


Abstract
Background The present study aimed to assess the efficacy of a new haplo-paraspinal-muscle-preserving (HMP) laminoplasty technique in the treatment of cervical myelopathy.
Methods The medical records of 68 patients diagnosed with multisegmental cervical myelopathy were retrospectively reviewed. Of these, 22 patients who underwent HMP laminoplasty were defined as the muscle-preserved group (MP), and 46 patients who underwent traditional open-door laminoplasty were enrolled and defined as the traditional open-door laminoplasty group (LP). Patient demographic data and surgical parameters like clinical and radiological parameters, operation duration, blood loss, and spinal canal expansion distance were compared.
Results Average surgical time and blood loss were significantly reduced in the MP group when compared with the LP group (P < 0.05). Both groups demonstrated significant improvements in neurological function and spinal canal expansion (P > 0.05). However, the visual analog scale score in the MP group was significantly lower compared with the LP group at the 6-month follow-up (P < 0.05), but no differences were found at the 1-year follow-up. The loss of lordosis was more prominent in the LP group when compared with the MP group at 1-year follow-up (P < 0.05). Lower events of persistent axial pain were found in the MP group but with no statistical significance. More hinge side laminae fractures could be found in the MP group, but more hinge side displacements were found in the LP group.
Conclusions The HMP laminoplasty technique is relatively safe, effective, easier to perform, and better for lordosis maintenance and complication control compared with the traditional open-door technique.
Clinical Relevance Although traditional open-door laminoplasty is an efficient approach in treating multisegmental cervical myelopathy, the complications could significantly affect the clinical outcome. Our new HMP laminoplasty technique has a lower complication rate and a better lordosis maintenance ability; therefore, it could be a better choice in treating multisegmental cervical myelopathy.
Level of Evidence 3.
Introduction
Laminoplasty has been proved to be an effective way to treat cervical myelopathy like ossification of the posterior longitudinal ligament or multilevel compressive disc herniation.1 As one of the most common posterior approaches in cervical spine surgery, laminoplasty is an established method to reconstruct the posterior elements of the cervical vertebrae, thus expanding the spinal canal, and is proved to be a safe and effective alternative approach compared with laminectomy.2 Although cervical laminoplasty has many merits over laminectomy and is a motion-preserving procedure compared with other fusion techniques, several complications at long-term follow-up affect the clinical outcome of the surgery, such as postoperative axial neck pain, C5 nerve root palsy, progressive lordosis loss, and reduction of cervical range of motion.3 The reason for such complications is believed to be related to the surgical nature of laminoplasty, like dissection of paraspinal muscles and ligaments attached to the laminae and spinous process, and the overtraction of the nerve root due to spinal canal expansion and spinal cord shifting.4,5 Since postoperative axial neck pain is more frequently observed in laminoplasty-treated patients, different surgical techniques were developed to protect the spinal muscles, thus reducing postoperative axial pain and lordosis loss after laminoplasty surgery.5–8
Studies have shown that protecting either C2, C6, and C7 spinous muscle and ligament attachment was effective in lowering the incidence of postoperative axial pain.9,10 However, such techniques may cause insufficient decompression of the spinal canal as both sides of the paraspinal muscles are prevented from complete dissection, and the force of the muscle strain could limit the expansion distance. In this study, we report a new surgical strategy named the haplo-paraspinal-muscle-preserving (HMP) technique, which could be an alternative strategy to solve these problems in laminoplasty.
Materials and Methods
Ethics Approval and Consent to Participate
This retrospective study was approved by our institutional ethics committee and Institutional Review Board (IRB number: 2021SL044). Written informed consent was obtained from all participants.
General Information
In this study, we retrospectively reviewed 68 patients diagnosed with multilevel cervical myelopathy from August 2019 to August 2020. Of these, 22 patients who underwent HMP laminoplasty were defined as the muscle-preserved group (MP group; 14 men, 8 women, mean age 61.2 ± 6.4 years), and 46 age- and sex-matched patients who underwent traditional open-door laminoplasty were defined as the traditional open-door laminoplasty group (LP group; 29 men, 17 women, mean age 60.9 ± 5.9 years). The inclusion criteria were as follows: (1) patients had typical cervical myelopathy symptoms and radiological examinations found the presence of either disc herniation or multilevel ossification of posterior longitudinal ligament; (2) diagnosed patients underwent cervical laminoplasty using either traditional open-door laminoplasty or the HMP technique; (3) surgically treated patients had >6 months of follow-up. Exclusion criteria were: (1) patients with cervical kyphosis >10° or who were K-line negative; (2) patients diagnosed with trauma, tumor, infection, or other systematic diseases; (3) patients with a mental or neurological disorder causing neurological symptoms. Patient characteristics such as age, sex, body mass index, and symptomatic duration were obtained before surgery.
Surgical Procedure
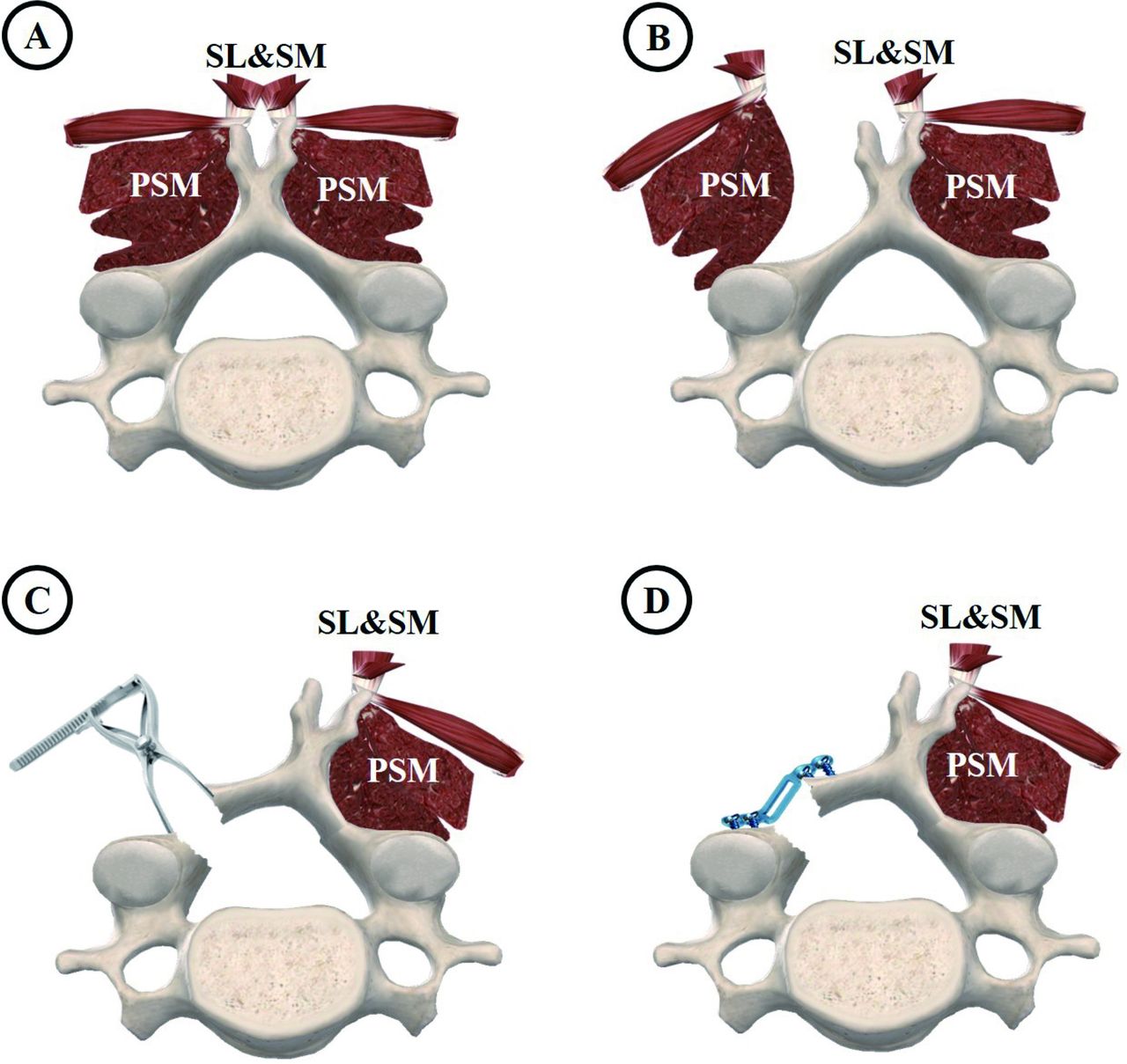
The surgical procedure of HMP laminoplasty is based on traditional open-door laminoplasty (Hirabayashi style) with modifications. A midline cervical back skin incision was made from the C2 (or C3) spinous process to the C7 (or C6) spinous process. The nuchal ligament was incised in the midline, and then the incision was continued only on one side of the splenius capitis and the semispinalis capitis down to the spinous processes from C2 (or C3) to C7 (or C6). Unilateral muscles attached to the spinous processes were preserved by the procedures, while the other side was dissected. The multifidus and rotatory muscles were dissected subperiosteally and retracted laterally off the inferior part of the spinous processes, laminae, and medial aspects of the facets at the open-door side (Figure 1). The facet capsules must be preserved, and the opening side is usually placed on the side that has worse symptoms or severe stenosis and compressions because it is technically easier to perform additional foraminotomy or other techniques to decompress the foramen and nerve root. A high-speed drill is used to cut the outer cortex at the junction of laminae and lateral mass in the process of door-opening, and a Kerrison rongeur is used to remove the ventral laminae cortex, thus creating a gutter to open the laminae. A small vertebral spreader was used to assist the opening of the laminae little by little to prevent hinge side fracture (Figure 2A–B). Epidural bleeding is controlled by bipolar electrocautery and absorbable hemostats. When the lamina is tilted, a Woodson elevator can be used to release any adhesions between the dura and ventral lamina on the open-door side. Subsequently, until the lamina is opened sufficiently, we fix an appropriately sized double-bent titanium miniplate (ARCH plate, DePuy Synthes, USA) via cortex screws on both the laminar and lateral mass sides (Figure 2C).

Illustration showing the surgical steps of haplo-paraspinal-muscle-preserving (HMP) technique in laminoplasty. (A) Representative image showing the structure of the cervical vertebra and its posteriorly attached muscle. (B) The main difference between the HMP technique and traditional laminoplasty is that only half of the laminae that are to be opened during the laminoplasty procedure are exposed. The paraspinal muscle is only dissected on the left side of the spinous process, and the right side of the paraspinal muscle remains intact. (C) After exposure, the left sides of the laminae are opened and flipped using a small vertebral spreader. During the opening, the spreader slowly separates the laminae to prevent hinge side laminae fracture. (D) After opening the spinal canal, an ARCH plate is fixed to maintain the canal enlargement. PSM, paraspinal muscles; SL, spinous process–attached ligaments; SM, spinous process–attached muscles.

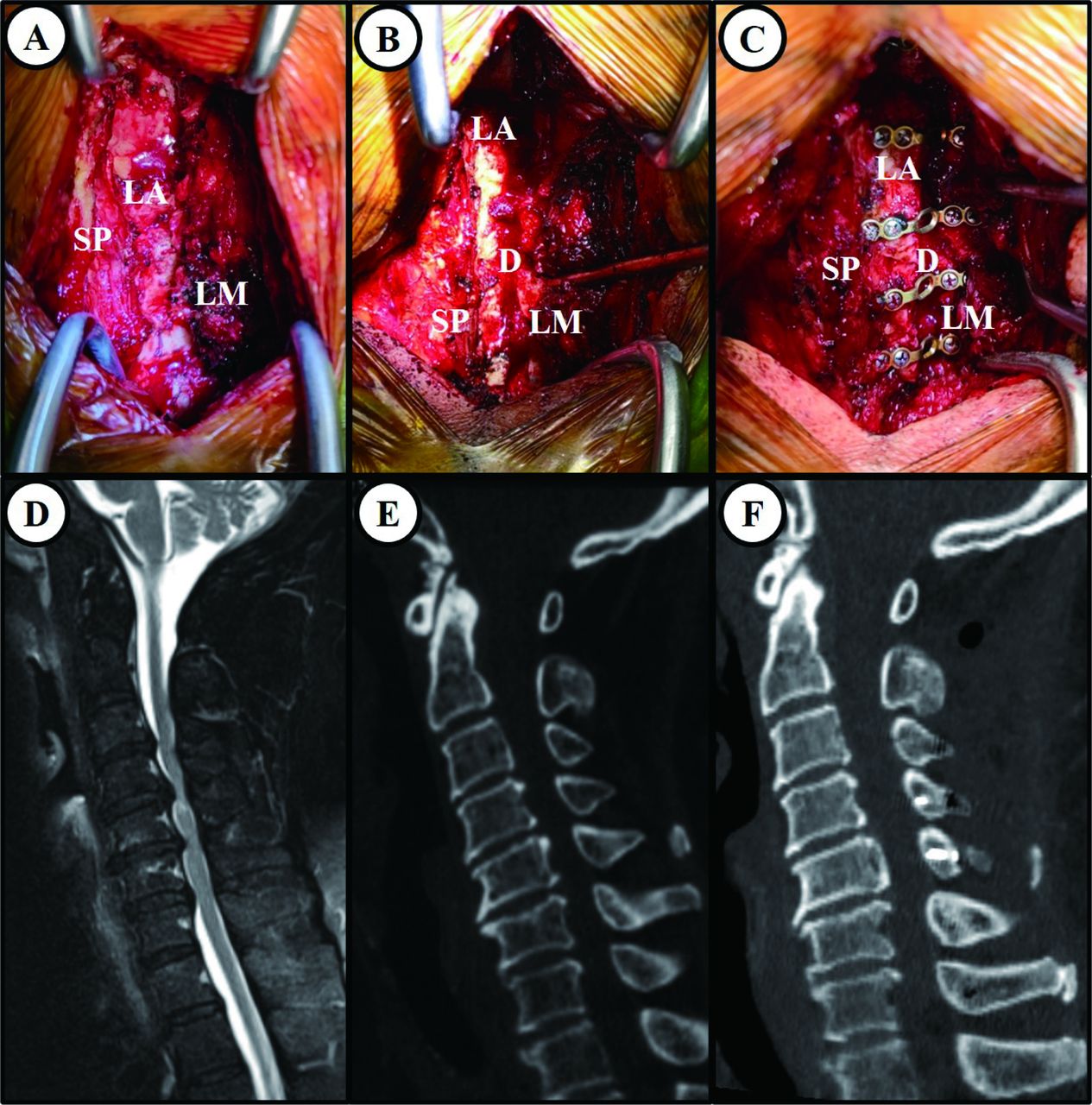
The surgical view, radiographic outcome, and intraoperative images showing the process of laminoplasty using the haplo-paraspinal-muscle-preserving (HMP) technique. (A) Only one side of the laminae is exposed and the paraspinal muscles, as well as spinous process–attached ligaments and muscles of the other side, were prevented from being dissected. (B) The laminae were cut to create an opening of the spinal canal with the assistance of a small vertebral spreader. (C) ARCH plates were used after the opening to finish the laminoplasty procedure. The radiological images show the preoperative magnetic resonance images (D), preoperative reconstructed computed tomography (E), and postoperative reconstructed computed tomography (F) of the same patient that received HMP laminoplasty. Note that the spinal canal is significantly enlarged after the surgery. LA, laminae; LM, dissected laminae–attached muscles; SP, spinous process.
The surgical procedure of traditional open-door laminoplasty is similar, but there is a bilateral muscle dissection and a hinge side gutter is created to facilitate the opening procedure, as documented before.5
Radiographic Analysis
General Measurement Methods
Cervical spine anteroposterior, lateral, flexion, and extension x-ray radiographs and cervical spine high-resolution computed tomography (CT) images were taken preoperatively and postoperatively. Radiological measurements were performed using the Centricity PACS 4.0 system (GE Healthcare, USA), and a contrast adjustment was made to visualize the vertebrae of the entire cervical spine. Two independent clinical research assistants, who were not involved with the study and were blinded to all clinical information, performed radiological measurements, and the average values of both observers were used in the present study.
Cervical Lordosis
Cervical lordosis was assessed using the C2–C7 Cobb angle as a measure of cervical alignment, which was defined as the angle formed by the inferior endplates of C2 and C7 in lateral-positioned radiographs. The loss of lordosis was calculated by comparing the initial postoperative C2–C7 Cobb angle with that of the final follow-up in standing lateral radiographs and using the following formula: lordosis loss (°) = (postoperative C2–C7 Cobb angle) − (final follow-up C2–C7 Cobb angle).11
Spinal Cord Expansion Distance
Spinal cord expansion distance was calculated by comparing the distance of laminae to the posterior margin of the vertebrate on horizontal CT images before and after surgery using the following formula: Spinal canal expansion (mm) = (postoperative spinal canal distance) − (preoperative spinal canal distance).12 The mean distance of each level in one patient is used for comparison for each group.
Paraspinal Muscle Volume Evaluation
The T2-weighted axial magnetic resonance images (MRIs) from levels C3 to C7 were used to quantify the volume of posterior paravertebral muscles. The muscle areas of the multifidus muscle, semispinalis muscle, and longissimus muscle were added and calculated as a group using RadiAnt DICOM Viewer software (Medixant Corporation, Poznan, Poland), and 2 image slices from each level were used for calculation. The average of the 2 measurements of each level was the representative area data, as described in previous studies.13 Two independent clinical research assistants, who were not involved with the study and were blinded to all clinical information, performed radiological measurements, and the average values of both observers were used in the present study.
Outcome Measurements
Surgical Information
Surgical duration, intraoperative blood loss volume, and intraoperative cerebrospinal fluid (CSF) leakage were documented in each patient for further comparison.
Neurological Function Assessment
The Japanese Orthopaedic Association (JOA) scoring system was adapted to evaluate neurological function. We used the neurological function improvement rate (IR) to assess symptom improvement, which was calculated as IR = (JOA scores 12 months after surgery − preoperative JOA scores) / (17 − preoperative JOA scores) × 100%.14 Two independent clinical research assistants, who were not involved with the study and were blinded to all clinical information, performed the assessments, and the average values of both observers were used in the present study.
Neck Pain Assessment
Neck pain was measured by the visual analog scale (VAS) system. Two independent clinical research assistants, who were not involved with the study and were blinded to all clinical information, performed the assessments, and the average values of both observers were used in the present study.
Complications
Postoperative CSF leakage, incidence of axial neck pain, and C5 nerve root palsy were recorded in both groups. Persistent axial neck pain was defined as unrelieved axial pain for >6 months.
Statistical Analysis
Data analyses were conducted using SPSS Statistics 20 for Windows (SPSS, Inc, Chicago, IL, USA). Data are presented as the number of subjects in each group or mean ± SD. Each independent variable, such as age, sex, follow-up period, JOA score, VAS score, and C2–C7 Cobb angle, was compared between the 2 groups using the Mann-Whitney U test for continuous variables, and the χ2 test or Fisher exact test for categorical variables. A statistically significant difference was set at P < 0.05.
Results
General Results
Of 68 total patients, 22 patients underwent HMP laminoplasty and were defined as the MP group, and 46 patients underwent a traditional single open-door laminoplasty using high-speed drills and were defined as the LP. There was no significant difference among age, sex, body mass index, operated levels, preoperative JOA score, and VAS score between the 2 groups (Table 1, P > 0.05). All patients enrolled had a follow-up period >12 months.
Comparison of patient demographics by laminoplasty group.
Surgical Outcomes
The average time of operation was 50.5 ± 12.8 minutes in the MP group, which is significantly lower (P = 0.01) than that of the LP group (74.0 ± 17.8 minutes, Table 2). In addition, the mean blood loss volume was 92.5 ± 49.3 mL and 189.4 ± 62.7 mL, respectively, with MP groups showing less than half of blood loss compared with the LP group (P < 0.01). Only 1 patient had CSF leakage during surgery in the LP group (P = 0.68). The initial spinal canal expansion distance showed no significant differences between the groups (P = 0.35, Figure 2D-F).
Comparison of surgical parameters between laminoplasty groups.
Radiographic Results
The preoperative C2–C7 Cobb angle was 10.2° ± 2.8° in the MP group and 10.8° ± 2.6° in the LP group, with no statistical difference between the groups (P = 0.65). At 6 months follow-up, the C2–C7 Cobb angle slightly increased in the MP group (to 11.7° ± 2.8°) and slightly decreased in the LP group (to 10.6° ± 2.7°). At the final follow-up, the C2–C7 Cobb angle was 10.7° ± 2.3° in the MP group and 9.2° ± 2.4° in the LP group, with significant differences between the groups (P < 0.01). The loss of lordosis in the 2 groups also showed significant differences (P = 0.01), with 1.4° ± 1.2° in the LP group and 0.7° ± 1.1° in the MP group (Table 3).
Postoperative clinical data comparison of the patients by laminoplasty group.
Clinical Outcomes
Neurological Function Assessment
Both groups demonstrated a significant improvement in neurological function, and there were no significant differences between the groups in JOA score (Table 3, P > 0.05) and IR rate (Table 3, P = 0.23).
Neck Pain Assessment
The average VAS scores decreased from 5.3 ± 2.6 to 2.5 ± 1.6 and from 5.2 ± 2.7 to 3.8 ± 1.6 for the MP and LP groups, respectively, with a significant difference between the 2 groups (Table 3, P < 0.01) at the 6-month follow-up. However, the VAS score of the final follow-up did not show a significant difference (P = 0.15).
Complications
For complications, 2 patients in the MP group and 7 patients in the LP group experienced persistent axial pain during the follow-ups, and all recovered within 1-year postoperation. Although there was no statistical significance between the groups, the percentage of persistent axial pain was lower in the MP group (Table 3, P = 0.75). In the LP group, 2 patients suffered C5 nerve root palsy after the surgery, while no events happened in the MP group (Table 3, P = 0.68). One patient in the MP group and 4 patients in the LP group experienced CSF leakage after the surgery (P = 0.91). There were no nerve root injuries, postoperative hematomas, or other complications that occurred after the operation.
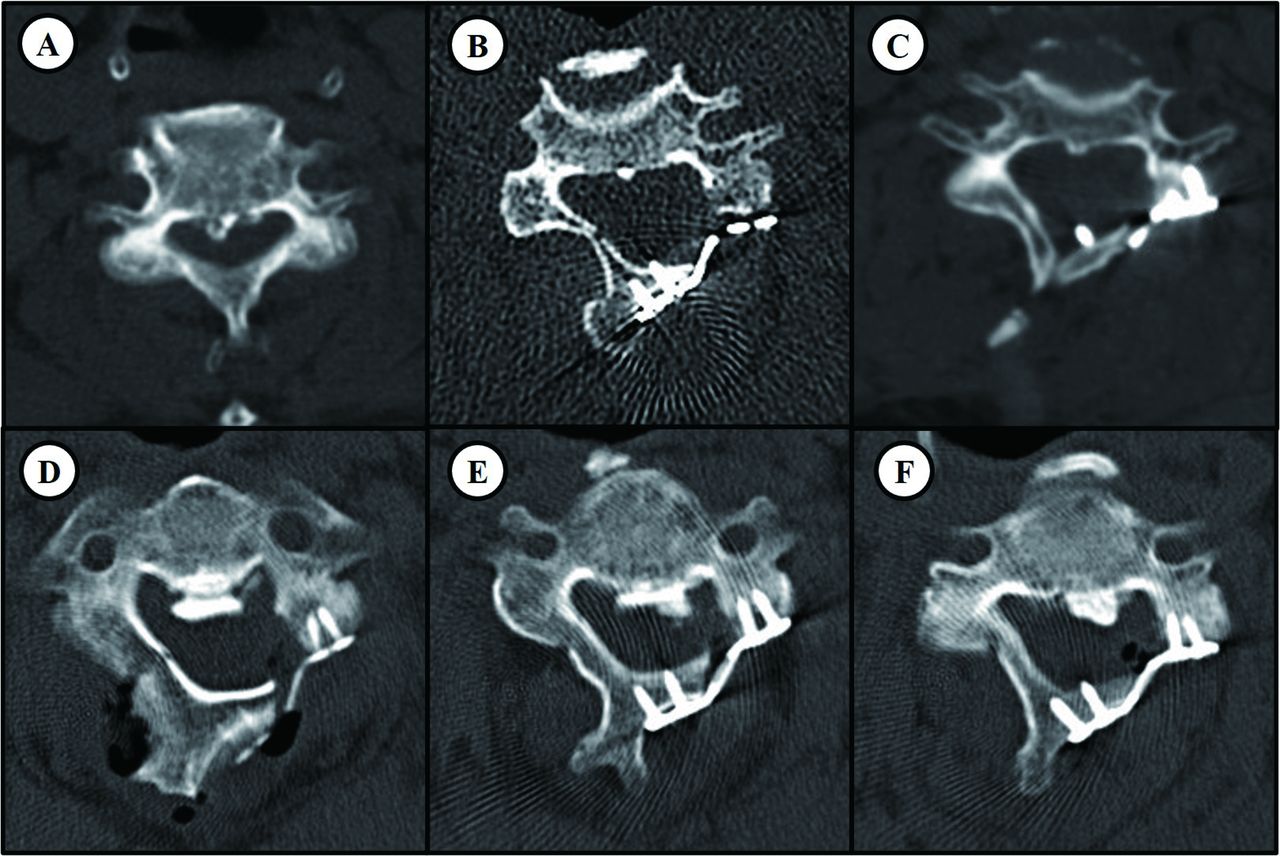
In the MP group, more hinge side fractures were found after the surgery in CT images (Table 4, P < 0.01). However, most hinge side fractures in the MP group occurred at the ventral lamina cortex, while the dorsal cortex was relatively intact (67 levels of ventral cortex fractures and 9 levels of dorsal cortex fractures). Complete fractures on both ventral and dorsal lamina cortexes were less frequent in the MP group (Table 4, P < 0.01), and no hinge side displacement was found in the MP group, while 3 levels of displacement were found in the LP group (Figure 3). No dorsal lamina cortex fractures were documented for the LP group because the diamond bar already removed the cortex of the hinge side lamina to make the hinge gutter (Figure 3).
Comparison of hinge side fractures between laminoplasty groups.

Computed tomography (CT) images showing the typical characteristics of hinge side fractures in different laminoplasty techniques. Typical CT images of a hinge side fracture in the C4 level of an haplo-paraspinal-muscle-preserving laminoplasty–treated patient (A–C). Stenosis is observed preoperatively (A), and the spinal canal enlarged significantly after the surgery (B), with a fracture in the cortical bone of the ventral side of the hinge laminar while the dorsal side of the hinge remained intact. The fracture is healed 6 mo after the surgery, with no sign of cortical bone fracture of the hinge side (C). Typical CT images of hinge side fractures in the C3 (D) and C4 (E) levels of a traditional laminoplasty–treated patient. The C5 (F) level is intact. Both ventral and dorsal sides of the hinge side laminae were compromised when the fracture occurred (D–E); typically, the dorsal side of the hinge is thinned due to the removal of cortical bone to form a hinge (F).
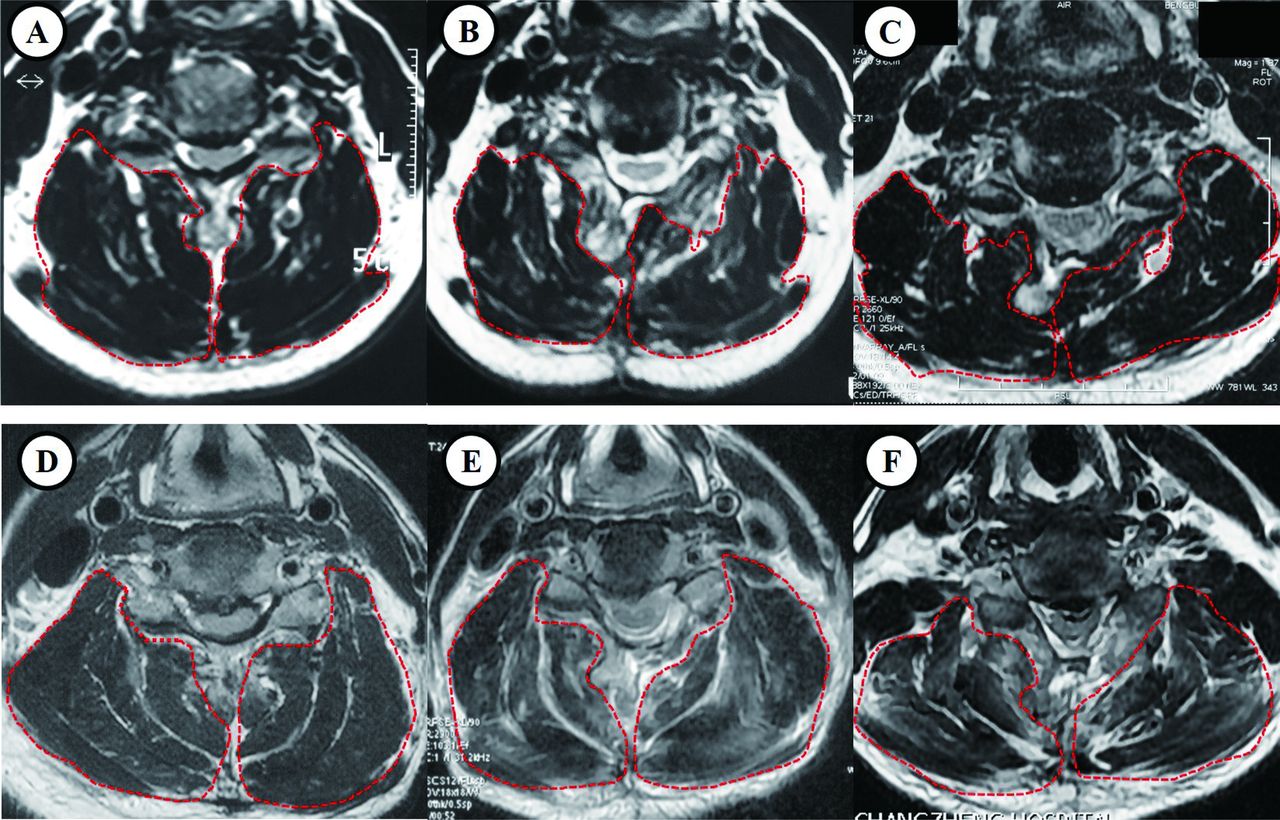
Moreover, we assessed the volume of posterior paravertebral muscles in patients before surgery, 3 days after surgery, and at 1-year follow-up (Figure 4). The changes in posterior paravertebral muscle volume on the open-door side were not significant between the 2 groups at each timepoint (Table 5). However, the changes in posterior paravertebral muscle volume on the hinge side decreased significantly in the LP group compared with the MP group at 3 days postoperation and at 1-year follow-up (Table 5, Figure 4).

Magnetic resonance images (MRIs) showing the posterior cervical paravertebral muscle volumes between different laminoplasty groups. Case example of a 55-year-old female patient who received traditional laminoplasty, with the T2-weighted axial MRI showing the paravertebral muscle volumes (A) preoperation, (B) 3 days postoperation, and (C) 1 year postoperation. Case example of a 57-year-old male patient who received haplo-paraspinal-muscle-preserving laminoplasty, the T2-weighted axial MRI showing the paravertebral muscle volumes (D) preoperation, (E) 3 days postoperation, and (F) 1 year postoperation.
Comparison of the posterior cervical paravertebral muscle volumes.
Discussion
Essentiality of Preserving Muscle Attachments in Laminoplasty
The main purpose of laminoplasty techniques is to expand the narrowed spinal canal by reconstructing the laminae to provide additional space for the spinal canal. Although muscles and ligaments attached to the laminae and spinous process are recognized as important components of neck dynamic equilibrium,15,16 dissecting paraspinal muscles is unavoidable during laminoplasty. On the other hand, sufficient opening of the laminae requires a wide range of posterior muscle and ligament dissection, which may thus further damage the stability of the neck, causing many complications like reduction of cervical range of motion and postoperative axial neck pain.17 Many muscle-sparing laminoplasty techniques have been developed based on this thesis for open-door laminoplasty.7,9,10,18 Many studies have focused on preserving the muscle attachment to the C2 or C7 spinous process, following demonstrations that muscle detachment at these levels greatly affect the incidence and severity of axial pain after laminoplasty.19
The decompression of the C2 and C7 levels will be accompanied by the sacrifice of the cervical deep extensor, especially the semispinalis cervicis, which plays an important role in maintaining the lordosis and alignment of the cervical vertebrae.20 Additionally, many researchers have suggested that laminoplasty preserving the posterior deep extensor muscle could decrease the atrophy rate and reduce the incidence of postoperative axial symptoms.21,22 However, we believed that dissection of the paraspinal muscle at each cervical spine level, not only in the C2 and C7 levels, will add to the damage of the stability of the posterior cervical structure, thus increasing the incidence of complications. So, in this study, we proposed a new muscle-preserving laminoplasty technique to minimize dissection of the paraspinal muscle by only exposing the door side laminae, which left the hinge side muscle and ligament intact and untouched, greatly preserving the paraspinal muscle from dissection and further functional damage.
Initial Outcome of HMP Laminoplasty
In this study, we reviewed the clinical outcome of 22 multilevel myelopathy patients who underwent HMP laminoplasty and compared them with age-matched multilevel myelopathy patients who underwent traditional open-door laminoplasty. The major difference of this new muscle-preserving open-door laminoplasty strategy compared with the traditional one is that we only expose the door side laminae and preserve the hinge side muscle from dissection. This haplo-muscle-dissection procedure greatly preserved the muscle and ligament attachment to the cervical laminae and spinous process, and indeed the patients showed better neck pain recovery than the traditional laminoplasty-treated patients (at 6-month follow-up), which confirmed the hypothesis that muscle preservation in laminoplasty can greatly affect the level and incidence of postoperative axial pain.
Another interesting finding is that HMP laminoplasty-treated patients showed better-sustained lordosis than the traditional laminoplasty-treated patients. Reports have shown that patients who undergo laminoplasty tend to undergo a change in kyphotic alignment and increased axial neck pain, which can lead to poor surgical outcomes.23,24 One possible cause may be due to the surgical strategy used in laminoplasty. Due to a different rationale, some clinicians prefer traditional open-door laminoplasty (the Hirabayashi type) while others prefer double-door laminoplasty (the Kurokawa type), and coincidentally, the incidence of postoperative lordosis loss is slightly higher in the double-door laminoplasty–related studies compared with the open-door laminoplasty studies.23 And interestingly, many reports of different posterior element–sparing techniques or restriction of the laminoplasty from C3 to C6 instead of C7 are shown to reduce kyphosis.7,25,26 These studies have shown that when less of the posterior element is compromised, it may improve the lordosis of laminoplasty-treated patients and thus affect the overall clinical outcome. In our data, we found that HMP laminoplasty-treated patients showed slightly improved cervical lordosis even after 6 months of follow-ups, while the cervical lordosis was slightly reduced at the 6-months follow-up in the open-door laminoplasty group, with continued loss of lordosis at the 1-year follow-up (Table 3). The results were consistent with the former hypothesis that more muscle protection may result in less lordosis loss.
We also found that hinge fractures occurred more often in HMP laminoplasty-treated patients, for 67 levels of ventral cortex fracture and 9 levels of dorsal cortex fracture (Table 4), while only 25.1% of the traditional open-door laminoplasty–treated levels were found. One of the main characteristics in the HMP laminoplasty–related hinge fracture is that it happened mostly in the ventral cortex of the lamina, while the dorsal side remained intact. This is probably related to the opening of the lamina that the cortex of the ventral side stretched most, while the dorsal side cortex receives compressive forces. However, although more hinge fractures could be found in HMP laminoplasty-treated patients, no hinge side displacement was found. We think that it is likely due to the muscle attachment to the hinge side lamina that restricts the fractured hinge from moving into the spinal canal, causing neurocompression. In the traditional open-door laminoplasty-treated patients, the dorsal side of the lamina cortex is already compromised, and if the ventral cortex breaks, it is very easy to cause a complete fracture and make the fractured hinge side move about, thus endangering the nerve root and the dural sac.5,27
Other Merits for HMP Technique
Despite the findings in this study, the HMP technique may have other merits over traditional open-door laminoplasty. It may be effective in revisions of minimally invasive cervical surgeries as it can easily avoid exposing the precedent surgical site, which may cause CSF leakage if an incision is made there. Another merit is that such a technique greatly lowers the risk of intraoperative complications related to poor health conditions like myocardial diseases, respiratory system–related diseases, and osteoporosis, because it halves the surgical time and blood loss and provides additional protection to the hinge side laminae via the attached muscles to reduce the possibilities of total fracture and fixation failure.
Although many studies have demonstrated their muscle-preserving techniques, we believed that our HMP laminoplasty strategy has merits over the reported ones. Many muscle-preserving techniques require muscle reconstruction, especially at the C2 and C7 levels.9,18 However, these techniques require additional surgical time for muscle reconstruction (more surgical time than the HMP surgical technique), and the damage to these muscles during exposure in the first place will inevitably affect the initial outcome. Meanwhile, other studies have developed unique unilateral laminoplasty techniques that preserve spinous process muscle attachment by exposure through the intermuscular plane between the semispinalis capitis and semispinalis cervicis,28 and similar techniques by resecting the spinous process rather than the attached muscles.13 These techniques were all sound and effective in protecting paraspinal muscles during the laminoplasty surgery. However, such techniques require extensive practiceand could be hard to perform until mastered. In our practice, the overall surgical time of our HMP technique was comparable to an anterior cervical decompression and fusion surgery, the similar surgical process was easy for the physicians to perform, and the low blood loss could help the patient recover more quickly from the surgical trauma, further reducing the patient’s time spent in the hospital.
Limitations
This is a retrospective study that evaluates the initial clinical outcome and safety of a new laminoplasty strategy, the HMP technique. The small sample size of the HMP laminoplasty patients may cause biases that interfere with the results. Furthermore, the follow-up interval is limited to 12 months in our present study and may not fully unveil the potential impact on the patient and cervical lordosis. Hence, a large sample size and longer follow-up are needed to fully evaluate this technique in the future.
Conclusions
Our findings have shown that the new HMP strategy in laminoplasty is both safe and effective in treating multilevel cervical myelopathy patients. This technique not only significantly lowered the surgical time and blood loss of laminoplasty surgery, but it also proved to be an effective alternative laminoplasty technique to use and may also have merits compared with traditional procedures in maintaining cervical lordosis and preventing axial pain.
Acknowledgments
We wish to thank the staff of Changzheng hospital for participating in the study.
Footnotes
* XiaoLong Shen, Chen Xu, Ruizhe Wang, and Zifan Zhang contributed equally to the work.
Funding This research was supported by grants from the National Natural Science Foundation of China (82172470, 81972090, 81772376, 82072471), Shanghai Science & Technology Commission Rising-Star Program (20QA1409200), Biopharmaceutical Science and Technology Supporting Foundation (21S31901400), Shanghai Shenkang Hospital Development Center Clinical Innovation Project (SHDC2020CR6018), Shanghai Changzheng Hospital Medical Service Innovation Project (2020CZWJFW15), and High-Quality Research Cultivating Project (2020YCGPZ-207).
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This retrospective study was approved by the ethics committee and the Institutional Review Board (IRB) of Naval Medical University (IRB number: 2021SL044). Written informed consent was obtained from all participants.
Authors’ Contributions Study conception and design: X.S., C.X., Y.L., R.W., Z.Z.; Acquisition, analysis, and/or interpretation of data: X.S., C.X., R.W., Z.Z., M.Q., Y.Z., Y.L., H.W.; Drafting/revision of the work for intellectual content and context: Y.L., C.X., X.S., W.Y.; Final approval and overall responsibility for the published work: Y.L., W.Y. All authors read and approved the final manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.