


Abstract
Background Patients with spinal epidural metastases (SEM) often experience a reduction in ambulatory status and, thus, the quality of life. Predicting which patients will benefit from a surgical intervention remains a challenge. Life expectancy is an essential factor to be considered in surgical decision-making, although not the only one. Prediction models can add value in surgical decision-making. The goal of this study was to develop and internally validate a novel model (Limburg spinal metastases score [LSMS]) and compare the predictive value with 2 commonly used models: modified Bauer score and Oswestry Spinal Risk Index (OSRI).
Methods We retrospectively analyzed 144 consecutive patients who underwent surgical decompression for SEM in our centers between November 2006 and December 2020. Clinical and surgical parameters were evaluated. The novel prediction model was based on multivariate analysis and was internally validated. External validation of the 2 most commonly used prediction models was performed.
Results The median survival was 17 months, 55.7% of the immobile patients regained ambulation postoperatively. In 50 patients (34.7%), at least 1 complication occurred within 30 days after surgery. The LSMS consists of 4 parameters: primary tumor type, Karnofsky performance score, presence of visceral metastases, and presence of multiple spinal metastases. Bootstrap internal validation of the model developed on this cohort yielded an optimism-corrected c-statistic of 0.75 (95% CI: 0.71–0.80). The c-statistic of the OSRI score and the Bauer score was 0.69 (95% CI: 0.64–0.74) and 0.67 (95% CI: 0.62–0.72), respectively.
Conclusion The LSMS consists of 4 parameters to assist surgical decision-making for patients with SEM. The score is easy to use and appears more accurate in our population in comparison with previous existing models.
Clinical Relevance A novel prediction model was developed to aid in surgical decision-making for patients with spinal epidural metastases.
Level of Evidence 3.
Introduction
Spinal epidural metastases (SEM) occur in about 5% to 10% of cancer patients. The most common primary tumors originate from breast, prostate, and lung.1,2 Patients with SEM generally present with axial pain, radiculopathy, and/or neurological deficit due to spinal cord compression. These complaints lead to a reduced ambulatory status and, thus, to a reduced quality of life.3–5 Considering that these patients are in the last stage of their lives, quality of life is of utmost importance. The main goal of surgery in this palliative setting is to maintain neurological function and ambulatory self-sufficiency. It remains difficult to predict whether the morbidity and associated complications outweigh the benefits of surgery. Adequate prediction of survival is, therefore, essential in surgical decision-making.
Patchell et al6 showed that selected patients with axial or neurological pain, or (impending) neurological deficit, who underwent direct surgical decompression and stabilization of the SEM followed by radiotherapy showed superior results in ambulatory status compared with patients who received radiotherapy alone. Moreover, they showed that quality of life improved significantly in surgically treated patients.7,8
Unfortunately, the perioperative complication rate and associated morbidity of these procedures are high, with major complication rates varying from 13% to 27%.9–11 The occurrence of complications does not only negatively affect the quality of life but also impedes adjuvant treatment, which in turn affects survival.11
Identifying factors to predict survival can help to select patients who will truly benefit from a surgical intervention.12 Factors such as the extent of the disease, tumor histology, and general physical condition of the patient could be relevant in choosing the appropriate treatment strategy in order to avoid over- or undertreatment.13
Several prediction models have been developed to assess whether an individual patient is a good candidate for surgery. Outcomes are based on improvement in quality of life in correlation with treatment burden.13–21 Two models are commonly used: the Oswestry Spinal Risk Index (OSRI)14 and the modified Bauer score.22 These prediction models have been internally and externally validated.23–28 However, results of those external validation efforts are inconsistent.29
The goal of this study was to develop and internally validate a novel model to optimize surgical decision-making in our population and to externally validate the OSRI and modified Bauer score models in our center. The Limburg spinal metastasis score (LSMS) will predict survival in patients with SEM in whom surgical intervention is considered.
Methods
A retrospective cohort study was conducted at 2 tertiary referral centers. Both institutional review boards approved this study (Medical Ethical Committee [METC) 2018–0602 and Z2021079). Patients were identified based on surgical coding in the hospital’s database. Patients who underwent surgery for SEM between November 2006 and December 2020 were included. Electronic medical records of all patients who underwent surgery for SEM between November 2006 and December 2020 were retrospectively evaluated for eligibility. Patients were eligible for inclusion when having a surgically treated SEM. Imaging was available for all patients and assessed by a radiologist. All patients had histologically confirmed metastases. Patients with any other pathology than SEMs were not considered eligible. Patients were excluded if insufficient data were available. Medical records and the municipal personal records database were consulted to obtain information regarding death. Demographical, clinical, surgical, and oncological characteristics, as well as imaging data, surgical details, and pathology results were collected.
Variables
Neurological status was categorized using the Frankel Scale and divided into 3 groups: major deficit (grade A, B, and C), minor deficit (grade D), and no deficit (grade E). The general condition was scored with the Karnofsky performance score (KPS). The KPS was divided into 3 groups: poor (≤40), moderate (50–70), and good (80–100). Both the Frankel score and KPS were retrieved based on the clinical condition of the patient as recorded in the medical records at the time of consultation or admission.
For statistical purposes, tumors were divided into 3 groups as suggested by Tomita16: (1) slow growth: breast, thyroid, prostatic, and testicular cancer; (2) moderate growth: renal, uterine, and ovarian cancer; (3) rapid growth: lung, gastric, esophageal, nasopharyngeal, hepatocellular, colorectal, and pancreatic cancer. According to the analysis by Balain et al,14 multiple myeloma and lymphoma were considered as slow-growing tumors and assigned to group 1, and tumors of unknown origin were considered as fast-growing tumors and assigned to group 3.
Spinal instability was assessed using the spinal instability neoplastic score (SINS).30 The score was categorized into: stable (0–6), potentially unstable (7–12), and unstable (13–18).
Complications within 30 days after surgery were graded according to the Clavien-Dindo classification.31 Based on this classification, complications were labeled as minor (grade I and II) or major (grade III, IV, and V), distinguishing between those with minor complications, who were treated with conservative or pharmaceutical treatment (including blood transfusions and parenteral nutrition), and those with major complications, which ranged from requiring surgical treatment to death.
Statistical Methods
Baseline characteristics of the cohort were described as median with range and mean with SD for continuous variables and absolute number and percentage for categorical variables. We calculated the median follow-up time and median survival, both supplemented by 95% confidence intervals. Survival of the cohort was described using Kaplan-Meier estimates.
Development of the Novel Prediction Model
Univariable and multivariable Cox proportional hazards regression were used to test the association between the predictor variables and survival. For multivariable analysis, we used stepwise backward elimination to eliminate variables that were not statistically significant using the Wald test to arrive at a more parsimonious model. The resulting model was internally validated using bootstrap methods to estimate optimism-corrected measures of model performance (ie, estimates of how well the model would perform on new patients not used to develop the model). The proportional hazards assumption was evaluated by computing the scaled Schoenfeld residuals and testing their association with time.
Performance of the model was quantified as the model’s discriminative ability using Harrell’s concordance statistic or c-statistic. The c-statistic can range between 0.5 (indicating no discriminative ability at all) and 1.0 (indicating perfect discriminative ability) and can be interpreted as the proportion of pairs from the dataset in which the patient with the highest predicted survival probability lives the longest.32 Measures of performance were adjusted for optimism, which was estimated by internal validation using bootstrap resampling, with 1000 bootstraps.
All analyses were performed in R version 3.6.1, and a P value of ≤0.05 was considered to indicate statistical significance.
External Validation of Existing Prediction Models
Scores were individually calculated for each patient on the OSRI14 and the modified Bauer score.22 An overview of these models is shown in Supplemental Tables 1 2. In accordance with the original study by Balain et al, the patients with scores of 2 and 3 and those with scores of 4 and 5 were combined into single classes for the OSRI score. Performance parameters were computed similar to those described for our novel model.
Results
General Results
A total of 144 consecutive patients underwent surgical decompression and stabilization for an SEM between November 2006 and December 2020. The median follow-up time was 14.5 months (range 0–176). Fifty-eight percent of the cohort was men (n = 84). The mean age at the time of surgery was 62.7 years (range 28–83). Preoperatively, 31 patients (21.5%) were in a good physical health (KPS 80–100), 80 (55.2%) in moderate condition (KPS 50–70), and 35 (22.9%) patients in poor condition (KPS 30–40). No significant differences in baseline characteristics were observed. All demographic and clinical variables are displayed in Table 1.
Demographic and clinical characteristics (N = 144).
Oncological Characteristics
The most common primary tumor type was breast cancer (n = 28, 19.4%), followed by nonsmall cell lung cancer (n = 26, 18.1%) and multiple myeloma (n = 19, 13.2%) (Table 1).
Surgical Characteristics
The main clinical surgical indications were neurological deficit in 96 patients (66.7%) and pain (radicular or axial) in 45 patients (31.2%). Decompression by laminectomy and partial corpectomy with stabilization by pedicle screw fixation and anterior support with cage was performed in 70 patients (48.6%), decompression by laminectomy with pedicle screw fixation in 63 patients (43.8%), decompression by laminectomy alone in 5 patients (3.5%), and stabilization by pedicle screw fixation alone in 6 patients (4.2%). The median duration of surgery for decompression with laminectomy and partial corpectomy with stabilization was 267 minutes (SD ±88) and for laminectomy with stabilization 210 minutes (SD ±60) (Supplemental Table 3).
The median time between the indication for surgery and the actual operation was 72 hours (4–320). The median score of the SINS was 11 (5–18). Eighty-six patients (59.7%) were classified as potentially unstable, 48 (33.3%) as unstable, and in 10 patients, the spine was considered stable (6.9%) (Table 1). In patients with multiple myeloma (n = 19), the indication for surgery was instability in 8 patients, with a median SINS of 12.3 (9–15). In the remaining 11 patients, the indication was impending neurological deficit.
Neurological Characteristics
Preoperatively, 42 patients (29.2%) had no neurological deficit (Frankel E), 53 (36.8%) had a minor motor or sensory deficit (Frankel D), and 49 patients (34.0%) had a major motor or sensory neurological deficit (Frankel A/B/C). Postoperatively, 26 patients out of 49 (53.1%) improved from Frankel A/B/C to Frankel D (n= 22) or E (n = 4). Seven patients improved from Frankel D to Frankel E.
Eight patients with a Frankel E or D score showed a decline in neurological function postoperatively (5.6%): 6 patients worsened from Frankel D or E to Frankel grade A/B/C, and 2 patients went from Frankel E to D. Ninety patients remained stable in either group A/B/C, D, or E. Total numbers are depicted in Supplemental Table 4.
Ambulatory Status
Preoperatively, 83 patients (57.6%) were ambulant, and 61 patients (42.4%) were nonambulant. This improved to 110 patients (76.4%) who were ambulant postoperatively, and 34 who were nonambulant (23.6%). A total of 7 patients lost ambulatory function from preoperative to postoperative. Patients who were bedridden postoperatively had a significantly poorer survival outcome compared with patients who could mobilize with a median survival of, respectively, 5 vs 18 months (P < 0.0001).
Complications
A total of 55 complications occurred (38.2%). Twenty-two complications were classified as major (15.3%) and 33 complications as minor (22.9%). The most frequent postoperative complications were: deep wound infection, urinary tract infections, and pneumonia. In 50 patients (34.7%), at least 1 complication occurred within 30 days after surgery (Supplemental Table 5). Of those patients, 14 patients had 2 or more complications. In a total of 16 cases (11.1%), a reoperation was needed. Two patients died as a result of a deep wound infection, causing a systemic inflammatory response (1.4%).
Survival
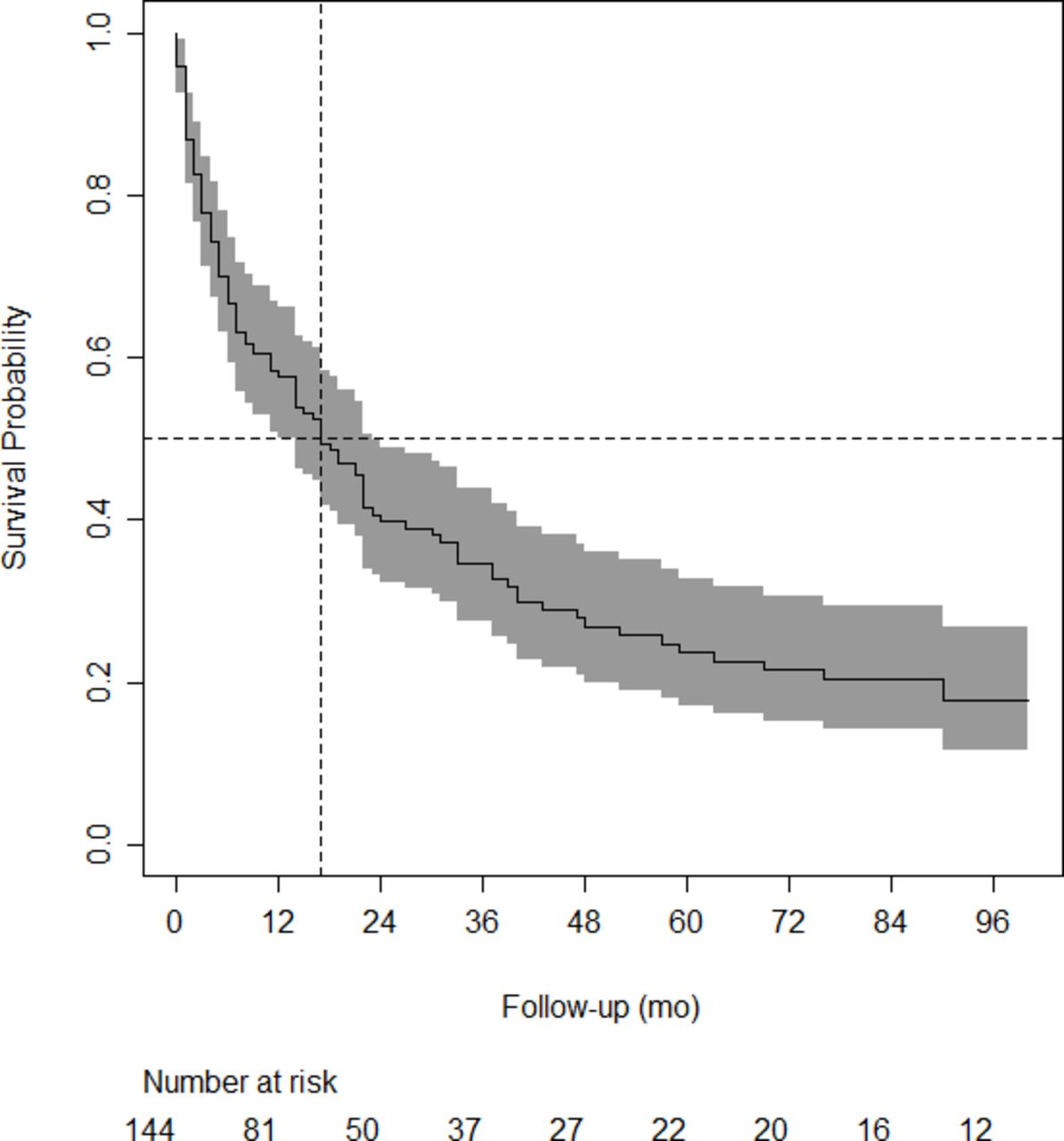
Median survival time was 17 months after surgery (95% CI 11–22 months). Figure 1 shows the Kaplan-Meier curve of our study cohort, with 95% confidence band. The probability of dying within 3 months after surgery was 22.2% (95% CI: 16.3–29.9).
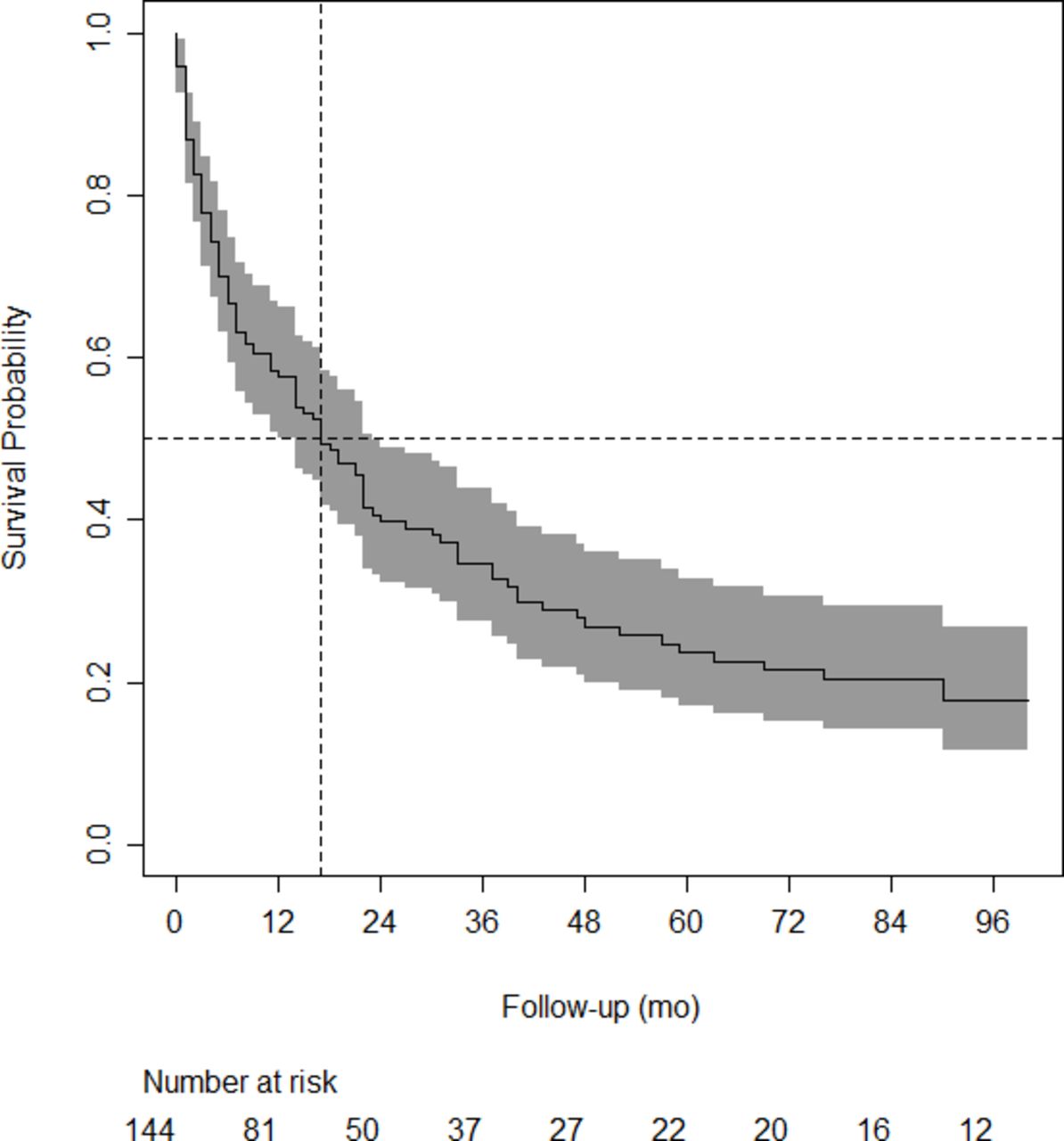
The Kaplan-Meier curve for the whole cohort, with 95% confidence band and median.
Validation Prediction Models
Internal Prediction Model
Univariable analysis shows significant influence on survival of the following preoperative factors: American Society of Anesthesiologists classification, preoperative Frankel score, preoperative KPS, number of spinal metastases, presence of extraspinal bone metastasis, presence of visceral metastasis, and primary tumor growth rate (Supplemental Table 6).
After multivariable analysis, primary tumor growth rate, KPS, presence of visceral metastasis, and presence of multiple spinal metastasis appeared to be independent predictors of decreased survival (Table 2). The scaled Schoenfeld residuals did not show any associations with follow-up time, indicating no evidence of violation of the proportional hazard assumption.
Multivariable Cox regression analysis on the association between predictor variables and decreased survival.
Cumulative risk score predicting the survival probability.
Bootstrap internal validation of the model developed on this cohort yielded an optimism-corrected c-statistic of 0.75 (95% CI: 0.71–0.80). Figure 2 shows a Kaplan-Meier curve stratified by groups based on risk terciles.

The Kaplan-Meier curve stratified by groups based on risk terciles of the newly developed model.
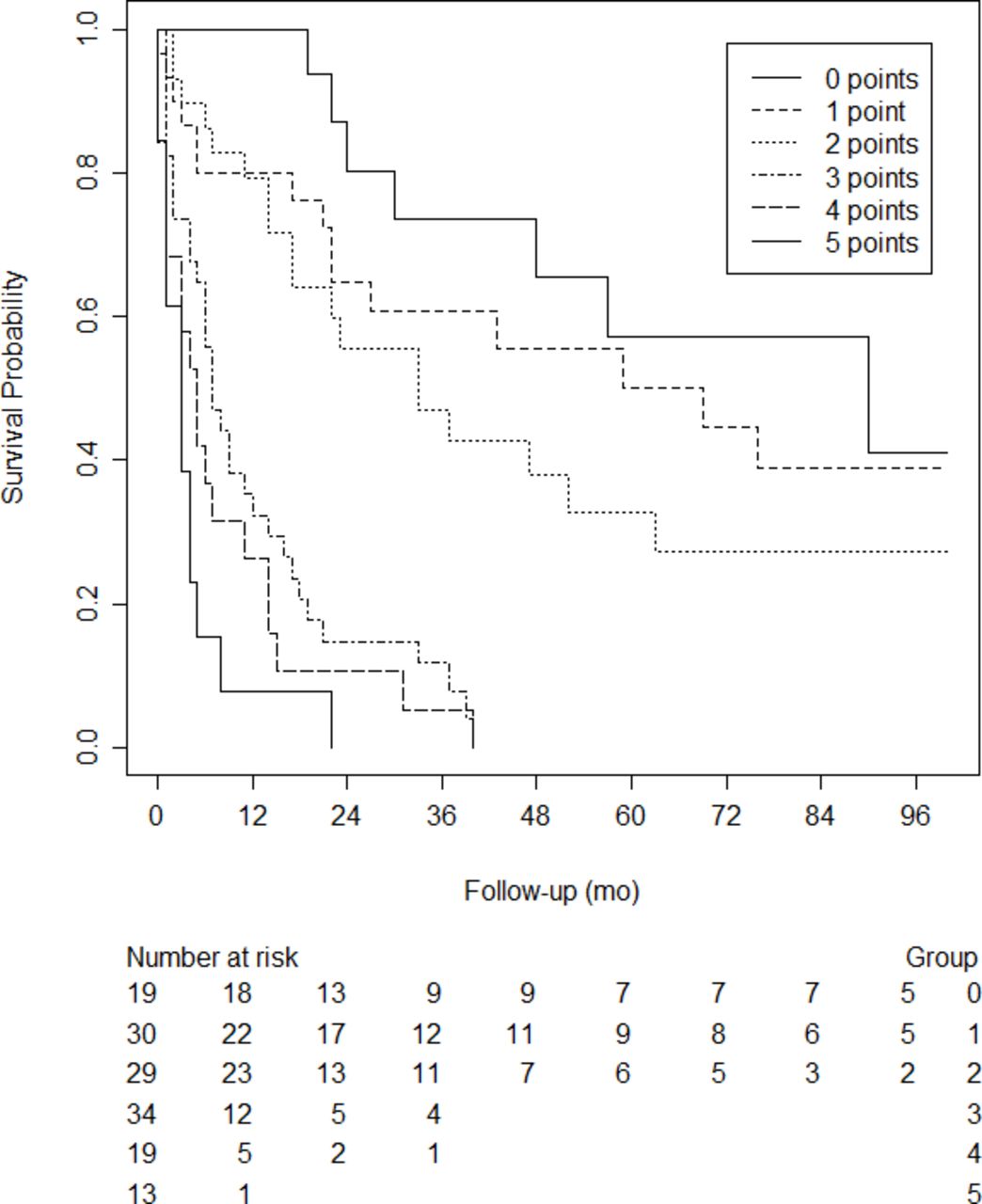
To accommodate easy use of the model, we simplified the regression coefficients by rounding them to the nearest integer (Table 3). This easy-to-use risk score still has a similar optimism-corrected c-statistic of 0.75. Figure 3 shows a Kaplan-Meier curve stratified by the number of points on the simplified risk score. Table 3 displays the predicted probability of survival based on the cumulative risk score at 3, 6, 9, and 12 months.
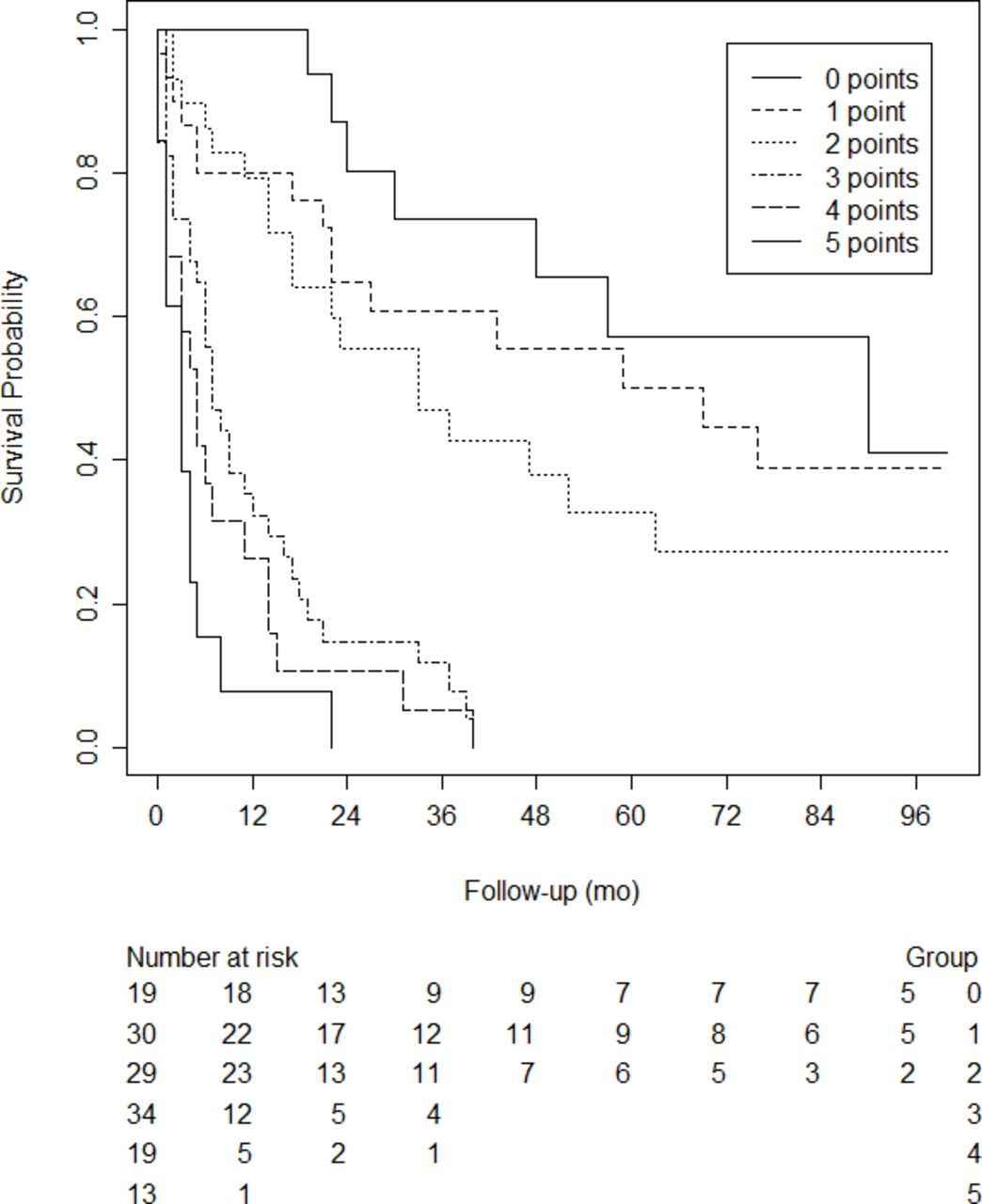
The Kaplan-Meier curve stratified by the number of points on the simplified risk score.
Oswestry Spinal Risk Index
The OSRI score considers primary tumor growth and KPS to estimate survival (Supplemental Table 1). The median OSRI score in our population was 3, ranging from 1 to 7. As suggested by the authors of the original article,14 the OSRI score was categorized into risk groups (ie, OSRI 1, 2/3, 4/5, and 6/7). The number of patients in each group was 20 (13.9%), 65 (45.1%), 35 (24.3%), and 23 (16.1%), for OSRI 1, 2/3, 4/5, or 6/7, respectively. The discriminative ability of the OSRI risk groups, quantified as the c-statistic, was 0.69 (95% CI: 0.64–0.74). Supplemental Figure 1 shows the Kaplan-Meier curve stratified by risk group and the number of patients at risk each year. Additionally, due to the small number of patients for each group, we dichotomized the OSRI score into 1 to 3 and 4 to 7. Supplemental Figure 2 shows the Kaplan-Meier curve for the dichotomized OSRI score. The c-statistic of the dichotomized score was 0.67 (95% CI: 0.62–0.71).
Modified Bauer Score
The modified Bauer score uses the presence of visceral metastases, lung cancer, solitary skeletal metastases, and the primary tumor, originating from breast, kidney, lymphoma, or multiple myeloma to predict survival (Supplemental Table 2). The median score of our population using the model by Bauer et al was 2 points, ranging from 0 to 4. The Bauer score was stratified into risk scores, the number of patients in each group was 36 (25.0%), 46 (31.9%), and 62 (43.1%) for a Bauer score of 0/1, 2, and 3/4, respectively. The c-statistic for the model by Bauer et al, categorized into risk scores, was 0.67 (95% CI: 0.62–0.72). The Kaplan-Meier curve stratified by risk score is shown in Supplemental Figure 3.
Limburg Spinal Metastasis Score
Based on the data obtained from our population, a prediction model was developed, the LSMS. This model contains 4 variables: primary tumor type, KPS, presence of visceral metastases, and presence of multiple spinal metastases. All of these can easily be obtained in routine investigations, which are commonly done in patients presenting with spinal metastases. A score of 0, 1, or 2 is designated to the different variables. The cumulative score ranges from 0 (most favorable survival outcome) to 5 (most unfavorable survival outcome). Internal validation of this model showed a good predictive value.
Discussion
The landmark study by Patchell et al revealed that surgical treatment of SEM followed by radiotherapy improves ambulatory status in comparison with radiotherapy alone, in carefully selected patients.6 Based on their study, it is generally accepted that patients with a poor prognosis (<3 months) can be treated palliatively without surgery, while those with a good-to-moderate prognosis (>3 months) can benefit from surgery.33,34 However, the prediction of survival in these patients is difficult.35 Many prediction models have been developed to assist in decision-making, but none are consistently reliable in the survival prediction of oncologic patients.29 In the present study, a survival analysis was performed. Subsequently, a prediction model was developed, the LSMS, which was compared with the results of 2 commonly used prediction models.
In our population, tumor growth rate, the KPS, presence of visceral metastases, and presence of multiple spinal metastases were independent predictors of survival. The primary tumor pathology is a key variable present in all models evaluated in this study as well in other prediction models.16,17,19,21,36 Several studies have shown the significance of the presence of multiple spine metastasis and visceral metastases on survival.36–40 A recent systematic review of prognostic factors for survival in SEM patients showed an association with these 2 variables; however, the level of evidence was considered inconclusive.41
The use of Karnofsky performance status as a predictor of survival is common in patients with spinal metastatic disease.41,42 As our multivariate analysis showed, the KPS was associated with survival. Interestingly, while performance status is used in several prediction models,14,19,25 other models did not include this variable in their model.16,22 Differences in study population, statistical analysis, or definition of variables may have contributed to these conflicting findings.
External validation of 2 established prediction models was performed. The c-statistic of the OSRI score was 0.69 (95% CI: 0.64–0.74) with 0.67 (95% CI: 0.62–0.71) for the dichotomized variant. For the modified Bauer model, the c-statistic score was 0.67 (95% CI: 0.62–0.72). Kramer et al performed an external validation of several risk scores; they found the modified Bauer and OSRI to be the most accurate predictors of life expectancy in their population, with a c-statistic of 0.66 and 0.70.43 These findings are comparable with those found in our population for these risk scores. The c-statistic of 0.75 of the LSMS thus appears to be very accurate in predicting life expectancy in our population.
It is important to note that the evaluated prediction models are based on different subgroups. Our internal model and the modified Bauer score are based on patients who were selected for surgery, and the OSRI is based on patients treated either surgically, possibly in combination with radiotherapy, or with radiotherapy alone. Therefore, we suggest that our model can be applied for patients who are considered to be surgical candidates. The OSRI model can be used in all patients with SEM.
The New England spinal metastasis score15,44,45 is a relatively new score, taking into account serum albumin as a predictor of survival. Since measuring serum albumin preoperatively is not a standard of care in our center, we could not compare the New England spinal metastasis score with the LSMS in our population. However, it could be argued that the proposed LSMS is more accessible as no additional laboratory measurements are required.
In 2019, Choi et al46 published a risk calculator to predict survival in patients with SEM. This prediction model included the primary tumor, ambulatory status, the presence of visceral metastasis, and the use of analgesics. Internal and external validation were performed. The obtained c-statistic was 0.68. It is a well-funded model, based on a large prospective cohort. However, the number of variables that need to be included is large, thereby decreasing the practical use. In addition, the statistic value is inferior to the model presented in this study.
In our cohort, 55.7% of the immobile patients regained their mobility postoperatively, which is similar to the results of Patchell (62.0%)6 and other studies, with rates ranging from 64.0% to 68.0%.3,47,48 The percentage of patients who regain ambulation after radiotherapy alone is estimated to be 14.0% to 40.0%.49 In another study, surgical patients were 1.3 times more likely to be ambulant after treatment and twice as likely to regain ambulation.50
This study includes multiple myeloma patients, but it could be argued they should be excluded because of their radiosensitive nature and longer overall survival.6 However, as this study specifically included patients with SEM and a surgical indication due to neurological impairment or instability, we deemed it relevant to include this group.51 Moreover, the publication by Leithner et al22 showed the difference in predicted survival, according to different scoring systems, to be equal when including or excluding multiple myeloma patients.
Despite not being included in the study by Patchell, surgery for metastatic disease of the lumbar spine with epidural compression is indicated in patients with neurological symptoms, pain, and/or instability.3 In our cohort, 11 patients with lumbar metastatic epidural compression were evaluated. The indication was instability in 5 patients (median SINS 11) and neurological symptoms in 6 patients.
The overall 30-day postoperative complication rate in the present study was 38.2%, with major complications in 15.3% of the patients. In the literature, similar numbers (13%–27%) are presented.9,11,52,53
This study has several limitations, including its retrospective nature. Furthermore, only surgically treated patients were evaluated; patients who were deemed unfit for surgery were not included for analysis. In addition, inclusion started in 2006. Oncologic treatment, immunotherapy especially, has evolved in recent decades with a significant impact on survival. However, the initial data collection was conducted until 2017, and later data collection was completed until 2020. The addition of data from patients treated in the last years did not significantly alter the outcomes. Therefore, we believe our findings are representative and are not altered too much by the inclusion of older data. It should be noted that the LSMS estimates 100% 1-year survival in those with a score of 0, this may differ in practice. The estimated survival rate is close in those with an LSMS score of 1 or 2. This can be explained by the low number of deaths in these groups, indicated by the wide 95% confidence intervals. It might thus be difficult to differentiate the survival probability in those with a score of 1 or 2. However, the predicted survival probability is more evident in those with an LSMS score higher than 2. Moreover, the proposed LSMS is not externally validated to determine its value in other patient populations.
Needless to say, prediction of survival is not the only measure to determine whether a patient is a suitable candidate for surgery. Specific patient factors and patient and/or family preferences must also be considered in the decision-making process.
Conclusion
Predicting in which patients with SEM the benefits of surgery will outweigh the morbidity is a challenge. Survival prediction models can assist in the surgical decision-making process. Based on the survival analysis of our cohort, we developed the LSMS to aid in predicting the oncological prognosis of surgical candidates. The prediction model is practical in use and appears to have a better predictive value in surgical candidates in comparison with previous models.
Supplementary material
TABLE S1.
TABLE S2.
TABLE S3.
TABLE S4.
TABLE S5.
TABLE S6.
FIGURE S1.
FIGURE S2.
FIGURE S3.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was approved by the Medical Ethical Committee (METC 2018-0602 and Z2021079) and was conducted according to principles enshrined in the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act (WMO).
Data Availability Statement The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.