


Abstract
Background The single-position prone transpsoas (PTP) lateral interbody fusion represents an alternative approach to the traditional lateral lumbar interbody fusion (LLIF) typically performed with the patient in the lateral decubitus position. Advantages of PTP surgery include improved segmental lordosis, single-position surgery, and ease of performing posterior techniques as needed. However, the learning curve of PTP is distinct from that of traditional LLIF surgery performed with the patient in the lateral decubitus position. Here, we highlight the senior author’s approach to PTP surgery. The authors review key strategies of the preoperative workup, patient selection, operative techniques, and intraoperative pearls. This technical guide aims to shorten the learning curve for new adopters, optimize workflow for the surgeon, and maximize patient safety.
Methods A detailed analysis of the PTP approach was conducted, incorporating preoperative imaging and planning strategies and technical adjustments in patient positioning to accommodate access following the senior author’s technical pearls. The workflow was structured to streamline transitions between levels, minimize time requirements, and reduce physical strain on the surgical team.
Results The application of PTP has demonstrated successful segmental lordosis correction and stable fusion across lumbar levels without requiring patient repositioning. The integrated workflow enabled sequential access and mastery of the PTP technique. These technical pearls have improved the efficiency of the PTP approach, according to the surgeon’s expertise.
Conclusion The PTP technical strategies offer a viable and effective alternative to traditional LLIF. Surgeons can enhance the safety and efficiency of the PTP approach, maximize procedural benefits, and minimize potential risks using these technical strategies for preoperative planning, patient positioning, and intraoperative monitoring.
- lateral
- lateral lumbar interbody fusion
- lumbar
- minimally invasive surgery
- patient positioning
- prone
- prone transpsoas
- spine
- surgery
Introduction
Lateral lumbar interbody fusion (LLIF) using the transpsoas approach has increasingly gained favor as a minimally invasive option that allows for indirect decompression, placement of interbody cages with large footprints, improved restoration of segmental lordosis, and decreased interbody subsidence risk.1 The prone transpsoas (PTP) lumbar interbody fusion method leverages the benefits of traditional LLIF while permitting direct posterior access without requiring the patient to be repositioned for percutaneous screw placement (Figure 1).2–4 This approach shortens anesthesia times, enhances operating room efficiency, offers concurrent posterior access for instrumentation, and has the advantage of familiar prone patient positioning.

Ergonomics of the prone lateral transpsoas approach during percutaneous pedicle screw fixation and lateral lumbar fusion.2–4 Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
The PTP approach has unique learning curve challenges that set it apart from traditional lateral surgery. The following step-by-step guide is based on the senior author’s preferred workflow. It details technical nuances, including preoperative planning, patient positioning, transpsoas approach, interbody preparation, implant placement, and essential safety measures designed to minimize complications.
Preoperative Planning and Surgical Methodology
Surgical Indications
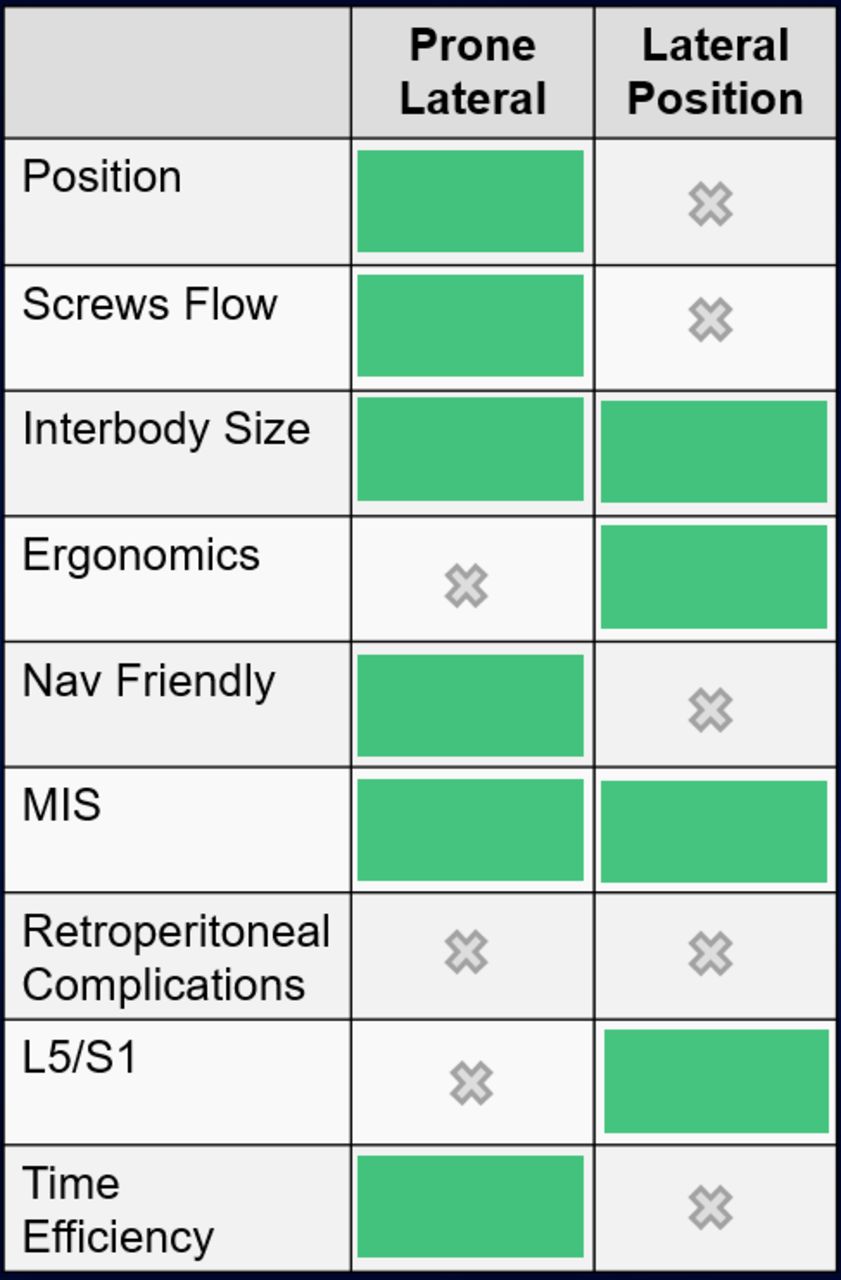
For the senior author, effective preoperative planning is the foundation of a successful PTP approach, involving careful evaluation of imaging, anatomical characteristics, and patient-specific risk factors. The indications for PTP surgery are similar to those for traditional LLIF and posterior lumbar fusion, though certain cases are particularly suited to PTP’s unique benefits. These include spinal degenerative disease, grade 1–2 spondylolisthesis, and complex scoliosis requiring instrumentation (Figure 2).5,6 Relative contraindications include high body mass index (BMI). Unlike traditional LLIF approaches, prone positioning does not allow the abdomen to fall away from the spine. Thus, in PTP, increased BMI and abdominal adipose will lengthen the distance from the skin to the lateral border of the disc space and prohibit safe access to the spine in the prone position. A high iliac crest may also be a relative contraindication. Manipulating the iliac crest from a caudal perspective is more challenging when the patient is positioned prone than in a lateral decubitus position. Beyond high BMI and crest positioning, similar contraindications for LLIF should be considered, including anterior psoas positioning and unfavorable great vessel anatomy.7

Senior author’s recommendations and advantages of the prone lateral transpsoas approach vs lateral lumbar interbody fusion. Used with permission from Barrow Neurological Institute, Phoenix, Arizona. Abbreviations: MIS, minimally invasive surgery; Nav, navigation.
Preoperative Imaging
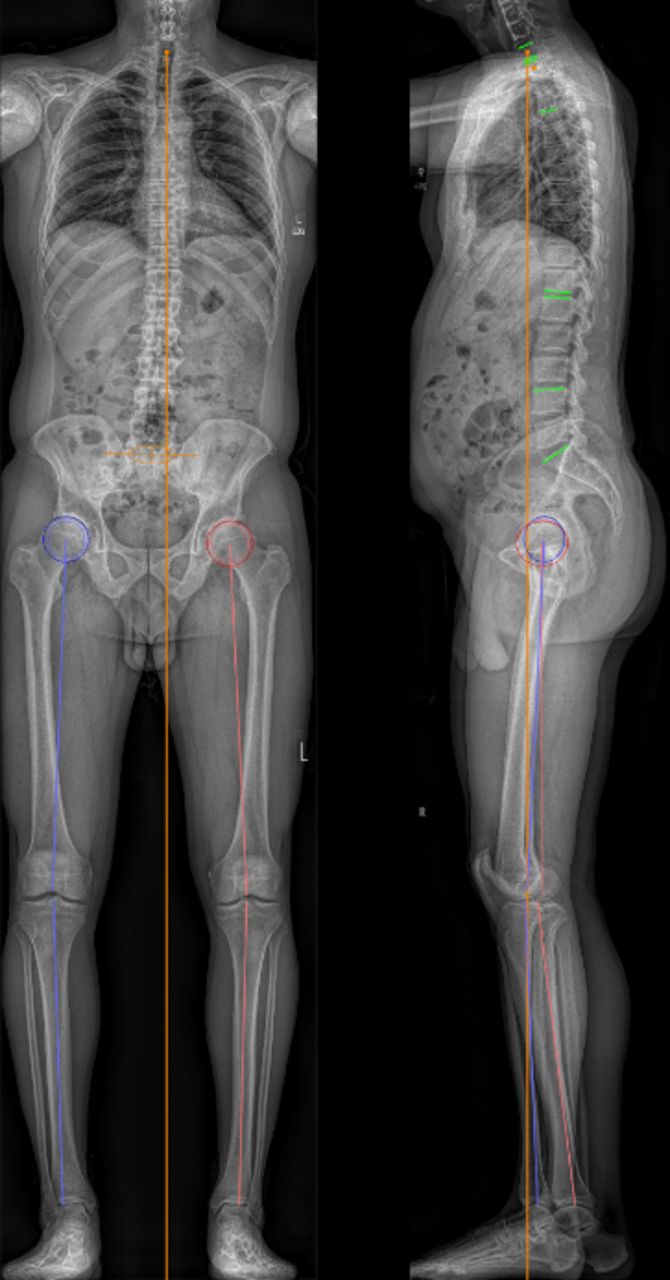
A comprehensive imaging assessment is crucial. Standing scoliosis radiographs, flexion-extension lateral radiographs, computed tomography (CT), and magnetic resonance imaging (MRI) are used to guide the senior author’s decisions on the surgical approach, level selection, and interbody cage placement. Standing scoliosis radiographs provide a view of coronal and sagittal alignment, aiding the surgeon in determining the degree of lumbar lordosis required at each level. The senior author uses preoperative planning software to set target alignment goals (Figure 3). CT scans are also obtained for all patients to assess vertebral bone density, pedicle morphology, and osteophyte development. Patients with osteopenia should be optimized with biologics before surgery to minimize the risk of mechanical complications. MRI is essential for evaluating neural element compression and assessing vascular structures to determine the safest side of the approach and to prevent intraoperative nerve or vessel injury.3,7,8

Standing radiographs using the electro-optical system (EOSedge, ATEC Spine Group) for preoperative spinal alignment and surgical planning. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Approach Side
Selection of the approach side is critical in PTP planning. When addressing patients with scoliosis, the senior author prefers an approach from the concave side of the curve.9 This approach provides easier access to multiple levels through a smaller incision. The location of the iliac veins can also dictate the approach side. When these vessels are dorsally located relative to the vertebral body on preoperative CT and MRI, the preferred approach is from the side of the vessel. It is easier to avoid injuring the vessel with initial docking on the ipsilateral side because the vessel can be more safely moved anteriorly using forward retraction of the anterior retractor blade rather than during contralateral osteophyte release or disc prep, where direct visualization contralaterally is impossible.10
Patient Positioning
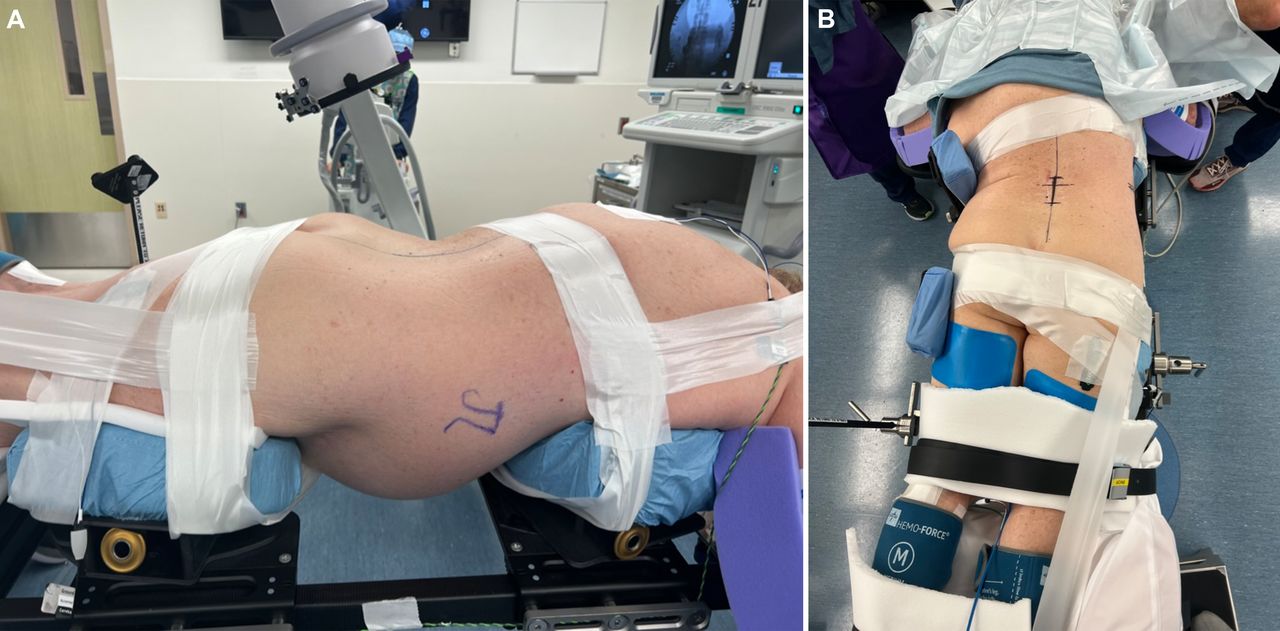
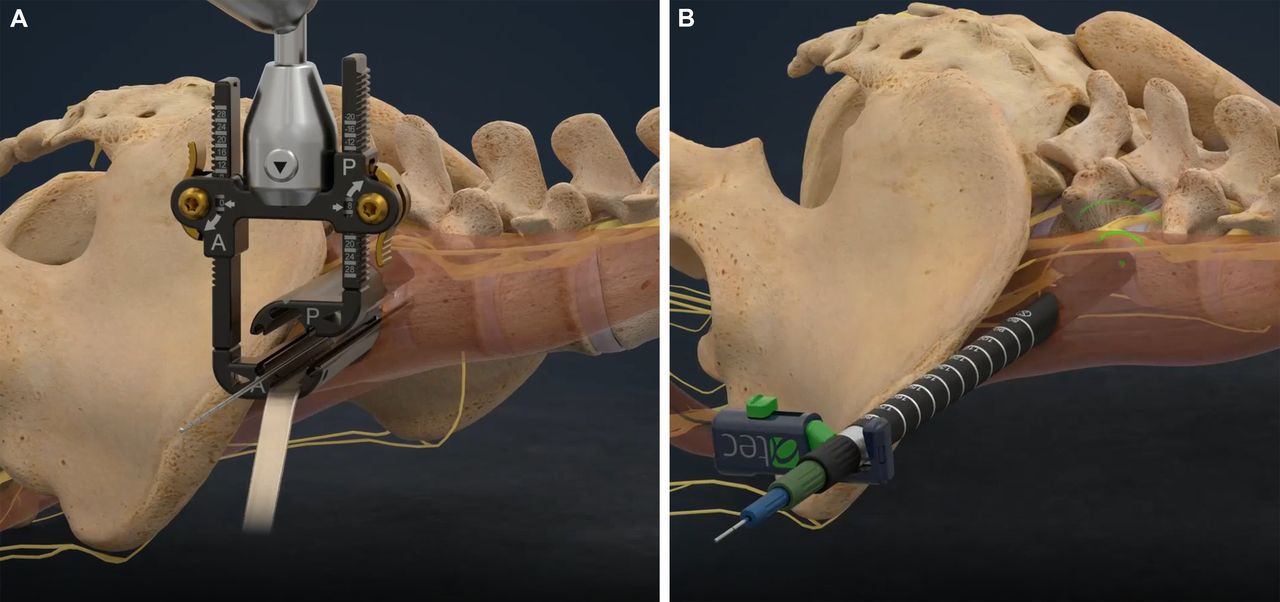
The patient is positioned prone on a Jackson radiolucent table, with the abdomen freely suspended to minimize venous pressure and maintain lumbar lordosis. A radiolucent table is essential for intraoperative fluoroscopy or navigation. Special attention is given to hip padding, with a bolster placed beneath the posterior superior iliac spine to stabilize the pelvis. The hips and knees are flexed slightly to improve disc space access and optimize working angles for enhanced lordosis.7,11 Tape is applied superiorly on the chest and inferiorly on the pelvis to stabilize the patient during the procedure. Prone positioning also has the benefit of elongating the psoas muscle, effectively retracting neural elements, and decreasing the risk of nerve injury.12 The senior author uses custom bolsters to allow coronal bending at the pelvis and chest to create a larger working window between the ribs and iliac crest. This technique allows for reliable and reproducible access, similar to breaking the bed in the lateral decubitus position in LLIF. In cases where a custom table is unavailable, a modified hip bolster can be placed on the contralateral side of the approach above the crest. This bolster provides counterpressure during the discectomy and cage placement and minimizes patient movement, particularly during malleting maneuvers. Securely taping and anchoring the patient is critical for stabilizing the patient throughout the procedure. The tape is secured at the lateral chest and hip to help mobilize the ribs cranially and the iliac crest caudally to open the working corridor (Figure 4).

Patient positioning for prone lateral transpsoas approach. (A) Lateral view during prone lateral positioning. (B) View from above prone lateral positioning with bedside breaking for surgical approach. The participants and all identifiable individuals consented to the publication of their images. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Results
Operative Procedure
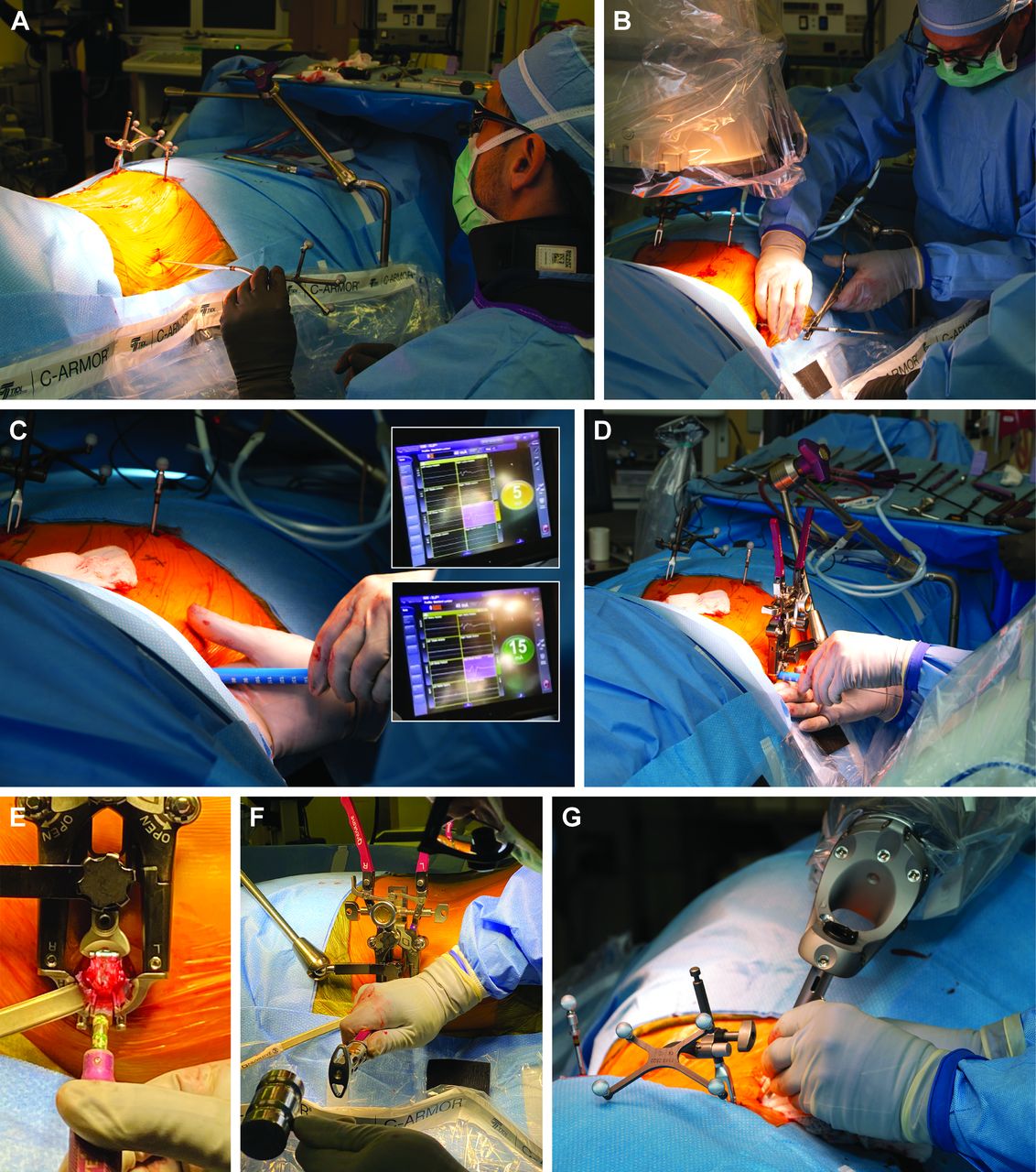
Fluoroscopy is used to plan the lateral incision. In planning the lateral skin marking, lateral and anteroposterior radiographs centered over the target disc space are taken. A line parallel to the desired disc space is marked on the skin and drawn through the center of the disc space based on lateral radiographs. This line is parallel to the angle of the endplates above and below. The length of the disc space is marked on the skin. In cases of multilevel PTP surgery, an oblique incision allowing access to the desired disc spaces can be used. The skin incision is sharply made, and electrocautery is used to dissect down to the muscle (Figure 5). Once the external obliques are in view, the muscles are bluntly spread to gain access to the retroperitoneal space. Dissection is done carefully with direct visualization to ensure that the peritoneum is not violated. Dissection down to the psoas is more challenging with the patient in the prone position than in the lateral decubitus position due to the increased distance between the skin incision and the spine. When the patient is prone, the abdomen hangs freely to minimize this working distance, alleviate abdominal pressure, and shorten the operative corridor. An assistant’s counterpressure to the contralateral side is beneficial to minimize this working distance. The index finger is used to palpate the quadratus lumborum and transverse process in a dorsally sweeping motion. Gravity aids in sweeping the peritoneum and its contents ventrally, establishing a safe working corridor to the psoas. At the L4 to L5 levels, the high iliac crest can obstruct access, especially in patients with a narrow intercrestal window; therefore, a specialized bed with chest and pelvic bolsters that can rotate in the prone position is preferred to help move the iliac crest away from the working corridor when accessing L4 to L5.

Operative steps. (A) The patient is placed in the prone position, and the surgeon is seated. (B) The initial dilator is placed. (C) Sequential dilation is performed. (D) A retractor is placed over the dilator. (E) The disc space is visualized, and a discectomy is performed. (F) The interbody cage is placed after discectomy and endplate preparation. (G) Pedicle screws are placed using computed tomographic navigation and robotic assistance. The participants and all identifiable individuals consented to the publication of their images. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
After palpating and identifying the psoas muscle, a dilator is placed through the flank incision and docked onto the surface of the muscle. Care is always used when advancing an instrument into the incision. The operative assistant passes all instruments dorsally to the surgeon’s finger, using the finger as a blunt guide from the incision to the psoas to minimize the risk of accidental peritoneal or bowel harm. Fluoroscopy is used to visualize docking to the disc space, aiming to dock two-thirds of the distance from the posterior border of the disc space. The initial dilator is advanced through the muscle, and the depth is determined to facilitate constructing the retractor system using appropriately sized blades. Triggered electromyography (t-EMG) confirms the correct anterior and posterior EMG thresholds. Generally, t-EMG thresholds for responses below 5 mA indicate direct contact with the nerve. In contrast, thresholds from 5 to 10 mA suggest proximity to the nerve, and those ≥11 mA imply a safer distance from the plexus. The dilator is translated posteriorly under t-EMG monitoring, targeting a position within the disc that is one-third from the posterior border of the disc space. Maintaining a strictly horizontal position of the dilator is crucial for creating an access corridor orthogonal to the spine, ensuring a safe working trajectory. A Kirschner wire (K-wire) is then inserted through the dilator into the disc space, followed by sequential placement of larger dilators, all while monitoring t-EMG to monitor for lumbar plexus traction and consequent signal changes.
After serial dilation, a retractor is placed over the final dilator. Care is taken to prevent the retractor from anterior migration due to gravitational forces and the weight of the soft tissue on the retractor. The retractor is affixed to the table with an articulating arm attached to the contralateral side of the bed. The retractor must be orthogonal to the disc space and parallel to the floor. The dilators are removed without displacing the K-wire, and the surgical corridor is visually inspected to ensure that the K-wire is centered in the retractor. t-EMG stimulates the posterior blade, ensuring low posterior EMG readings. A posterior shim is inserted into the disc space, and the retractor is gently opened to use a stimulating probe, confirming the absence of nerve tissue within the exposure. After removing the K-wire and placing retractor lights, a shim is placed in the posterior retractor blade to anchor the posterior margin of the retractor. A rounded anterior shim is then placed in the anterior retractor blade, the anterior retractor blade is opened, and the shim is secured. A safe anteroposterior working corridor within the disc space is established. Once the retractor is securely positioned and anchored with a shim, the bed can be rotated up to 10° away from the surgeon.
An annulotomy is performed using an 11 blade, with the annulus and underlying disc removed using a pituitary rongeur. A Cobb elevator is preferred for dissecting the disc along the endplates, ensuring the disc is released without violating the endplates to minimize the risk of subsidence. Fluoroscopy guides the appropriate depth of the Cobb elevator. Sequential trials are used to size the disc space. The remaining disc material is extracted using a combination of tools, including a box chisel, rasp, and ring curettes. Concurrently with endplate preparation, the interbody cage is packed with allograft material and prepared. After the disc is removed and the endplates are prepared, the graft is malleted into position under fluoroscopic guidance. Retaining an anterior annulus or anterior longitudinal ligament (ALL) cuff is essential to minimize the risk of ALL rupture. The final position of the implant is confirmed using fluoroscopy, and the retractor is removed, allowing direct visualization of the psoas. Hemostasis of the psoas under direct visualization while the retractors are slowly removed is achieved to minimize the risk of postoperative psoas hematoma. Following standard closure of the flank incision, posterior pedicle screws are placed using traditional minimally invasive approaches with a Wiltse incision.
Intraoperative Monitoring
Avoiding lumbar plexus injury remains a primary concern during transpsoas approaches.13 Intraoperative monitoring has been essential for minimizing lumbar plexus injury and reducing the incidence of neurological complications from 30% to less than 1% since its implementation.13,14 The prone position allows the hips to be neutral or extended, lengthening the psoas muscle and drawing the plexus posteriorly to avoid nerve injury. With each dilator placement, unidirectional t-EMG is used for stimulation in anterior–posterior, cranial, and caudal directions to assess proximity to the nerve. The initial dilator should be readjusted if the threshold is 10 mA or less to position the nerve safely behind the retractor. The threshold gradient from posterior to anterior of the dilator is critical in guiding safe placement anterior to the plexus. Somatosensory evoked potentials are now incorporated as an additional neuromonitoring modality alongside t-EMG. Although changes in somatosensory evoked potential have proven useful in identifying patients at risk for postoperative weakness, larger studies are needed to validate this approach for PTP lateral interbody fusion (LIF).
Intraoperative Navigation of the Interbody
CT navigation in PTP LIF can assist with incision planning, disc preparation, and interbody placement.15,16 However, navigation should not be used in place of fluoroscopy. The standard of care for PTP LIF continues to be fluoroscopy guidance. The major limitation in using navigation for interbody cage placement, as noted by the senior author, is the inability to verify the accuracy of the navigation system. Bony landmarks can be employed in open posterior approaches to confirm navigation system accuracy. However, the absence of internal reference points or bony landmarks in PTP LIF complicates the confirmation of navigation accuracy.17,18 Figure 5 exemplifies the operative procedure of the PTP approach.
Discussion
Technical Pearls
Surgeons should anticipate a steep learning curve when transitioning to the PTP LIF technique. PTP LIF has unique technical nuances and complications that distinguish it from conventional methods performed with the patient in the lateral decubitus position. The following technical pearls aim to streamline the learning process, enhance surgical workflow, and reduce the risk of complications specific to PTP LIF (Figures 6 and 7).

Illustration exemplifying intraoperative monitoring and retractor positioning for the prone transpsoas approach. (A) The initial dilator is placed. (B) Sequential dilation is performed. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.

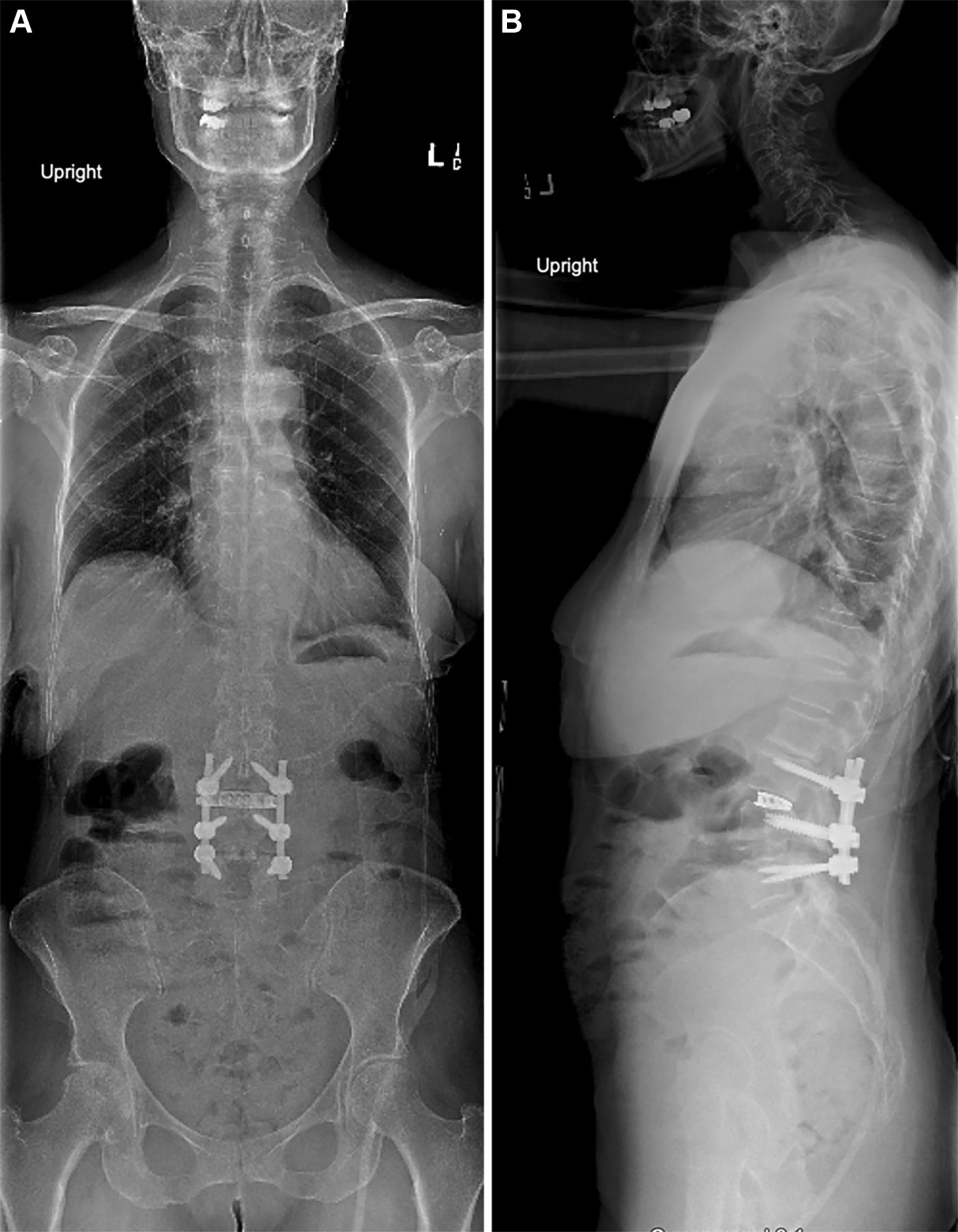
Postoperative (A) coronal and (B) sagittal standing radiographs after the prone transpsoas approach for previous lumbar fusion extension. The participants and all identifiable individuals consented to the publication of their images. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Surgical Ergonomics
Once surgeons become accustomed to the PTP LIF procedure, they can rotate the bed up to 10° away from themselves after docking the retractor. This adjustment improves ergonomics in the prone position by reducing the required neck extension for optimal visualization along the surgical corridor created by the retractor system. Appropriate contralateral bolsters are necessary to ensure patient stability during this maneuver. The surgeon should also position themselves orthogonal to the retractor handles to accommodate the bed’s rotation. An assistant positioned at the foot of the bed can confirm that the correct working angle is maintained. Obtaining ideal anteroposterior and lateral fluoroscopy images with the patient in the prone position can be challenging, especially with the bed rotated. Proper adjustments in patient positioning and optimization of the fluoroscope C-arm angle are essential to facilitate accurate implant placement and prevent complications. Returning the bed to a neutral position during interbody placement may be beneficial. Intraoperative navigation and adjusting the surgical table for better alignment can address these challenges.
Soft Tissue and Surgical Corridor
Accessing the disc space via a lateral approach necessitates placing the retractor within the retroperitoneal corridor. When the retractor is opened, retroperitoneal fat can creep between the blades, obscuring the surgical view and heightening the risk of complications. A strip of Ioban drape (3M) should be cut to the length of the retractor blades and placed circumferentially over the partially opened blades to mitigate this issue. Applying mineral oil to the adhesive side of the Ioban minimizes self-adhesion, creating a barrier that separates retroperitoneal soft tissue from the surgical corridor.
Retractor Positioning and Migration
Surgeons often dock the retractor more anteriorly than less during PTP LIF because gravity pulls the instrumentation ventrally, and the prone position shifts the lumbar plexus posteriorly. Awareness of this difference is critical, as it increases the risk of unintentional ALL rupture or injury to the great vessels.19 The mechanism for inadvertent ALL rupture is likely linked to ventral interbody placement within the disc space due to prone positioning and the gravitational effects on the retractor system. Continuous reassessment of the retractor’s position throughout discectomy, endplate preparation, and interbody selection trial is essential. A lateral interbody plate can provide additional stability if an ALL rupture occurs.20
Medial and lateral forces applied during discectomy and interbody placement may dislodge the retractor from its intended position by losing contact with the spine or migrating ventrally during the discectomy. Therefore, monitoring and correcting the retractor’s position is crucial for maintaining a safe working corridor.21 Ventral migration, particularly during discectomy, raises the risk of ALL and great vessel injury. An ALL retractor or anterior blade and posterior blade shims can help prevent retractor migration and ensure adequate visualization throughout the procedure.22
Appropriate counterpressure to the retractor system should be applied during maneuvers that exert high medial-lateral forces to avoid dislodgement and displacement, especially when using discectomy tools or malleting to deploy the interbody.23
Retractor Time
Femoral nerve injury is a serious complication associated with PTP LIF, particularly at the PTP approach. The risk of lumbar plexus injury escalates with prolonged retractor placement. Neurological injuries following LLIF procedures often result from neurapraxia due to extended retractor time. Minimizing retraction duration is critical to reduce the risk to the lumbar plexus and avoid postoperative symptomatic neuropraxia. The target is approximately 15 minutes of retraction time per level, though achieving this can be challenging during the initial learning phase.24 Periodically releasing the retractor can help mitigate the risk of lumbar plexus injury (Figure 6).
Cage Size and Subsidence
The lateral approach allows the placement of large interbody grafts that span the apophyseal ring on both sides to maximize structural support and minimize the risk of cage subsidence into adjacent vertebral bodies.22 Subsidence can lead to loss of disc height, segmental lordosis, and diminished indirect decompression, increasing the likelihood of reoperation. Although PTP LIF aims for indirect foraminal decompression, surgeons should avoid “oversizing” the interbody graft, as this can raise the risk of subsidence.23 We recommend using cages with a minimum width of 22 mm to help minimize subsidence risk. In cases of spondylolisthesis at the target level, an 18-mm cage is often used, given the decreased overlapping surface area between the 2 vertebral bodies.
Conclusion
PTP LIF is a nuanced technique that presents a viable alternative to traditional LLIF with the patient in the lateral decubitus position for the PTP approach. The advantages of this single-position technique include facilitating segmental lordosis, eliminating the need for repositioning for posterior instrumentation, and allowing access for posterior decompression. While PTP LIF can be effective and efficient, navigating this approach entails overcoming certain challenges. The reviewed technical pearls can assist surgeons in overcoming the initial learning curve while enhancing ergonomics, surgical workflow, and overall safety.
Acknowledgments
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures J.S.U. receives royalties from NuVasive Medical, Inc., consulting fees and royalties from SI-BONE, Inc., and consulting fees from Aclarion, Misonix, Inc., Viseon, ATEC Spine, Inc., and Mainstay Medical, Inc. The remaining authors have nothing to report.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.