As described earlier, there are different subtypes of EDS and patients within each subtype can have varying degrees of disorder severity. The most common form of EDS is subtype III, or the hypermobility type, in which patients have generalized excessive hypermobility of the large and small joints. Although it is usually considered the least severe type of EDS, it is associated with subluxations and dislocations, as well as degenerative joint diseases. In general, patients with EDS subtypes I (classical, gravis), II (classical, mitis), and especially IV (vascular) carry the highest risk for vascular complications,14, 15, 17–20 although reports of vascular compromise with other EDS subtypes have been reported in the literature.12, 16 Gastrointestinal complications also frequently occur, either spontaneously or during the postoperative period, and include large bowel and sigmoid perforations, paraesophageal hernias, small bowel obstructions, and peritonitis.15 On the basis of the potential for serious vascular complications among the varying subtypes of EDS, special considerations must be taken when a patient with EDS presents for surgery.
In addition to vascular risk, another clinical feature of EDS that should be taken into account when one is planning orthopedic surgery is the degree of joint hypermobility. A recent survey of 246 EDS patients found that 93% of the patients reported joint hypermobility and 78% had experienced dislocations.21 Presumably, there is an increased risk for continued hypermobility and instrumentation failure after arthroplasty in this population. As a result, surgeons may be more likely to recommend arthrodesis over arthroplasty. However, if a patient does not show extreme hypermobility, then arthroplasty may potentially be an appropriate option. Unfortunately, there are no comprehensive studies of hip, knee, or spine arthroplasty outcomes in EDS; therefore it is unclear whether varying degrees of joint hypermobility place these patients at differential risk for poor outcomes after arthroplasty.
The following case report describes a patient with a previous clinical diagnosis of EDS who presented with recurring low-back pain, numbness, and paresthesias in the lower extremities. After clinical assessment and surgical consideration, she was found to be an appropriate candidate for disc replacement despite her diagnosis of EDS.
Case Report
A 52-year-old woman with a clinical diagnosis of EDS (without formal genetic evaluation) presented with progressive, debilitating low-back pain and right lateral hip pain of 3 to 4 years’ duration. She also complained of numbness and tingling on the plantar aspect of the right foot including the second and third toes. The patient had a history of 3 prior microdiscectomies over a period of 6 years at L4-5 (right), L4-5 revision (right), and L4-5 (left). These surgeries were performed at another institution through a posterior approach without significant reported complications. The patient's surgical history was also remarkable for bilateral patellar replacements, 4 cesarean sections, right thumb carpometacarpal arthroplasty, bilateral medial collateral ligament repair, ventral hernia repair, and laparoscopic gastric banding. She had no gastrointestinal or vascular complications from these surgeries.
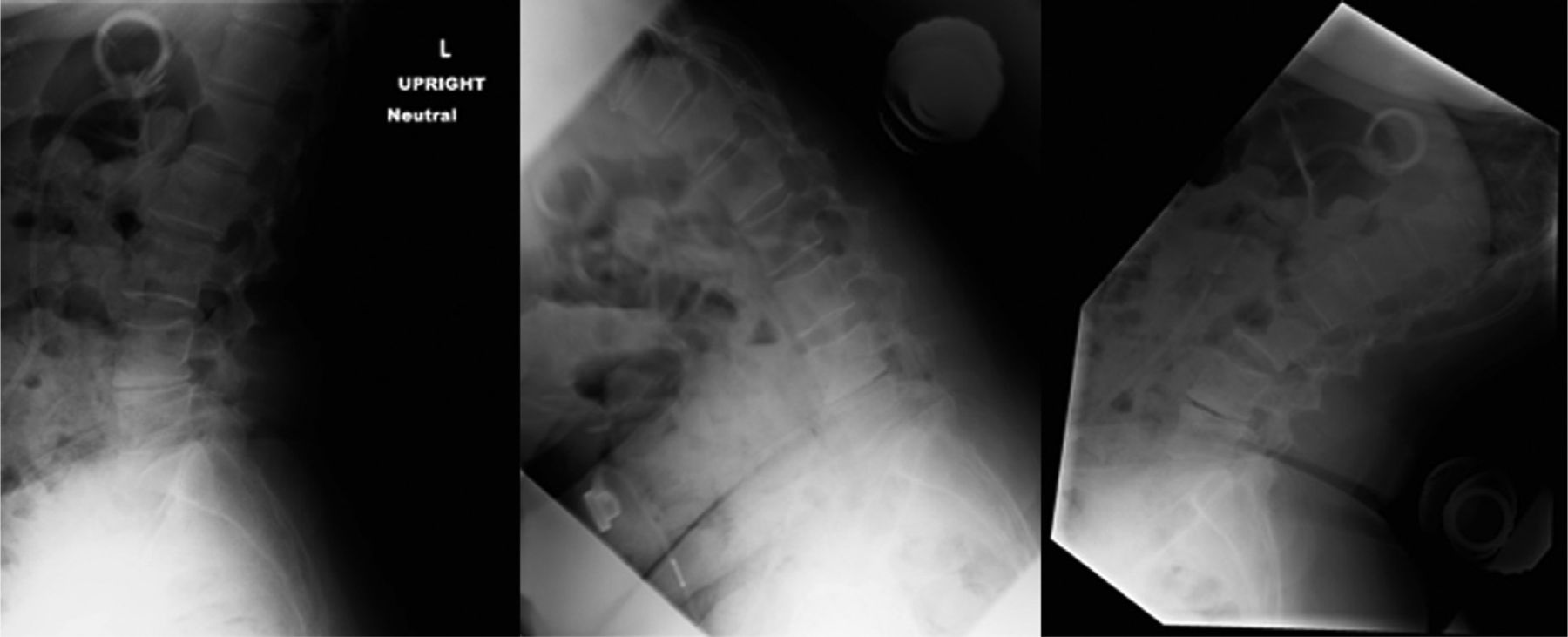
Physical examination and radiographs showed mild increased flexibility of the lumbar spine in flexion and extension that did not exacerbate the patient's pain (Fig. 1). She had tenderness to the sacroiliac joint bilaterally, the greater trochanters bilaterally, and the paraspinal region between L4 and S1 bilaterally. There was decreased tactile sensation in the second and third toes bilaterally and lateral thighs bilaterally. Lower extremity strength was intact and rated as 5/5, and range of motion was also intact. Physical features of EDS IV, such as translucent velvety skin, bitemporal narrowing, and absence of earlobes, were not present on physical examination.

Preoperative flexion/extension radiographs show possible mild hyperflexibility but no evidence of extreme hypermobility.
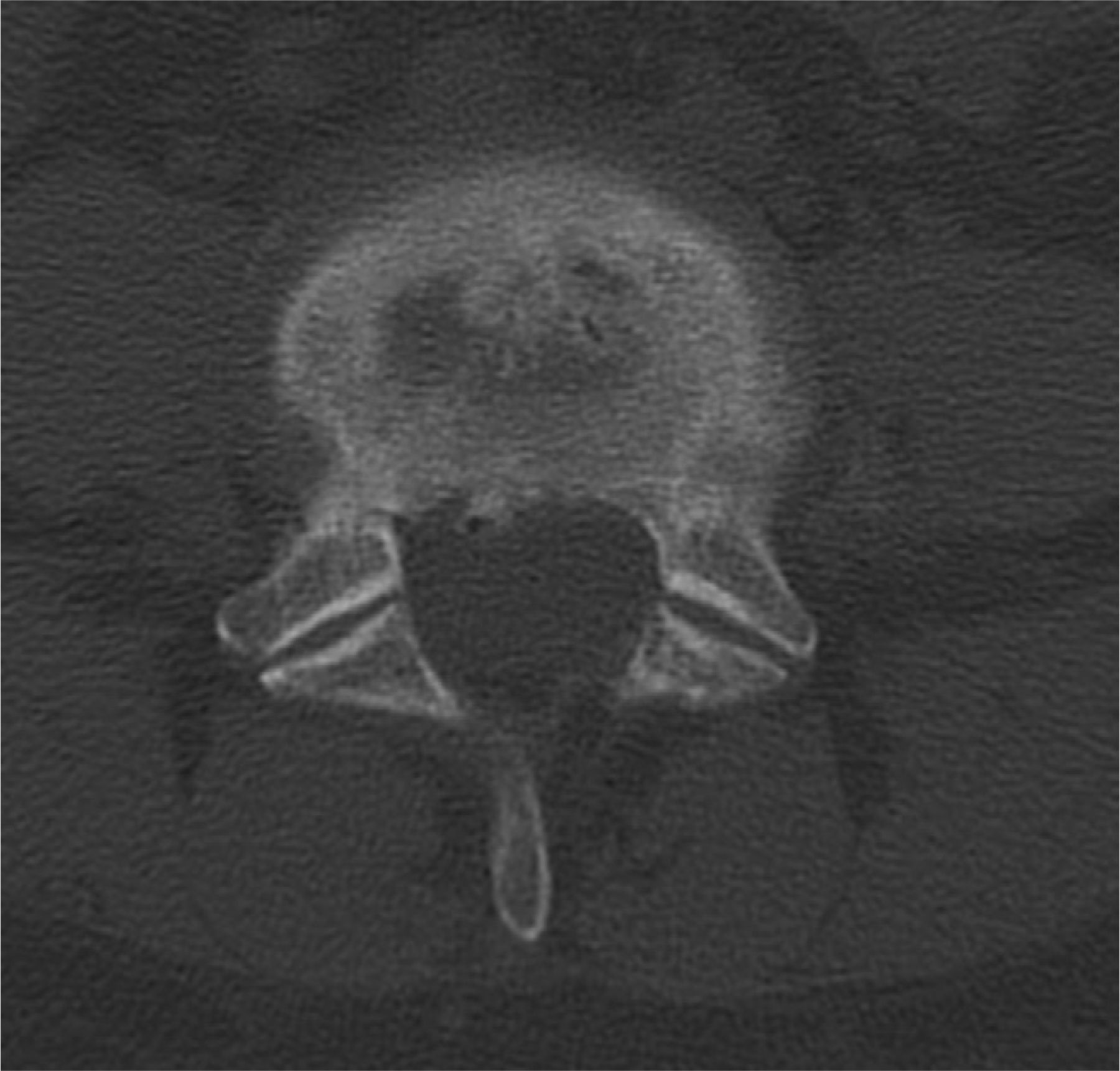
Computed tomography and radiographs of the lumbar spine showed degenerative disc disease at L4-5 with bilateral foraminal stenosis and bulging of the disc (Fig. 2). L5-S1 showed moderate degenerative disease of the disc with mild bulging. There was no radiographic evidence of spondylolisthesis, and computed tomography discogram images showed minimal facet arthrosis at L4-5 (Fig. 3). Thus the patient met the general indications for either artificial disc replacement (ADR) or fusion. However, given the prior clinical suspicion for a subtype of EDS, the patient was referred to the department of genetics for evaluation and confirmation of her EDS subtype before formulation of a surgical plan. In light of the numerous case reports in the literature detailing excessive blood loss in EDS patients, the possibility of vascular injury when performing an anterior surgical approach in this patient was a significant concern. Subsequent genetic evaluation and clinical opinion classified the patient as having type III EDS, or the hypermobility type. After confirmation of her EDS subtype and extensive consultation with the geneticist and the vascular approach surgeon, surgical consent was undertaken with the patient with regard to the general and specific risks and benefits of fusion versus disc replacement, particularly in relation to her EDS diagnosis of the hypermobility subtype. Although biomechanical studies have shown that ADR is associated with a decrease in adjacent level forces relative to fusion and thus may be beneficial at decreasing adjacent level degeneration, it is unclear whether this would necessarily support ADR more than fusion in a patient with EDS. After due consideration of the informed consent, the patient elected to undergo ADR despite encouragement toward fusion. Given the patient's lack of extreme spinal hypermobility on examination and the absence of literature or clear contraindications regarding ADR in type III EDS, the decision was made to proceed with ADR.
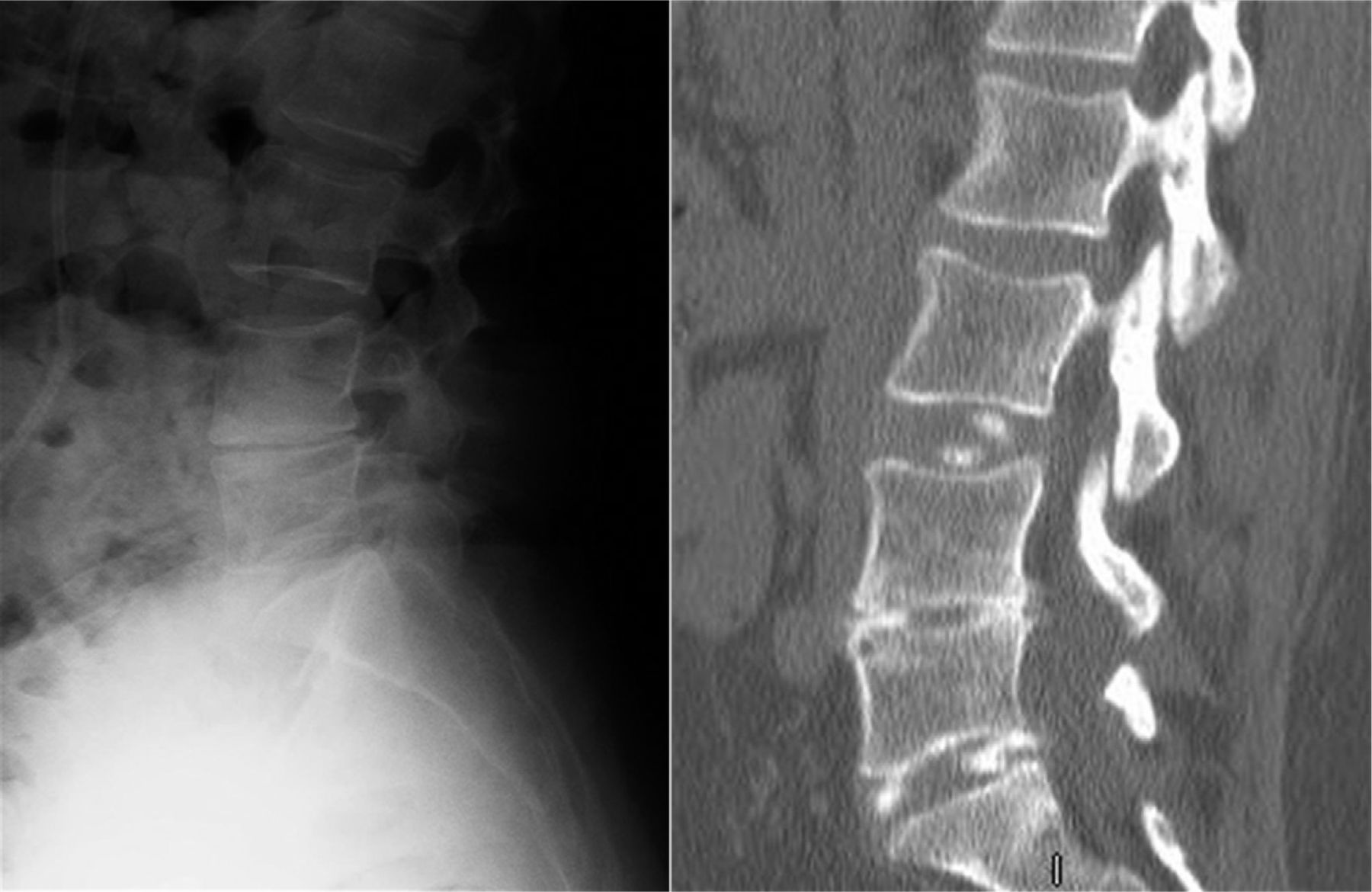
A preoperative lateral radiograph and computed tomography image of the lumbar spine show degenerative disc disease at L4-5 with bilateral foraminal stenosis and bulging of the disc.

A preoperative axial computed tomography discogram image shows L4-5 facets with minimal arthrosis and previous laminectomy defect.
The patient was taken to surgery for an L4-5 ADR procedure, which was performed through an anterior approach by the vascular surgeon. The retroperitoneal space was entered below the semilunar line to the left of midline, and bipolar cautery was used to develop the retroperitoneal plane and fully mobilize the left common iliac artery and vein to the right of midline. The L4-5 disc was completely removed, followed by a decompression of the posterior aspect of the disc. Great caution was taken to not remove more annulus than absolutely necessary. A ProDisc-L implant (Synthes Spine, West Chester, Pennsylvania) was then placed under fluoroscopic guidance. Meticulous hemostasis was maintained through a combination of FloSeal (Baxter, Deerfield, Illinois) and gentle compression. The wounds were closed in a multilayered fashion. The patient had no intraoperative or postoperative complications. Flexion and extension radiographs (Fig. 4) at 9 months postoperatively showed excellent motion at L4-5 without hypermobility. The motion at the treated and adjacent levels as measured on preoperative and postoperative flexion/extension radiographs was similar, if not improved, after surgery but not beyond a physiological range (change from preoperative to postoperative of 13° to 15° at L3-4, 11° to 16° at L4-5, and 12° to 10° at L5-S1). At 1 year postoperatively, the patient's low-back pain and radicular symptoms had completely resolved (pain rated 0 of 10 on a visual analog scale) and her range of motion, strength, and sensation were all within normal limits bilaterally. Anteroposterior and lateral radiographs showed no subsidence or migration of the artificial disc at that time (Fig. 5).

Flexion and extension radiographs at 9 months postoperatively show excellent motion at L4-5 without hypermobility.
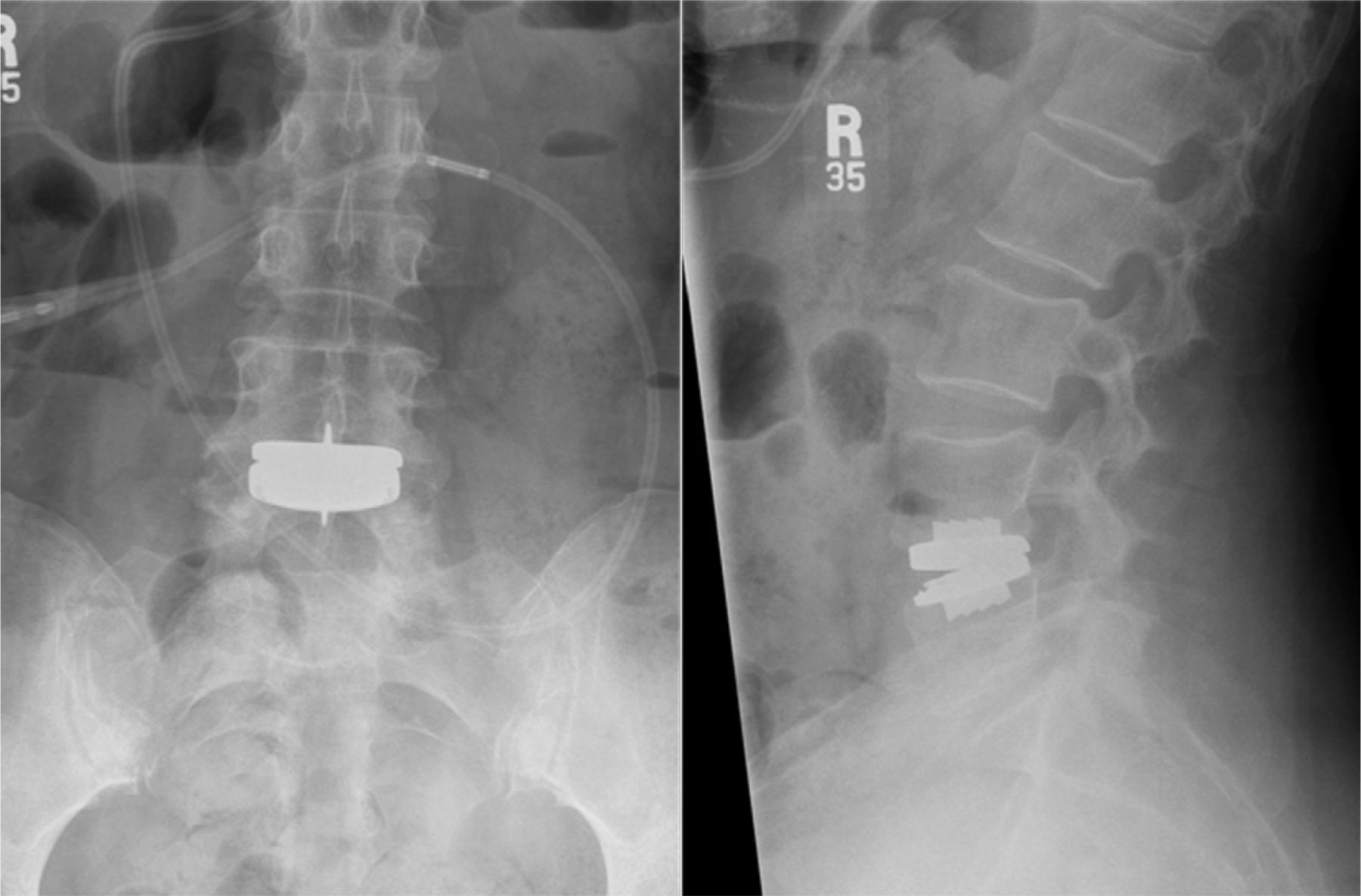
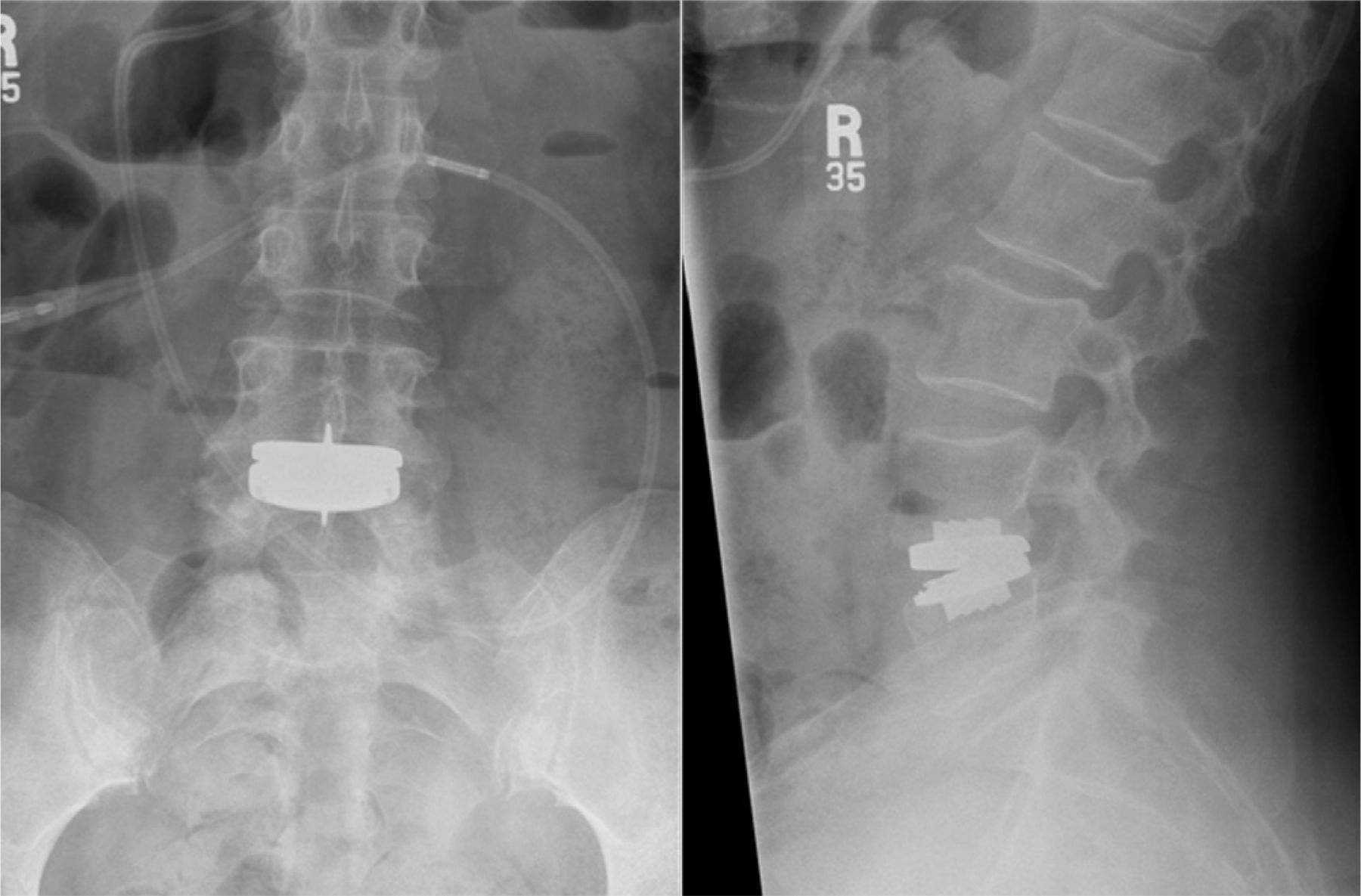
Anteroposterior and lateral radiographs at 1 year postoperatively show no subsidence or migration of the artificial disc.
Discussion
EDS is a complex group of disorders that includes skin hyperextensibility, delayed wound healing, joint hypermobility, atrophic scarring, tissue fragility, and excessive bleeding. Spinal malformation is a common finding in these patients, and many patients may seek surgical treatment. However, it is imperative for surgeons to recognize the increased risk for serious surgical complications in patients with EDS, most notably vascular compromise, and to exercise vigilance when planning the appropriate surgical approach. Case reports in which patients have lost anywhere from 1 to 6 L of blood intraoperatively show the extreme vascular fragility of patients with EDS. Other reports have described catastrophic complications, including paraplegia, quadriparesis, and death.13, 16 In addition to perioperative vascular complications, there is also a potential risk for poor postoperative arthroplasty outcomes due to extreme joint hypermobility and dislocation.
This study describes a patient who presented with a clinical diagnosis of EDS and a history of recurring lowback pain and paresthesias that were not alleviated by her 3 prior microdiscectomies at L4-5. Given concerns regarding the vulnerability of the abdominal aorta and iliac vessels during an anterior approach to the spine, the patient underwent genetic testing to verify her EDS diagnosis and to discuss the risks of an anterior approach. This testing classified her as having EDS type III (hypermobility type) and excluded, on clinical grounds, a diagnosis of type IV (vascular type). Although this diagnosis did not eliminate the potential risk for vascular compromise during surgery, it placed the patient at lower risk for major bleeding and vascular damage than those patients with other subtype of EDS, such as types I, II, and IV. In addition to the vascular concerns associated with an anterior approach in this patient, there was a question as to whether her EDS classification of the hypermobile type was a contraindication to undergoing ADR. The primary concern was that hypermobility could result in dislocation of the disc replacement, and the patient was encouraged to consider fusion. However, after thorough physical examination and review of her flexion/ extension radiographs, there was no evidence of extreme spinal hyperflexibility that would have increased the risk for postoperative dislocation of the disc replacement device. In addition, the biomechanics of the ball-and-socket design of the ADR device provided more confidence in the stability once the endplates integrated to the bone. The patient ultimately opted for ADR, and we proceeded with disc replacement at L4-5 using an anterior approach. The patient did not have any perioperative complications, and she was symptom free at her most recent follow-up of 1 year postoperatively. Radiographs at that time showed no migration of the ADR implant or evidence of hypermobility at the treated level.
The variability in presentation and severity of EDS is dramatic. Given the numerous publications that detail serious complications resulting from vascular injury and major bleeding during surgery, surgeons should be circumspect when operating on patients with EDS. In particular, an anterior approach requires dissection and mobilization of tissues and vessels, which can be excessively fragile in certain types of EDS. Although caution should be emphasized when one is considering surgery, this case report suggests that some patients with less severe forms of EDS may be able to successfully undergo anterior spine surgery, including disc replacement. The referral to a geneticist is an integral step in the decision to proceed with surgery. Had we not obtained genetic counseling in this patient to determine her ADS III subtype, anterior spine surgery most likely would have been deemed too risky. Furthermore, had this patient displayed extreme hypermobility of the spine, her EDS hypermobility diagnosis would have been considered a contraidication to arthroplasty. Given the combination of a nonvascular subtype of EDS and the lack of extreme hyperflexibility in the spine, this patient was ultimately deemed suitable for disc replacement and she encountered no intraoperative or postoperative complications.
This case highlights the importance of a multidisciplinary approach that includes spine and vascular surgeons as well as a geneticist to manage a patient with EDS. This approach may be helpful when one is considering surgical treatment of EDS patients, in whom there is the potential for significant perioperative complications. To our knowledge, this is the first article to describe a patient with a subtype of EDS who underwent an anterior approach for disc replacement in which there were no complications. It is important to note, however, that we are not suggesting that all EDS patients are candidates for anterior spine surgery or disc replacement. Only those with decreased risk for vascular and hypermobility complications should be evaluated, and even then, extreme caution and careful judgment should be exercised.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}