


Abstract
Background Although interspinous and supraspinous ligaments of the lumbar spine are thought to contribute to spinal stability, little is known about their dynamic biomechanics. We demonstrate that shear wave elastography (SWE) offers a novel technique to noninvasively and quantitatively evaluate posterior spinous ligament complex functional loading and stiffness in different physiologic positions.
Methods We performed SWE and measured the length of the interspinous/supraspinous ligament complex in cadaveric torsos (N = 5), isolated ligaments (N = 10), and healthy volunteers (N = 9) to obtain length and shear wave velocity measurements. For cadavers and volunteers, SWE was utilized in 2 lumbar positions: lumbar spine flexion and extension. In addition, SWE was performed on isolated ligaments undergoing uniaxial tension to correlate shear wave velocities with experienced load.
Results Average shear wave velocity in cadaveric supraspinous/interspinous ligament complexes increased for lumbar levels (23%–43%) and most thoracic levels (0%–50%). This corresponded to an average increase in interspinous distance from extension to flexion for the lumbar spine (19%–63%) and thoracic spine (3%–8%). Volunteer spines also demonstrated an average increase in shear wave velocity from extension to flexion for both the lumbar spine (195% at L2-L3 to 200% at L4-L5) and thoracic spine (31% at T10-T11). There was an average increase in interspinous distance from extension to flexion for the lumbar spine (93% at L2-L3 to 127% at L4-L5) and thoracic spine (11% at T10-T11). In isolated ligaments, there was a positive correlation between applied tensile load and average shear wave velocity.
Conclusion This study creates a foundation to apply SWE as a noninvasive tool for assessing the mechanical stiffness of posterior ligamentous structures and has potential applications in augmenting or evaluating these ligaments in patients with spine pathology.
Clinical Relevance The interspinous and supraspinous ligaments are critical soft tissue supports of the posterior lumbar spine. Disruption of these structures is thought to have a negative impact on spinal stability in trauma and spine deformities.
Level of Evidence 4.
- shear wave elastography
- ultrasound
- spine
- ligament
- biomechanics
- interspinous
- supraspinous
- stiffness
- scoliosis
- proximal junctional kyphosis
Introduction
As spine surgery evolves with the goal of optimizing function, an improved understanding of the soft tissue supports may offer new opportunities for novel surgical interventions. Chief among the soft tissue supports at the posterior lumbar spine are the interspinous and supraspinous ligaments. Disruptions of these ligamentous structures are thought to have consequences for spinal stability in trauma,1 scoliosis,1–3 and degenerative disease.4–6
To better understand its role in healthy, injured, and pathologic states, the posterior thoracolumbar ligamentous complex has been well studied in cadaveric specimens to assess mechanical properties.5–15 However, it is well accepted that cadaveric tests often do not fully replicate in vivo function of tissues,16–18 and for this structure, very little is known about its dynamic, physiologic biomechanics.
To address this, we evaluated the ability of shear wave elastography (SWE) to noninvasively assess changes in the supraspinous/interspinous ligament complex under tension in physiological positions.3,19–37 In this technique, shear waves are generated in the ligamentous complex by an ultrasound probe placed on the skin above the spinous process interspaces. The ultrasound calculates a velocity map of these waves, proportional to the stiffness of the observed tissues.
For application to the spine, when ligaments of the posterior structures are in flexion, they are under more tension, stiffening the ligaments. Thus, we hypothesized that shear wave velocity (SWV) measurements would be higher when the spine is in flexion and increased tension than in extension and less tension. We tested this in cadaveric specimens, isolated ligaments, and healthy volunteers as a pilot study for future assessment of the dynamics of posterior ligamentous spine structures in living patients.
Methods
Institutional Review Board (HSS IRB #2016–0071) approval was obtained for the cadaveric specimen portion of this study. Institutional Review Board (HSS IRB #2021–0997) approval was obtained to perform shear wave ultrasonography on healthy volunteers.
Given that there was no prior literature on SWE velocity changes in the supraspinous/interspinous ligament complexes during spine positional changes, we used prior data from SWE velocity changes in similarly loaded soft tissue of the ankle to estimate our sample size.26 To detect an effect size of 1.37 with an SD of 1.6 m/s at an alpha of 0.05 and power of 0.8 using a paired t test analysis, we would need 5 subjects.
Thus, for this study, 5 fresh frozen cadavers, 9 healthy volunteers, and 10 isolated thoracolumbar ligament complexes (5 L4-L5 and 5 L2-L3 complexes) were measured using the following SWE methods. Nine ligament levels were measured in each cadaver, resulting in 45 ligament samples. Four ligament levels were measured in each volunteer, except for 2 volunteers with 3 measured levels, resulting in 34 volunteer ligament samples.
Five fresh frozen cadaveric torsos amputated at the distal femur were placed in 2 positions (Figure 1). The specimens were placed prone, first in a hip extension/lumbar spine extension position (Figure 1A) and second in a hip flexion/lumbar spine flexion position (Figure 1B). Ultrasound and SWE measurements were made using a LOGIQ E9 Ultrasound system with a 9-MHz linear transducer (GE Healthcare, Milwaukee, WI). The dorsal interspinous ligaments at each spinous interspace were identified via ultrasound guidance by counting spinous processes moving proximally from the sacrum. For measurements, the transducer was coated with ultrasound gel and placed lightly on the skin surface in a longitudinal direction along the ligaments. The SWE region of interest was set in the supraspinous/interspinous ligament region (Figure 2). A single operator obtained triplicate SWV measurements, and images were taken at each posterior ligament complex from T9 to S1 in each cadaver. Images were saved and stored in an electronic repository for further analysis, including distance measurements between spinous processes at each level. SWV and interspace distance measurements at each level were obtained in lumbar spine extension and flexion positions to compare different magnitudes of tensile force through the thoracolumbar ligaments.

The cadaveric torso and volutneers assumed two positions: (A) lumbar extension/hip extension and (B) lumbar flexion/hip flexion.

Representative images showing visualization of the interspinous and supraspinous ligaments with superimposed anatomic labeling (A) and example shear wave velocity measurements using a region of interest within the interspinous ligament region in extension (B) and flexion (C).
SWE was performed similarly on healthy volunteers, with the exception that measurements were only taken at selected levels: T10-T11, T12-L1, L2-L3, and L4-L5. For these experiments, the measurements were performed by an musculoskeletal attending radiologist who specializes in ultrasonography.
To confirm that SWV measurements were proportional to tensile load across the interspinous/supraspinous ligament complexes, complexes from levels L2-L3 and L4-L5 were isolated. After removal, the facet joints, remaining capsule and anterior posterior soft tissue of each ligament complex were disrupted so that applied loads were directed solely through the interspinous ligaments during mechanical testing.
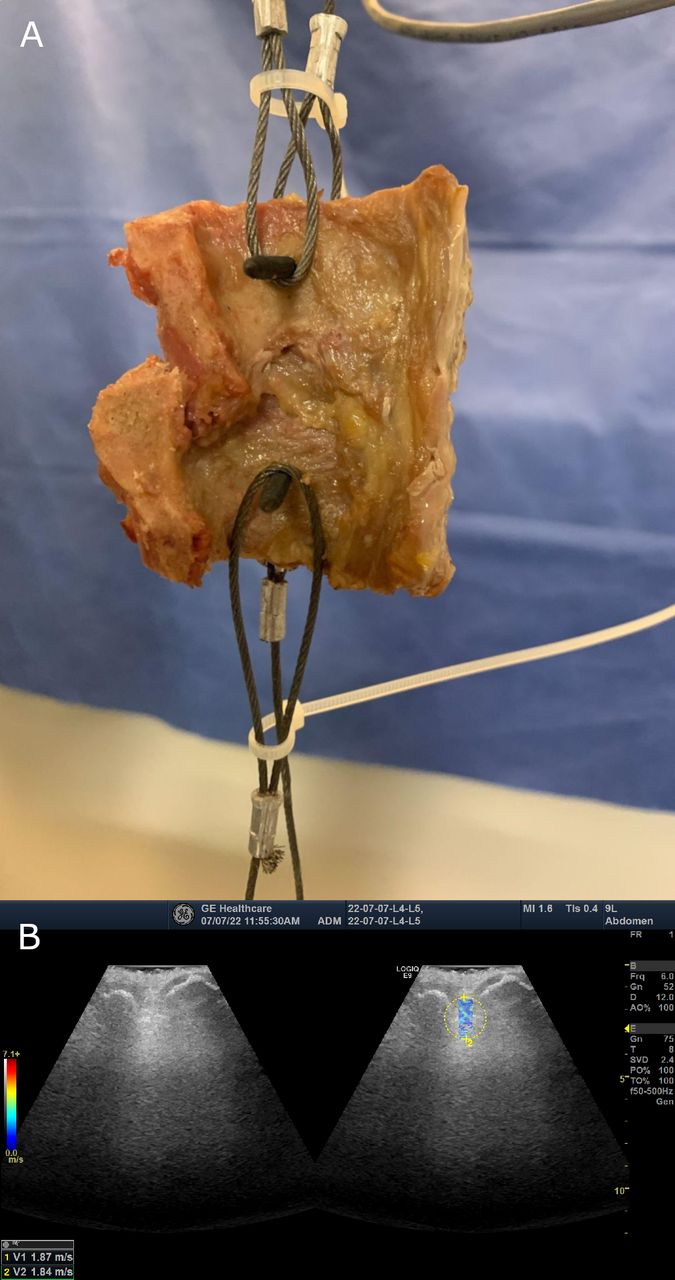
To control the magnitude of force exerted through a ligament complex and control for viscoelastic relaxation, we performed SWE velocity measurements in a load-controlled regime using an Instron material testing system (Instron, Norwood, MA) with a 25-lb load cell. After generating constant tension across the specimen, we then measured the SWV at known loads (Figure 3A and B). Before applying load, the distance between the spinous processes was measured using digital calipers to obtain a baseline length of the interspinous ligaments. The ligament complex was then preconditioned by loading the sample to 5% strain at a strain rate of 0.05 /s. Following preconditioning, the sample was loaded to 10 N at a rate of 0.5 N/s to minimize viscous effects, which resulted in quasistatic strain rates significantly lower than 0.5 /s for each sample.8 The ultrasound operator lightly placed the gel-coated transducer to the interspinous/supraspinous ligament complex and obtained 3 SWV measurements at 10 N. The process was then repeated at 20 N increments up to a maximum of 90 N. The sample was sprayed with phosphate-buffered saline between each load increment to prevent the sample from drying during testing.

Shear wave velocity measurement of excised interspinous ligaments. (A) Tensile testing setup. Shown are no. 8 drywall screws driven through the spinous processes bordering the interspinous ligament and k-wires were used to connect the screws with the tensile tester. (B) Example shear wave image of a ligament pulled by the tensile device.
Statistical Methods
SWVs for cadaveric specimens were compared between physiologic extension and flexion using paired 2-sample t tests for means to control for physiologic differences between cadavers. Volunteer data were similarly analyzed using paired t tests to analyze the difference between extension and flexion SWVs for levels T10-T11, T12-L1, L2-L3, and L4-L5. Linear slope regression was performed on data for isolated L2-L3 and L4-L5 ligaments to obtain the relationship between load and SWV.
Power analysis was performed using G*Power 3.1 (Heinrich Heine University, Düsseldorf, Germany) to determine the number of ligament samples from cadavers and volunteers to achieve statistical power of 0.8 with an alpha of 0.05.
Results
In intact cadaveric torsos, changing position from lumbar extension to lumbar flexion (Figure 1) increased the interspinous distances from T9 to the pelvis (Table 1). The thoracic region had smaller, nonsignificant increases in interspinous distance, ranging from 3% (P > 0.05) to 8% (P > 0.05). The lumbar interspinous distances had greater change in interspinous distances from extension to flexion, ranging from 19% (P < 0.01) to 63% (P < 0.01). The smallest difference was found at the L1-L2 level, and the largest difference was found at the L3-L4 level. There was an intermediate increase in interspinous distance from extension to flexion of 27% at the thoracolumbar junction, level T12-L1 (P < 0.01).
Average distances, in cm, between spinous processes at interspaces for 5 cadavers (n = 5) in physiologic extension and flexion positions, with relative percent increases. The designated percent increase was calculated by a paired methodology whereby the increase was calculated in a single ligament moving from flexion to extention prior to being averaged.
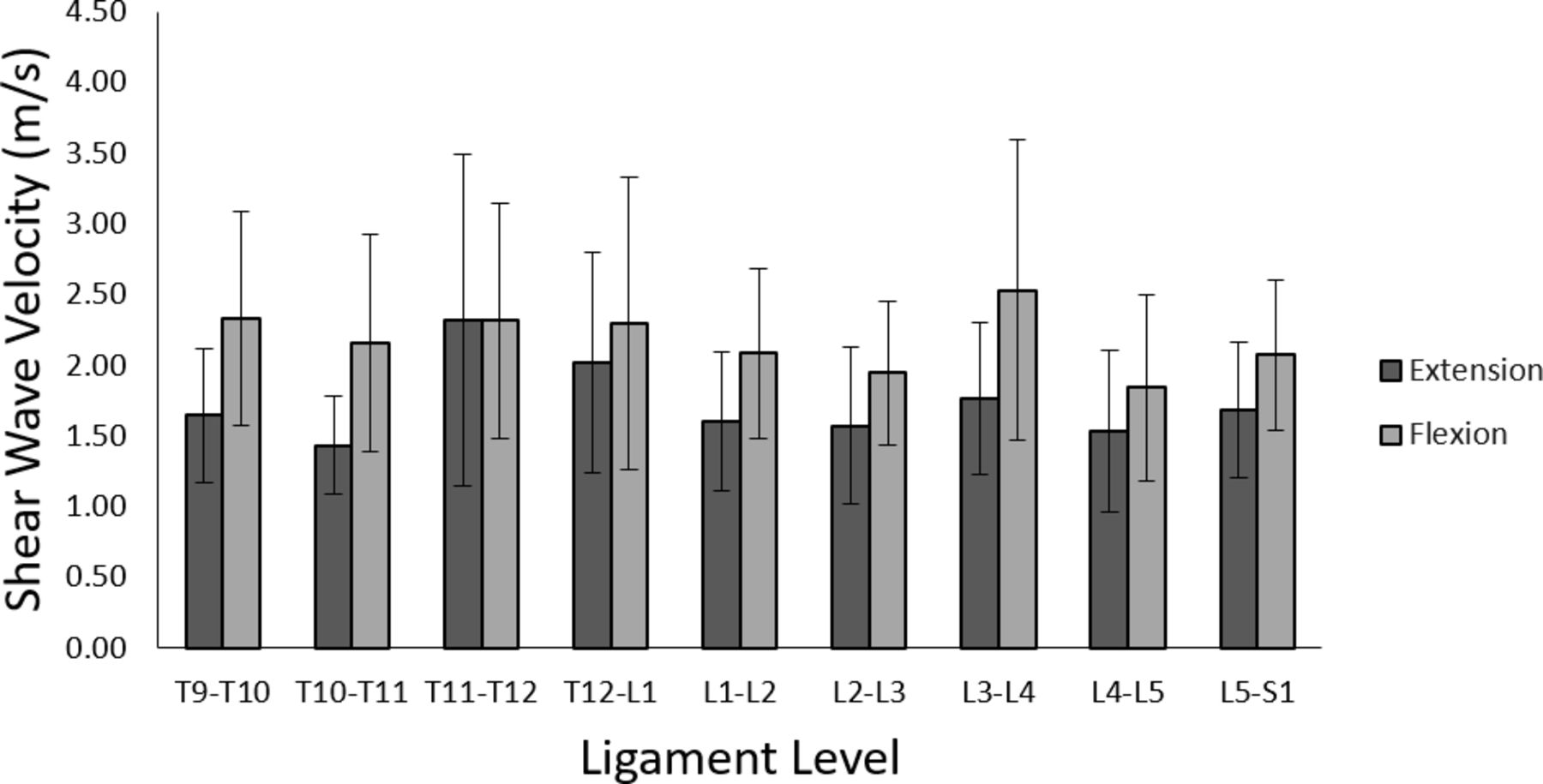
Average SWVs in flexion exceeded those in extension when aggregated for all cadavers (Figure 4), but these differences were not statistically significant because of the large variability between cadavers. However, when analyzed in paired methodology, whereby the SWV measures were compared for a single cadaver and paired t test performed, there was a difference in SWVs found for all levels (P < 0.01) except the T11-T12 level (P > 0.05). The greatest SWV change was 51%, increasing from an average of 1.43 to 2.16 m/s, at the T10-T11 level (P < 0.01). Figure 5 shows SWVs for selected cadaveric interspaces T10-T11, T12-L1, L2-L3, and L4-L5.

Aggregate shear wave velocities of all tested cadavers (N = 5), separated by ligament level. Error bars indicate standard deviations of measurements.

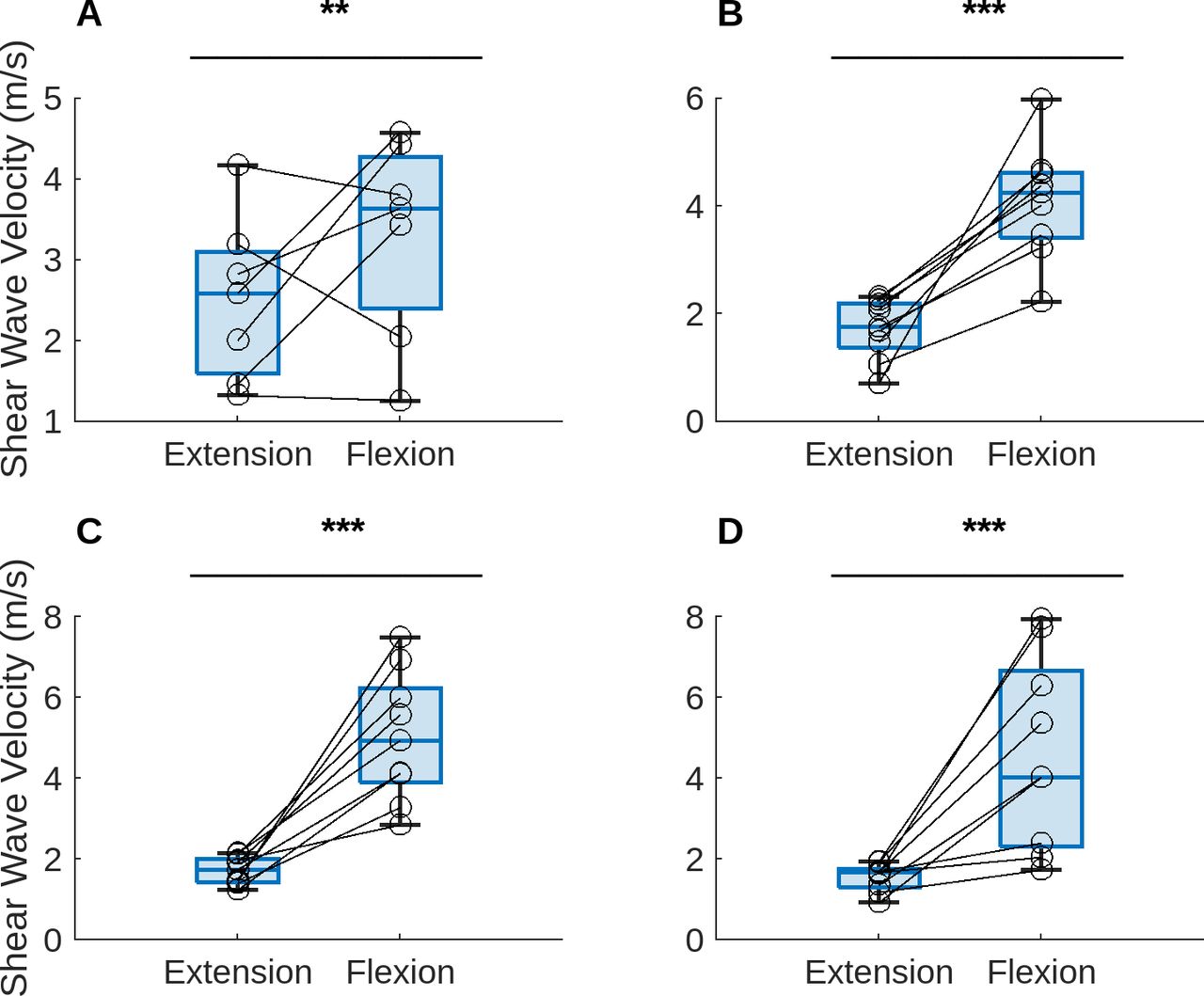
Shear wave velocities obtained from cadavers (N = 4 or 5), separated into ligament levels T10-T11 (A), T12-L1 (B), L2-L3 (C), and L4-L5 (D). To perform a paired t test, each extension velocity was paired with the flexion velocity from the same cadaver. *P < 0.05, **P < 0.01, ***P < 0.001.
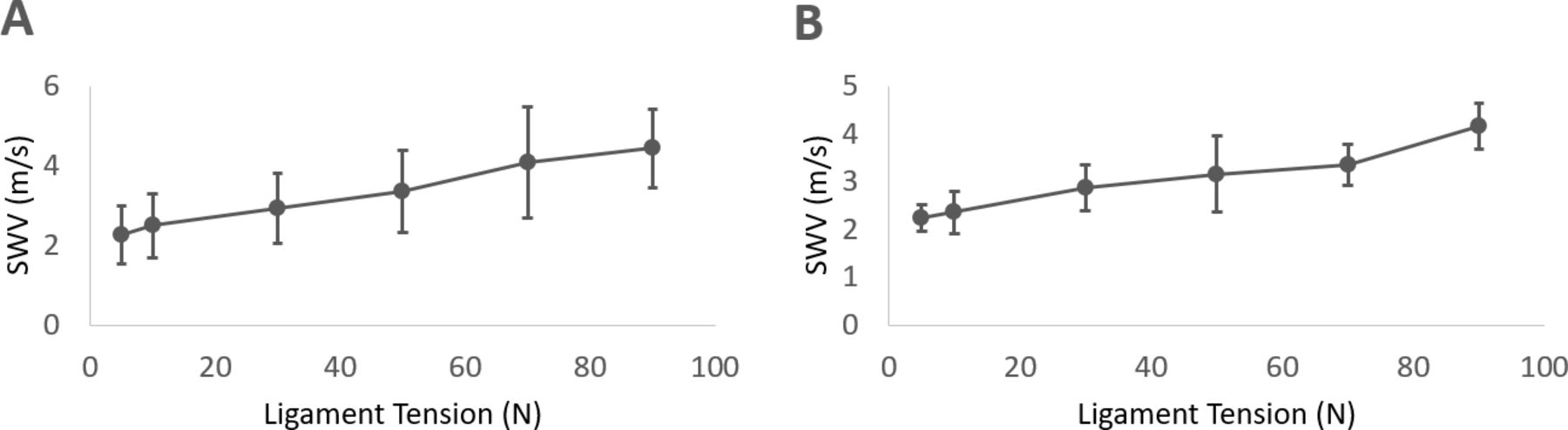
In isolated ligament complexes from L2 to L3 and L4 to L5, where tension was applied at specified loads, there was a positive correlation between tensile load and average SWV (Figure 6, Table 2). For the L2-L3 level, increasing the load applied across the ligament complex from 5 to 90 N increased the average SWV from 2.26 ± 0.73 to 4.43 ± 0.98 m/s (P < 0.01). Similarly, for the L4-L5 level, increasing the load from 5 to 90 N across the ligament structure increased the average SWV from 2.23 ± 0.28 to 4.15 ± 0.48 m/s (P < 0.01). For each increment of increased load, there was an increased average SWV (Table 2). Linear regression of the SWV and load plot (Figure 6) demonstrated a positive correlation between load applied over the ligament and SWV (Table 2).

Aggregate shear wave velocity (SWV) values of excised L2-L3 (A) and L4-L5 (B) interspinous ligaments from all cadavers, dependent on load exerted on the ligament at the time the shear wave measurement was made. Error bars indicate standard deviations of measurements.
Regression P values and 95% confidence intervals for the relationship between shear wave velocity and load for levels L2-L3 and L4-L5.
For healthy volunteers, changing position from physiologic lumbar extension to lumbar flexion (Figure 1) increased the interspinous distances in levels T12-L1, L2-L3, and L4-L5 (Table 3, P < 0.01). The increase in interspinous distance ranged from 127% at L4-L5 to 58% at T11-L1, decreasing with more proximal interspinous levels. The interspinous distance at level T10-T11 did not increase significantly from extension to flexion (P > 0.05).
Collected SWV data from volunteer subjects, including interspinous distances in physiologic extension and flexion, percent increase between the positions, and SWV in both positions.
Also for healthy volunteers, there was a significant increase in SWV from extension to flexion at all measured levels (Figure 7, P < 0.01). On average, the increase in SWV was most pronounced at the L4-L5 level, whereby the average increase in SWV was 200% from 1.53 ± 0.37 m/s in extension to 4.59 ± 2.31 m/s in flexion (P < 0.001). The T10-T11 level had the lowest increase in SWV at 31% from 2.50 ± 0.97 m/s in extension to 3.28 ± 1.20 m/s in flexion (P < 0.01).

Shear wave velocities obtained from volunteer subjects (N = 7 or 9), separated into ligament levels T10-T11 (A), T12-L1 (B), L2-L3 (C), and L4-L5 (D). To perform a paired t test, each extension velocity was paired with the flexion velocity from the same volunteer to account for physiologic differences between volunteers. *P < 0.05, **P < 0.01, ***P < 0.001.
Discussion
These results show that SWE can quantitatively detect changes in applied load in the supraspinous/interspinous ligament complex of the thoracolumbar spine. In this work, SWVs were higher in flexion and, similarly, increased with higher tensile loads applied through the ligament. The use of SWE has been broadly explored for its utility in musculoskeletal health, although there are few studies where it is explored in the spine. In Chen et al, the authors examined the SWV of the thoracolumbar fascia and found that stiffness of the thoracolumbar fascia can be determined reliably using shear wave ultrasonography.20 Our pilot cadaveric study performed at multiple levels in the thoracolumbar spine shows that ultrasound can distinguish spinous processes and visualize the interspinous ligament/supraspinous ligament complex to obtain SWV measurements. These results add to current literature on the feasibility of SWE for evaluating ligament stiffness for spine applications.
In this study, once the interspinous/supraspinous ligament complex was isolated, increased tensile loads applied across the structure correlated with higher SWVs. Prior studies have reported a dose-dependent change in SWV with tension across tendon and muscle in other nonspine structures.3,19–37 For clinical applications, this study indicates that greater tension in the spine from lumbar flexion will result in relatively high measured SWVs compared with lumbar extension in healthy, functioning ligament complexes. The reduced velocities measured in the thoracolumbar ligaments while in physiologic extension are likely due to reduced tensile loads not compressive loads; in physiologic lumbar extension, the interspinous and supraspinous ligaments are under relatively low tension, but the ligament does not have redundancy and is not under compression.11 Additional studies may explore how the relationship between SWV and tension is affected in pathologic or traumatized tissue.
We found a larger difference in SWVs between flexion and extension positions in healthy volunteers compared with cadavers. One possible cause of this effect is that freezing cycles reduced the stiffness response of the thoracolumbar ligaments during stretch. In addition, the amount of lumbar positional change being transmitted by placing only the cadaveric hips in flexion vs extension is likely less than a healthy volunteer with completely intact limbs activating their muscles to change position. In either case, it is advantageous that SWVs in live volunteers show a clear distinction between flexion and extension states for clinical applications of this technique. This work sets a foundation for understanding normative SWE velocities and ligament stiffnesses for healthy spines. It also will allow investigation of pathological states, as many believe this ligament complex plays a critical role in preserving stability in thoracolumbar trauma,38 prevention of proximal junctional kyphosis,1,39,40 and spondylolisthesis.41–45 Understanding more about how these ligaments tolerate loads may lead to improvements in treatments and improved design of spinal implants that preserve motion while reducing pathologic instability.
Limitations in the design of this study included the small number of cadavers and volunteers used. Because of this, we could not propose a normative range of SWE thoracolumbar ligament stiffness, and we expect there will be individual variation across patients. However, the presented data show that higher tensile forces in lumbar flexion, relative to extension, increase SWV within individual patients. As a result, this tool shows promise in its ability to compare changes in SWV as a biomechanical marker of ligament health compared with absolute SWV measures. Our SWE velocity measurements were also limited in that they did not directly take into account time-dependent or viscoelastic properties of the ligaments. Instead, our initial results presented here were designed to hold ligaments at a constant load in tension.8,46–48 Future studies could explore beyond these static load measurements by characterizing the ability of SWE to measure time-dependent relaxation and utilizing SWE to detect the response of ligaments to compressive or torsional strains. These types of loads would more closely resemble physiologic function of these ligaments in vivo. Future work could also investigate the ligaments’ spatially dependent response to tension; superficial portions of the thoracolumbar ligament complex would likely be under increased tension from lumbar flexion compared with deeper portions, resulting in gradients of SWVs throughout a single ligament complex.
Although we had a single musculoskeletal attending radiologist specialized in ultrasonography perform all SWV and length measurements in the healthy volunteer experiments, we did not have access to multiple radiologists and, thus, cannot estimate interoperator reliability for this study. However, prior studies have shown that inter- and intraoperator reliability are high when performing shear wave ultrasonography on soft tissues.19,20,28 Another weakness is that our SWE measurement technique included both interspinous and supraspinous ligaments and did not distinguish between these 2 structures. We plan to expand upon these initial studies to address these limitations in future work.
Conclusion
SWE may be used as a noninvasive technique to quantitatively measure the stiffness across the interspinous/supraspinous ligament complex. This opens up possibilities for real-time and dynamic functional evaluation of loads across ligaments not afforded by conventional imaging techniques. As spine surgery progresses and addresses motion-preserving techniques requiring dynamic soft tissue supports, understanding the function of these soft tissue supports in healthy and pathologic spines will become increasingly important. These data support the development of SWE as a valuable tool in these investigations.
Acknowledgments
We thank Dr. Suzanne Maher and Kate Meyers for their assistance in our study design and mechanical testing.
Footnotes
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Sariah Khormaee reports unpaid leadership roles for Enuval (Co-Director) and Surgical Implant Generation Network (Committee Member) and stock ownership in Merck and Novo Nordisk. The remaining authors have nothing to report.
Institutional Review Board Institutional Review Board (HSS IRB #2016-0071) approval was obtained, and informed consent was exempted for this pilot study due to the use of cadaveric specimens. Institutional Review Board (HSS IRB #2021-0997) approval was obtained to perform shear wave ultrasonography on healthy volunteers.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.