


Abstract
Background Preoperative lumbar epidural steroid injections (LESI) are known to be a risk factor for intraoperative dural tears in traditional spine surgery. However, whether the same holds true after minimally invasive surgery is debatable. The authors decided to investigate the incidence of complications in patients undergoing minimally invasive lumbar discectomy after a preoperative LESI.
Methods A retrospective analysis was carried out on patients ages 21 to 65 years who underwent minimally invasive lumbar discectomy over 3 years between November 2017 and October 2020. These were classified into 2 groups based on the administration of an LESI within a year of surgery. Those receiving LESI were further subdivided on the basis of the proximity of the injection to the surgery. The complications encountered during and up to 6 months after the surgery were recorded. Various demographic variables were also noted.
Results A total of 315 patients were included in the study, of which 129 were in the LESI group and 186 were in the non-LESI group. The overall complication rate was 13.65%, with 17.83% in the LESI group and 10.75% in the non-LESI group (P = 0.07). Patients receiving an LESI were 2.49 times more likely to suffer from intraoperative dural tears compared to the other group (95% CI: 1.00–6.20, P = 0.049). This was more prevalent in those who were administered an LESI within 3 months of the surgery (OR: 3.24, 95% CI: 1.12–9.40, P = 0.03). However, the rates of other complications including infections were comparable.
Conclusions A history of LESI within 3 months of the surgery is a risk factor of intraoperative dural tears. However, other complications, including infections, are not affected by a preoperative LESI.
Clinical Relevance A history of an LESI within 3 months of a proposed minimally invasive discectomy should make the surgeon extra-cautious of the risk of a dural tear.
Level of Evidence 3.
Introduction
Lumbar epidural steroid injection (LESI) forms an important part of modern spine care. It helps in the conservative management of patients mainly with pathologies such as radiculopathy. These can be performed by a transforaminal, interlaminar, or caudal approach by injecting either a steroid alone or with a local anesthetic agent. Although the exact mechanism of action is not clear, it is probably because of the local anti-inflammatory and membrane stabilizing effects of the steroid and independent modulation of the peripheral nociceptor input.1 All of these methods have proved to be efficacious, but controversy exists regarding the relative efficacies of each approach.2,3
LESI may provide a short-term benefit in terms of pain relief and functional outcomes and may even make the need for a surgical intervention less likely.4,5 In spite of this, a proportion of patients still undergo surgery for residual or recurrent symptoms.5–7 Steroids can have a significant effect on the local biochemistry and thus can result in altered tissue biology, such as hypervascularity and epidural scarring. This can lead to numerous challenges that are not usually seen. The evidence in literature as to whether this can lead to an increased incidence of perioperative and postoperative complications, such as bleeding, dural tears (DTs), and infections, is sparse. Furthermore, we could not find a single study evaluating these parameters in patients undergoing management by minimally invasive spine surgery (MISS).
The authors felt the need to investigate whether the incidence of complications after MISS changes after an LESI is given preoperatively and whether there was a time-dependent pattern seen with regard to the complications. Thus, the study was designed to evaluate the association of a previous LESI on the incidence of various complications in patients undergoing minimally invasive, microtubular discectomy for a lumbar prolapsed intervertebral disc (PIVD).
Methodology
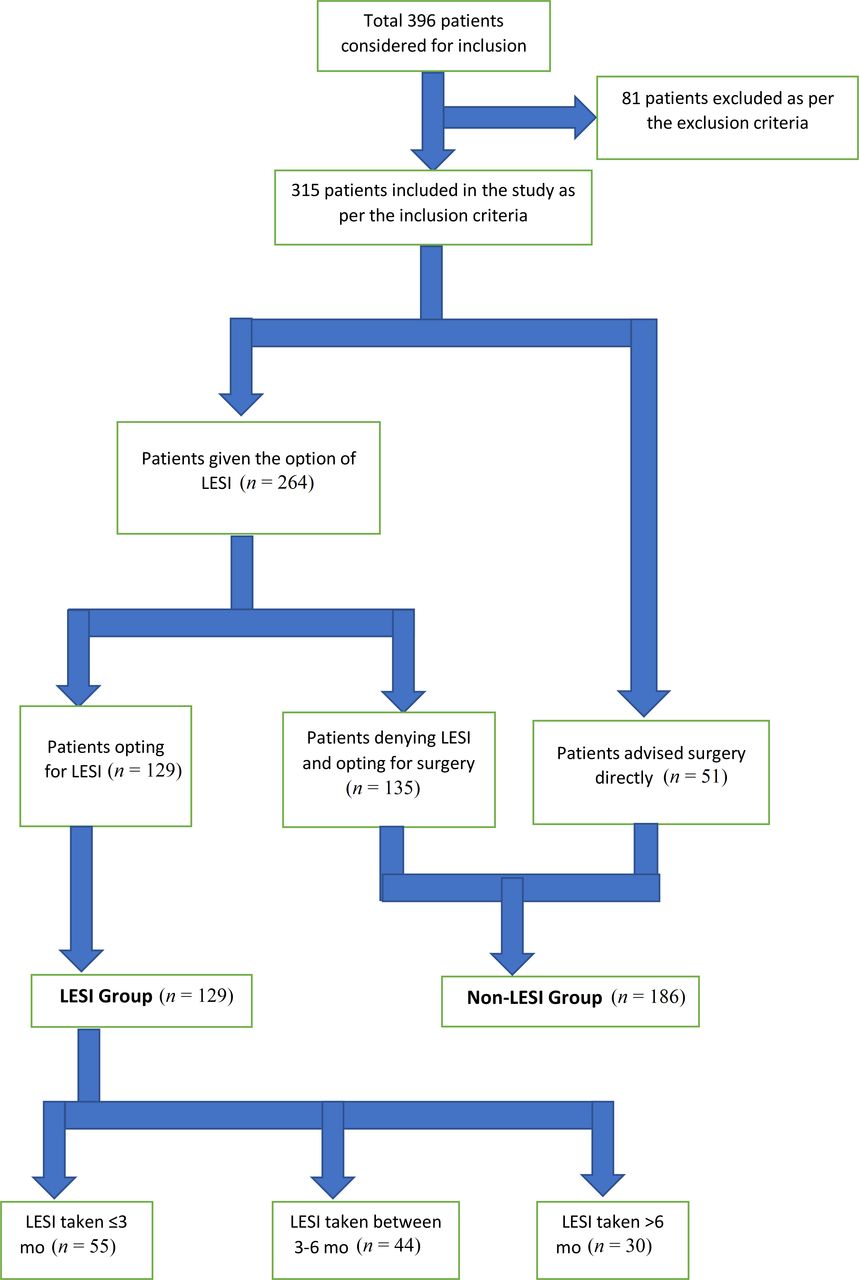
A retrospective study was undertaken at a tertiary care spine center after obtaining a waiver of approval from the local ethics committee. Written informed consent was obtained from all of the participants for participation in the trial. All patients who were operated on between November 2017 and October 2020 by minimally invasive microtubular discectomy for radiculopathy secondary to a PIVD were included in the study as per the inclusion and exclusion criteria (Table 1). At our institute, all patients with symptomatic radiculopathy due to a PIVD are given a trial of transforaminal LESI as a protocol except in cases of cauda equina syndrome, recent onset neurologic deficit, severe pain, and patient denial. Those patients who improve are further managed conservatively, if required, with a follow-up LESI. Those with inadequate or incomplete relief are not offered a second LESI but are instead offered a further option of surgery. The process for patient selection is demonstrated in Figure 1. The preoperative data were recorded from the hospital records. These included the comorbidities, history of an LESI preoperatively, and other necessary demographic variables. Similarly, the perioperative and postoperative data including the complications were recorded from the case records of the department and the hospital records. The patients were divided into 2 groups, as follows: one who received an LESI at a maximum of 1 year preoperatively and the other who did not receive the intervention. The patients in the LESI group were further subdivided based on the interval between LESI and the surgery into 3 groups, as follows: ≤3 months, 3 to 6 months, and >6 months. All the surgeries were performed using the standard approach described in the literature.8
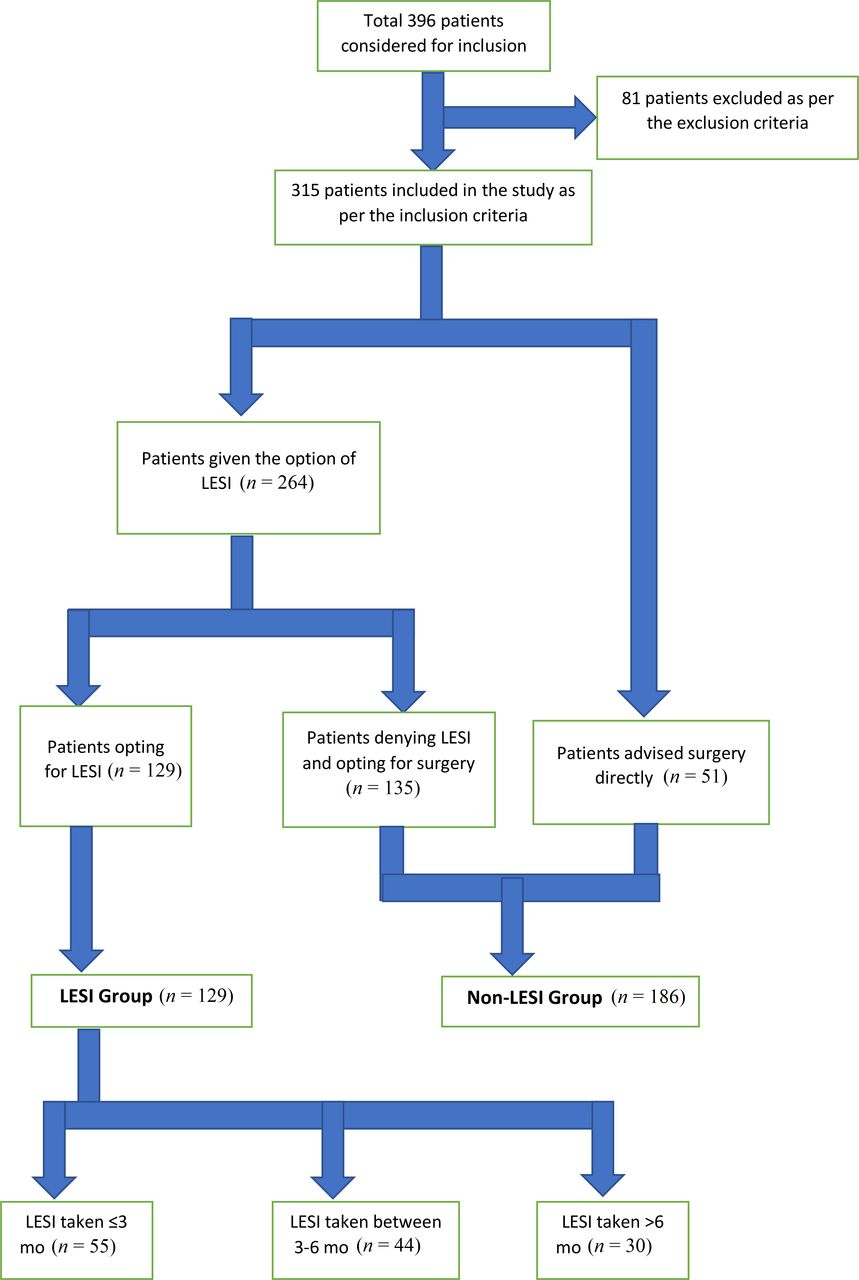
Flowchart depicting patient selection for the study (LESI, lumbar epidural steroid injection).
Inclusion and exclusion criteria for patient selection.
The complications encountered were subdivided into DT and non-dural tears (NDT). NDT included infections, new-onset neurological symptoms, and other medical issues needing specialist medical care, such as urinary tract infection, pneumonia, myocardial infarction, deep venous thrombosis, and so on. All the DTs were managed with fibrin glue and fat application over the site of durotomy, and none required an open repair. The DT closure was confirmed by a Valsalva maneuver given intraoperatively. Mobilization was delayed in all such cases for 48 hours. Patients were kept in Trendelenburg’s position and advised to lie prone as per the comfort level. A lumbar drain or acetazolamide was not used in any case. All asymptomatic cases were mobilized after 48 hours. All the surgeries were done using an 18-mm tubular system by a single team of surgeons. Clinical data were reviewed for at least 6 months postoperatively to recognize any delayed complications.
Statistical Analysis
The statistical analysis was performed by SPSS 23.0 version. Continuous variables were described as mean and variation of each observation from the mean value represented as mean ± SD (analyzed using independent t test). Categorical variables were described by taking percentages and analyzed using the χ 2 test or Fisher exact test when appropriate.
A binomial logistic analysis was performed to analyze the association between DT and LESI at the various time intervals between intervention and surgery, and OR was calculated with respect to the group not given the intervention. Furthermore, the NDT complications were analyzed for association with the intervention. A P value of <0.05 was taken as significant.
Results
A total of 315 patients were included in the final analysis as per the inclusion and exclusion criteria. A total of 129 patients were given LESI in the 12 months before surgery and 186 patients were not given LESI. All the patients in the LESI group received the injection only once and then proceeded to surgery as there was no substantial relief postinjection. We could not find a single patient who required surgery either for incomplete relief or recurrence of the disease after having had 2 or more LESIs. The mean age of the patients was 53.2 ± 11.8 years. There were 192 males and 123 females, and the mean body mass index was 23.7 ± 2.9 kg/m2. The distribution of patients across the 2 groups was similar with respect to age, gender, and body mass index (Table 2). Similarly, the comorbidities were evenly distributed between the 2 groups with the most common comorbidity being diabetes mellitus, which was seen in 39 patients (12.4%). However, the patients in the LESI group had a significantly longer duration of symptoms before being operated upon (P = 0.002) (Table 2).
Demographic variables of the patients in the 2 groups.
A total of 43 complications (13.65%) were witnessed in the study with 23 seen in the LESI group (17.83%) and 20 seen in the non-LESI group (10.75%), and the difference was not statistically significant (P = 0.07). A total of 21 DT were seen with an overall incidence of 6.67%. An incidence of 10.08% was seen in the LESI group in comparison to 4.30% in the non-LESI group, and this difference was statistically significant (P = 0.049) with an OR of 2.49 (Table 3). The subgroups of the LESI group were further analyzed. The incidence of DT in the ≤3 months, 3–6 months, and >6 months were 12.72%, 9.09%, and 6.67%, respectively. The OR calculation revealed that the patients receiving LESI within 3 months of the surgery were 3.24 times more likely to have a DT (P = 0.03). Although the ORs of the other 2 groups were >1, they were not significant and hence not considered to have a causal relationship with DT (Table 3). None of the patients were symptomatic for the DT postoperatively with no case of cerebrospinal fluid leakage witnessed.
Distribution of DT in the 2 groups and further subdivided on the basis of duration between LESI and surgery.
Twenty-two NDT complications were seen in the study, of which 10 were in the LESI groups and the rest in the non-LESI group over the 6-month postoperative period (Table 4). These were further subdivided into surgical and medical complications. The difference in the incidence of complications in the 2 groups was not significant (P = 0.83). Surgical complications included surgical site infections (SSI) and neurological complications arising after the surgery. One SSI was seen in the LESI group and 2 were seen in the non-LESI group. One SSI in the non-LESI group required surgical debridement, and the others were managed conservatively with dressing and antibiotics. Two incidences of new-onset neurological complications were seen in each group. These included a case of urinary incontinence in 1 patient in the LESI group, which was managed with a revision surgery with decompression and interbody fusion. Three patients developed new-onset radiculopathy that was managed with a revision decompression in 2 cases within 6 weeks of the first surgery, and the symptoms were relieved in both. One patient reported resolution of the symptoms at 6 weeks with conservative management.
Non-dural tear complications between the 2 groups.
Medical complications were seen in 15 patients, of which 7 were in the LESI group and 8 were in the non-LESI group (Table 4). These included 5 urinary tract infections, which were managed with antibiotics; 2 episodes of pneumonia, which were treated under specialist care in the postoperative intensive care unit; and 3 episodes of deep venous thrombosis, which were also managed conservatively. One patient in the LESI group was complicated with delirium, which also required intensive care for a week. One patient in the non-LESI group was diagnosed with a major depressive disorder 1 month postoperatively. Two patients in the LESI group and 3 patients in the non-LESI group required readmission within 1 month of discharge after the surgery.
Discussion
LESI remains one of the most commonly used management modalities in cases of a PIVD, and its use has gradually increased. Although the short-term results have generally been encouraging, the long-term results remain controversial.3,5 Functional outcomes have been shown to be similar or even slightly worse in the patients who have had an LESI before the surgery.7,9 Also, with the widespread use of MISS, the scenario has changed a lot. In general, MISS has shown to have comparable or even lesser complications compared to the open surgery, and whether this is reflected in the cohort of patients having already received the LESI remains a topic of discussion with not enough data available in the published literature to either support or refute the same.10–12 Furthermore, we could not find a single study in the published literature comparing the complications following MISS in patients receiving a prior LESI. Evaluation of complications after LESI in open surgery has been described to some extent but has centered mainly around SSIs.7,13,14
The demographic variables were comparable in the 2 groups as was the prevalence of comorbidities. The majority of the patients were less than 50 years old with 108 (83.7%) and 161 (86.5%) of the patients in the LESI and non-LESI group, respectively, being ≤50 years old thereby representing a younger population. The mean duration of symptoms was significantly higher in the LESI group (3.5 ± 1.5 months) as compared to the non-LESI group (2.9 ± 1.8 months). It was most likely due to the temporary or partial relief obtained after the LESI that delayed the surgery.
The present study reported an overall incidence of DT of 6.67% after MISS, which was comparable to that published in the literature.12,15–17 The incidence of DT after LESI (10.08%) was higher than that in the control group (4.30%; P < 0.05). Several studies have evaluated the risk factors for DT. Advanced age, obesity, diabetes mellitus, female gender, and revision surgeries have been stated as high-risk factors.16,17 However, a preoperative LESI as a risk factor has not been widely studied, especially after MISS. We observed that a preoperative LESI given within 3 months of the surgery leads to a 3.24 times higher risk of an intraoperative DT, which was statistically significant (P < 0.05). This significance was not observed beyond 3 months. A similar finding was also seen by Labaran et al, but they observed a significantly higher OR up to 6 months.14 However, Kolstov et al found that a preoperative LESI does not lead to a higher incidence of DT.13 None of these studies stated if they included patients operated by open or MISS approaches. Also, both the studies had a higher mean age as compared to our study. MISS has shown to have variable incidences of DT as compared to open surgeries and thus the results from the open surgery cannot be extrapolated to the minimally invasive approach.11,12,15 Hence, the present study is unique as all the patients were operated upon by the MISS approach exclusively.
The higher incidence of DT can be explained by the direct effects of steroids on the local tissue. The most common structure in the extracellular matrix of the meninges has been shown to be collagen with its various types like I, II, and IV. These are produced by the fibroblasts that are also commonly found there.18 Dura injected with corticosteroids showed a significantly decreased number of the intracytoplasmic mitochondria in the dural fibroblasts leading to an inhibitory effect on their function.19,20 This leads to a decreased production of collagen eventually causing a compromise in the material properties of the dural tissue that can make it susceptible to tear with even a minor injury. This can also explain the increased incidence of DT seen in the patients injected with a steroid within 3 months of the surgery as the effects of steroid are the highest then, with a gradual reduction as time passes with the return to a normal function of the fibroblasts.
We observed a comparable rate of postsurgical infection among the 2 groups. Kolstov et al and Hartveldt et al also witnessed similar infection rates after LESI injection as compared to the non-LESI group13,21 In contrast, Zusman et al observed a 7.4-fold greater risk of infection in patients receiving LESI before the surgery, which was attributed to the epidural scarring, increased vascularity, and introduction of infection at the time of injection.7 A higher infection rate was also noted elsewhere.22,23 Yang et al reported a 3.2 times higher rate of infection when LESI was given within 1 month of surgery.22 Another study demonstrated an increased risk of postsurgical infection between 1 and 6 months after epidural steroid administration.23 No infection in any group was seen by Ozturk et al.24 A comparable infection rate in our study could be explained by the minimally invasive nature of the surgeries. We also performed the procedure of LESI administration under strict aseptic precautions. Also, a much smaller sample size owing to a single center nature of the study as compared to some of these studies, which included large databases, can cause a sampling bias.
We noticed that the resurgery rates were comparable among the 2 groups, which was contrary to the findings of Kolstov et al, who observed a higher rate of resurgery within a month of the surgery in the LESI group.13 However, the incidence of a new-onset neurological symptom after the surgery was comparable to their study. Similarly, other complications including medical conditions were also comparable. Of note, we did not witness any case of mortality up to 6 months after surgery. We also witnessed psychiatric complications in the postoperative period. One case of delirium was seen in a 57-year-old woman in the LESI group, which was managed by the multidisciplinary team of neurologists, psychiatrists, and intensivists. It was attributed to a lower hematocrit and serum sodium level perioperatively and a gradual correction resulted in the recovery of the patient. The above-mentioned risk factors have already been described in the literature.25 A case of major depressive disorder was reported 1 month postoperatively in a 41-year-old man in the non-LESI group and was managed under the care of a psychiatrist with pharmacotherapy and behavior therapy. Spine surgery has been described as a risk factor for the development of new-onset depression, and it is essential to keep a watch for these complications postoperatively to obtain a better result.26
The study has a few limitations. First, the effect of these complications on the functional outcomes is not studied, and thus a direct correlation between the incidence of complications and outcomes cannot be obtained. Second, the smaller sample size could lead to the introduction of bias, especially concerning the rarer complications. A post hoc power analysis was performed, and the power was found to be 52.2%. Thus, a study with a larger sample size done in the future may shed further light on the topic. Third, delayed complications occurring after a duration of 6 months of the surgery are not reported. Finally, the study is limited by its retrospective nature.
Conclusion
In patients operated with MISS, there is a 3.2 times higher risk of an intraoperative DT if the surgery is performed within 3 months of the LESI. Furthermore, the incidences of postoperative infection and other complications remain comparable irrespective of the history of LESI.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Ethical approval was waived by the local Ethics Committee of the hospital in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Data Availability Statement The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.