


Abstract
Background Endoscopic spine surgery is a minimally invasive approach that offers several advantages over the traditional open approach, including less tissue trauma, faster recovery, and lower rates of complications. However, the learning curve and the requirement of separate equipment limits the acceptability of this technique for many spine surgeons. Using a short survey, the authors sought to report the current status regarding the use of endoscopy among French spine surgeons and to identify the barriers faced by spine surgeons to adopting endoscopy into their practice.
Methods A cross-sectional survey was conducted in which a predefined questionnaire was sent as a Google form to 522 members of the Societe Francaise de Chirurgie du Rachisspine. Respondents were asked to respond within 3 months, with reminders sent regularly to nonresponders. Responses were collected and analyzed.
Results Among all 123 survey respondents, 39 practiced endoscopy and 84 did not practice endoscopy. Most of the surgeons acquired skills by visiting other surgeons (74.4%) or attending cadaver-based workshops (56.4%). A substantial portion of respondents were in between 1 and 3 years of experience (48.7%) and performed 5 to 10 endoscopic procedures per month(30.8%). Although 92.1% of respondents observed better outcomes in their patients with endoscopy, lack of training (26%) and high equipment cost (13.8%) were the most limiting factors reported by surgeons.
Conclusion The results of this survey contribute to the existing literature and highlight the current trends of endoscopic spine surgery in France. Although the benefits of minimally invasive spine surgery are well documented and were confirmed by surgeons in this survey, lack of training and cost of equipment are major barriers that need to be controlled to expand the adoption of this technique.
Clinical Relevance Understanding the factors influencing the adoption of endoscopic spine surgery in France provides valuable insights for surgeons and educators. By identifying key barriers and motivations, this study may help guide strategies for improving training, accessibility, and implementation of endoscopic techniques in spinal surgery.
Level of Evidence 4.
- endoscopic spine surgery
- minimally invasive spine surgery
- spine surgery
- transforaminal approach
- biportal endoscopy
- uniportal endoscopy
- full endoscopy
- endoscopic discectomy
Introduction
Endoscopic technique in spine surgery has grown significant popularity over the past decade. The advent of endoscopic spine surgery has provided potential benefits to patients, such as shorter hospital stays, faster recovery, reduced postoperative pain, and less disruption of muscle and soft tissues.1 Even with many advantages over traditional approaches, endoscopic spine surgery is limited by its steep learning curve, technical limitations, and financial constraints.2 Apart from these limitations, it is also challenged by the need for specialized equipment and its access in complex and revision cases. Additionally, patient selection plays a critical role in determining successful outcomes, further complicating its widespread acceptance.
In 1993, the “Destandau” endospine technique was introduced by a neurosurgeon in France.3,4 It has been largely employed worldwide for patients with lumbar disc herniation and lumbar spinal stenosis with favorable outcomes.5–7 Since then, endoscopic spine surgery has increased in France, and many surgeons are routinely practicing it to give better outcomes to their patients. However, although its use has increased, adoption by surgeons is still slow due to the associated limitations of the technique. Therefore, we conducted a survey to report the status of endoscopic spine surgery use in France, the challenges faced by spine surgeons, and overall surgeon satisfaction with the procedure.
Given the importance of the endoscopic technique in the advancement of minimally invasive spine surgery, understanding the overall experience and limitations of a surgeon is crucial. This survey may potentially have important implications for formulating future guidelines about endoscopic spine surgery in France.
Methods
Study Design
A survey was designed to capture comprehensive data regarding the use of endoscopy in spine surgery, focusing on key areas like frequency of use, type of endoscopic procedure used, perceived benefits and limitations, and training sources. A mixed-method approach was used, including multiple-choice questions and open responses to allow for both quantitative and qualitative analysis.
The questionnaire was developed by spine surgeons from the spine unit at Center Orthopedique Santy-Lyon in collaboration with experts in the field. It consisted of 2 separate surveys: 1 designed for surgeons who practice endoscopic spine surgery and a second survey for surgeons who do not (Table 1). Spine surgeons not practicing endoscopy were targeted to gain more knowledge about its limitations. Both surveys covered various aspects of the technique.
Questionnaire distributed to spine surgeons.
Participants
The survey targeted a sample of spine surgeons in France across various geographic regions. The survey was distributed electronically via Google forms to 522 members of the Societe Francaise de Chirurgie du Rachis. All surgeons were included irrespective of their experience. Participation was voluntary, and responses were collected anonymously. The survey remained open for 3 months, during which reminder emails were sent at regular predetermined intervals.
Data Collection and Analysis
Descriptive statistics were used to analyze the quantitative responses, with percentages and frequencies reported for key variables such as the percentage of cases utilizing endoscopy, types of procedures, and satisfaction levels. Qualitative analysis was performed for open-ended responses to identify common themes regarding challenges, benefits, and barriers to wider adoption.
Results
Participant Demographics
The survey was sent to 522 spine surgeons, of whom 123 surgeons participated with complete responses for a 24% response rate. Among the respondents, 39 surgeons (31.7%) practiced endoscopic spine surgery regularly (user group), and 84 surgeons (68.3%) did not (nonuser group). Although the geographic details of the respondents were not collected, 35 surgeons (89.7%) in the user group and 70 (83.3%) in nonusers group practiced in private hospitals. The rest of the surgeons worked in the public sector. Most of the surgeons who participated in the survey were orthopedic surgeons (n = 82, 66.7%).
Usage Pattern
A wide variation in the usage pattern was observed. A majority of surgeons using endoscopy gained experience by visiting other experienced surgeons (74.4%) or attending cadaver-based workshops (56.4%). Along with these resources, all of them were involved in regular reading and learning by beginning the procedure at their practice. In the user group, a large number of surgeons were using endoscopy for 1 to 3 years of their practice (n = 19, 48.7%). The distribution of experience is shown in Figure 1. In addition to this, 10 surgeons (26.3%) reported using endoscopy for 25% to 50% of their practice in spine surgery. Interestingly, 4 surgeons reported using endoscopic spine surgery in 100% of their cases.

Experience of surgeons in endoscopy.
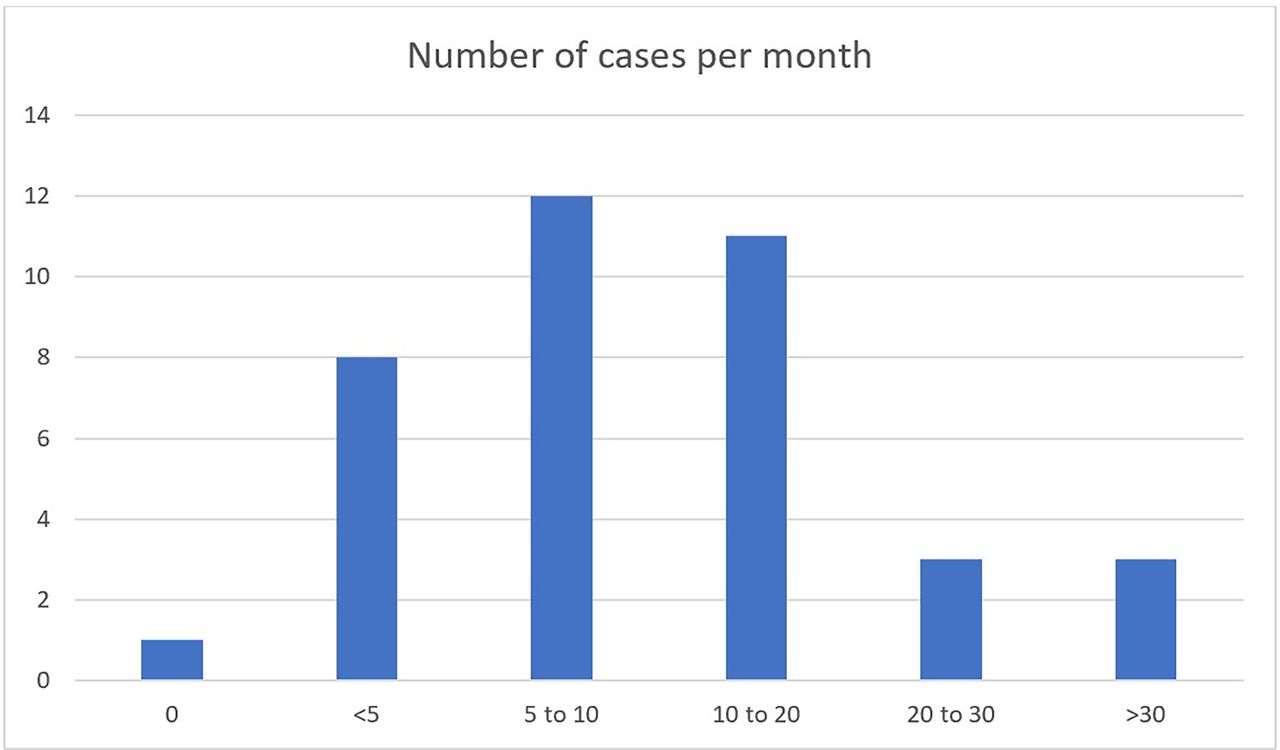
Looking at the monthly volume of cases performed by surgeons, 12 surgeons perform endoscopic spine surgery on 5 to 10 patients per month, whereas 3 surgeons perform it for >30 cases per month. One surgeon responded with 0 cases per month due to inconsistent use of endoscopy, and we instructed them to respond to this based on their last 3 months of practice. Figure 2 depicts the volume of cases performed by the surgeons.
Depending on their training, the respondents perform mixed approaches for endoscopy. Interlaminar approaches were reported by most of the respondents (n = 36; 97.3%). On the other hand, lumbar fusion surgery by endoscopy was reported by only 5 respondents (13.5%). The details of other approaches are given in Table 2. Most of the surgeons use biportal endoscopy (n = 28, 73.7%), a few of use uniportal (n = 16, 42.1%), and endospine is used by only 1 surgeon. The majority of surgeons (n = 33; 91.7%), perform their procedure using general anesthesia, 2.8% (n = 1) use local anesthesia, and the remaining 5.6% (n = 2) use both, depending on the case.

Volume of endoscopic spine surgery cases performed per month by spine surgeons in France.
Different approaches used for endoscopy by spine surgeons in France (n = 39).
Benefits and Satisfaction
Despite the challenges, a significant number of surgeons agreed to the benefits associated with endoscopic spine surgery. Most of the surgeons (n = 29, 78.4%) started this practice because they were convinced about its clinical benefits to the patients. However, a close number of surgeons (n = 23, 62.2%) started because of technical curiosity. Eight respondents (21.6%) believed using endoscopy has helped them to recruit more patients.
Looking at their perspective after starting endoscopy, 35 surgeons (92.1%) found clinical benefits in relation to their patients. However, 3 surgeons (7.9%), practicing endoscopy regularly, believed that it does not provide any extra benefits to the patients when compared with traditional open techniques. The observed advantages over the open technique response included reduced postoperative pain, early recovery, better patient outcomes, and reduced complications. The surgeons even mentioned better visualization of anatomic structures with the help of endoscopy.
Challenges and Barriers
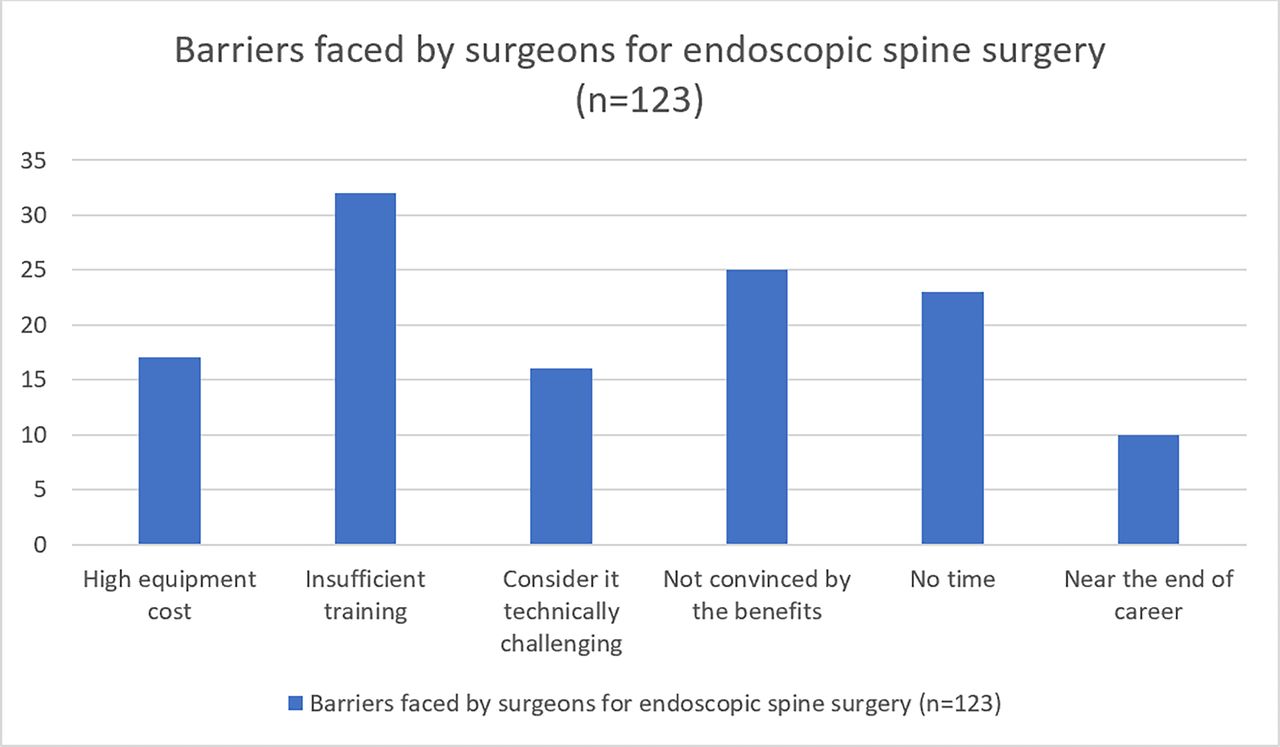
Most of the users (n = 17, 43.6%) of endoscopy reported the high cost of the equipment as the major barrier to expanding their practice in endoscopy. Insufficient training (n = 16, 41%) and lack of appropriate scientific evidence (n = 15, 38.5%) were also been considered to be barriers. When the nonusers’ responses were evaluated, we found the majority (n = 30, 38%) were not convinced with the benefits as the major reason for not using endoscopic spine surgery. There were surgeons (n = 4, 5.1%) who believed endoscopy was too difficult to learn, and a group of surgeons (n = 23, 29.1%) reported no time to learn any new technique. Additionally, 65.8% (n = 25) of surgeons using endoscopy believe their operating time has increased compared with if they do the same with open technique. The barriers are shown in Figure 3 with both groups of surgeons.

Barriers faced by surgeons for the usage of endoscopy in spine surgery.
Discussion
The results of this survey provide valuable insight into the current state of endoscopic spine surgery in routine practice among spine surgeons in France. While a substantial number of surgeons have incorporated it into their practice, challenges, such as learning curves and financial barriers, have limited its widespread adoption. The fact that most of the surgeons are in the early phase of their experience (1–3 years), endoscopy will become more prevalent as these surgeons gain experience and influence the field.
Although the history of endoscopic spine surgery is approximately 30 years old,3,4,8 it has gained popularity among spine surgeons over the past few years. Surgeons have shown a willingness to learn, which can be appreciated in the survey responses. Most of the surgeons are in an early phase of experience, and there are surgeons who have been doing 100% of their cases using endoscopy. These findings suggest a rising trend of adoption and align with the advantages of endoscopy over open technique.9
Most of the usage of endoscopy and related research work originated in China and South Korea.10 Native surgeons would be inclined more toward this technique due to easier availability of training, and this, in turn, is responsible for higher usage of endoscopy in these countries. Thus, there is a geographical disadvantage to France, leading to insufficient training as a major barrier, as also seen in our survey. The second most common limitation was that the surgeons were not convinced of the benefits associated with endoscopic spine surgery. However, according to the available current literature, the advantages strongly supported are less tissue destruction and muscle trauma, reduced blood loss, less damage to the epidural blood supply and consequent epidural fibrosis and scarring, reduced hospital stay, early functional recovery, improvement in the quality of life, and better cosmesis.11,12 Apart from these aspects, the surgery can be performed on a day-care basis, and the complication rates are low, which, in turn, reduces the financial burden.13 Although we expect a contradictory response from surgeons not using endoscopy, we noticed 3 respondents from the user group mentioning no added benefit of endoscopy over open technique. These surgeons did notice an increase in surgical time and no difference in patient recovery. Due to the anonymity of the responses, we could not find the other responses of these surgeons, but we assume these surgeons must be the ones who have less experience and perform fewer cases per month. Fleiderman et al14 looked at the learning curve in 41 cases of transforaminal endoscopic lumbar discectomy. For the initial 20 cases, the mean operating time was 114 minutes, and it reduced to 80 minutes in the next 21 cases. They had a 17% incidence of recurrent disc herniation; however, the interesting finding to note here is that the last recurrence was observed in the 23rd case. Thereafter, for the next 18 cases, no recurrence was observed. Therefore, they concluded that at least 20 cases were to be operated initially to observe a significant reduction in operating time and complications.
It is interesting to note that only 67.6% of endoscopic users in France perform the transforaminal approach, compared with 92.5% of users in Australia.15 This is likely related to the overrepresentation of biportal endoscopy compared with the uniportal technique among endoscopic spine surgery users in France. We find this particularly surprising, as we consider the transforaminal approach to be a game changer in the latest endoscopic spine surgery techniques.
Another major barrier that needs separate mention is high equipment cost. We observed that more than 80% of the respondents are practicing in a private setup, where there is no financial support available by the government. Therefore, the cost becomes the major deciding factor in the treatment of patients. Manabe et al16 looked at the cost of endoscopic surgery in Japan in association with the amount reimbursed to the hospital. They observed that the hospital is not adequately reimbursed for the surgery, and the major burden is due to equipment costs. Similarly, Wu17 mentioned equipment cost as 1 of the major challenges, even if the surgeon is a well-trained endoscopic spine surgeon. This scenario is similar for every minimally invasive spine surgery. The surgery can only be cost-effective if the improvement in patients is durable, thereby reducing the overall financial burden.18 The rest of the constraints observed in our respondents were lack of time for training due to ongoing busy practices, and few surgeons are near retirement, which makes them less motivated to acquire new skills.
The indications of endoscopic spine surgery are still expanding. The procedure started with lumbar discectomy and is now also being used for lumbar interbody fusion, cervical disc herniation, and thoracic disc herniation.19 A similar trend was observed in our survey, where few surgeons are performing thoracic discectomy and lumbar fusion procedures regularly. The implications of the wider adoption of endoscopic techniques in spine surgery are significant. As more surgeons become proficient in these methods, the potential for improved patient outcomes and reduced healthcare costs increases. However, addressing the barriers to adoption, particularly in regions where reimbursement and equipment costs pose challenges, will be critical to ensuring that more patients can benefit from these minimally invasive approaches.
It is important to acknowledge the limitations of the study. First, the number of surgeons who responded is small. Therefore, the findings cannot be generalized to the whole population. Second, there is potential response bias, as the surgeons trained and performing endoscopy regularly are more like to respond in favor compared with surgeons not trained. Even with these limitations, the findings of the survey highlight the current status of endoscopic spine surgery in France and are worth mentioning.
Conclusion
This survey of spine surgeons provides important insights into the current usage patterns, benefits, and challenges associated with endoscopic spine surgery among surgeons in France. While endoscopy offers numerous advantages, its widespread usage is hindered by training difficulties and equipment costs.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.