


Abstract
Introduction Osteoporotic vertebral compression fracture (OVCF) is a growing health care problem in today’s aging population. Since the advent of kyphoplasty and vertebroplasty, these interventions have been commonly utilized in the treatment of symptomatic OVCF. However, the use of these interventions varies because there is not a standard of care for the management of OVCF. There remain disparities in the use of these procedures as treatment for OVCFs in the United States.
Methods The 2012 to 2016 Nationwide Inpatient Sample was queried for all patients admitted for OVCF. These patients were then grouped based on whether they received conservative vs surgical (kyphoplasty/vertebroplasty) management and compared with respect to various socioeconomic factors including race, insurance coverage, income quartile, hospital control, and geography. Propensity score matching was utilized to control for potential baseline confounders as well as the influence of other endpoints.
Results The search criteria identified 35,199 patients admitted with OVCF, of whom 7900 (22.4%) received spine augmentation. Blacks/African Americans (risk ratios [RR] = 0.79, P < 0.001), Hispanics/Latinos (RR = 0.82, P < 0.001), Asians/Pacific Islanders (RR = 0.81, P = 0.048), and unknown/other races (RR = 0.88, P = 0.037) were less likely to receive surgical management than whites/Caucasians. When compared with Medicare patients, those with Medicaid (RR = 0.76, P < 0.001) were less likely to receive surgery while privately insured patients were more likely (RR = 1.06, P = 0.42). Patients in the West (RR = 0.90, P < 0.001) were less likely to receive surgery for OVCF than those in the Northeast.
Conclusions A wide variety of socioeconomic disparities exists in the use of spinal augmentation for the management of OVCF in the United States, limiting patient access to a potentially beneficial procedure.
Clinical Relevance Retrospective Analysis.
Level of Evidence 3.
Introduction
Considering the 10.3% prevalence of osteoporosis in those older than 50 years1 combined with the advancing age of the US population, an 8 times increased risk of mortality,2,3 and a predicted cost of over $1.5 billion annually by 2025,4,5 the osteoporotic vertebral compression fracture (OVCF) is an important pathology to consider in regard to management as well as more population-based factors such as socioeconomic status, hospital factors, cost, and geographical setting.
Management for OVCF is either through conservative options, such as bracing and physical therapy, or operative management involving percutaneous vertebral augmentation via either vertebroplasty or kyphoplasty.6 Vertebroplasty is performed via injection of cement into the fractured vertebral body, with solidification of the cement intended to provide stability and pain relief as the fractured defect becomes filled. Though logical in theory, technical limitations of vertebroplasty include lack of original vertebral height restoration, extravertebral leakage of cement, and cement retropulsion.7–9 Kyphoplasty was developed more than a decade later than vertebroplasty, and it differs in that a balloon is inserted and expanded into the fracture space to regain vertebral height by separation of endplates prior to injection of cement material.7 Controversy exists as to which procedure is superior due to a paucity of high-quality studies, with well-regarded randomized controlled trials showing no significant improvement in pain or function from vertebroplasty vs control.7,10,11
Though direct outcome studies are necessary, given the known racial disparities existing between patients’ pain management and bone health understanding, it is crucial to assess whether differences exist between management of different demographic groups. Prior studies focused on OVCF procedural management disparities have highlighted differences in operative rates between racial groups and insurance status, as well as a trend of decreasing vertebroplasty rate.4,7,12,13 Our study aims to expand on current trends and socioeconomic comparison of spinal augmentation procedures for OVCF, as well as perform unique analyses regarding OVCF operative management as it relates to other hospital, geographic, and socioeconomic factors.
Methods
The Nationwide Inpatient Sample (NIS) for years 2012 to 2016 was queried for all patients admitted as inpatients with osteoporotic compression fractures, defined by International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) codes 733.0 (osteoporosis) with 733.13 (pathologic fracture of vertebrae) and 10th Edition, Clinical Modification (ICD-10-CM) diagnosis code M80.08 (age-related osteoporosis with current pathological fracture, vertebra[e]). As the largest all-payer administrative database available for public use in the United States, the NIS has been nationally validated for the assessment of in-hospital mortality, morbidity, disposition, and inpatient outcomes.14–18
Endpoint and Risk Factors
OVCF patients were then grouped by receipt of kyphoplasty or vertebroplasty, defined by ICD-9 procedure codes 81.65 and 81.66 and ICD-10 procedure codes 0QU0, 0QU1, 0QU2, 0QU3, and 0QU4. Patients undergoing “open” procedures such as spinal fusion or laminectomy, were excluded using codes 81.0 (ICD-9), 0RG4, 0RG6, 0RG7, 0RG8, and 0RGA (ICD-10). Age, sex, race, insurance status, income quartile, hospital teaching status, hospital ownership, and geographic region were collected for each patient as potential socioeconomic correlates. Last, for each patient, overall comorbidity was estimated using the Elixhauser Comorbidity Index based on validated code from Thompson et al (2015).19
Statistical Analysis
A univariate analysis was conducted using χ 2 or Fisher’s exact tests, as appropriate, and unadjusted risk ratios (RR) were generated for each of the aforementioned baseline variables with respect to receipt of kyphoplasty/vertebroplasty vs conservative/medical management. Following this, a multivariate analysis was performed for each potential socioeconomic factor using propensity score matching under a logistic regression model. The model for each of these variables would incorporate Elixhauser Comorbidity Index, as well as all other covariates in order to account for potential interactions between baseline variables. Adjusted RRs were then calculated using these propensity-matched subgroups, along with a P-value corresponding to these calculated ratios. A P-value of less than 0.05 was utilized throughout this study to define statistical significance.
Because this study involved an administrative database void of direct patient identifiers, institutional review board approval was not required.
Results
The search criteria identified 35,199 patients who were admitted with OVCF (Table 1). There was a large female predominance (82.1%), with the mean age of 78.7 ± 11.1 years. The majority of the population was white/Caucasian (82.1%), which was followed by Hispanic/Latino (5.4%), Asian/Pacific Islander (3.0%), and black/African American (2.5%). The vast majority of patients were insured by Medicare (87.3%), which was followed by private insurance (8.1%) and Medicaid (2.9%) (Table 1). There was a relatively equal distribution of income quartiles among the population with 21.5%, 25.8%, 25.9%, and 25.3% falling into the first, second, third, and fourth income quartiles, with the first representing the lowest incomes and fourth being the highest incomes. In terms of geographical region within the United States, 29.6% of patients were in the South, 26.9% in the Midwest, 22.9% in the West, and 20.6% in the Northeast. A majority of the patients were treated at urban teaching hospitals (54.5%) with urban nonteaching hospitals being the second most common (34.4%), which was followed by rural being the least frequent (11.1%) hospital setting (Table 1). Analysis of hospital ownership reveals that most patients were treated at private nonprofit hospitals (80.5%), which were followed by private for-profit (11.1%) and public (8.5%) hospitals.
Total study cohort characteristics.
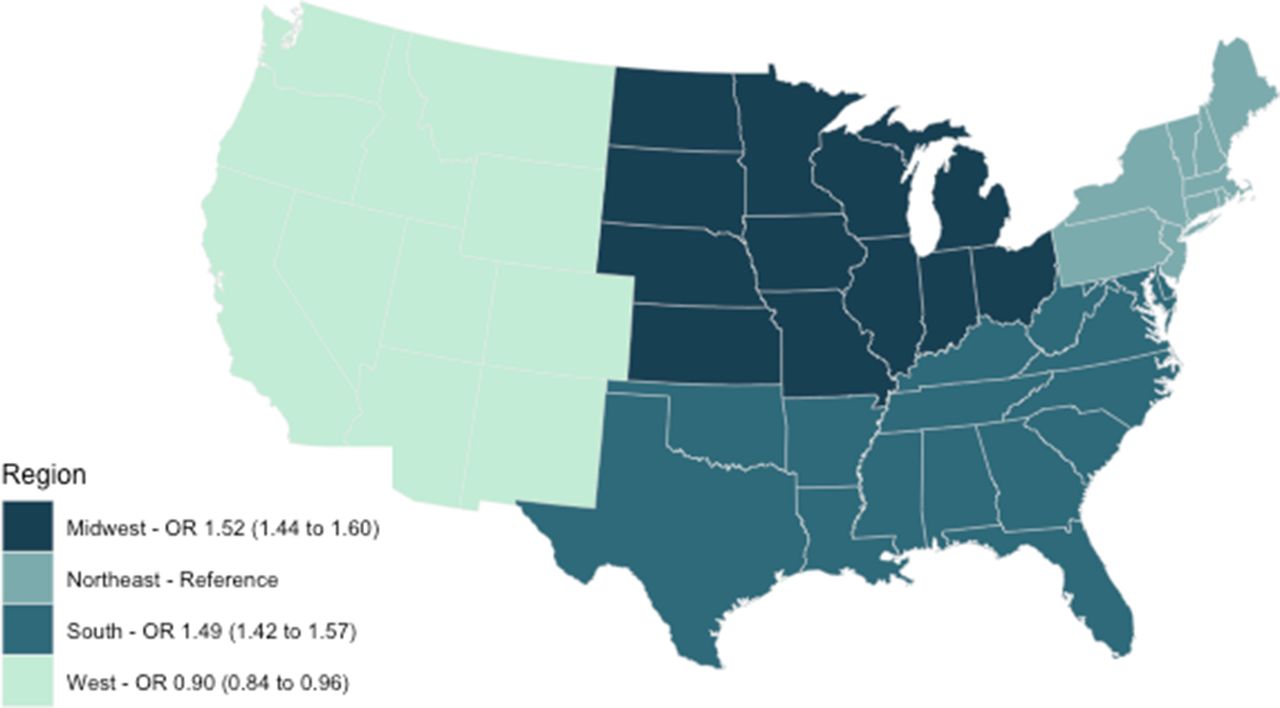
To understand the factors that influence OVCF management, the cohort characteristics previously described (Table 1) were statistically compared between the patients who underwent surgical and conservative management (Table 2). Of all the patients, 7900 (22.4%) received spinal augmentation procedures. When looking at demographics, age did not significantly impact the chance of receiving spine augmentation (P = 0.543; Table 2). Women were less likely to be surgically managed (RR = 0.9, P < 0.001) than men. When analysis was done between races, blacks/African Americans (RR = 0.79, P < 0.001), Hispanics/Latinos (RR = 0.82, P < 0.001), Asians/Pacific Islanders (RR = 0.81, P = 0.048), and unknown/other races (RR = 0.88, P = 0.037) were all less likely to receive surgical management when compared with whites/Caucasians. No statistical difference in the risk of undergoing surgical intervention existed when native Americans were compared with whites/Caucasians (Table 2). Using the Northeast as the reference population, patients in the Midwest (RR = 1.52, P < 0.001) and South (RR = 1.49, P < 0.001) had statistically significant increased probability of undergoing kyphoplasty or vertebroplasty, while patients in the West (RR = 0.90, P < 0.001) were less likely to receive these procedures for OVCF (Table 2, Figure 1). Note that these findings are for the regions unified by color, not the individual states (Figure 1). When compared with patients with Medicare insurance, people covered by Medicaid (RR = 0.76, P < 0.001) were significantly less likely to undergo surgery, while patients with private insurance (RR = 1.06, P = 0.42) were significantly more likely to undergo surgical intervention (Table 2). Patients of the wealthiest income quartile (RR = 0.95, P = 0.031) had statistically significantly reduced risk of undergoing spine augmentation when compared with the poorest income quartile. It was found that, when compared with rural hospitals, patients in urban nonteaching (RR = 1.56, P < 0.001) and urban teaching (RR = 1.59, P < 0.001) hospitals were more likely to undergo augmentation procedures. Last, patients in both private nonprofit (RR = 1.35, P < 0.001) and private for-profit (RR = 1.51, P < 0.001) hospitals were statistically more likely to undergo spine augmentation than patients in public hospitals (Table 2).

Regional geographical distribution of ORs (95% CIs) for receiving spinal augmentation for management of osteoporotic vertebral compression fracture in the Midwest, Northwest, South, and West regions of the United States.
Analysis of socioeconomic predictors.
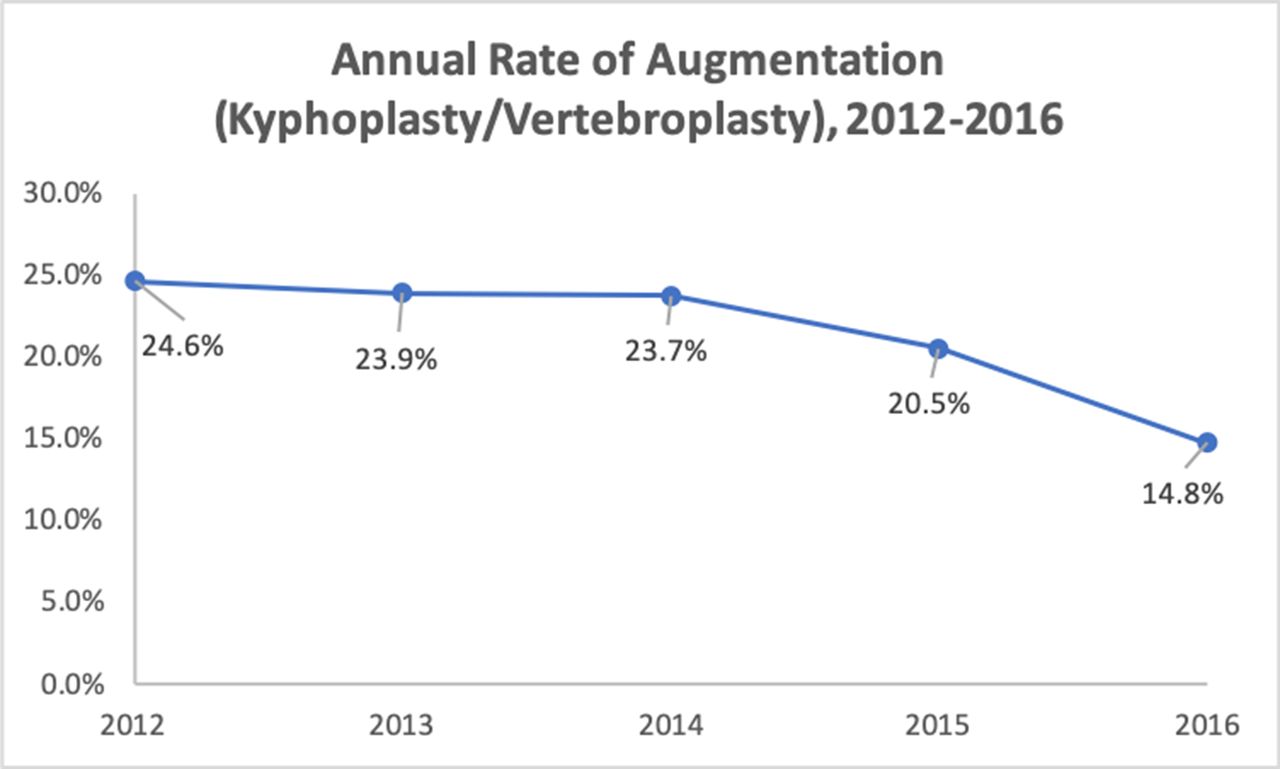
In terms of overall utilization rates, as previously stated, 22.4% (n = 7900) of the entire patient cohort admitted for OVCF received spine augmentation. Further analysis of annual usage rates revealed that 24.6% of patients admitted during 2012, 23.9% of patients in 2013, 23.7% of patients in 2014, 20.5% of patients in 2015, and 14.8% of patients in 2016 received spine augmentation procedures. This constitutes a near 10% decrease in usage over the time period. Thus, rates of spine augmentation in the management of OVCF have decreased significantly between 2012 and 2016 (Figure 2).
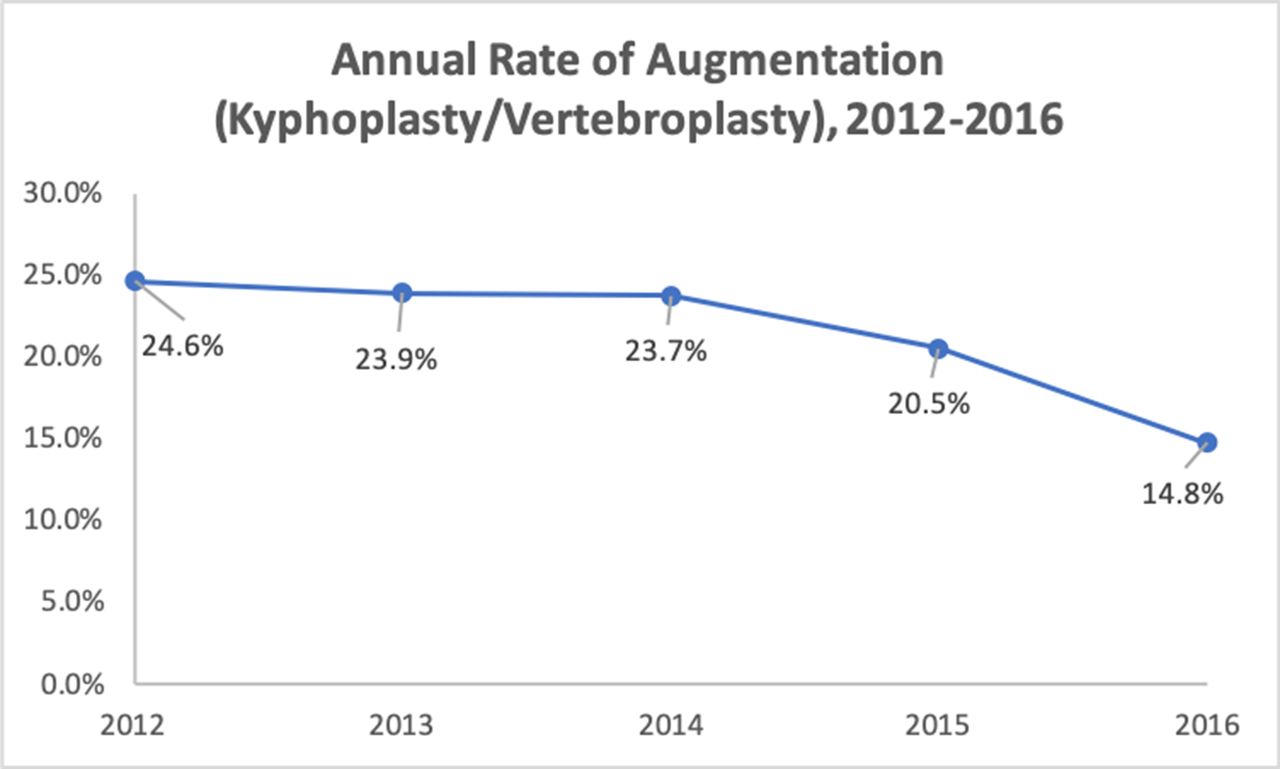
Annual rate of spinal augmentation procedure utilization for the management of osteoporotic vertebral compression fracture from 2012 to 2016.
Discussion
The goal of our study was to analyze the current trends in utilization of spine augmentation procedures such as kyphoplasty and vertebroplasty in the management of OVCF. While performed differently, both of these procedures attempt to achieve the common goal of stabilizing fractures by restoring vertebral body height and thus reducing pain and preventing further deformity.7,20,21 Although overall utilization rates appear to be decreasing, a variety of socioeconomic disparities continue to exist in the use of spine augmentation for OVCF in the United States. We found that blacks/African Americans, Hispanics/Latinos, Asians/Pacific Islanders, and patients of other races were all significantly less likely to receive spine augmentation procedures than white/Caucasian patients. In terms of insurance status, we found that compared with patients insured by Medicare, those with Medicaid were significantly less likely to receive vertebroplasty or kyphoplasty, while those with private insurance were significantly more likely to receive these interventions. Geographically, patients in the southern and midwestern regions of the United States were significantly more likely to receive operative intervention for their OVCF, while patients in the western United States were less likely. Finally, as it pertains to hospital ownership status, patients were more likely to receive spinal augmentation procedures at private for-profit and private nonprofit hospitals compared with public hospitals. Thus, there are various, yet potentially interrelated, disparities in the usage of spinal augmentation procedures for OVCF management in the United States.
The effects of racial and socioeconomic disparities on health care delivery and outcomes have been well documented in the literature. Across diverse specialties and delivery strategies, racial minorities and individuals of lower socioeconomic class have been shown to demonstrate lower access to care and worsened outcomes. The cause of this well-documented phenomenon is a complex issue that may be influenced by health literacy, perceived discrimination, physician bias, and potentially genetic variations. The results of our investigation in OVCF management are largely in agreement with findings in other pathologies, finding that racial and ethnic minorities are less likely to undergo surgical intervention for OVCF. The spine patient outcomes research trial study found that black/African American patients underwent elective spine surgery at significantly lower rates than white/Caucasian patients (54% vs 67%, P = 0.003), suggesting a similar disparity in delivery of overall surgical care in spine patients.22,23 Several investigations have also noted similar disparities in surgical intervention rates in anterior cervical spine surgery, while also suggesting increased delay in diagnosis times.24,25
Pain management and the known racial disparities that exist regarding pain assessment and analgesic prescriptions may play a large role in the delay of diagnosis and disproportionate use of procedural interventions. Multiple studies have shown that black/African American and other nonwhite/Caucasian patients are less likely to prescribe analgesics, especially opioids, than white/Caucasian patients.26–30 According to Tamayo-Sarver et al, this was especially true in conditions with fewer objective findings, such as back pain.26 Thus, biases in pain and disability assessment could lead to delayed diagnoses and subsequent underutilization of pain management procedures. Undertreatment of pain as well as underlying conditions could also contribute to worsened postoperative outcomes in these minority patients. Previous studies have shown that compared with white/Caucasian patients, black/African American patients undergoing spinal surgery have increased rates of major intraoperative complications, postoperative hospital length of stay, and 30-day readmissions, as well as worsened postoperative patient satisfaction ratings.31–34 Thus, as is seen in most areas of medicine, significant racial disparities exist in spine surgery, and the use of spine augmentation for OVCF is no exception.
Our investigation also reports a significant difference dependent on insurance status, finding that compared with Medicare patients, privately insured patients are more likely to undergo surgical intervention whereas Medicaid patients are less likely. However, it is important to note that insurance status cannot be viewed in a vacuum as access to health insurance coverage is heavily related to race. Significantly greater proportions of white/Caucasian patients are privately insured compared with black/African American and Hispanic/Latino patients largely due to rates of employment-related coverage. Lower rates of employment among black/African American and Hispanic/Latino populations limit access to private insurance and lead to increased rates of public insurance, or lack of any health insurance at all.35 These disparities in insurance status may then, in turn, influence where a patient is treated, as public insurance may not cover private hospital stays. Thus, our finding that private hospitals were more likely to provide spinal augmentation than public hospitals may largely be attributed to insurance status and subsequently race.
While not assessing rates in surgical intervention itself, Rasouli et al reported that publicly insured patients were found to have prolonged length of stay and postoperative emergency department visits.36 An investigation by Elsayed et al noted that publicly insured patients showed less improvement after decompression for lumbar spinal stenosis.37 While our analysis was unable to assess long-term outcomes due to limitations of the NIS, innumerous studies have demonstrated worsened outcomes in regard to rates of mortality, readmission, complications, and overall cost in association with nonwhite/Caucasian race.31,38,39 Interestingly, our study also revealed that wealthier patients were significantly less likely to receive spinal augmentation compared with the poorest patients. While seemingly contradictory, this could also be explained by increased access to follow-up as well as potentially more sufficient conservative treatment measures, such as pain control, provided to wealthier patients. This could be the result of wealthier patients being less likely to suffer from the bias in pain and disability assessment compared with poorer patients. Thus, the results of our investigation, in conjunction with other similar studies on health care disparities, support further research into the causes and consequences of disparities in addition to potential strategies for mitigation.
Finally, geographic variations in rates of kyphoplasty or vertebroplasty for OVCF show higher rates of these interventions in the South and midwestern regions of the United States and lower rates in the Northeast and West. These findings are identical to those of previous studies regarding geographical variation in the rates of lumbar fusion and lumbar discectomy in terms of regional distribution.40 While this variation could be attributed to a combination of differences in patient preference and surgeon experience, it is more likely that lack of consensus on efficacy of spinal augmentation procedures for OVCF results in variations in practice.
Overall usage rates of spinal augmentation procedures have decreased dramatically over the past decade. In a similar analysis of trends in usage of spinal augmentation between 2005 and 2010, Gu et al12 found that 56.6% of patients admitted for vertebral fracture were treated with either kyphoplasty or vertebroplasty. In our study of patients from 2012 to 2016, only 22.4% of patients admitted for OVCF received spine augmentation. Furthermore, our analysis of annual rates of augmentation shows a decrease in usage from 24.6% of OVCF patients in 2012 to just 14.8% of patients in 2016 (Figure 2). These findings are consistent with previous analyses such as those of Laratta et al, which found that vertebroplasty rates decreased by 53% and kyphoplasty rates decreased by 17% between 2008 and 2014.7 Decreased rates of surgical intervention may be partially an effect of several high-profile conflicting randomized clinical trials over the past decades in regard to the efficacy of spinal augmentation. A randomized, double-blinded, placebo-controlled trial of 78 patients by Buchbinder et al published in the New England Journal of Medicine found no beneficial effect to vertebroplasty in comparison with a sham procedure for painful osteoporotic fracture.10 However, a similarly designed investigation of 120 patients by Clark et al published in The Lancet found that vertebroplasty was superior to placebo for acute osteoporotic compression fractures.41 A recent meta-analysis of 21 trials conducted by Buchbinder et al for the Cochrane Database of Systematic Reviews found moderate to high-quality evidence that vertebroplasty had no significant positive impact on pain, disability, or quality of life in the treatment of osteoporotic compression fractures.42 These findings and subsequent lack of consensus in clinical benefit have likely significantly impacted the trends in spinal augmentation for osteoporotic vertebral fractures.
Limitations
Most of the limitations of this study are due to the inherent limitations of large patient databases such as the NIS database. There may be inaccuracy of billing records and coding errors, underreporting of procedures, exclusion of missing cases in the NIS database, and errors transferring data from hospital records to administrative data. There may also be an indication bias inherent to this large database containing data on surgeries performed by a variety of surgeons at a variety of institutions. Additionally, the NIS does not include long-term outcome data, so no conclusions can be drawn regarding disparities in outcomes for patients with OVCF.
Conclusion
Spinal augmentation procedures continue to be a treatment option for pain control in patients with OVCF. Our findings corroborate the wide variety of socioeconomic disparities that continue to exist in management of OVCF as well as in all of spine surgery as a whole. Additionally, our findings are consistent with the literature showing a declining trend in utilization of spine augmentation procedures for OVCF. Furthermore, prospective analyses must be done to perform more thorough analyses of long-term outcomes and elicit further information regarding efficacy as well as disparities in outcomes of spine augmentation in the management of OVCF.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.