


Abstract
Introduction An estimated 15%–25% of patients with chronic low back pain may in fact suffer from sacroiliac (SI) joint dysfunction. SI joint fusion has become a common treatment option for the management of SI joint dysfunction. However, little is known about opioid use prior to and after surgical treatment in this patient population.
Methods The medical records of 62 patients treated with SI joint fusion at our institution were reviewed in this retrospective study. The Colorado Prescription Drug Monitoring Program (CPDMP) was accessed to gather opioid prescription information for these patients. Only those patients who had received an opioid prescription within 3 months prior to their surgery were included in the study. Patients who had SI joint fusion but underwent another surgical procedure during the 12-month follow-up period were excluded from analysis. Preoperative (6 and 3 months) and postoperative (3, 6, 9, and 12 months) mean morphine milligram equivalents (MME) were collected from the CPDMP database for each patient. Patient demographic and medical comorbidity data were also documented to identify any correlations or potential risk factors for chronic opioid prescribing. Visual analog scale (VAS), Oswestry Disability Index (ODI), and Denver SI Joint Questionnaire (DSIJQ) scores were recorded for each patient to assess clinical outcomes.
Results At 3 months prior to surgery, patients were prescribed an average of 47.2 mean MME/d. At no point postoperatively did the quantity of opioids, measured in MME/d, change significantly from the 3-month preoperative prescription quantities. There was no significant difference in the quantity of opioids received by men vs women, in patients with vs without anxiety and/or depression, or in younger vs older patients. Low body mass index was correlated with decreased opioid prescriptions at 6 months postoperative but became statistically insignificant again by 9 months postoperative.
Significant improvements in VAS scores were recorded for all postoperative clinical evaluation timepoints (at 6 weeks and 3, 6, and 12 months) and compared to preoperative scores. By 12 months, VAS scores had decreased from 6.2 to 3.9 (P < 0.001). This change is not only statistically significant but also meets the criteria for minimum clinically important difference in scores. Both the ODI and DSIJQ patient-reported outcomes scores also showed significant improvements at 12 months after surgery (ODI: 48.9 preoperative vs 24.6 postoperative, P = 0.02; DSIJQ: 53.2 preoperative vs 17.4 postoperative, P = 0.014). The ODI improvement also met the minimum clinically important difference criteria. By 6 months postoperatively, there was no significant correlation in VAS or ODI and opioid use. There was no significant correlation between the DSIJQ scores and the daily dose of opioids at any point postoperatively.
Conclusion Quantity of opioid prescriptions received by patients with SI joint pain did not change significantly from 3 months preoperatively to any point postoperatively despite significant improvements in all patient-reported outcome measures. This discordance between long-term opioid requirements and positive clinical outcomes is concerning and warrants further investigation.
Level of Evidence 3.
Introduction
The opioid epidemic has been affecting the US population for years. The United States is responsible for the consumption of 80% of global opioids and nearly 99% of the world’s hydrocodone.1 This excessive use and abuse of opioid medications place a significant toll on the healthcare system and are associated with alarming degrees of morbidity and mortality. Opioid prescription misuse is estimated to cost the country $78.5 billion annually, most of which is economic burden due to lost productivity.2 Approximately 128 people die every day in the United States due to an opioid overdose,3 and although many of these deaths are due to illicit drugs like heroin, around 80% of heroin users misused opioid prescriptions first.4 Unfortunately, surgeons still face the ever-growing challenge of providing adequate pain control while avoiding the unintentional initiation of addiction for their patients. Orthopedists are the fourth most active prescribers of opioids in the United States, providing almost 8% of all opioid prescriptions,5 and thus have a large stake in this epidemic. Due to the nature of their field, orthopedists perform surgeries that often require a significant amount of pain control augmentation. Additionally, there has been evidence showing that the use of nonsteroidal anti-inflammatory drugs to control pain may lead to impaired bone healing,6,7 which further complicates the pain management of the orthopedic patient.
Low back pain is the leading cause of disability worldwide.8 Furthermore, an estimated 15%–25% of chronic low back pain complaints are due to the sacroiliac (SI) joint.9,10 SI joint fusion has become a common treatment option for the management of SI joint dysfunction. However, little is known about opioid use prior to and after surgical treatment in this patient population. There are similar studies examining the objective change in opioid use after other back surgeries, but nothing to our knowledge on SI joint fusions specifically. Studies that do examine the change in opioid use after SI joint fusion use patient-reported opioid use instead of objective measures.11,12 This study aims to evaluate the impact of SI joint fusion surgery on the use of opioids in patients with chronic low back/SI joint pain in a way that eliminates the potential bias in patient reporting.
Methods
Under local institutional review board approval, the medical records of patients who were treated with SI joint fusion by 1 of 4 fellowship trained orthopedic spine surgeons at our institution were reviewed in this retrospective study. Patients received a navigation-assisted mini-open SI joint fusion with direct bone grafting and minimally invasive fixation using the iFuse Implant system from SI Bone Inc (Santa Clara, CA). Only those patients who had received an opioid prescription within 3 months prior to their surgery and were between the ages of 18 and 95 years were included in the study. Patients who had SI joint fusion but underwent another surgical procedure during the 12-month follow-up period or who were treated for traumatic spine injuries were excluded from analysis. After exclusion criteria, 62 patients remained in the study. For outcome evaluations involving visual analog scale (VAS), Oswestry Disability Index (ODI), and Denver SI Joint Questionnaire (DSIJQ),13 only 45 patients had sufficient data for analysis. When necessary, a separate statistical analysis was performed using only those patients with sufficient patient-reported outcome data. No patients included in the study had spinal cord stimulators or indwelling intrathecal pumps.
The Colorado Prescription Drug Monitoring Program (CPDMP) was accessed to gather opioid prescription information for these patients. Preoperative (6 and 3 months) and postoperative (3, 6, 9, and 12 months) mean morphine milligram equivalents per day (MME/d) were collected from the data reported by the CPDMP for each subject. Patient demographic and medical comorbidity data from chart review were also documented and compared to identify potential risk factors for chronic opioid use. Additional variables that were evaluated include age, sex, body mass index (BMI), and habits such as smoking, alcohol use, marijuana use, etc. Data on diagnoses including bipolar disorder, gout, rheumatoid arthritis, and psoriatic arthritis that might be associated with opiate use for other purposes were also collected. Ultimately, there were insufficient data for statistical analysis regarding a number of these criteria.
VAS, ODI, and DSIJQ scores for each patient were assessed via questionnaires at in-person clinical visits to record clinical outcomes preoperatively and postoperatively every 3 months. The ODI is a 10-question survey that measures the extent of impact of back pain on selected activities of daily living. The DSIJQ is similar to the ODI, but assesses SI joint dysfunction across 10 key domains: sitting, getting up from a chair, walking, walking up/down stairs, getting in/out of a car, bending at the waist, kneeling/squatting, lifting, daily activities, sleep, and SI joint instability. Lower scores represent less SI joint disability and higher scores represent more disability.
Statistical Analysis
Statistical analysis was performed using the statistical program JMP Pro 15.0.0. Differences were considered as statistically significant if P ≤ 0.05. Description of the studied population was performed using the following characteristics of distribution: mean values, standard deviation, minimum and maximum values for continuous variables, and the rates (percentage) for categorical variables. Comparative analysis of consuming of opioids in the studied population at different follow-ups was analyzed using analysis of variances with following statistical indices: mean, median, standard deviation, minimum and maximum values; P value of differences between different follow-ups was defined by the paired 2-sided t test. Evaluation of influence of potentially confounding factors on the consumption of opioids at different follow-up appointments was performed using the stratification method. If confounding factors were categorical (gender, anxiety), differences between subgroups were defined using the Wilcoxon nonparametric test. If confounding factors were described by continuous variable (age, BMI), the Pearson correlation test was applied. A correlation between patient-centered characteristics such as VAS, ODI, DSIJQ, and their changes with consumption of opioids was defined by the Pearson correlation test at different follow-ups.
Results
At 3 months prior to surgery, patients were prescribed an average of 47.2 MME/d. Compared to opioid use at 3 months before surgery, there was no difference in opioid use at any point postoperatively (Table 1). Furthermore, there was no significant difference in the quantity of opioids received by men vs women (Table 2), patients with anxiety and/or depression vs patients without these conditions (Table 3), or patients of different ages (Table 4). Lower BMI was correlated with decreased opioid prescriptions at 6 months preoperative (Pearson correlation coefficient (r) = 0.27, P = 0.033) and 6 months postoperative (r = 0.25, P = 0.049); however, these correlations became statistically insignificant by 9 months postoperative (Table 5). Data were also collected on a variety of medical comorbidities including incidence of gout, psoriatic arthritis, rheumatoid arthritis, bipolar disorder, substance abuse, and “other psychological diagnoses”; however, there were not enough data within these categories to create correlation analyses.
Quantity of opioids prescribed over time (N = 45).
Impact of sex on quantity of opioids prescribed over time (N = 62).
Impact of anxiety/depression on quantity of opioids prescribed over time (N = 62).
Correlation between age and dose of opioids prescribed over time (N = 62).
Correlation between body mass index and dose of opioids prescribed over time (N = 62).
Significant improvements in VAS scores were recorded for all postoperative clinical evaluation time points (6 weeks, 3, 6, and 12 months) compared to preoperative scores. By 12 months postoperative, VAS scores had decreased from 6.2 to 3.9 (P < 0.001). This change is not only statistically significant but also meets the criteria for minimum clinically important difference in scores. Both the ODI and DSIJQ patient-reported outcomes scores also showed significant improvements at 12 months after surgery (ODI: 48.9 preoperative vs 24.6 postoperative, P = 0.02; DSIJQ: 53.2 preoperative vs 17.4 postoperative, P = 0.014). These changes in ODI scores also met criteria for minimum clinically important difference. By 6 months postoperatively, there was no significant correlation in VAS or ODI, and opioid use. There was no significant correlation between the DSIJQ scores and the daily dose of opioids at any point postoperatively.
Discussion
Numerous studies have demonstrated the efficacy of minimally invasive SI joint fusion surgery as a treatment for chronic low back pain.11,12,14–17 Similarly, our study showed a statistically significant improvement in patient-reported outcomes based on changes in VAS, ODI, and DSIJQ scores at 12 months. Importantly, the use of opioids did not reflect this improvement in outcomes after surgery. Rather, at 12 months postoperative, patients’ use of opioids was unchanged their preoperative levels and did not correlate with their patient-reported outcome values. This finding is concerning and warrants further exploration centered on the effectiveness of SI joint fusion surgery.
At the facilities where these surgeries were performed, there is a policy stating opioids should not be prescribed to patients beyond 90 days after surgery except in extreme circumstances. One would expect that opioid prescribing would decrease to correspond with patient reports of improvements in pain and function. However, patients in our study were still receiving opioid prescriptions at and beyond 90 days; the majority of patients continued to receive prescriptions out to the 12-month endpoint of data collection. Thus, it is possible that an external physician was prescribing continued opioid medications for these patients. It is also possible that opioid abuse was a factor with these patients.
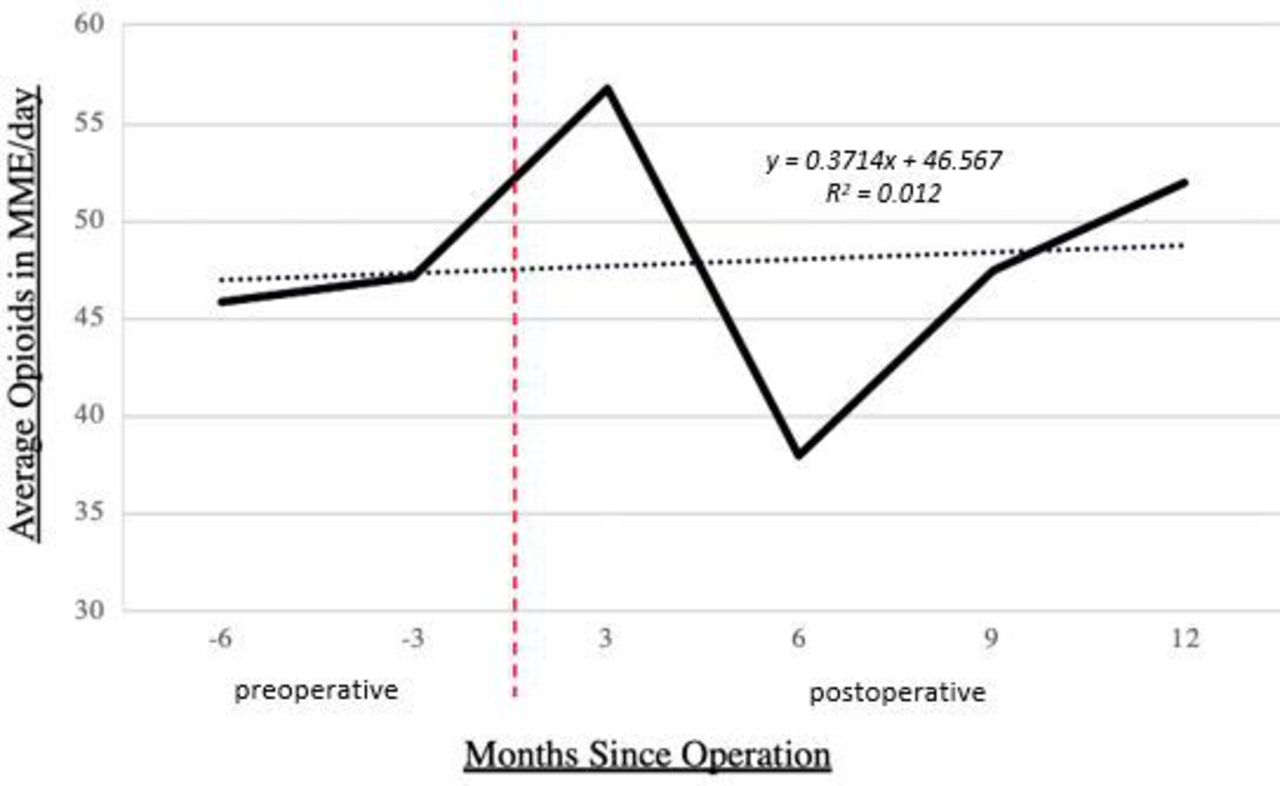
Another consideration is whether the opioid use for back pain ever really decreased even though VAS scores improved. Though not statistically significant, our study showed that the mean MME of opioids prescribed per day decreased minimally from 3 months preoperatively to 6 months postoperatively (Table 1). Additionally, by 12 months postoperatively, the average MME/d prescribed returned to and even appeared to exceed the average daily opioid prescribed from 3 months preoperatively, though not by a significant amount (Figure). This brings into question the effectiveness of the intervention—did the SI joint fusion really improve the pain of the patients, or is there a placebo effect at play? There has been long-standing disagreement among medical professionals as to the efficacy of the SI joint fusion as a solution to SI joint pain. Dengler et al12 compared outcomes of SI joint arthrodesis vs conservative management. Our findings aligned in regard to improved VAS, ODI, and other quality of life measures after surgery. However, their findings showed that after SI joint fusion, the prevalence of opioid use decreased significantly from baseline whereas no significant change was observed in the group receiving conservative management. Importantly, their data regarding opioid use were self-reported by patients. This is where our study differs: we aimed to examine the use of opioids objectively using data from the CPDMP in place of a survey or other patient-reported method. Our data show that the patient-reported outcomes do not reliably correlate with the pain medication they are actually prescribed. Vanaclocha et al11 evaluated patients with SI joint dysfunction and assessed outcomes and opioid use following conservative management, SI joint denervation, and SI joint fusion. Their study showed a reduction in the number of patients using opioids from 63% at baseline to only 7.4% at final follow-up. However, this study was limited by its small sample size as only 17 patients underwent SI joint fusion. Furthermore, it is not clear as to how they recorded opiate use data. Polly et al showed similar though less dramatic effects with a larger randomized controlled trial in the United States, reporting a 29.6% reduction in opioid use 24 months after SI joint fusion compared to an increase in opioid use in the nonsurgical management group.18

Average opioid prescriptions before and after sacroiliac joint fusion. Mean morphine milligram equivalents per day (MME/d) as reported per the Colorado Prescription Drug Monitoring Program data as above in Table 1 with linear regression superimposed. No significant differences in mean MME/d.
Despite efforts to educate patients, enhance monitoring, improve proper disposal, and limit diversion of opioids,19 more than 10 million people in the United States were reported to be opioid “misusers” in 2018.20 Our findings raise the issue of interdisciplinary communication when it comes to medication reconciliation. Medication reconciliation is a critical component of quality patient care as it ensures patient safety and reduces polypharmacy, but it is a time-consuming task and is rather inefficient when patients’ providers lack a shared electronic health record.21 There are various approaches to tackle this challenge of cross-specialty medication reconciliation; however, there are still barriers to implementation.22,23 Currently, it remains difficult to achieve full communication across provider specialties at various healthcare institutions.
It is also possible that patients in our analyses had confounding illnesses requiring prescription opioids that were not included in their internal medical records. To accurately evaluate for a change in opioid use after an orthopedic intervention such as SI joint fusion, additional studies are necessary to distinguish the diagnoses for which the study subjects take opioids. In our study model, we were unable to evaluate whether the patients who had continued opioid use were using this form of analgesia for their back pain or some other medical problem. Evaluating the use of opioids by diagnosis is necessary to distinguish whether the intervention of an SI joint fusion is addressing the problem for which the patient takes his or her opioids. In previous studies comparing the efficacy of surgery vs medical management of SI joint pain, opioid use data were self-reported based on whether or not patients were taking the opioids specifically for their SI joint or low back pain.24–26 Because we measured opioid prescribing data as a surrogate for use based on reporting through the CPDMP database, we had no way of knowing whether our patients continued to fill prescriptions of opioids for their back pain, or if they had another condition requiring pain management with opioids. We collected data to understand whether comorbid risk factors for increased opiate use existed; however, there were insufficient data to run reliable correlations. Risk factors and comorbidities examined included habits like smoking, alcohol use, marijuana use, etc as well as diagnoses including bipolar disorder, gout, rheumatoid arthritis, and psoriatic arthritis. There were sufficient data to compare opioid use after SI joint surgery and whether or not patients had depression/anxiety; however, there was no significant difference in patients with vs without these diagnoses in particular.
This study has several limitations. First, the study included a relatively small cohort. Interpretation of study results would be dramatically improved with a larger sample size. Additionally, we depended on the CPDMP for opioid prescription monitoring. This system fails to account for any prescription opioids attained out of the state of Colorado. Even for those prescriptions obtained within the state of Colorado, the CPDMP tracks only which prescriptions are filled and does not reflect the quantity that a patient consumes. Furthermore, the CPDMP software calculates the MME based on the number of pills prescribed divided by the number of days for which the prescription is intended to last. However, the number of days recorded for each prescription is entered at the discretion of the dispensing pharmacy and may not be uniform across all pharmacies. Our study was also unable to account for the full list of reasons for which a patient may be receiving opioids. While we excluded patients who had another surgery within the 12-month follow-up period, other health issues could have come into play. For example, a patient may have been receiving opioids from their family physician for a problem unrelated to SI joint pain, and thus would still be filling and using an opioid prescription regardless of their surgery status. An additional consideration is the possibility of recall bias, observation bias (Hawthorne effect), and the overall accuracy of the patient-reported outcome scores.
Conclusion
Opioid prescription filling did not change significantly from 3 months preoperatively to any point postoperatively despite significant improvements in all patient-reported outcome measures. This discordance between long-term opioid requirements and positive clinical outcomes implies the use of opioid medications is much more complex than simply reducing pain, which warrants further investigation. Furthermore, the fact that there was no correlation between VAS, ODI, and DSIJQ, and the MME/d of prescribed opiate medications indicates that further evaluation into the efficacy of SI joint fusion surgery is necessary. Ultimately, this study reveals the fact that databases like the CPDMP may not be reliable for clinical use. Efforts should be made to correct the known flaws in how this data are recorded to make it more clinically meaningful, especially in the context of the opioid epidemic. A measured approach should be taken when utilizing this data and any conclusions drawn from this data should be interpreted with caution.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial relationships related to this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}