


Abstract
Background Lumbar laminectomy is a surgical procedure allowing for decompression of neural structures. A wide laminectomy to adequately decompress neural elements without compromising the structural integrity of the spinal column is ideal. Pars interarticularis fractures with spinal instability after isolated laminectomy from overresection of the posterior elements have been reported. There are limited anatomical studies in the spine literature that measure the pars interarticularis distance (PID) and spinal canal width (SCW) in the lumbar spine.
Objective The purpose of this study was to assess the differences in PID and SCW at each level of the lumbar spine and to determine their effects on the extent of laminectomy at each lumbar level.
Methods We performed an anatomic study measuring PID and SCW in the lumbar spine from 93 skeletally matured osseous specimens. Groups were compared using an independent sample t test, 1-way analysis of variance, and Wilcoxon test, and significance was set at P < 0.05.
Results Our study suggests that the distance between PID and SCW increases from L1 to L5 in African American and Caucasian women and men. However, the respective increase in SCW at each lumbar level is less than the respective increase in PID at the same levels. This trend suggests that there is a wider window available for decompression without compromising spinal stability in the lower lumbar spine compared with the upper lumbar spine.
Conclusions Our findings suggest that the upper lumbar spine has a narrower window for decompression; therefore, care should be taken to preserve as much of the pars at L1-L3. Understanding the variations in PID and SCW in the lumbar spine will help surgeons perform adequate decompression of a stenotic canal while avoiding postoperative spinal instability.
Clinical Relevance Awareness of PID to SCW ratio may help spine surgeons avoid iatrogenic instability, postoperative intractable back pain, spondylolisthesis, or complications involving alterations of the lumbar spine biomechanics.
Level of Evidence 3.
- pars interarticularis distance
- spinal canal width
- lumbar laminectomy
- lumbar spine anatomy
- iatrogenic instability
- postoperative complication
Introduction
Lumbar spinal stenosis is a degenerative disease that is a well-recognized cause of lower back pain and can cause neurological symptoms such as sciatica, lower extremity pain, claudication, and diminished motor/sensory activity.1 Surgery may be indicated, particularly with worsening of neurological function. Laminectomy is typically performed to minimize pain and restore function by adequately decompressing neural structures.2 In patients with a stable spinal alignment without evidence of instability, such as spondylolisthesis, the goal of surgery is to decompress neural elements while maintaining spinal stability. In this regard, care must be taken to preserve essential components of the posterior ligamentous complex (PLC), particularly when performing laminectomy alone.3
As part of the stabilizing posterior complex, the pars interarticularis (PI) is a bony vertebral segment that lies between the lamina and pedicle and joins the facet joints posteriorly.4 A possible complication arising from lumbar laminectomy is the excessive shear displacement in the intervertebral joint resulting from overresection of the posterior elements.5 This ultimately may lead to symptomatic clinical instability and create the need for instrumented fusion, which exposes the patient to the risks of additional surgery.6 Surgeons typically attempt to limit bone removal along the PI to avoid iatrogenic instability. Case reports of pars fractures after laminectomy due to overresection of the posterior elements have been reported even in the absence of spondylolisthesis.7
There are only a few studies in the literature evaluating the anatomical variations in the PI at different lumbar levels; however, they are limited in the number of specimens available for analysis.8 To the best of our knowledge, anatomical studies in the spine literature that measure correlative values of pars interarticularis distance (PID) and spinal canal width (SCW) are limited; moreover, such values may be predictive when considering the extent of PLC resection during lumbar laminectomy.9 In this study, we aimed to assess the relationship between the PID and SCW in the lumbar spine and correlate such values with various anatomical, demographic, and clinical parameters. We hypothesized that there are significant PID and SCW variations across the lumbar levels that may influence the extent of resection when performing a laminectomy.
Materials and Methods
A total of 93 skeletally matured osseous specimens, collected between 1912 and 1938, were obtained from the Hamann-Todd Osteological Collection in the Cleveland Museum of Natural History. Anatomic studies were conducted on naïve specimens without prior spinal surgery, malformation, or metastatic lesions. We used skeletally matured specimens between the age of 20 and 30 years at the time of death to avoid the presence of advanced degenerative changes that could potentially compromise our measurements.
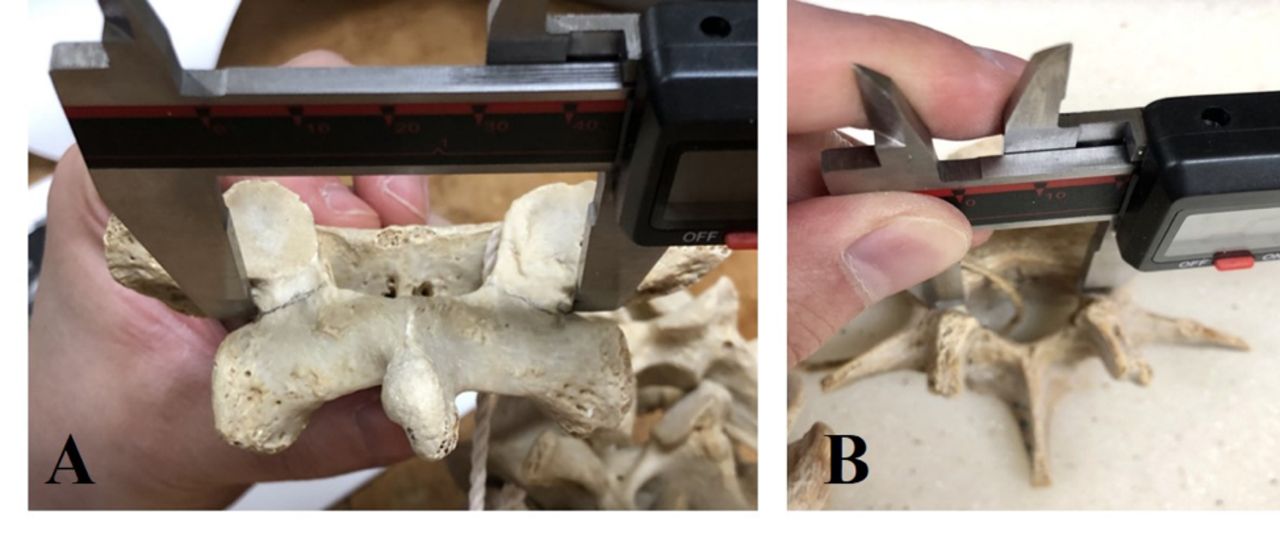
Of the 93 specimens obtained, 50 were men, 43 were women, 50 were of African American (AA) descent, and 43 were Caucasian (Table 1). We defined the PID as the narrowest distance between lateral edges of the PI. The width of the spinal canal was measured from the medial wall of a pedicle to the medial wall of the contralateral pedicle. The PID and SCW were measured at each lumbar level using digital display calipers (Figure 1A and B). Values were averaged and analyzed according to the lumbar level, gender, and race.
Demographics for specimens.

(A) Measuring interpars distance using manual calipers from the lateral edge of one pars to the lateral edge of the contralateral pars. (B) Measuring spinal canal width using manual calipers from the medial cortex of one pedicle to the medial cortex of the contralateral pedicle.
Statistical analyses were conducted on the following groups: lumbar level, gender, and race. Such values were assessed using the independent sample t test, 1-way analysis of variance, and the Wilcoxon test. Means and SDswere calculated, and significance was set at P <0.05. Analyses were performed using SPSS software.
Results
The mean age of death for all specimens was 26 ± 3 years (Table 1). There was a significant increase in the mean PID from L1 to L5 in all specimens, with mean values of 24.61, 26.16, 28.96, 33.43, and 41.57 mm, respectively (P < 0.01) (Figure 2A). For male specimens, the average PID from L1 to L5 was 25.01, 26.6, 29.43, 34.08, and 42.7 mm, respectively. For female specimens, the average PID from L1 to L5 was 24.13, 25.65, 28.41, 32.67, and 40.26 mm, respectively. The mean PID at L1, L2, and L5 was significantly greater in men compared with women (P < 0.05) with no difference at L3 or L4 (Figure 2B).
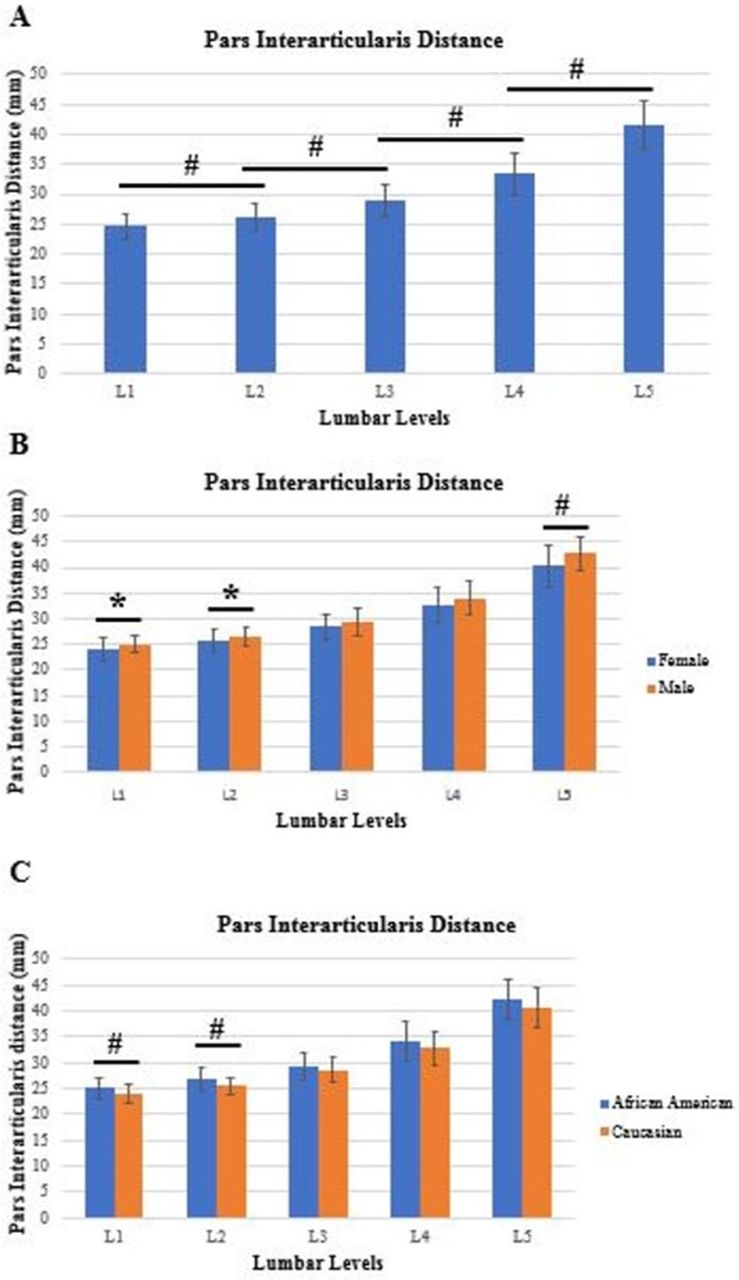
Differences in mean pars interarticularis distance among (A) lumbar levels, (B) sex, and (C) race. *Statistically significant (P < 0.05). #Statistically significant (P < 0.01).
For Caucasian specimens, the average PID from L1 to L5 was 24.01, 25.45, 28.62, 32.76, and 40.7 mm, respectively. For AA specimens, the average PID from L1 to L5 was 25.12, 26.77, 29.25, 34.01, and 42.32 mm, respectively. Mean PID at L1 and L2 was significantly greater in AA compared with Caucasian (P < 0.01) with no difference at L3, L4, and L5 (Figure 2C). Differences in mean PID between lumbar levels were all statistically significant in AA men (P < 0.05), Caucasian men (P < 0.05), and Caucasian women (P < 0.05). Differences in mean PID between lumbar levels were statistically significant in AA women (P < 0.05) except for L1 vs L2 (P = 0.092). Differences in mean PID were not significant at each lumbar level among AA man vs woman, AA man vs Caucasian man, and AA woman vs Caucasian man. Mean PID at each lumbar level was significantly greater in AA men compared with Caucasian women (P < 0.05). L1 and L2 mean PID was significantly greater in AA women than Caucasian women (P < 0.05). L3 and L5 mean PID was significantly greater in Caucasian men than women (P < 0.05) with no differences in the other levels.
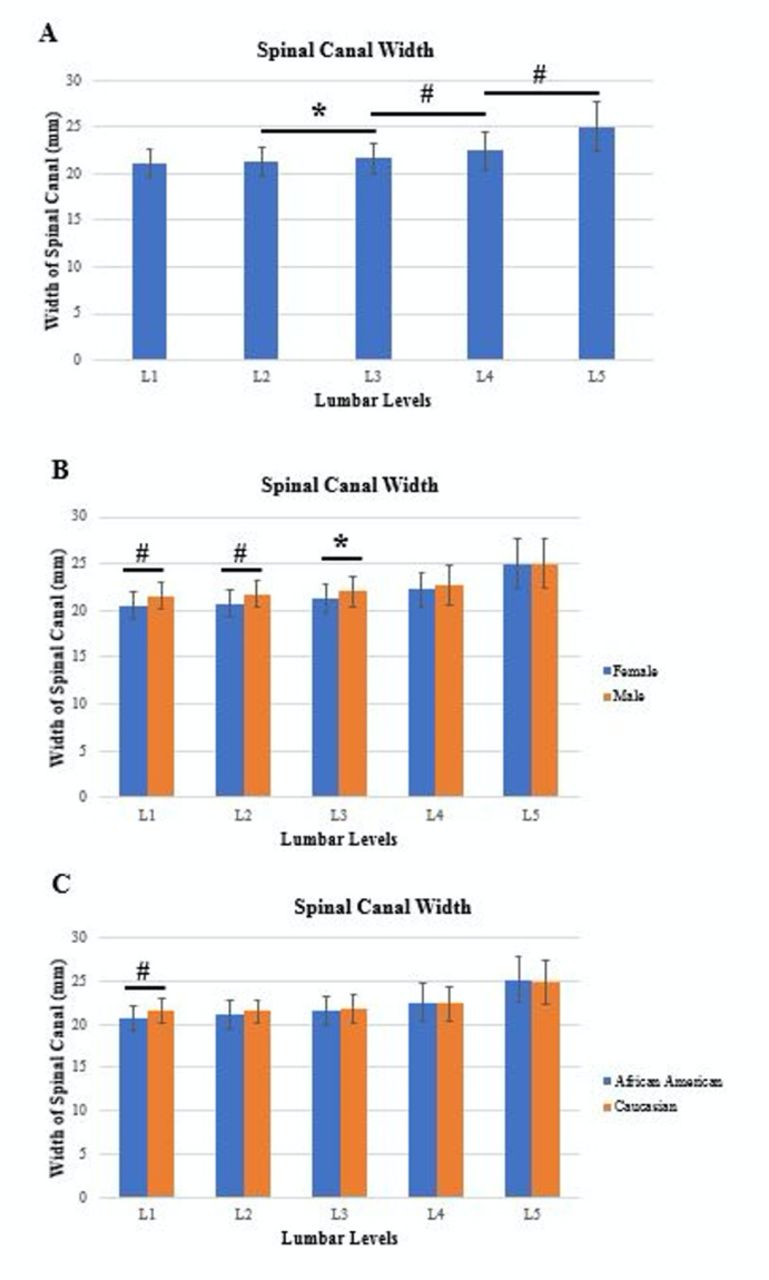
For all specimens, the average SCW increased from L1 to L5 in all specimens, with mean values of 21.07, 21.3, 21.69, 22.48, and 25.01 mm, respectively (Figure 3A). Significant differences were seen among L2-L3 (P = 0.02), L3-L4 (P < 0.01), and L4-L5 (P < 0.01) with no difference between L1 and L2 (Figure 3A). For male specimens, the average SCW from L1 to L5 was 21.55, 21.75, 22.04, 22.7, and 25.01 mm, respectively. For female specimens, the average SCW from L1 to L5 was 20.52, 20.77, 21.29, 22.24, and 25.01 mm, respectively. Mean SCW was significantly greater in men compared with women at L1, L2 (P < 0.01), and L3 (P < 0.05) with no difference at L4 and L5 (Figure 3B). For AA specimens, the average SCW from L1 to L5 was 20.69, 21.13, 21.59, 22.55, and 25.12 mm, respectively. For Caucasian specimens, the average SCW from L1 to L5 was 21.51, 21.49, 21.8, 22.4,1, and 24.89 mm, respectively. Mean SCW was significantly greater in Caucasians compared with AA at L1 (P < 0.01) with no difference at L2, L3, L4, and L5 (Figure 3C). The ratio of PID to SCW significantly increased from L1 to L5 (P < 0.01) (Table 2). Ratios at L1 to L3 were less than 1.5, and ratios at L4 and L5 were 1.5 or greater.
Ratio of pars interarticularis distance to spinal canal width for each vertebral lumbar level.

Differences in mean spinal canal width among (A) lumbar levels, (B) sex, and (C) race. *Statistically significant (P < 0.05). #Statistically significant (P < 0.05).
Discussion
The PI has been shown to play an important role in maintaining the stability of the spinal column. As an integral element of the PLC, it can be subjected to vulnerability under high repetitive stresses.10–12 Therefore, instances of iatrogenic spondylosis can be particularly detrimental to the stability of the lumbar spine. In several biomechanical studies, it has been demonstrated that even unilateral spondylosis of the pars can translate into segmental motion instability.13 Similarly, in a study of adolescent athletes by Sairyo et al, it was shown that more than 50% of this cohort had evidence of contralateral stress fractures and/or radiographic evidence of sclerotic change as the direct result of unilateral pars fractures.13 This concept becomes more relevant when considering factors that may affect outcomes of lumbar spine surgery.
When planning to perform a lumbar laminectomy, considerations such as bone mineral density, intervertebral disc space size, and osteophyte presence are important features to account for. Often, however, concerns of postoperative instability can be associated with overresection of the PLC.14 In a study by Yang et al, the incidence of instability in patients was significantly higher in cases of wide laminectomy as compared with those undergoing partial laminectomy.15 Additionally, in a biomechanical study by Ivanov et al, the authors observed increases in stresses at both the PI and the inferior facet after limited decompressions and suggested that surgeons should be aware of possible stress fractures.16 Therefore, understanding the structural parameters of the PI in relation to the spinal canal can help the spine surgeon strategize the surgical approach and ultimately minimize the risk of postoperative instability.
Morphometric studies have shown the interdimensional relationship among the pedicle, vertebral bodies, and spinal canal; however, the literature is limited in demonstrating the direct anatomic relationship among the pars, SCW, and demographical differences in gender and/or ethnicity.17–19 Given the intricate role of the pars within the posterior complex, it is worthwhile to understand the variations in PID and SCW within the lumbar spine. The ratio of PID to SCW would allow surgeons to better appreciate the window available for laminectomy in order to decompress a stenotic spinal canal while preserving a reasonable amount of bone in the pars to prevent postoperative spinal instability.
In our study, we chose specimens without degenerative changes (eg, osteophytes), which may confound and alter interarticularis distance. We analyzed 465 lumbar vertebral levels using caliper measurements and demonstrated a trend in which the ratio of PID to SCW significantly increases with progressive levels in the lumbar spine. Our data suggest the width between the PI increases from L1 to L5 irrespective of gender or ethnicity, which is similar to findings in previous studies.8 PID was significantly higher in men than women at L1, L2, and L5 and in Caucasians at L1 and L2 compared with AA. Similar to Peters et al, there was an increase in SCW from L2 to L5 with no difference between L1 and L2. SCW at L1, L2, and L3 was significantly wider in men than women and significantly wider at L1 in Caucasians than AA.8 When comparing the increase in SCW with the increase in PID, the increase in SCW across the lumbar levels was less than the increase in PID across lumbar levels, as demonstrated by the ratio of PID to SCW.
We sought to provide a large anatomical cohort study of the lumbar PI and SCW in young cadaveric spine specimens. Limitations in our study include skeletal specimens lacking any soft tissue and ligamentous structures that aid in the structural integrity of the lumbar spine. However, by utilizing our described methods, we allow for a more accurate and accessible analysis of the PID and SCW. Additionally, given that our cadaveric specimens were obtained between 1912 and 1938, it may be unclear whether modern day populations would share similar measurements and proportions given environmental and nutritional differences.19
Conclusion
Our findings provide spine surgeons with a better frame of reference to work within the confines of the lumbar spine. Generally, greater care must be taken when decompressing the canal within the proximal lumbar region because our findings suggest that there is a wider window for decompression and a smaller lumbar PI as one moves cephalad along the lumbar spine. Awareness of the PID to SCW ratio will help spine surgeons avoid iatrogenic instability, postoperative intractable back pain, spondylolisthesis, or complications involving alterations of the lumbar spine biomechanics.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.