


Abstract
Background This is a multicenter observational registry analysis of 1-year radiographic and clinical outcomes following anterior cervical discectomy and fusion (ACDF) using hydroxyapatite (HA)-infused polyetheretherketone (PEEK) intervertebral cages.
Methods Radiographic and clinical outcome data were collected preoperatively and at 6 weeks, 3 months, 6 months, and 12 months postoperatively. To assess fusion, dynamic flexion-extension radiographs were independently evaluated with a validated method. Clinical outcomes were assessed using the following disease-specific measures: Neck Disability Index (NDI) and visual analog scale (VAS) for neck, left arm, and right arm pain. Patient satisfaction was also evaluated.
Results A total of 789 ACDF patients (men: 51.5%/women: 48.5%; mean body mass index: 29.9 kg/m2) were included at the time of analysis, and 1565 segments have been operated. Successful fusion was confirmed in 91.3% of all operated levels after 6 months and 92.2% after 12 months. Mean NDI scores improved significantly (P < 0.01) preoperatively (46.3, n = 771) to postoperatively (12 months: 25.2, n = 281). Consistently, mean VAS neck (preoperative: 64.2, n = 770; 12 months: 28.6, n = 278), VAS right arm (preoperative: 42.6, n = 766; 12 months: 20.4, n = 277), and VAS left arm (preoperative: 41.1, n = 768; 12 months: 20.8, n = 277) decreased significantly (P < 0.01). Patients reported high satisfaction rates after surgery with no significant changes in postoperative patient satisfaction between 6 weeks and 12 months (95.1%, n = 273).
Conclusions ACDF with HA-infused PEEK cages demonstrates promising radiographic and clinical outcomes, supporting the potential benefits of incorporating HA into PEEK cages to enhance fusion rates and improve patient outcomes.
Clinical Relevance This study demonstrates a >90% fusion rate by level with reliable improvements in patient reported outcomes, along with a high rate of patient satisfaction, in a large patient cohort undergoing ACDF with HA-infused PEEK cages.
Level of Evidence 2 .
Introduction
Anterior cervical discectomy and fusion (ACDF) is a standard procedure for the surgical treatment of degenerative pathologies of the cervical spine. The use of intervertebral implants (ie, interbody cages) is a well-established technique for achieving the goals of ACDF, decompression of neural structures, restoration and preservation of intervertebral disc height, and fusion at the operated segment or segments.1,2 However, as material technology has advanced, there are limited data on the superiority of any particular material. Thus, novel implant materials have become the subject of increasing interest for potentially improving radiographic and clinical outcomes in cervical fusion but have thus far lacked rigorous scientific evaluation on large, real-world scales.
Historically, implants in ACDF have undergone intensive development in attempts to optimize fusion. The concept of using an interbody cage device was first proposed in the 1980s using a stainless steel implant.3 While the design of interbody implants has since been largely consolidated to hollow, wedge-shaped cages to allow for graft packing,1,2,4–6 discordance regarding optimal cage material and surface characteristics remains in the literature and the spine community at large.7 Today, titanium and polyetheretherketone (PEEK) are among the most frequently employed implant materials in ACDF interbody cages.6,8,9 Titanium and its alloys, on the one hand, are osteoconductive and thus facilitate the formation of the bone-implant interface.10 However, there remains a well-documented limitation of titanium: its relatively large difference in modulus of elasticity when compared with both trabecular and cortical bones, which may ultimately manifest as cage subsidence.11 Subsidence unfortunately is not solely a radiographic issue as it is proposed to contribute to long-term loss of segmental and global lordosis.12 Furthermore, titanium (a metal) is radiodense, complicating the use of postoperative imaging for diagnosis of complications or assessment of fusion. To improve upon the limitations of titanium, PEEK implants found increasing application in cervical fusion procedures starting in the 1990s. While PEEK indeed shares a more similar elastic modulus to bone, which may contribute to lower stress shielding, bone remodeling, and subsidence, it too is not without limitations.11 As a hydrophobic polymer, PEEK has been associated with poor bone-implant interfacing due to the proposed attenuation of osteoblast differentiation and proliferation and an associated proinflammatory response at the implant site.7,13–15 Often described in the literature is the so-called “PEEK-halo effect,” where gaps between bone and implant material indicate poor surface osseointegration.16–18 In extreme cases, this has been postulated to be a cause of implant failure.7 Hence, there remains a need to improve the osseointegration of PEEK implants while also taking advantage of its superior biomechanical properties.
Enhancing PEEK implants with bioactive, osteoconductive materials such as hydroxyapatite (HA) has gained attention as a strategy to overcome its previously discussed limitations. HA is an osteoconductive, radiolucent, ceramic biomaterial that makes up 70% of human calcified bone.19,20 Surface hydrophilicity, increased cell attachment and proliferation, and affinity for multiple bone growth factors are noteworthy advantages of this combination, with animal studies and clinical evidence demonstrating improved bone formation in HA-PEEK composite implants over traditional PEEK implants.16,20–23 Additionally, other subspecialties of orthopedics have begun employing HA-augmented implant components, including total hip arthroplasty (THA) and external fixator half pins. Evidence exists in these domains with varying degrees of support for HA. Clauss et al, for example, demonstrated a 5-year THA femoral stem survival rate of >98% with low rates of subsidence with HA-coated stems.21 Conversely, Tyagi et al noted no significant difference between HA-coated and conventional femoral stems.22 In the use of external fixator half pins composed of HA, studies empirically confirm the theoretical advantages of HA, such as improved bone-implant interface, but lack sufficient data to back their wide-scale application.23,24 HA-PEEK specifically has thus far found purpose primarily in nonspine applications, particularly in dentistry, where osseointegration of implants is key to surgical success.25 To date, the study of HA-PEEK spinal interbody cages has been limited to small patient cohorts.26–28 Radiographic and clinical efficacy in large patient cohorts undergoing spine surgery have not been reported in the literature to date.
Therefore, the purpose of the current study is to present an interim report of the radiographic and clinical outcomes of patients undergoing ACDF using HA-infused PEEK implants with data from a large, multicenter, prospective observational patient cohort. We hypothesized that HA-infused PEEK implants would be safe and effective implants in facilitating interbody fusion.
Methods
Materials
This study represents a large radiographic and clinical evaluation of patients undergoing ACDF with HA-infused PEEK interbody cages using data collected from a “Biobase Registry.” The registry is composed of patients from a large, growing, multicenter, observational cohort. Patient enrollment into the registry began in 2018; today, the registry contains data from 789 operated patients at varying stages of follow-up from 20 US-based clinical sites. The registry aims to obtain unbiased, generalizable data from a diverse group of patients undergoing surgical procedures for a host of cervical conditions. Thus, inclusion criteria are any cervical spine fusion surgery involving HA-PEEK interbody cage, including, for instance, degenerative disc diseases, radiculopathy, and myelopathy.
Surgical Technique
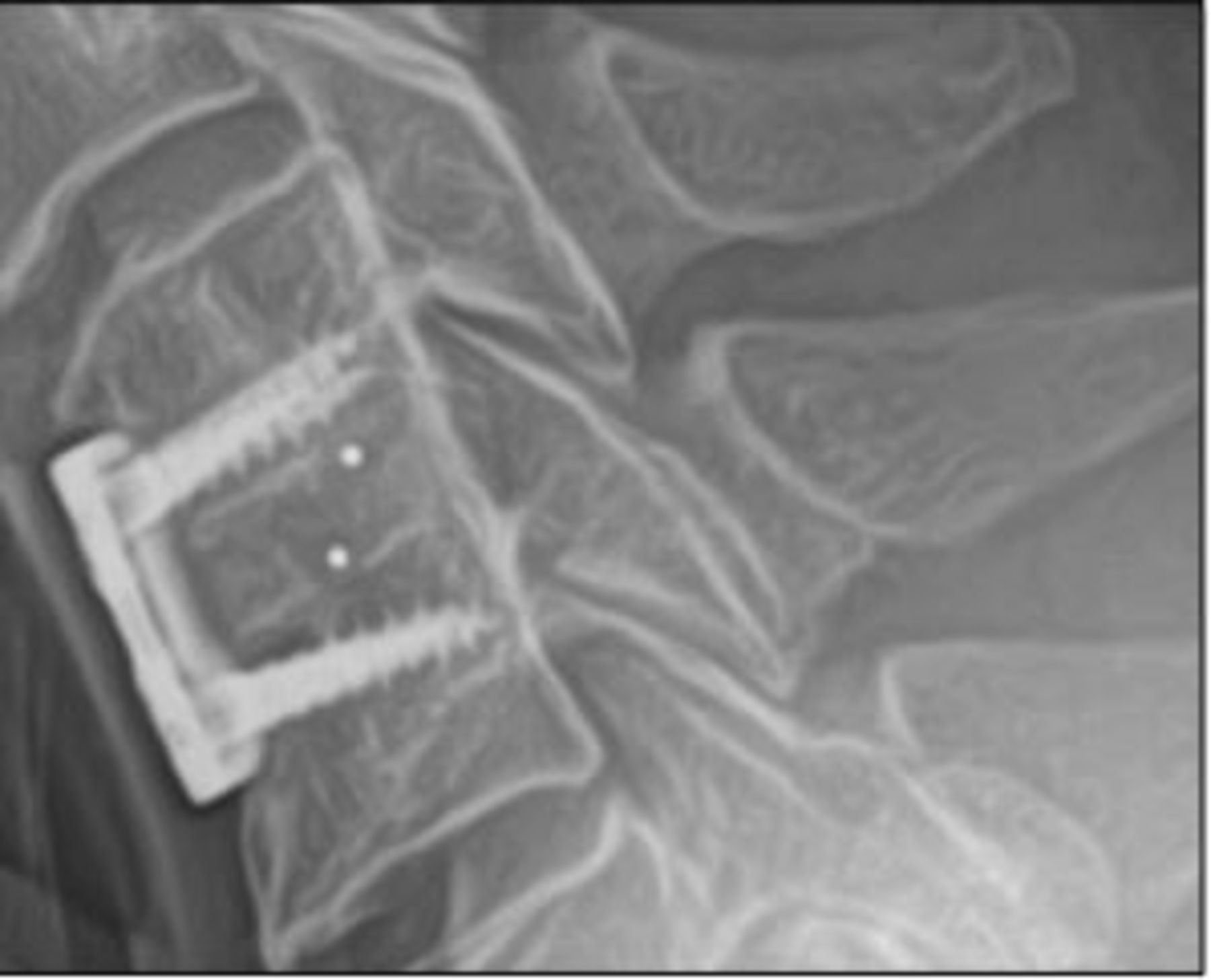
After medical clearance was obtained, patients were consented for their respective operation. Patients were administered general anesthesia in all cases. They were positioned supine throughout the case, and a standard Smith-Robinson approach to the anterior cervical spine was used for exposure—left- or right-sided approach was chosen based on patient anatomy/pathology and/or surgeon preference. At each operative level to be fused, an anterior cervical discectomy was performed. Following discectomy, an appropriately sized HA-PEEK interbody cage (CxHA, Innovasis, Inc., Salt Lake City, UT, USA) was inserted into the intervertebral disc space—notably, the hollow cage was filled with graft material per surgeon preference (eg, iliac crest bone graft, allograft, and synthetic). The CxHA interbody cage consists of a fully HA-impregnated PEEK implant matrix consisting of 80% PEEK and 20% HA. The cages are outfitted with tantalum markers to improve intraoperative placement and postoperative imaging evaluation (Figure 1). After the interbody cage was placed and confirmed radiographically, plate fixation was then performed spanning all fused levels.
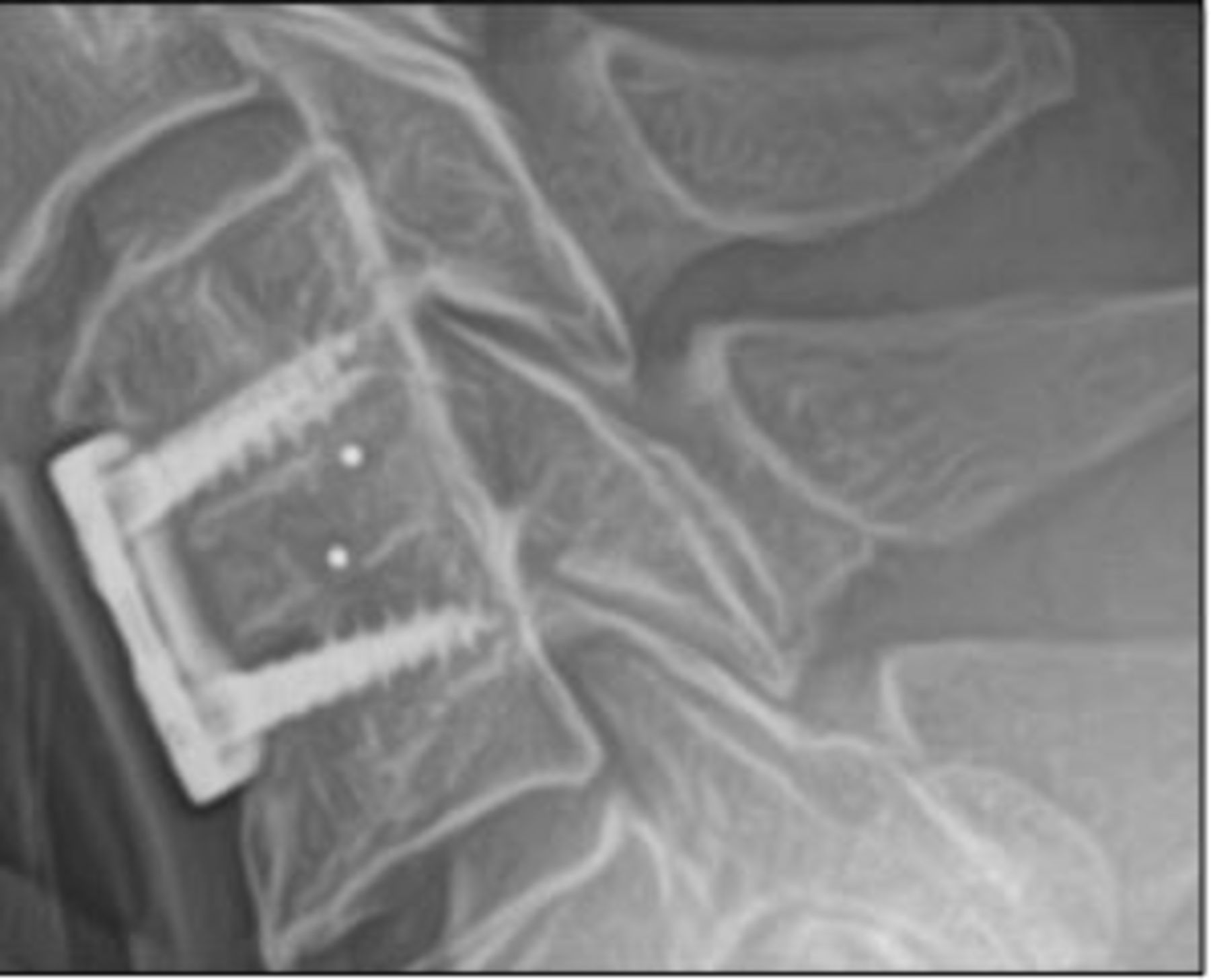
Example of a 1-level anterior cervical discectomy and fusion using a hydroxyapatite-polyetheretherketone interbody cage at 1 year postoperatively. Note that the tantalum markers are useful for both intraoperative placement and postoperative radiographic evaluation.
Radiographic Outcomes
This study aimed to evaluate postoperative interbody fusion as a primary outcome. Using dynamic flexion-extension radiographs, postoperative fusion was assessed on the basis of the angular range of motion (RoM, in degrees) and anteroposterior translational motion (in mm) at each individual operative interbody segment (ie, C4–C5 ACDF has 1 individual operative segment; C4–C7 ACDF has 3 individual operative segments, C4–C5, C5–C6, and C6–C7). Based on existing literature and radiographic standards, and to allow for comparison with contemporary investigations of fusion rates in ACDF, successful interbody fusion was defined as <4° RoM at each operated level on dynamic flexion-extension radiographs.8,29,30 Additionally, translational anteroposterior motion between adjacent vertebral bodies was evaluated. Less than 3 mm of translational motion was considered to constitute fusion. Four-view x-rays of the cervical spine (anteroposterior, lateral neutral, lateral flexion, and lateral extension) images were obtained preoperatively and postoperatively at 6- and 12-month follow-ups. Parameters were evaluated independently by an imaging core lab using a validated software, FXA (Functional x-ray Analysis, RAYLYTIC GmbH). Calculation of angular and translational motion is based on an evolutionary optimization algorithm that superimposes images by means of a 2D gradient-based registration of the vertebrae of interest.31 The software has been employed in numerous scientific studies and has proven to be a reproducible and accurate method of calculating differences in segmental RoM between preoperative and postoperative radiographs.29–32
Clinical Outcomes
Clinical outcomes were assessed preoperatively and at 6 weeks, 3 months, 6 months, and 12 months postoperatively using the following disease-specific measures: Neck Disability Index (NDI) and visual analog scale (VAS) for neck, left arm, and right arm pain. In addition, patient satisfaction was evaluated. Patients were prompted to answer whether they were satisfied with their treatment (dissatisfied, somewhat dissatisfied, somewhat satisfied, or satisfied) and whether they would undergo the same treatment again (definitely not, probably not, probably yes, or definitely yes).
Adverse Events
All adverse events directly related to the HA-PEEK interbody cage implanted (eg, device subsidence and device breakage) that eventually required cage revision were recorded by the operating surgeon in a database surrounding the patient registry cohort.
Statistical Methods
Descriptive (mean and SD) and inferential statistics were analyzed using “R” statistical programming language, a common method used in the evaluation of radiographic and clinical outcomes in ACDF.33 A 1-way analysis of variance (ANOVA) was performed, followed by post-hoc analysis using Scheffé’s test to evaluate significant changes in patient outcomes. Alterations in the distributions of patients’ satisfaction were evaluated with Fisher’s exact test followed by post-hoc pairwise testing. A P value of <0.01 (α) was considered to be statistically significant.
Results
Demographics
A total of 789 patients (men: 51.5%/women: 48.5%; mean BMI: 29.9 kg/m2) had undergone operations at the time of analysis. In total, 1565 individual interbody segments had undergone ACDF with placement of HA-PEEK interbody cages. Of these, 34.2% of patients had 1 segment fused, 41.7% had 2 segments fused, and 24.1% had 3 or more segments fused. Table 1 presents a complete overview of the demographics of patients included in the study.
Demographics and operative data of patient population.
Outcome Measures
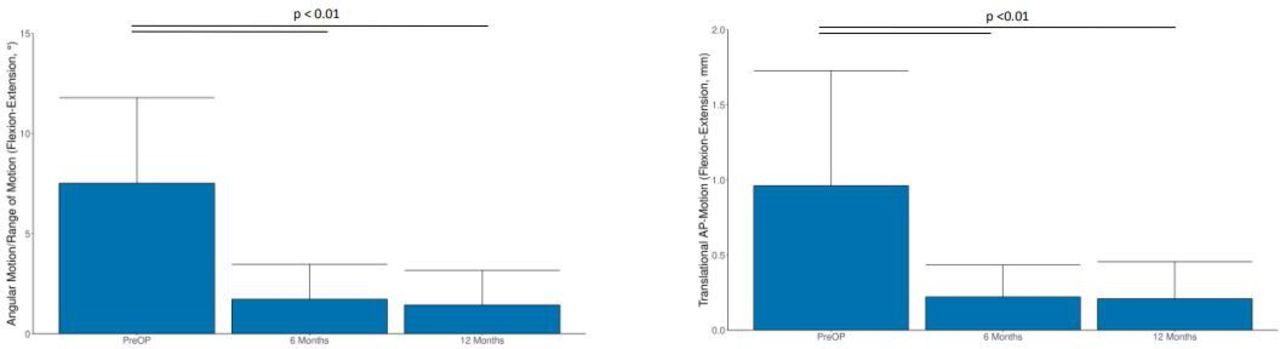
At baseline, patients showed a mean RoM of 7.5° at all segments (Figure 2). Mean segmental RoM at the operated segments decreased significantly (ANOVA: P < 0.01) to 1.7° at 6 months (post-hoc: P < 0.01) and 1.4° at 12 months (P < 0.01) postoperatively. Based on a radiographic threshold of <4° of angular motion and <3 mm of translational motion per interbody level, successful fusion was confirmed in 91.3% of all operated levels after 6 months and 92.2% after 12 months. Mean translational motion decreased from a mean of 1.0 to 0.2 mm by 6 months (P < 0.01) and 0.2 mm (P < 0.01) by 12 months postoperatively.
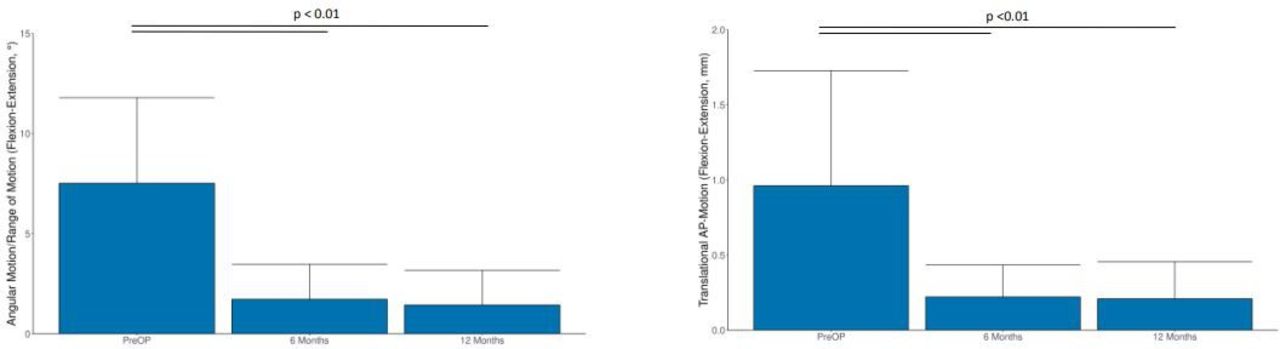
Bar plots for the radiographic outcome measures (left: angular range of motion; right: translational anteroposterior motion), including mean scores with SDs. Horizontal bars indicate post-hoc significant changes between preoperative and postoperative follow-up time points.
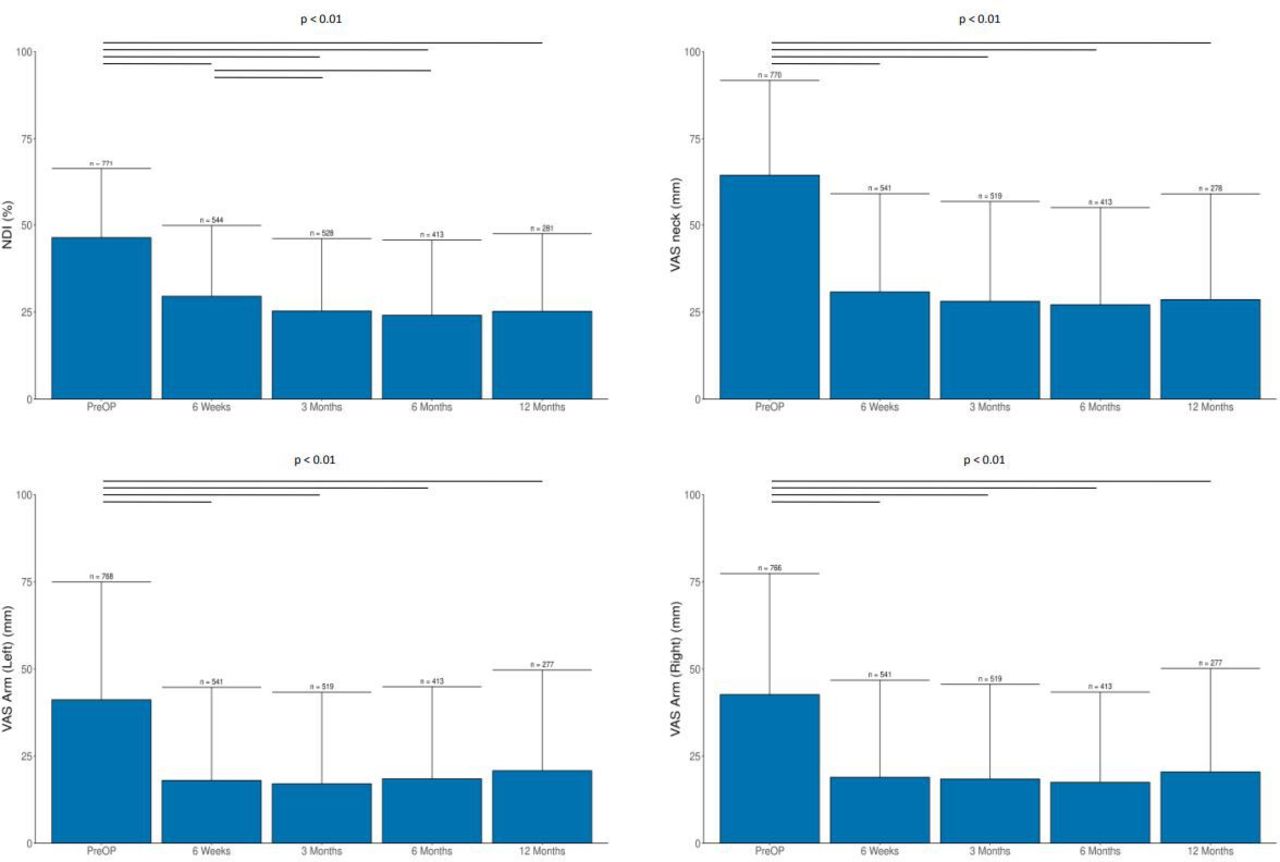
Regarding clinical outcomes, mean NDI scores declined significantly (ANOVA: P < 0.01; Table 2) from 46.3 preoperatively (n = 771) to 29.5 at 6 weeks (n = 544, post-hoc: P < 0.01), 25.3 at 3 months (n = 528, P < 0.01), 24.0 at 6 months (n = 413, P < 0.01), and 25.2 at 12 months (n = 281, P < 0.01). The percentage of patients exceeding the minimum clinically important difference (MCID) in NDI relief (MCIDNDI = 10%) at 12 months was 80.8% (n = 227). Mean VAS scores for neck pain decreased significantly from 64.2 preoperatively (n = 770) to 30.7 at 6 weeks (n = 541, P < 0.01), 28.1 at 3 months (n = 519, P < 0.01), 27.1 at 6 months (n = 413, P < 0.01), and 28.6 at 12 months (n = 278, P < 0.01). The percentage of patients exceeding the MCID in VAS relief (MCIDVAS-NECK = 20%) was 62.2% (n = 173). Mean VAS scores for left arm pain decreased significantly from 41.1 (n = 768) to 18.0 at 6 weeks (n = 541, P < 0.01), 17.0 at 3 months (n = 519, P < 0.01), 18.5 at 6 months (n = 413, P < 0.01), and 20.8 at 12 months (n = 277, P < 0.01). Reductions in right arm pain VAS scores exhibited a similar behavior, with statistically significant decreases between preoperative and all postoperative mean values (42.6 preoperatively [n = 766] to 18.9 [n = 541, P < 0.01] at 6 weeks, 18.4 [n = 519, P < 0.01] at 3 months, 17.4 [n = 413, P < 0.01] at 6 months, and 20.4 [n = 277, P < 0.01] at 12 months). Figure 3 visualizes the development of clinical outcomes of patients at each follow-up.
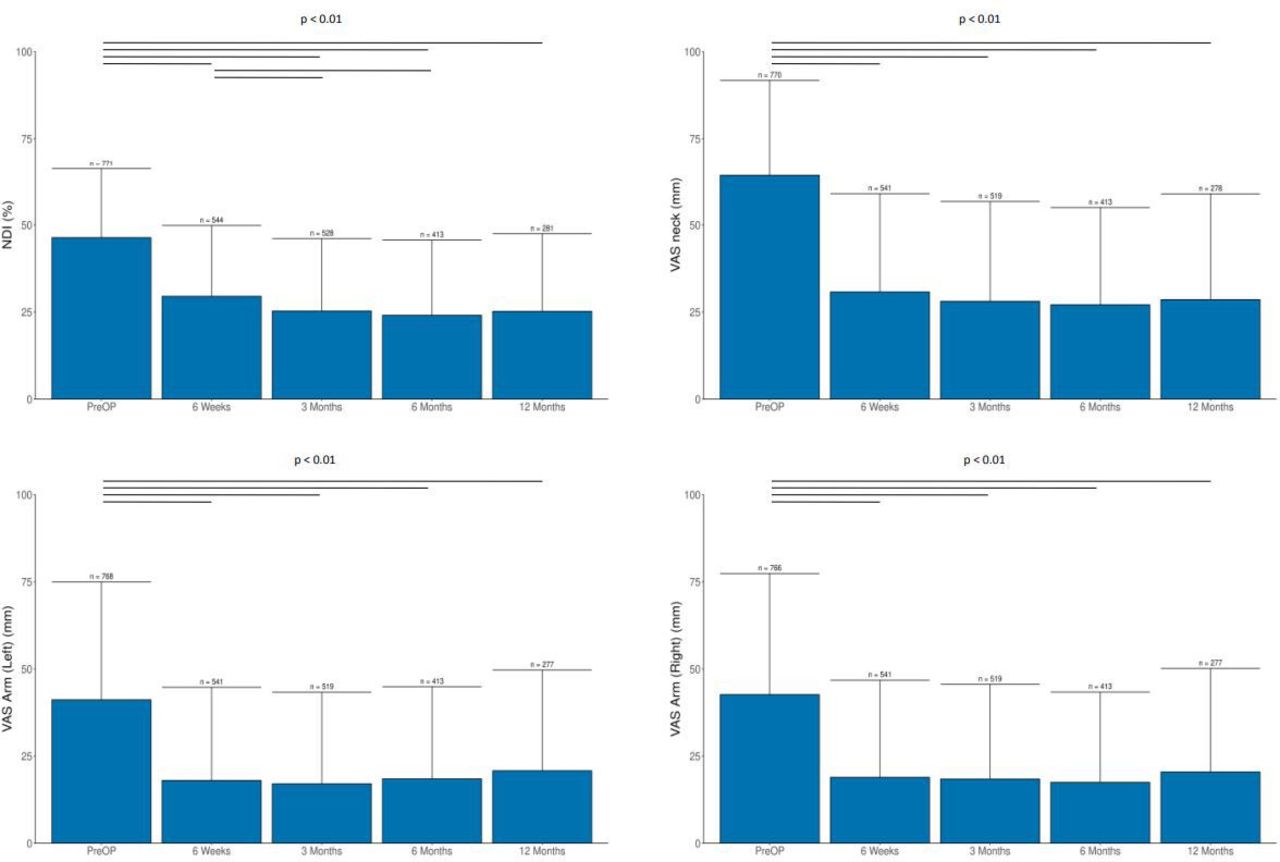
Bar plots for the clinical outcome measures, including mean scores with SDs. Horizontal bars indicate post-hoc significant changes between time points.
PROMS at preoperative and standard postoperative periods.
Patient satisfaction remained consistent across the entire postoperative examination period (Table 3). At 6 weeks postoperatively, 97.7% of patients reported being satisfied or somewhat satisfied with their treatment (n = 556). At 3, 6, and 12 months postoperatively, this number remained statistically unchanged (P = 0.13)—95.6% (n = 527), 96.8% (n = 419), and 95.1% (n = 273), respectively. The percentage of patients who reported they would definitely or probably have the treatment again was 93.7% at 6 weeks (n = 533), 92.0% at 3 months (n = 507), 93.3% at 6 months (n = 404), and 92.3% at 12 months (n = 265) postoperatively (statistically unchanged at P = 0.75).
Analysis of patient satisfaction for all evaluated examination periods.
Based on the entire cohort and 1565 inserted implants, 3 patients (0.2% of all devices implanted) underwent a revision of their HA-PEEK device. The reasons for cage revision were as follows: distal junction failure/kyphosis, device loosening, and device breakage during implantation, which was replaced directly during the index surgery.
Discussion
Contemporary literature lacks large-scale evaluations of radiographic and clinical outcomes following ACDF using HA-PEEK composite implants. The incorporation of HA into PEEK has gained attention as a strategy to improve the osseointegrative capacity of implants in other areas of spine surgery and orthopedics, as well as in dental applications.34 Although the basic science has produced promising results, outcomes have not always reflected the benefits of HA evident in these studies. Objections regarding its cost and lack of long-term data have surfaced here. This study was conducted to offer the first large-scale, multicenter outcome evaluation of HA-PEEK interbody cages in patients undergoing ACDF. The analysis revealed significant improvements in clinical outcomes at all postoperative time points, as well as promising radiographic outcomes at 6- and 12-month follow-ups. Additionally, with a cage revision rate of less than 0.2%, the data support HA-PEEK cages as a safe and effective alternative to conventional implant materials.
The literature currently lacks true consensus regarding a radiographic definition of fusion.8,9 Oshina et al in a systematic review of 59 studies identified 10 unique criteria for assessing radiographic outcomes following ACDF.8 Another systematic review of 34 ACDF clinical studies by Goldberg et al echoes this dilemma.9 Unfortunately, inconsistencies in radiographic parameters (eg, trabecular bone bridging, angular and translational motion, subsidence, and radiolucency), use of different imaging modalities (plain x-ray, flexion-extension x-ray, and computed tomography [CT] scan), and cage surface technologies have proven to be challenging in performing direct comparisons between previous studies and the current study. Other confounding parameters include differently sized patient cohorts, variable indications for surgery, medical comorbidities, and a number of levels fused (ie, 1-level fusion vs multilevel fusion). To overcome these challenges and the limited reliability and objectivity inherent to manual measurements and assessments typically done by radiologists, fusion success was evaluated in our study by an independent imaging core laboratory using a highly precise, validated method.31 When compared with recent studies using equivalent imaging data and radiographic parameters, the present study demonstrates equally favorable fusion rates and mean reductions in segmental RoM. Mayer et al assessed a smaller cohort of patients in 18 ACDF patients receiving bioactive 3D-printed titanium cages filled with autologous bone marrow. Fusion was defined using a RoM threshold of <4° at the operated level on dynamic flexion/extension radiographs. They found a reduction in mean RoM of 7.7° to 1.8° at 12 months postoperatively, which translated to a fusion rate of 94.4%.29 Arts et al conducted a similar evaluation of a 3D porous titanium cervical device, and in their 49 patients, observed a reduction in mean RoM from 8.7° to 1.6° at 12 months. Similarly, their RoM threshold of <4° produced successful fusion in 91% of their patients. Both of these recent studies using similar methods of fusion evaluation compare quite closely with data from our patient cohort, with a mean reduction in RoM from 7.5° to 1.4° after 12 months. Of the studies mentioned, our current study demonstrates the lowest mean RoM of 1.4° in the setting of a considerably larger, multicenter patient cohort.
Current research has reported fusion rates for ordinary PEEK implants ranging from 62% to 100% after 1 year.9,30,35,36 At a mean follow-up of 16 months, Pechlivanis et al found fusion rates of 71.4% in nonfilled PEEK cages.37 Similarly, Suess et al assessed the radiographic and clinical outcomes of 292 patients receiving empty PEEK cages and found radiographic fusion in only 43% of patients at 6 months and 73% of patients at 12 months.35 Both studies partially evaluated fusion using CT imaging to confirm the presence of continuous trabecular bone bridging. While CT imaging is an additional method to confirm fusion, it poses additional costs and exposure to radiation without revealing the presence or absence of segmental motion, as is the case in flexion-extension radiographs. Whether the HA-PEEK cages studied here facilitate bone bridging as an additional fusion criterion should be the topic of future research.
In addition to the radiographic analysis, the significant improvements in VAS and NDI scores up to 12 months after surgery expand upon previous findings in ACDF studies using HA-infused PEEK implants. Chin et al compared 41 patients undergoing ACDF with HA-impregnated PEEK (80% PEEK/20% HA) and 47 patients receiving standard PEEK cages.26 Patients receiving HA-PEEK cages demonstrated significant improvements in VAS neck (58 ± 3 down to 25 ± 3, P < 0.001) and NDI (23.3 ± 1.1 down to 8.2 ± 1.0, P < 0.001) scores when comparing mean preoperative and 24 months postoperative scores. Comparing these results to our study population, there exist many similarities, simply on a much larger scale.
There are some notable limitations to the present study. While the study is prospective, it did not perform a comparison of patients receiving a direct control group of PEEK, titanium, or even allograft implants. Thus, the radiographic and clinical data compiled can simply be compared with data existing in related studies. The study analyzed a limited but critical subset of radiographic parameters to evaluate fusion—angular and translational motion. We chose not to analyze other radiographic parameters such as cage subsidence, cage migration, and parameters of cervical sagittal balance (eg, segmental lordosis and C7 slope) that might be affected by interbody cage placement and could influence patient outcomes. The current study aimed to present preliminary outcomes of a large, growing patient cohort, so future studies are planned that will analyze 2-year outcome data for the ongoing patient cohort. Even with limited follow-up to date, the number of included patients in this study far exceeds existing smaller, single-centered published studies.
Conclusion
The current study is the first of its kind to present real-world data of ACDF using fully HA-infused PEEK cages. The study demonstrates promising radiographic and clinical outcomes, supporting the safety and efficacy of these bioactive cages. The findings support the potential benefits of incorporating HA into PEEK implants to enhance fusion rates and improve patient outcomes. Further studies with control groups and expanded radiographic parameters are warranted to validate these findings and provide a more comprehensive understanding of HA-impregnated PEEK cage performance.
Acknowledgments
We thank Preston Melchert for his exceptional contribution to the development and editing of the manuscript.
Footnotes
Funding The authors received no funding for the work. However, Innovasis supported the registry and performed the data analysis.
Disclosures Kris Radcliff discloses royalties or licenses from Corelink and Globus (both unrelated to the current topic; consulting fees from Innovasis, Corelink, Stryker, and Orthofix (all unrelated to the current topic; and payment for expert testimony for various law firms in New Jersey; and stock or stock options from 4 web medical and Orthofix (both unrelated to the current topic). Fred Mo discloses consulting fees from Spinewave, Stryker, and Innovasis and participation on a Scientific Monitoring Board—Ossdsgn. S. Babak Kalantar discloses payments from Innovasis made to their institution for registration of registry patients; royalties or licenses from Nuvasive and Royal Biologics; and consulting fees from Stryker, Nuvasive, Innovasis, and Royal Biologics. The remaining authors have no disclosures or conflicting interests.
IRB Approval Innovasis works with local IRB and WIRB to complete requirements to conduct the BioBase Registry at participating sites.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.