


Abstract
Background Fluoroscopy is widely used in spine surgery to assist with graft and hardware placement. Previous studies have not measured radiation exposure to a surgeon during minimally invasive lateral lumbar spine surgery for single-level discectomy and interbody cage insertion. This study was performed to model and measure radiation exposure to a surgeon during spine surgery using the direct lateral lumbar procedure.
Methods The study was performed using a mannequin substituting for the surgeon and a cadaver substituting for the patient. Radiation was measured with dosimeters attached to 6 locations on the mannequin using a OEC Medical Systems 9800 C-arm fluoroscope (OEC Medical Systems, Salt Lake City, Utah). Three different fluoroscopy setups were tested: a standard imaging setup, a standard setup using pulsed-mode fluoroscopy, and a reversed setup. The experiment was tested 5 times per setup, and the dosimeters’ values were recorded.
Results The highest amount of radiation exposure occurred when obtaining an anteroposterior view of the spine in the standard setup. Compared with the standard setup, the pulsed-mode setting decreased the radiation exposure to the mannequin by a factor of 6 times (P < .001). Compared with the standard setup, the reversed setup also decreased the radiation exposure to the mannequin by a factor of 6 times (P < .001) and it had the lowest amount of radiation exposure to the eye level (P < .001).
Conclusions Care should be taken when one is obtaining an anteroposterior view of the lumbar spine during lateral lumbar procedures to limit radiation exposure. Radiation exposure to the surgeon can be greatly minimized by using either a pulsed imaging mode or the reversed setup. The reversed setup has the lowest amount of radiation exposure to the eye level.
Minimally invasive spine surgery offers benefits over traditional spine surgery, including less tissue injury, less intraoperative blood loss, and a shorter hospital stay.1–6 However, to perform these types of spinal surgeries, fluoroscopy is essential to visualize the spinal anatomy for accurate placement of graft material and hardware. Ionizing radiation continues to be a safety concern for many surgeons, especially because this has been associated with skin cancer, glaucoma, and thyroid cancer.7–9 It is important that surgeons understand the potential risks of scatter radiation when using fluoroscopy to prevent these iatrogenic medical conditions.
Compared with nonspinal procedures, the spine surgeon can be exposed to 10 to 12 times the amount of radiation when performing spinal procedures under fluoroscopic guidance.10 Radiation exposure to the surgeon has been evaluated for both cervical and posterior lumbar procedures. 10–13 General principles have been identified to reduce the amount of radiation exposure to the surgeon, such as increasing the distance from the fluoroscope source and having the radiation source inferior to the patient to reduce X-ray scatter to the surgeon.7
This study was undertaken to quantify radiation exposure to the surgeon performing a single-level discectomy and insertion of an interbody cage while using the lateral lumbar approach with intraoperative fluoroscopic guidance. The second purpose of this study was to evaluate potential methods to reduce radiation exposure to the surgeon by changing the image intensifier position or by altering the fluoroscopic exposure time.
Methods
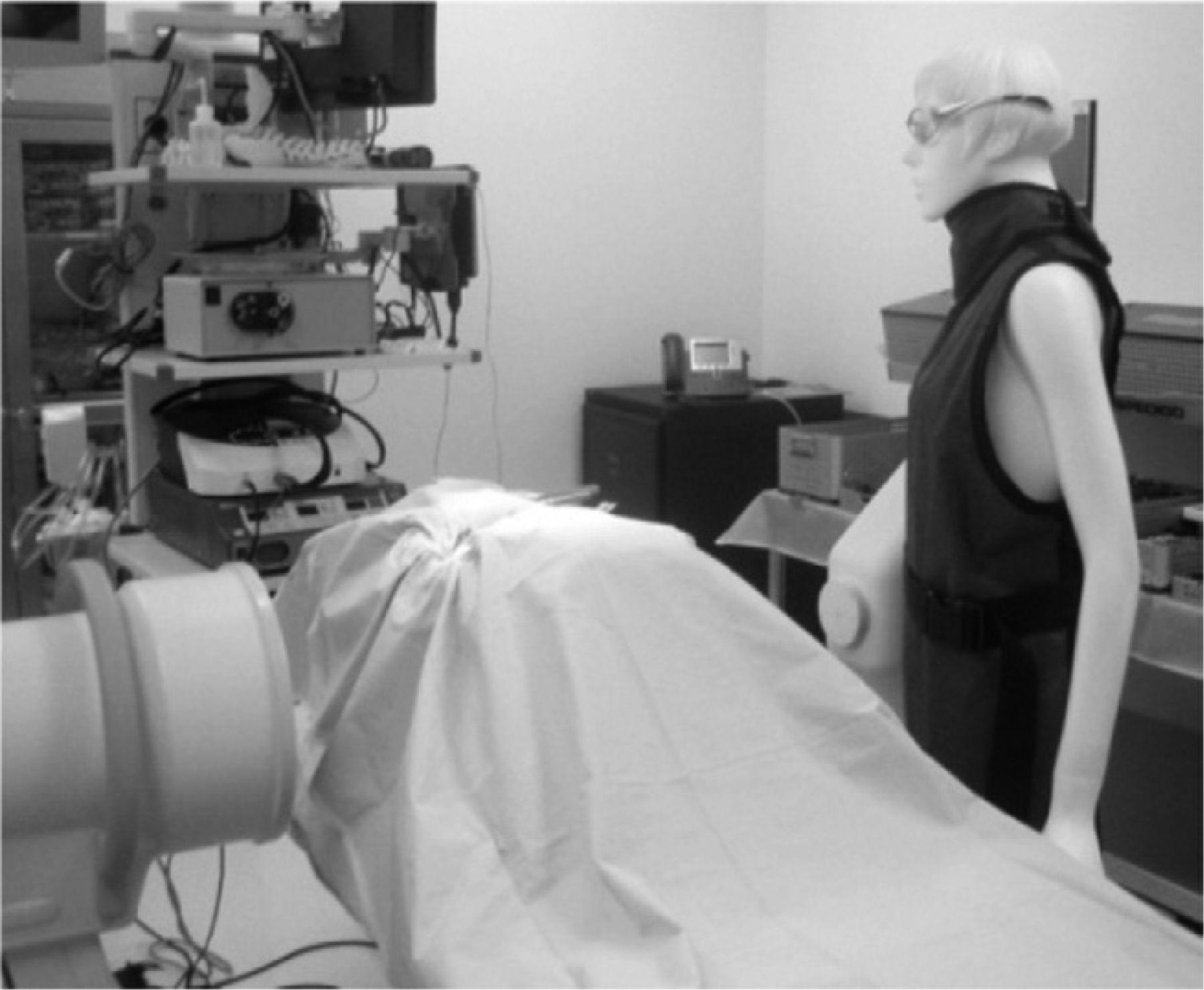
A cadaver (68-year-old female cadaver, 5 ft 8 in, 150 lb) was placed in the lateral decubitus position for preparation of a lateral interbody procedure on an operating table. The cadaver was draped in a normal sterile fashion. In place of an actual surgeon, a mannequin was used, standing at the dorsal aspect of the cadaver torso where a surgeon would typically stand. Film badge mini-dot dosimeters (Landaurer, Glenwood, Illinois) were placed on the mannequin. These dosimeters accurately detected exposures from 10 to 1 million mrem. The dosimeters were placed at the midline eye level, thyroid, right and left chest, and right and left thigh (Fig. 1). A calibrated 9-inch fluoroscope (9900 Elite series; OEC Medical Systems, Salt Lake City, Utah) was used to image the cadaveric specimen. The machine was set to the “automatic mode” so that the image adjusted automatically to penetrate the cadaver.

Mannequin with dosimeters.
Three testing scenarios each were performed 5 separate times to obtain radiation exposure levels. Before each event, a new series of dosimeters were applied to the mannequin. During each testing event, the cadaver was imaged for 22 seconds while the lateral image was obtained and for 13 seconds while the anteroposterior (AP) image was obtained. These time values reflected the average times the author recorded from 15 prior patient cases while orienting, navigating, and inserting a single-level interbody lumbar cage without instrumentation during the lateral lumbar procedure.
The three different scenarios studied were as follows:
For the standard setup, the lateral image was taken with the source underneath the cadaver. The AP image was taken with the source near the back of the cadaver (closest to the mannequin). The exposure time was 1 second. In the lateral image position, the receiver-tocadaver distance was 12 inches, the source-to-table distance was 7 inches, and the receiver-to-surgeon distance was 13 inches. In the AP image position, the receiver-to-cadaver distance was 10 inches, the source-to-cadaver distance was 12 inches, and the source-to-surgeon distance was 6 inches (Figs. 2 and 3). The fluoroscope settings (auto) were 9.1 kVp and 4.1 mA in the lateral image position and 8.2 kVp and 3.2 mA in the AP image position.
For the standard setup in pulsed mode, the same setup as that in scenario 1 was used but the machine was in pulsed mode, meaning the exposure time was one-sixth of a second. Thus 6 times more images were obtained for the given amount of time. The fluoroscope settings were 8.8 kVp and 3.8 mA in the lateral image position and 8.7 kVp and 3.7 mA in the AP image position. In the lateral image position, the receiver-to-cadaver distance was 12 inches, the source-to-table distance was 7 inches, and the receiver-to-surgeon distance was 13 inches. In the AP image position, the receiver-to-cadaver distance was 10 inches, the source-to-cadaver distance was 12 inches, and the source-to-surgeon distance was 6 inches.
For the reversed setup, the lateral image was taken with the source underneath the cadaver. The exposure time was 1 second. The AP image was taken with the source near the front of the cadaver. In the lateral image position, the receiver-to-cadaver distance was 12 inches, the source-to-table distance was 7 inches, and the receiver-to-surgeon distance was 6 inches. In the AP image position, the receiver-to-cadaver distance was 10 inches, the source-to-cadaver distance was 12 inches, and the receiver-to-surgeon distance was 6 inches. The fluoroscope settings were 8.9 kVp and 3.9 mA in the lateral image position and 8.4 kVp and 3.4 mA in the AP image position (Figs. 4 and 5).

Standard setup: AP image.

Standard setup: lateral image.

Reversed setup: lateral image.

Reversed setup: AP image.
Results
Anatomic radiation localization
Results with the standard setup showed that the right and left abdomen of the surgeon had the highest exposure to radiation. Results with the standard setup in pulsed mode and the reversed setup also showed that the right abdomen and left abdomen were the areas of highest radiation exposure (Table 1). Other anatomic areas (eg, eye and thyroid) received significantly less radiation than the abdomen.
Radiation dosages by scenario
Scenario evaluations
The standard setup scenario showed radiation exposure to the head and thyroid between 1.6 and 2.6 mrad and exposure to the chest and abdomen between 3.2 and 6.6 mrad (Table 1). The standard setup using the pulsed mode of imaging had between 0.4 and 1.4 mrad of exposure. The reversed setup had radiation exposure between very low levels and 1.4 mrad (Table 1).
There were no significant differences in radiation exposure between the standard setup in pulsed mode and the reversed setup when the separate anatomic regions were compared except for the eye, where the reversed scenario caused less radiation exposure than the pulsed mode (Table 2). When the standard setup was compared with the standard setup in pulsed mode, the pulsed procedure caused less radiation exposure to all anatomic areas (Table 2). When the standard setup and reversed setup scenarios were compared, the reversed setup also caused less radiation exposure to all anatomic areas (Table 2).
Comparison of 3 scenarios
Discussion
Fluoroscopy will continue to be used by surgeons, especially as more minimally invasive techniques evolve. Fluoroscopy offers the benefits of accurate implant placement and anatomic visualization with the caveat of increased radiation exposure to the surgeon. There have been many studies that have evaluated the scatter radiation exposure to the surgeon for the cervical and lumbar spine, but no previous study has evaluated the lateral lumbar approach that demands the use of fluoroscopy.
On the basis of this study's results, the surgeon's torso receives the most radiation exposure during thoracic spine procedures. This intuitively makes sense because the surgeon's trunk is closest to the radiation source of the fluoroscope while obtaining an AP image of the spine. While the surgeon is obtaining a lateral image of the spine, the radiation source is inferior to the bed and scatter radiation is deflected to the floor, reducing exposure to the surgeon.
Our results show that one practical way to decrease radiation exposure is to use pulsed-mode imaging. The exposure time is changed to one-sixth of a second, and thus 6 times as many images can be obtained for the same amount of total radiation exposure. Another benefit with this technique is that surgeons do not have to change the fluoroscope position. A potential limitation, however, is that imaging obese patients using this setting can decrease image clarity. The author often obtains the initial localization of the disc space of interest using the continuous fluoroscope setting and then switches to the pulsed mode during the actual procedure. More importantly, the pulsed-mode setting can be used while obtaining AP images of the spine, when the fluoroscopic source is closest to the surgeon.
Another technique to decrease radiation exposure to the surgeon is to reverse the fluoroscopy setup such that the source is opposite the surgeon while obtaining an AP view of the spine. The benefit of this technique is that the image clarity will not be compromised in obese patients. Furthermore, there is less scatter radiation to the eye level because the fluoroscope radiation source is farther from the surgeon. Surgeons who place posterior hardware while the patient is in the lateral decubitus position might also find this scenario beneficial because it produces less radiation scatter while obtaining AP spine images. One caveat to using the reversed fluoroscopy setup is that the fluoroscope base can limit surgeon elbow room, depending on the arc length of the apparatus.
The shortcomings of this study are that the fluoroscopy times were calculated averages from actual operative times for single-level lateral interbody fusion. These times may be longer or shorter depending on the surgeon's experience with the lateral-based lumbar procedure. These predetermined times included the time to localize and insert a lateral interbody cage only. This study did not include the radiation exposure while inserting posterior hardware because this has already been published.10, 12, 14
Another shortcoming of this study is that the radiation exposure of the hands was not evaluated. Typically, the surgeon's hands have the greatest risk for radiation exposure with cervical and lumbar procedures because they are close to the wound.15 With the lateral lumbar procedure, the hands are typically the farthest away from the radiation source with the advent of long-handled instruments and holders. Other studies have already evaluated radiation exposure to the hands and reported that it is around 53.3 mrem/min.
It is important to develop strategies to reduce scatter radiation to limit the cumulative lifetime radiation exposure to the surgeon. The National Council on Radiation Protection & Measurements recommends a maximum radiation dosage of 5000 mrem/y for the whole body.15 On the basis of this value, one could perform 757 single-level procedures with the standard setup. Using the standard setup in pulsed mode or with the reversed scenario, one could perform up to 3571 single-level procedures. Rampersaud et al10 found that radiation exposure to the torso was 53 mrem/min near the source and 2.2 mrem/min near the intensifier (there was no pulsed setup performed in this study). When including 1 minute of fluoroscopy to insert posterior pedicle screws near the intensifier along with a single-level interbody lateral procedure, the surgeon could perform 324 procedures using the standard setup or 1388 procedures using the reversed setup and still be within annual radiation exposure guidelines (Tables 3 and 4).
Number of fluoroscopically assisted cases to reach 5000 mrem
Annual exposure limits
Fluoroscopy for spine surgery cases is often necessary for accurate spine hardware insertion, especially in minimally invasive procedures. Spine surgeons need to be aware of techniques to reduce direct or indirect radiation exposure. Our study shows that radiation exposure can be reduced by using fluoroscopy in the pulsed mode for surgeons who prefer the standard fluoroscopy setup or by reversing the fluoroscopy setup to radiate from the ventral aspect of the patient to keep the source away from the surgeon while obtaining AP images.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.