


Abstract
Background One of the common complications of adult spinal deformity (ASD) correction is the failure to relieve pain. This may result from the failure of implanted hardware to provide adequate stabilization. While numerous studies exist, characterizing complications that can occur with minimally invasive correction of ASD and data regarding hardware failure in this setting are limited.
Objective This article characterizes the rate and mode of posterior hardware failure in the setting of circumferential minimally invasive surgery (CMIS) for ASD correction.
Methods Patients undergoing staged CMIS correction of ASD from January 2007 to September 2018 were identified. Patients with a minimum 2-year follow-up were included in the study.
Result A total of 263 patients (168 women and 95 men) were included in the study. The mean age of patients was 64 years (21–85, SD 13.7), and the mean length of follow-up was 90 months (24–164, SD 40.2). An average of 6 levels (3–16, SD 3.15) was fused per patient.
Eight patients had a mechanical hardware failure and required revision surgery (3.04%). No catastrophic failures were noted in our series. Hardware failures were characterized as follows: 2 patients with broken screws, 5 patients with loose screws, and 1 patient who had symptomatic T12-L1 and L5-S1 nonunion with bilateral distal rod fractures, iliac set screw loosening, and proximal T12 screw loosening. Following revision surgery, all of these patients had confirmed solid fusion on computed tomography (CT) scan at their latest follow-up visit.
Interestingly, 3 other patients had loosening of the set screw on their iliac bolts. Five patients had rod fractures between L5 and S1 or below S1. All 8 of these patients were asymptomatic with confirmed fusion at L5-S1 on CT scans.
Conclusion The prevalence of clinically significant hardware failure needing revision in our series was low at 3.04%. Symptomatic hardware prominence requiring revision was 2.3%. Specifically, rod fractures were not common (2.2%). Our study suggests that in the appropriately selected patient, CMIS to correct ASD without osteotomies may result in acceptable rates of hardware failure. Future studies should compare the results of CMIS deformity correction to a matched population of patients undergoing open deformity correction.
Clinical Relevance This study suggests that in the appropriately selected patient, CMIS to correct ASD without osteotomies may result in acceptable rates of hardware failure.
Level of Evidence 4.
Introduction
Recent estimates place the prevalence of adult spinal deformity (ASD) at upward of 60%. While only a small proportion of these individuals ultimately become symptomatic, associated pain may be quite severe,1,2 resulting in significant dysfunction and debility.3 Subsequently, ASD has been associated with very poor health-related quality of life measures.1,4 With an aging population and with spinal fusions becoming more commonplace, the burden of ASD on our society appears to be only increasing.
Fortunately, ASD correction has been proven to substantially improve outcomes in well-selected patients.2,5 However, traditional open deformity corrective surgery comes with a high cost of potential morbidity with rates of all-cause complications as high as 86%6–8 and a rate of major complications of up to 18.5%.6 Notably, the rate of postoperative hardware failure can also be quite high and is now a leading cause of revision surgery in this patient population.9 Rod fractures alone have an incidence of 18.4% in this surgical setting10 with even higher rates noted in patients undergoing 3-column osteotomies.11
Consequently, in the past decade, minimally invasive techniques have been incorporated into the surgical management of spinal deformity as a potential mitigation strategy for these obstacles. While supportive data are somewhat limited, the results published to date have nonetheless been quite favorable. Minimally invasive surgery (MIS) for deformity correction has been associated with decreased blood loss,12–18 potentially quicker operative times,13,14 and shorter hospital lengths of stay.14,18 Furthermore, all-cause complications may additionally be less frequent with circumferential minimally invasive surgery (CMIS) for deformity correction.15,17,19,20
Failure of implanted hardware to provide adequate stabilization is a potential source of significant postoperative debility,10 and despite emerging data supporting the clinical efficacy of CMIS, the rate of hardware failure in this patient population has not been well defined.21 Thus, the purpose of this study was to characterize the rate and mode of posterior hardware failure in patients undergoing CMIS for ASD correction.
Material and Methods
Patient Data
This was a retrospective review of a prospectively collected data registry of 358 patients who underwent CMIS correction of ASD from January 2007 to September 2018. ASD was defined utilizing the following parameters: a Cobb angle >20 or sagittal vertical axis (SVA) >50 mm or a pelvic incidence/lumbar lordosis (LL) mismatch >10°. Of the patients identified, 281 patients had undergone CMIS correction of ASD at 3 or more levels for severe back pain with or without radicular pain that had been recalcitrant to extensive conservative management for at least 6 months. Only patients with a minimum clinical and radiographic follow-up of 2 years were included in the analysis (N = 263). Informed consent was obtained from all patients. Institutional Review Board approval from Cedars Sinai was obtained for this study (IRB no. Pro00015483).
All patient demographic information was collected. Patient comorbidities were additionally noted. Radiographic parameters including thoracic kyphosis, LL, pelvic tilt, PI, SVA, and coronal balance were measured preoperatively, 3 months postoperatively, and at latest follow-up utilizing full-length 36″ standing films. PI-LL was additionally calculated off preoperative and postoperative images. Postoperatively, any hardware-related complications including loosening, fracture of instrumentation, or symptomatic hardware were noted based on detailed review of each postoperative radiograph and/or computed tomography (CT) image, which was routinely performed from 2011 at 18 months to 2 years to assess fusion. All patients with radiographic evidence of hardware failure had a CT image to assess for underlying fusion.
Patient-reported outcome measures including the visual analog score, treatment intensity score,22 Oswestry Disability Index, Short Form-36 survey, and the Scoliosis Research Society-22 item survey were collected preoperatively, at 1 year, and at latest follow-up.
CMIS Protocol
The CMIS protocol and its evolution over time have previously been described23 and are outlined here. Under the CMIS protocol, patients with identified ASD underwent 2-staged deformity correction with an intervening 3-day interval. The old protocol was executed as follows: Stage 1, multilevel lateral lumbar interbody fusions and Stage 2, axial lumbar interbody fusion (AxiaLIF) at L5-S1 as needed with subsequent MIS posterior pedicle screw fixation with rod contouring and derotation/translation. The new protocol was instituted in May 2011 and was executed accordingly: Stage 1, multilevel oblique lateral lumbar interbody fusion and MIS L5-S1 oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF) and Stage 2, MIS pedicle screws with rod contouring and derotation/translation. For both protocols, 5.5-mm titanium alloy rods were utilized. Posterior segmental “pars-facet-pars” fusions were done at those segments that did not have an interbody fusion. These were usually proximal to the L1-L2 segment. No patient had any facet resection or any grade of posterior column osteotomy or an anterior column realignment procedure other than at L5-S1 where an ALIF would require release of the anterior longitudinal ligament.
On postoperative day 2 following Stage 1, a standing radiograph was obtained, and patients were subsequently mobilized. Any persistence of radicular pain or neurogenic claudication was noted during this time, and sagittal alignment was reassessed using plain radiography. These data were then utilized to plan for the second stage accordingly including the need for additional posterior decompression, if needed. After Stage 1, only 4 patients needed a posterior microdecompression due to persistent radiculopathy.
Also, as part of the protocol, all patients had magnetic resonance imaging besides full-length standing radiographs preoperatively. The feasibility of CMIS techniques was assessed by studying anatomical corridors and vascular anatomy. CT was performed if any doubt exists of a segmental fusion or facet fusion. Dual-energy x-ray absorptiometry was also performed to document bone density. If the dual-energy x-ray absorptiometry T score was less than 3.0, minimally invasive surgical correction was deferred. If T score was between 2.0 and 3.0, daily injection of teriparatide (Forteo) was recommended and continued for 1 year after surgery.
Statistical Analysis
Descriptive statistics were calculated with SDs and ranges. Patient characteristics for both groups were analyzed using χ 2 and student t tests. A χ 2 test was used for categorical variables, and an independent student t test was used to assess continuous variables. A P value of <0.05 was set as our measure of statistical significance.
Results
Patient Data
A total of 281 patients met the criteria to be included in this study. A total of 263 patients (168 women and 95 men) were available for review with minimum 2-year follow-up. The mean age of patients undergoing CMIS for spinal deformity correction was 64 years (SD 13.7). The mean length of follow-up was 90 months (SD 38.2). A total of 1686 levels were fused with an average of 6 levels fused (SD 3.1) per patient. Mean body mass index was 27 kg/m2 (SD 5.9). Patient clinical and radiographic outcomes are noted in Tables 1 and 2, respectively.
Clinical and functional outcomes.
Radiographic outcomes.
Hardware Failure
A total of 8 patients had mechanical hardware failure requiring revision surgery (3.04%). No catastrophic failures were noted in our series. Of the 8 patients with hardware failure, 4 were women and 4 were men. Hardware failures were characterized as follows: 2 patients with broken screws, 5 patients with loose screws, and 1 other patient who had symptomatic T12- L1 and L5-S1 nonunion with bilateral distal rod fractures, iliac set screw loosening, and proximal T12 screw loosening. Following revision surgery, all of these patients had confirmed solid fusion on CT scan by their latest follow-up visit.
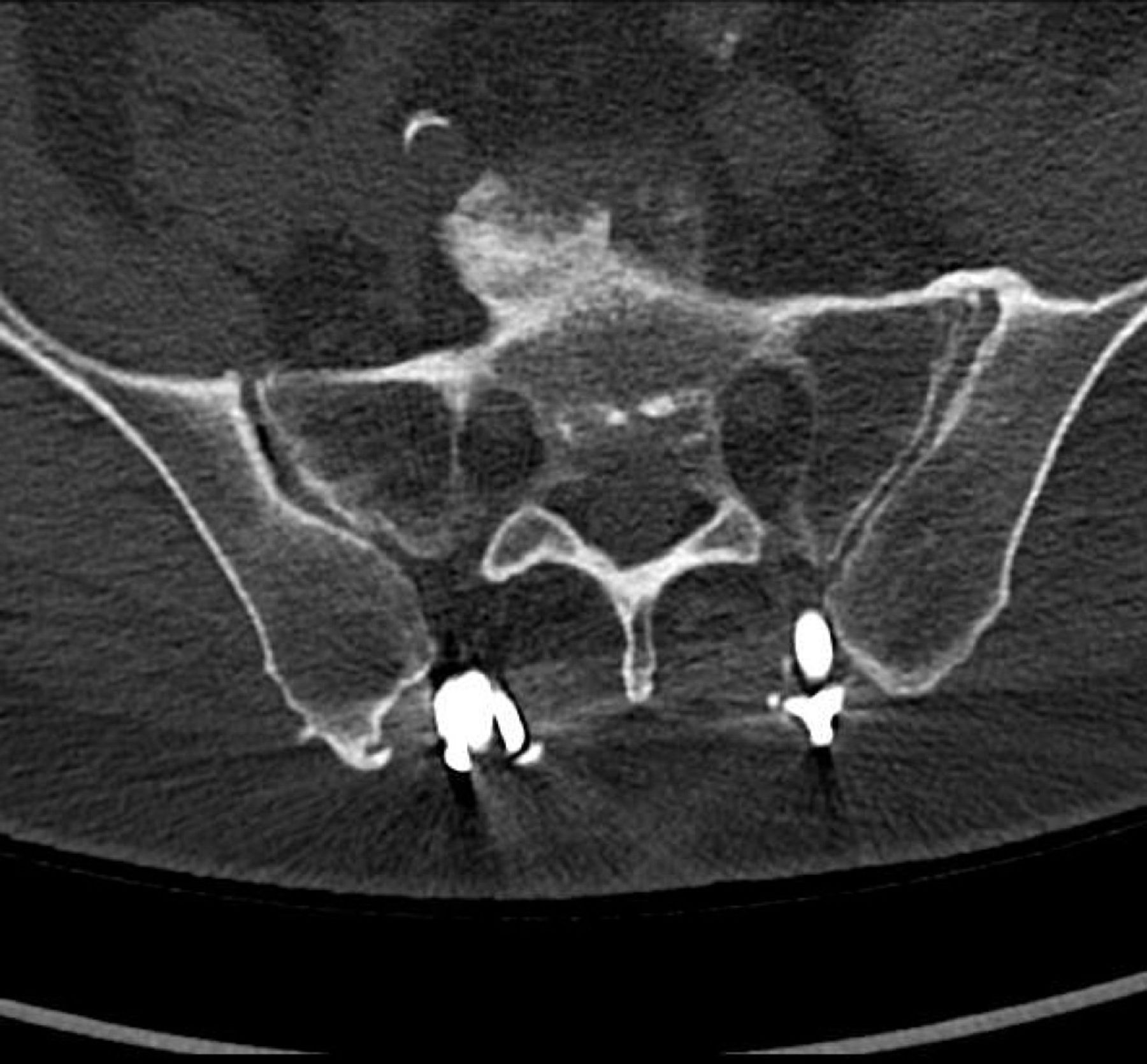
Interestingly, 3 other patients had set screw loosening of their iliac bolts (Figures 1 and 2). Five patients had rod fractures between L5 and S1 or below S1 (Figures 3 and 4). All 8 of these patients were asymptomatic with confirmed fusion at L5-S1 on CT scans. No catastrophic failures were noted (Table 3).

Anterior-posterior and lateral scoliosis films demonstrate rod fracture between L5 and S1, and below S1.

Corresponding sagittal computed tomography image demonstrates fusion at L5-S1.

Axial computed tomography image demonstrating absence of set screw in right iliac screw.

Axial computed tomography image demonstrating corresponding loosened set screw of empty iliac screw seen in Figure 3.
Hardware failure (21 patients)—2-y follow-up.
From a temporal standpoint, rod fractures were detected at varying times with 5 of the 6 patients totally asymptomatic and showing solid fusion on CT scan (Table 4). Six other patients had symptomatic hardware prominence that did need revision surgery. A further 5 patients had malpositioned screws that needed revision.
Rod fractures.
Of the 263 patients in the study, 8 had an lowest instrumented vertebra between T10 and T12, 4 between L1 and L3, 11 at L4, 63 at L5, and 177 at S1. Of 177 patients who had fusions spanning L5-S1, 70 had iliac screw fixation and 107 did not (Table 5). Of patients fused to the ilium, the mean number of levels fused was 9 levels (4–16). For those not fused to the ilium, the mean number of levels fused was 6 levels (3–15). Of patients not fused to L5-S1, there were only 3 hardware failures.
Failures with iliac screw vs no iliac screws.
Lumbosacral Fusion
There were 56 patients who had an AxiaLIF at L5-S1. There were 47 patients with ALIF at L5-S1 and 74 patients with OLIF at L5-S1. Out of all 23 hardware failures, 3 of the hardware failures occurred in 3 patients undergoing AxiaLIF (2 with sacral screw loosenings and 1 proximal hardware prominence). The failure rate of the AxiaLIF fixation screw has been previously reported, and we have strongly recommended in prior publications not to use AxiaLIF as a means of stabilizing L5-S1 in the setting of a spinal deformity. We have not used AxiaLIF in our protocol since 2011.24–26
Discussion
A common complication following ASD correction is the failure of implanted hardware to provide adequate stabilization, which in turn is a source of significant postoperative morbidity and a common reason for revision surgery.10 While hardware failure in open surgical correction for ASD has been relatively well characterized,10,11,27 similar data in the setting of CMIS for ASD correction remain significantly limited. In our series, we found that with use of CMIS for ASD, the rate of all comers of hardware failure including hardware prominence was 8.7%. However, only 5.3% of patients required surgery. Excluding prominent symptomatic hardware, symptomatic mechanical hardware failure rate was 3.0%. This is in stark contrast to the high rates of hardware failure that have been cited in the setting of open deformity correction.10,11,27
Rod fracture has been cited as one of the most common reasons for revision spinal deformity surgery.10 Utilizing traditional open deformity corrective techniques, rates of rod fracture may approach 18.4%.10,11,27 With use of 3-column osteotomies, rates of rod fracture may be much higher (31.7%).11 In our series, the prevalence of actual rod fracture was quite low with only 6 patients of 263 experiencing the complication (2.2%). There may be several explanations for this. First, with the CMIS protocol, the use of multilevel interbody cages enables load sharing, and the use of ligamentotaxis enables creation of a physiological and harmonious restoration of LL. This minimizes the need for hyperacute bends in the rod, which have been linked to higher rates of rod failure.28 The lack of anterior column support around oft-used osteotomies in the setting of open deformity may also contribute to fatigue failure of rods in this setting.29 In comparison with our staged protocol for CMIS deformity correction, robust anterior column support and the absence of posterior-based osteotomies mitigate this latter risk. Additionally, staged correction with interval re-evaluation of sagittal alignment may allow for more optimal fine-tuning of sagittal parameters potentially further mitigating risk of overcorrection and early hardware failure.23 An important aspect of our technique is that rod contouring is smooth and graduated and only done in the sagittal plane. No coronal bends or in situ contouring, other than distally to seat the rod in the iliac screw, are created. Furthermore, bone density is an integral part of our preoperative workup before embarking on CMIS correction of ASD, and this may also explain the low hardware failure rate.30
Most importantly, all of the above collectively may explain the paradox of only a 2.2% rod fracture rate despite universal use of 5.5-mm titanium alloy rods. The latter has been associated with higher rates of fatigue failure in open spinal deformity correction.29,31,32 Rod fractures in our series only occurred distally, either between L5 and S1 or below S1. In order to seat the rod into the iliac screw in some patients, the use of in situ bending distal to the S1 screw was utilized. The focal hyperacute bend in the rod likely served as a localized stress riser leading to fatigue failure of the rod.28 Also noted in 4 patients was iliac bolt set screw loosening. We theorize that this may have been due to the direct inline attachment of the rod to the iliac screw. In this construct, increased repetitive stress at the set screw-rod interface may have caused the screw to slowly back out over time. This is in contrast to the more traditional iliac screw construct, which diffuses the aforementioned mechanical stresses through use of a side connector. Ultimately, while there was initial concern for underlying pseudarthrosis in these latter patients with rod fractures and iliac set screw loosening, 8 of these 9 patients were fortunately asymptomatic and needed no intervention. Furthermore, CT scans confirmed fusion at L5-S1 in all of these patients. Hence, we would caution against routine revision in these patients with set screw loosening or distal rod fractures. Prior publications have suggested that rod failure is associated with poorer health-related quality of life measures.10 Thus, CMIS may be an effective technique for ASD correction under the appropriate indications.
There were 6 patients with prominent, symptomatic hardware that needed revision (2.2%). Early on in our experience, we inadvertently left pedicle screws slightly prominent to facilitate subfascial passage of the rod. In 2 patients during rod reduction, the proximal screws did back out. In this setting, several of our very thin patients who were already predisposed to developing symptoms from hardware did develop symptoms.
It is important to note the rationale for transitioning from AxiaLIF to ALIF or OLIF at L5-S1 in our practice. While beyond the scope of this study, we found an unacceptably high number of pseudarthroses in patients undergoing AxiaLIF (6 patients in our series). Furthermore, we found that AxiaLIF was suboptimal at sagittal correction when compared to an ALIF.24 Consequently, we abandoned the use of AxiaLIF, since 2011, in favor of ALIF and OLIF at L5-S1.
The number of available MIS surgical techniques has rapidly expanded over the past 2 decades. As surgeons have become more proficient with these techniques and technology has evolved, there is increasing evidence to support the benefits of MIS procedures when compared to equivalent open procedures. Maximal preservation of native anatomy, decreased blood loss12–18 and postoperative pain, shorter hospital lengths of stay,14,18 and a quicker return to function have all been attributed to MIS techniques.12,33–38 While comparative data of postoperative complications in MIS vs open deformity techniques are still limited, preliminary data suggest that MIS deformity correction may mitigate the high complication rates seen with open surgery.15,19 Importantly, these latter benefits may explain why recent studies have even suggested that MIS approaches to deformity correction result in significantly lower costs/hospitalization charges when compared to open approaches.12,14 Ultimately, in an increasingly patient centric and cost-conscious environment, as MIS deformity corrective techniques continue to evolve, they may very well represent the future of spinal deformity management.
Limitations
There are some notable limitations with our study. First, although data were pulled from a prospectively collected database, this was nonetheless, a retrospective study and is subject to all the respective inherent limitations. Furthermore, with a low incidence of hardware failure, with inherent categorical heterogeneity further limiting the numbers of each mode of failure, more sophisticated multivariable risk analyses were not feasible. Finally, surgeon selection bias in this particular patient population could have contributed to more optimal results. A criticism often heard is that CMIS correction is only for mild deformities. In our series, 146 (55.5%) patients had severe ASD as categorized by having one of the following (Cobb angle >50° or SVA >95 mm or PI/LL mismatch >20 or pelvic tilt >30).39,40 Furthermore, all patients in the cohort, except for those with persistent thoracic kyphosis after first stage or those with upper instrumented vertebra greater than T10 (12 patients), had a physiological harmonious correction of their spinal deformity without any osteotomies. Our alignment goals were also in agreement with published literature on age-adjusted sagittal parameters that above all, aim to optimize patient clinical outcomes.41–43 Furthermore, it would have been ideal to compare our results to the results of a propensity-matched cohort of patients with adult deformity treated with open correction techniques. Nonetheless, in spite of these potential limitations, our study is the first of its size to characterize long-term hardware failures in a well-selected cohort of ASD patients undergoing CMIS spinal deformity correction.
Conclusion
The prevalence of clinically significant hardware failure needing revision in our series was low at 3.04%. Symptomatic hardware prominence requiring revision was 2.2%. Specifically, rod fractures were not common (2.2%). Our study would suggest that in the appropriately selected patients, CMIS to correct ASD without osteotomies may result in acceptable rates of hardware failure. Future studies should compare the results of CMIS deformity correction to a matched population of patients undergoing open deformity correction.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures Neel Anand reports consulting fees from Medtronic and Depuy-Synthes; royalties from Medtronic, Globus Medical, and Elsevier; and stocks/stock options in Paradigm Spine, Theracell, Spinal Balance, Spinal Simplicity, Viseon, Bonovo, Globus Medical, all outside of the submitted work. The remaining authors have no disclosures.
IRB Approval Hospital IRB approval was received for this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}