


Abstract
Background Blunt spinal injuries (BSIs) are associated with substantial morbidity and mortality. Management typically involves stabilization of the spinal column and may include chemoprophylaxis for venous thromboembolism (VTE) prevention. The optimal timing of chemoprophylaxis initiation in operatively managed BSI patients remains debated.
Objective Analyze available literature on optimal chemoprophylaxis timing for the prevention of VTE in patients postinjury undergoing operative repair.
Study Design Systematic review and meta-analysis.
Methods A systematic review and meta-analysis were conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. PubMed and MEDLINE were searched for studies assessing chemoprophylaxis timing in adult BSI patients. Inclusion criteria focused on operatively managed BSIs and anticoagulant usage assessment.
Results Three studies involving 4345 patients were included. Early chemoprophylaxis initiation was associated with significantly lower deep vein thrombosis (DVT) and overall VTE incidence compared with late initiation. No significant differences were found in pulmonary embolism (PE) incidence or mortality.
Conclusion Early anticoagulant administration after spinal fixation for BSI reduces DVT and overall VTE risk without impacting PE incidence or mortality. Further research is recommended to solidify these findings and address existing gaps in the literature.
Clinical Relevance Early chemoprophylaxis initiation in operatively managed BSI patients reduces DVT and overall VTE risk without affecting PE incidence or mortality
Level of Evidence 2.
- Spinal injury
- blunt trauma
- venous thromboprophylaxis
- neurosurgery
- thromboembolism
- trauma
- deep venous thrombosis
- pulmonary embolism
- heparin
- low molecular weight heparin
Key Points
Early chemoprophylaxis initiation in operatively managed blunt spinal injury patients significantly reduces the incidence of deep vein thrombosis and overall venous thromboembolism.
No significant differences in pulmonary embolism incidence or mortality were observed between early and late chemoprophylaxis initiation.
Further research is necessary to confirm these findings and refine guidelines on the optimal timing of chemoprophylaxis in blunt spinal injury patients.
Introduction
Spinal injuries are a devastating consequence of trauma, resulting in substantial morbidity and mortality.1 Blunt spinal injuries (BSIs) include injury mechanisms such as falls and motor vehicle accidents.2 The American Association of Neurological Surgeons/Congress of Neurological Surgeons guidelines state that the first-line management for trauma patients who are awake, alert, and do not have intoxication is a combination of a rigid cervical collar and supportive blocks on a backboard with straps is adequate to limit motion of the cervical spine.3 Furthermore, surgical management of BSI often involves stabilization of the spinal column and decompression of the spinal cord to prevent further damage.
In addition to the primary injury, patients are also at risk of developing secondary complications such as venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE).4 Chemoprophylaxis for VTE prevention involves using medications to reduce the risk of VTE. Understanding the optimal time of chemoprophylaxis use is crucial to providing the best possible care. This requires balancing the benefit of preventing VTE and minimizing the risk of bleeding.
While the current data are mostly retrospective and need further research, several studies have been conducted to determine the optimal timing of chemoprophylaxis for VTE in trauma patients who were operatively managed. These studies have compared the efficacy and safety of early chemoprophylaxis, initiated within 24 to 48 hours postinjury, vs late chemoprophylaxis, commenced after 48 hours postinjury. One study found that administering chemoprophylaxis within the first 24 hours was associated with a significantly lower incidence of VTE than late chemoprophylaxis.5 In contrast, another study showed that initiating chemoprophylaxis within 72 hours postinjury resulted in a lower incidence of DVT and PE than delayed initiation beyond 72 hours postinjury.6 Notably, the 2022 American College of Surgeons Trauma Quality Program Best Practice Guideline for Spine Injury recommends chemoprophylaxis within the first 72 hours.7
This meta-analysis aimed to systematically review the existing evidence on the optimal timing of chemoprophylaxis initiation in adult patients with BSIs managed operatively. By comparing early vs late initiation of chemoprophylaxis, we aim to evaluate its impact on mortality; the total incidence of VTE, DVT, and PE; and length of stay in the hospital.4–7
This involved searching from the date of inception of the databases till January 2024. Databases included were PubMed and MEDLINE using only English. The PubMed search string included terms related to blood prophylaxis, VTE, trauma, and spinal cord.
Materials and Methods
For this meta-analysis, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses8 guidelines were taken into account. The population of this study was adult patients with BSIs managed operatively. The intervention was early chemoprophylaxis in VTE, the comparison was late chemoprophylaxis in VTE, and outcomes were mortality, total VTE, DVT, and PE. All studies published prior to January 2024 were evaluated thoroughly to assess whether they met the inclusion criteria.
This study’s primary outcome was the occurrence of overall VTEs defined as the formation of a clot in a blood vein either manifesting as a PE or DVT. Secondary outcomes included number of DVTs, PEs, and mortality.
Data Sources and Search Strategy
The electronic databases PubMed and MEDLINE were searched from their inception to January of 2024. The following search strategy was used to search PubMed: “prophylaxis OR prophylactic AND VTE OR thrombus OR embolism AND trauma OR traumatic AND spine OR spinal OR spinal cord.” To further identify relevant and eligible studies, a manual search was conducted on Google Scholar and using the citations list of retrieved studies and relevant publications.
Study Selection
Studies were included if they met the following inclusion criteria: (1) involved isolated blunt traumatic spinal injuries managed operatively, (2) assessed anticoagulant usage both late and early based on their own definition, (3) postinjury status mentioned within the study, and (4) included only adult patients. Studies were excluded if they involved a pediatric population, if they combined injuries involving an injury severity score of more than 3 (to rule out other possible confounding injuries), if the spinal injury was managed conservative, or if the study was published as a case series, report, or conference abstract. Studies not published in English were also excluded.
Data Extraction and Assessment of Study Quality
EndNote Reference Library software was utilized to import the findings of the comprehensive literature search. The software automatically detected and removed duplicates. Formal screening of titles and abstracts was performed by 2 independent investigators (F.A.A. and N.A.A.) to determine which studies met the inclusion criteria. The full texts of the studies that passed the initial screening were obtained and evaluated for eligibility. All disagreements were resolved through consensus and discussion with a third reviewer (M.O.A.). Data on the primary and secondary outcomes, as well as patient characteristics and study details, were extracted.
Statistical Analysis
The statistical analysis was performed utilizing Review Manager (RevMan, version 5.4.1; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The primary and secondary outcomes data were combined using a random effects model. The results for continuous outcomes were represented as mean differences. For dichotomous outcomes, odds ratios (ORs) with 95% confidence intervals (CIs) were expressed. A P value less than 0.05 was considered to be statistically significant. The Higgins I2 statistic was used to evaluate heterogeneity, and a value greater than 50% indicated significant heterogeneity.
Results
Results of Literature Search
As seen in Figure 1, from our literature search of 2 databases, 787 studies were initially retrieved. After the removal of duplicates, 583 studies were left. A further 571 studies were excluded based on title and abstract screening. Of the 12 studies that remained, 2 could not be retrieved even after contacting their respective corresponding authors. Of the remaining 10 studies, 5 involved severe injury defined as an injury severity score (ISS) of 3 or more in other areas of the body, 2 studies were managed conservatively without surgical intervention, with the remaining 3 studies meeting the inclusion criteria. The results of the meta-analysis of these 3 observational studies comparing the outcomes of early thromboprophylaxis to late thromboprophylaxis are shown in Figure 2 with their respective forest plots depicting the effect size.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram showing literature search.

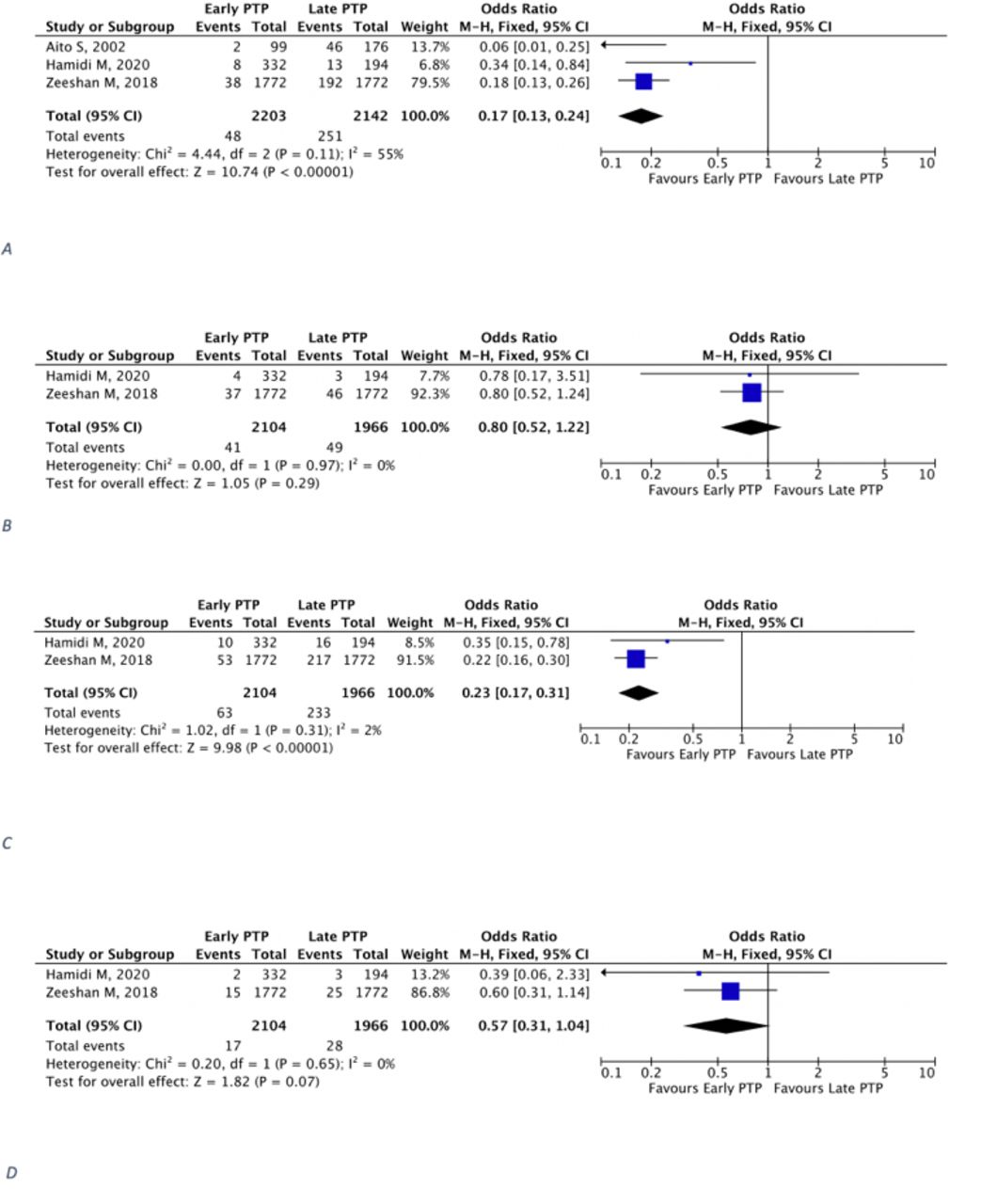
Forest plots showing (A) deep venous thrombosis, (B) mortality, (C) overall venous thromboembolism, and (D) pulmonary embolism.
Study Characteristics
The 3 studies included in this review were all retrospective observational studies. The total number of patients involved was 4335, with 2203 given VTE prophylaxis early and 2132 receiving it late. Other baseline characteristics and clinical features of the studies can be seen in Tables 1 and 2, respectively.
Characteristics of the included studies.
Design and clinical characteristics of included studies.
Outcomes
Deep Venous Thrombosis
Three studies (Figure 2A) reported on the incidence of DVT in early PTP compared with late PTP (early PTP group: 2203 patients and 48 events; late PTP: 2142 patients and 251 events). The early PTP group had a significantly lower incidence of DVT compared with the late PTP group (OR 0.17, 95% CI 0.13–0.24; P < 0.00001; I 2 = 55%), and the result was significantly heterogeneous.
Mortality
Two studies (Figure 2B) reported on mortality in early PTP compared with late PTP (early PTP group: 2104 patients, and 41 events; late PTP: 1966 patients and 49 events). There was no difference between the 2 groups in terms of mortality (OR 0.80, 95% CI 0.52–1.22; P = 0.29; I 2 = 0%), and the result was homogeneous.
Venous Thromboembolism
Two studies (Figure 2C) reported on the total overall VTE in early PTP compared with late PTP (early PTP group: 2104 patients and 63 events; late PTP: 1966 patients and 233 events). The early PTP group had a significantly lower incidence of VTE compared with the late PTP group (OR 0.23, 95% CI 0.17 to 0.31; P < 0.00001; I 2 = 2%), and the result was homogeneous.
Pulmonary Embolism
Two studies (Figure 2D) reported on the incidence of PE in early PTP compared with late PTP (early PTP group: 1772 patients and 17 events; late PTP: 1966 patients and 28 events). There was no difference between the 2 treatment groups in terms of PE (OR 0.57, 95% CI 0.31–1.04; P = 0.07; I 2 = 0%), and the result was homogeneous.
Discussion
Blunt spinal trauma is a complicated and potentially fatal injury that frequently results in severe neurological impairment.8 These injuries have a significant impact on a person’s quality of life and functional independence because they can cause a range of neurological deficits, such as paralysis, sensory loss, and autonomic dysfunction. Our study aimed to assess the optimal timing of chemoprophylaxis for VTE in adult patients with BSIs managed operatively. The data consist of 4345 patients from 3 studies.9–11 Patients were divided into 2 groups: those with the early initiation of pharmacological thromboprophylaxis (n = 2203) and those with late initiation were (n = 2142).
In the treatment of BSI, VTE, which includes PE and DVT, becomes a major concern.12 The pathophysiological alterations brought on by BSI predispose patients to a hypercoagulable state, raising the risk of thromboembolic events. These factors include immobilization, endothelial damage, and changes in blood flow dynamics.13
For this reason, effective VTE prophylaxis is crucial to the management of BSI in order to reduce the chance of thromboembolic complications and enhance patient outcomes. Pharmacological treatments like unfractionated heparin and low molecular weight heparin have shown promise in lowering the incidence of VTE in patients with BSI without appreciably raising the risk of hemorrhagic complications. These medications work by stopping the formation of clots and thrombus, which lowers the risk of DVT and subsequent PE.14
In our analysis, patients who had undergone operative fixation for blunt spinal trauma receiving anticoagulation early were less likely to develop PEs and VTE as a whole. This is in accordance with numerous other studies that had described different population groups that had similarly gone through trauma.5,6,15,16 However, the timing of restarting early vs late anticoagulation therapy in patients with recent spinal surgery is still debatable.17 The reasoning behind this is due to the lack of sufficient evidence. Regardless, guidelines have come out in support of early administration in the majority of circumstances in which trauma is involved as a whole.17–19 In terms of PEs and mortality, the possible reasoning behind the lack of statistical significance could be due to insufficient numbers of cases. For example, in the Hamidi study, PE only occurred in 2 and 3 patients in the early and late groups, respectively.9
Limitations
Limitations of the present study include a lack of studies, with only 3 being included in the analysis. This is mostly due to the precise inclusion criteria used in our study, in which the population group was specified as much as possible. Another limitation is the variation in defining early initiation of chemoprophylaxis, with 1 study defining early as less than 72 hours and the remaining 2 as less than or equal to 48 hours. Furthermore, complications such as spinal bleeding could not be assessed as only 1 study included this within their results. Lastly, the 3 included studies were cohort studies that had no randomization or blinding, which could introduce different biases associated with such study types.
Conclusion
We found that early administration of anticoagulant in patients who had undergone spinal fixation for isolated blunt trauma to the spine was associated with a statistically significant decreased risk of developing DVT and overall VTE. There was no difference in terms of PEs, mortality rate, or hospital length of stay. To further consolidate any conclusions, we recommend additional studies be performed on the same population group to address the gaps in the literature.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Author Contributions Conceptualization: Faisal A. AlGhamdi, Mohammed M. AlKabbani, and Renad M. AlJoaid. Data acquisition, analysis, or interpretation: Mohammed O. Alzayer, Nasser A. AlJoaib, and Kawther M. Hadhiah. Software creation: Nisreen H. AlMaghraby. Drafting the work or substantive revision: Renad M. AlJoaid, Nasser A. AlJoaib, and Kawther M. Hadhiah. Data collection: Faisal A. AlGhamdi, Mohammed O. Alzayer, and Mohammed M. AlKabbani. Statistical analysis: Renad M. AlJoaid and Kawther M. Hadhiah. Interpretation of results: Faisal A. AlGhamdi and Nisreen H. AlMaghraby.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.