


Abstract
Background Hangman’s fractures are bilateral fractures of the C2 pars interarticularis produced during hyperextension injuries. The Levine-Edwards classification divides these fractures into 4 categories determined by injury stability. While stable fracture patterns are typically managed conservatively, prolonged traction required in unstable fractures may be superseded by surgery in its practicality. Surgical approaches can be divided into anterior and posterior: the anterior approach allows access to the disc and is used for anterior cervical discectomy and fusion (ACDF); the posterior approach includes C2 direct pedicle screw (DPS), which preserves motion segments and may be done with a minimally invasive surgery (MIS) approach. Multilevel rod and screw fusion provide the strongest biomechanical fixation. This systematic review compares indications, complications, and functional outcomes of different approaches.
Methods A search of multiple databases with keywords “hangman fracture,” “hangman’s fracture,” “axis fracture,” and “C2 fracture” was conducted; articles were included if they described the surgical technique and included at least one of the primary outcomes: functional outcomes, complication rates, operation time, and blood loss.
Results A total of 1889 abstracts were screened, 137 full text articles were analyzed, and 36 articles were included, yielding a combined total of 627 patients. ACDF was preferred in unstable fracture patterns. Pre- and postoperative visual analog scale (VAS) scores fell in all groups, with MIS DPS producing the lowest VAS scores. Approaches had excellent neurological improvement and fusion rates. Reported complication rates were generally low; self-limiting dysphagia was most common in the anterior approach and higher volumes of blood loss occured with the posterior approach (255.9 mL in open posterior approach, 75.8 mL in MIS, and 64.3 mL in ACDF).
Conclusion All surgical methods of hangman’s fracture fixation have their indications and advantages; surgeons should be equipped to perform all options. Anterior approaches may be preferred for their lower blood loss and access to the disc; however, MIS may improve outcomes in posterior approach.
Clinical Relevance This systematic review can assist spinal surgeons in the selection of the most appropriate surgical option for hangman’s fracture and allow surgeons to inform patients of the risks and benefits.
Level of Evidence 3.
- Hangman’s fracture
- cervical spine
- anterior cervical discectomy and fusion
- minimally invasive surgery
- C2 direct pedicle screw
INTRODUCTION
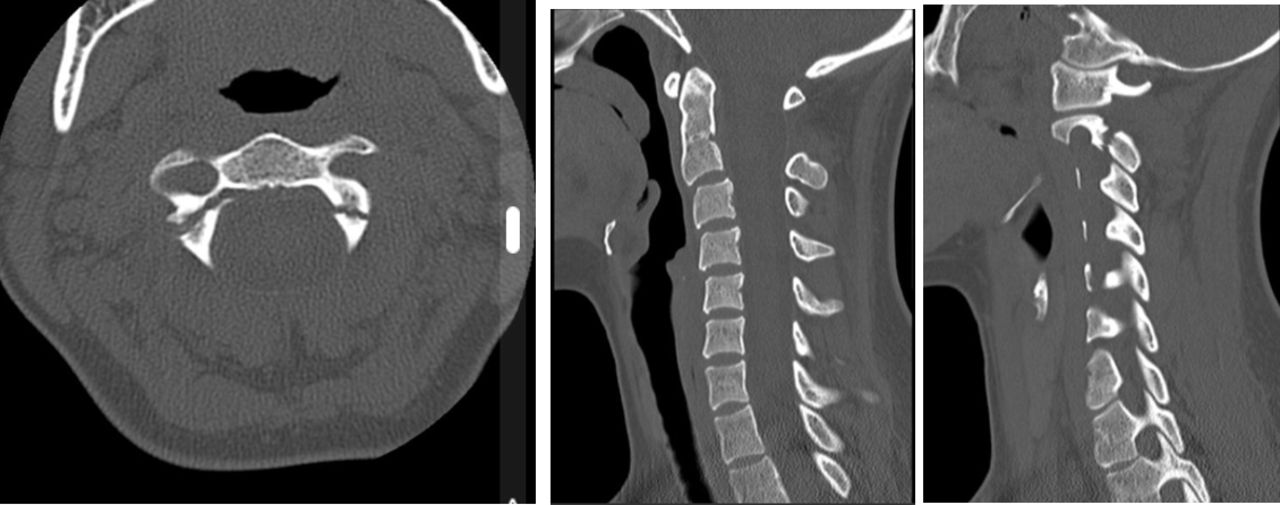
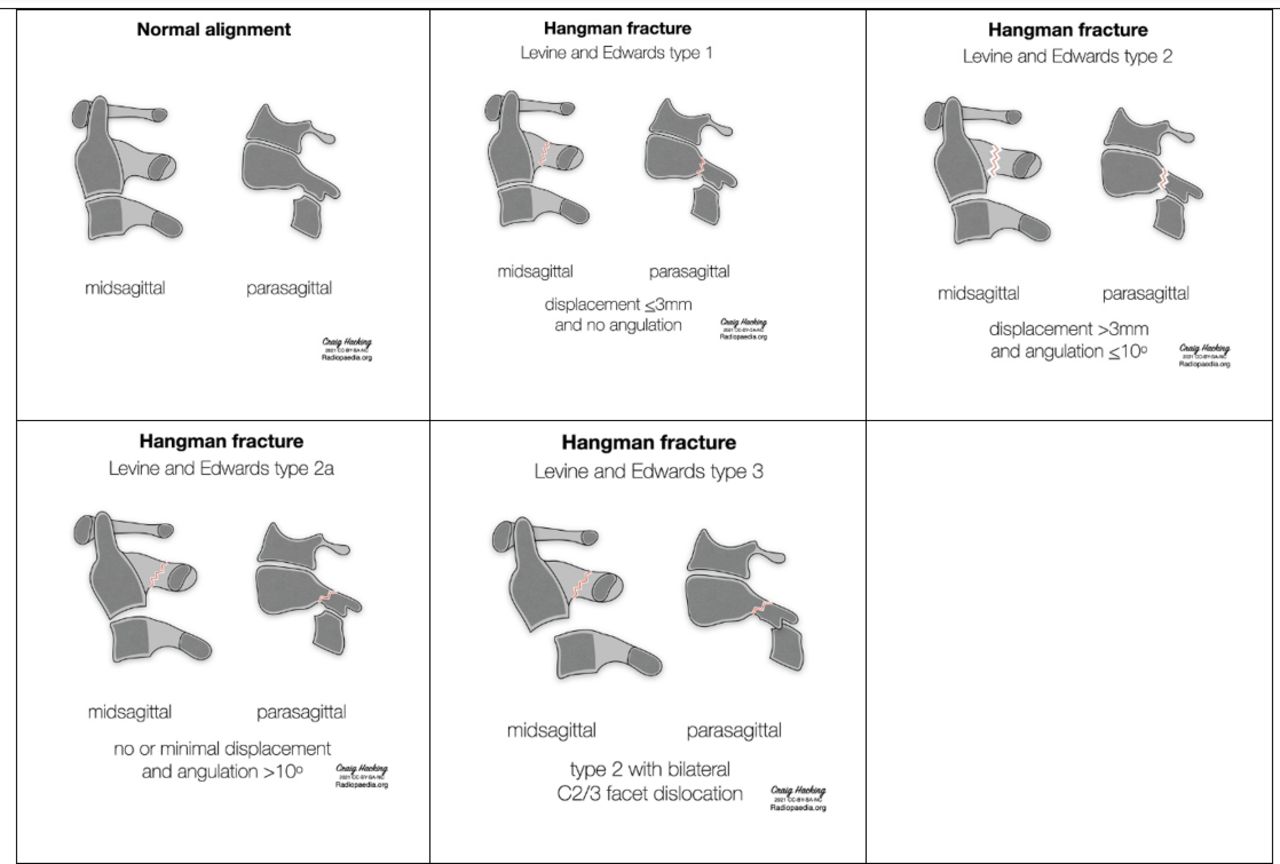
Hangman’s fractures were first described by Schneider in 1965, who observed a specific fracture pattern in road traffic accidents involving bilateral fractures of the pars interarticularis of C2,1,2 noting the similarity of the lesion to that found in victims of judicial hanging.3 These different mechanisms both cause hyperextension of the neck.1,4–6 The skull, C1, and C2 vertebrae are collectively a functional unit termed the cervicocranium and hyperextend together against C3, which is a fixed point—the bending force passing through the C2 causes a break through its weakest part: the pars interarticularis.1,5,7 Examples of hangman’s fractures are shown in Figures 1 and 2. Associated discoligamentous injury is frequent, particularly the anterior longitudinal ligament (ALL) and posterior longitudinal ligament (PLL) and intervertebral disc; these structures are crucial to the stability of the joint.4,8 Neurological injury is rare due to a fracture through both sides of the spinal canal causing the space to widen, thus decompressing the spinal cord.7,9 The most popular classification system was devised by Levine and Edwards in 198510 and is illustrated in Figure 3:
Type I: <3 mm displacement, no angulation
Type II: >3 mm displacement, significant angulation
Type IIA: the most striking modification, significant angulation without translation due to hinging of the ALL
Type III: angulated anterior fragment with facet joint dislocation
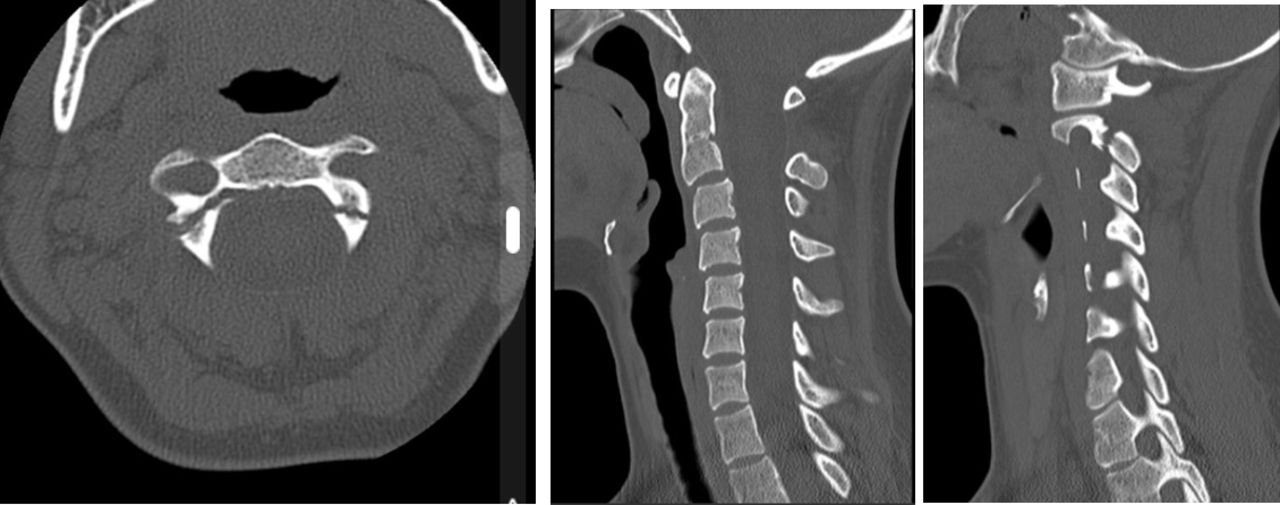
Transverse, sagittal, and parasagittal computed tomographic images of a 25-year-old woman in a road traffic accident. Note the asymmetry of pars interarticularis fractures. Source: Dixon A. Hangman fracture. Case study, Radiopaedia.org. https://doi.org/10.53347/rID-10130.

Lateral plain x-ray image of a patient with hangman’s fracture with visible anterior translation of the C2 vertebral body and fracture through the pars interarticularis. Reprinted with permission from Gaillard F. Hangman fracture. Case study, Radiopaedia.org. https://doi.org/10.53347/rID-36014.
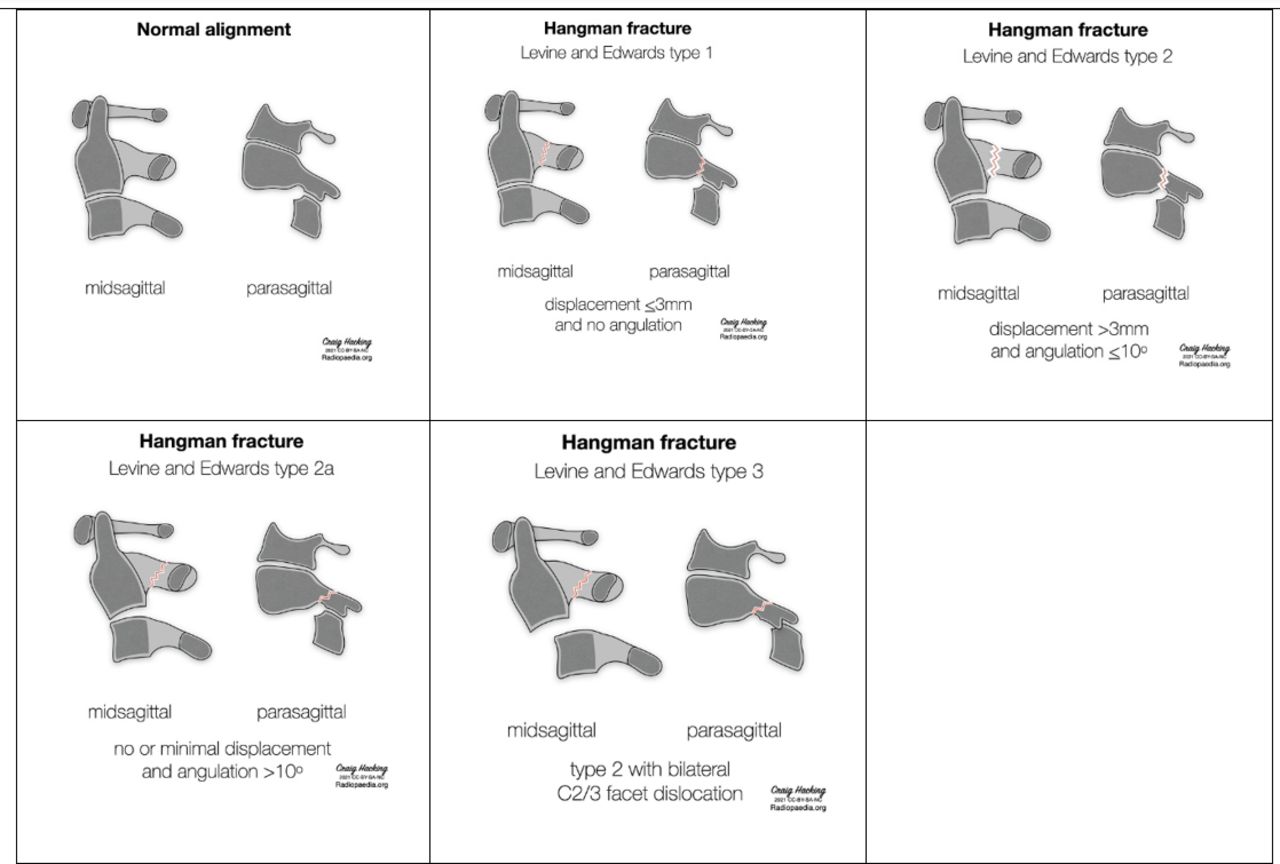
Illustration of hangman fractures by Levine and Edwards classifications. Reprinted with permission from Hacking C. Levine and Edwards classification of hangman fractures (diagrams). Case study, Radiopaedia.org. https://doi.org/10.53347/rID-88380
Most surgeons accept that stable fractures may be managed conservatively and that type I or stable type II fractures may be managed with methods ranging from a cervical collar to traction.11 Despite avoiding the traditional risks of invasive surgery, traction carries its own risks, including deep vein thrombosis, pulmonary infection, and bed sores12; halo traction involving pins has high rates of complications, including pin loosening, overpenetration, and infection.13 Furthermore, the rate of fusion falls with increasingly unstable fracture patterns managed conservatively: 60% in type II, 45% in type IIA, and 35% in type III.14 Avoiding the issues associated with prolonged traction and ensuring speedier fusion rates have spurred the popularity of managing unstable hangman’s fractures surgically.12,15
Currently, no clear algorithm exists in guiding the selection of surgical management of hangman’s fracture, and selection of treatment options remains controversial.15–17 Surgical approaches can be broadly divided into anterior and posterior—anterior approaches expose the disc and allow anterior cervical discectomy and fusion (ACDF); posterior approaches include direct pedicle screw (DPS), occipitocervical fusion, or multilevel posterior fusion.11,15,18 Posterior approaches allow direct fixation of the pars and may be supplemented by more recent technological advances, including navigation and minimally invasive surgery (MIS) techniques.15,19,20 Certain fracture patterns may necessitate a combined anterior-posterior approach.21
The present systematic review analyzes the literature investigating outcomes of different surgical approaches and techniques in the management of hangman’s fractures. Issues on safety and precision in spinal surgery have evolved over years, and a modern perspective on hangman’s fracture is required to guide its future use. Previous systematic reviews conducted on hangman’s fracture management have largely focused on delineating between the indications for conservative and surgical management22,23 and do not include several studies that have been recently published. The present review will focus on different surgical approaches and their indications, complications, and outcomes to illustrate current trends and understand the management of this injury and assist in decision-making.
METHODS
This systematic review on hangman’s fracture surgical management was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 checklist and was registered on PROSPERO, the international prospective register of systematic reviews.
A comprehensive search was carried out using the PubMed, Embase, and Cochrane Library databases; additional articles were identified through Google Scholar and reference snowballing from high-quality reviews and previous systematic reviews.
The search was performed on 08 March 2022. Search terms were “hangman fracture,” “hangman’s fracture,” “axis fracture,” and “C2 fracture.” Search terms were deliberately kept short and broad to ensure that all articles that may be relevant would be found. The search results were stored in the Mendeley Reference Application, where the articles could be analyzed and sorted.
The primary outcomes were to break down surgical approaches by fracture classification, functional outcomes, complication rates, operation time, and blood loss. Secondary outcomes were fusion rates and neurological deficits.
Inclusion criteria for the review were as follows:
Randomized, prospective, or retrospective clinical trials on living, human adults
Articles published since 2000—it was around this time that advances in segmental posterior cervical instrumentation became widely accepted22
Study on hangman’s fracture; however, patients with concomitant spinal injuries were included
Any surgical approach with a clear description of the surgical technique
Measurement of at least 1 primary outcome
Exclusion criteria were as follows:
Case reports, systematic reviews, meta-analyses, and cadaveric studies
Pediatric studies
Articles lacking a clear description of operation technique and not commenting on primary outcomes; articles only commenting on secondary outcomes, such as fusion
Two authors were responsible for screening abstracts and subsequent data extraction; discrepancies were reviewed, and if not resolved, they were referred to a third author.
Functional outcomes were expressed differently by different authors—the most popular scoring system to objectively measure functional outcomes was the visual analog scale (VAS) and was the preferred measure for analysis. However, authors frequently made general comments stating the overall findings—these were noted.
Bias was assessed by the risk of bias in nonrandomized studies of interventions tool. Of particular concern was selection bias or bias in the measurement of outcomes24; articles deemed to have a high risk of bias were omitted.
Studies were subdivided according to the surgical approach being described, and data from the trials were synthesized to provide a systematic review on the incidence and rates on various outcomes. Due to the high levels of heterogeneity between trials and the scarcity of trials comparing 2 or more types of surgeries, it was deemed that a meta-analysis would be inappropriate.
RESULTS
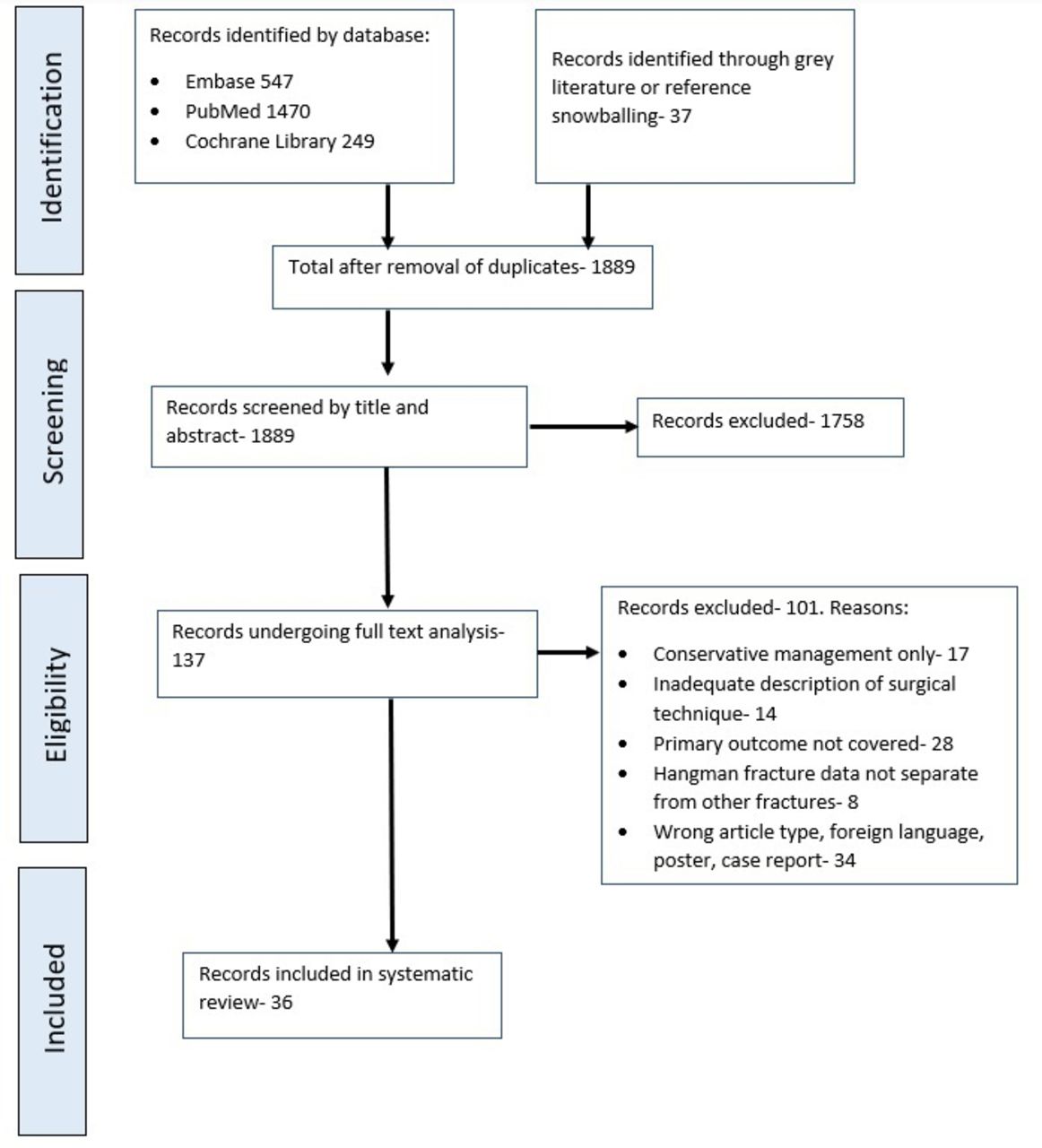
A total of 1889 records were screened, 137 underwent full-text analysis, and 36 were included for review. The final 36 articles included 627 patients. Figure 4 is a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart summarizing the selection process. Table 1 summarizes the articles included in the systematic review.

A preferred reporting items for systematic reviews and meta-analyses flowchart.
Summary of studies included.
Pre- and Intraoperative Techniques
Articles were included if the surgical approach and technique were described; however, the level of detail in describing preoperative and surgical management varied.
Articles that described preoperative management all described placing the patient in traction; the weight and duration varied among authors and among patients within the same study, ranging from 1.5 to 8 kg and lasting from 2 to 9 days. Many authors obtained radiographs in the preoperative period to monitor reduction, and many adjusted the weight and angle of traction accordingly. All patients had either complete or partial reduction of the fracture site preoperatively.
Most authors described continuing traction intraoperatively, most commonly with a Mayfield clamp. Techniques to reduce any outstanding displacement intraoperatively included adjusting the angle of the Mayfield clamp under fluoroscopic guidance19,37,41,47; reducing the fracture by extending the neck and pushing the body of C233,46,48; and using Caspar distractors.46,50,51 In the posterior approach, when threading pedicle screws across a fracture site, the screws compressed the fracture.37,47
Jain et al, in describing the anterior approach, commented on whether screw purchase was unicortical or bicortical using unicortical locking screws49; other authors describing both anterior and posterior approaches emphasized that great care was taken not to penetrate the far cortex when inserting screws. Authors used a variety of anterior cervical plates—of those specified, the most common was the Zephir plate; all were variable angle plates.
Where a combined approach was used, authors began with the anterior approach to perform ACDF before turning the patient prone and fusing C2-C3 with screws and rods. One author described that where adequate reduction could not be achieved with cervical distractors during the anterior approach following discectomy, the anterior wound would be temporarily closed, the posterior fusion would be performed, and then the patient would be placed supine again, have their wounds reopened, and the ACDF would be completed.51
Surgical Treatment by Levine-Edwards Classification
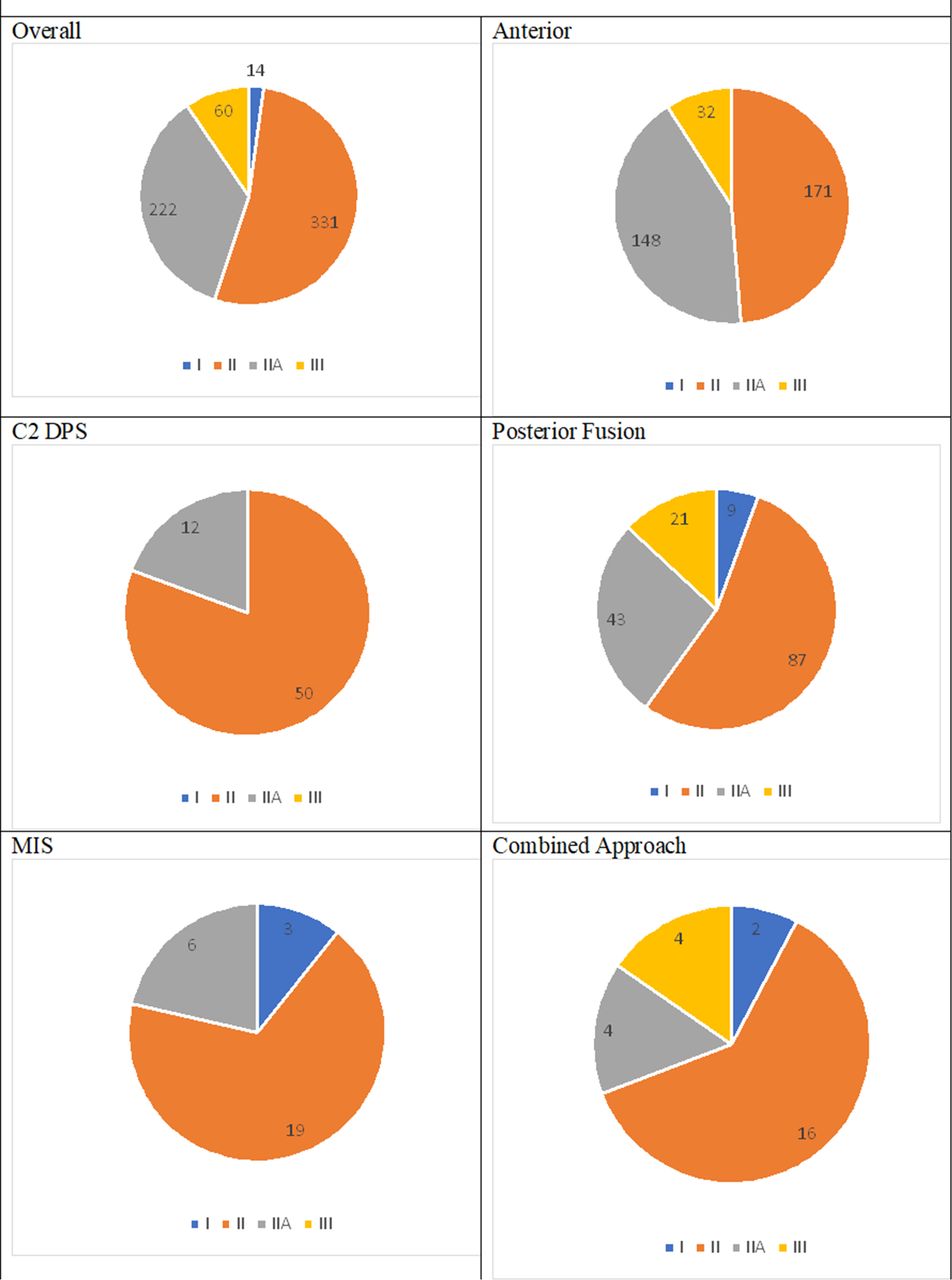
Figure 5 displays the surgical options employed and their use in different fracture types as per the Levine-Edwards Classification. The posterior approach was used 33% of the time in type IIA or III fractures, whereas the anterior approach was used 51% of the time for type IIA or III fractures. The anterior approach was preferred in unstable fractures.
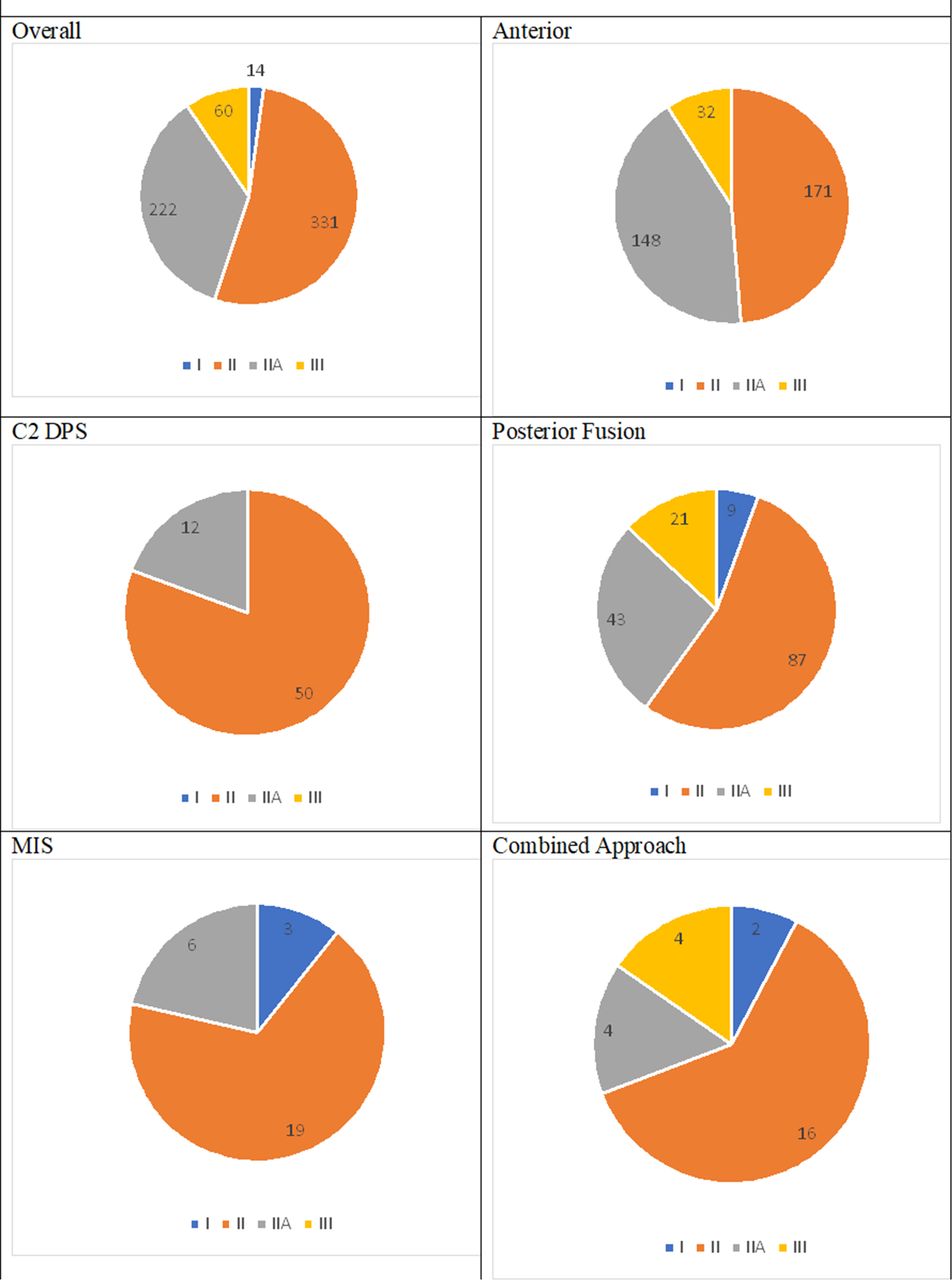
Surgical approach by fracture classification. MIS, minimally invasive surgery; DPS, direct pedicle screw.

Lateral x-ray image of patient from Figure 2 who has had an anterior cervical discectomy and fusion procedure. Reprinted with permission from Dixon A. Hangman fracture. Case study, Radiopaedia.org. https://doi.org/10.53347/rID-10130 https://doi.org/10.53347/rID-10130
Functional Outcomes
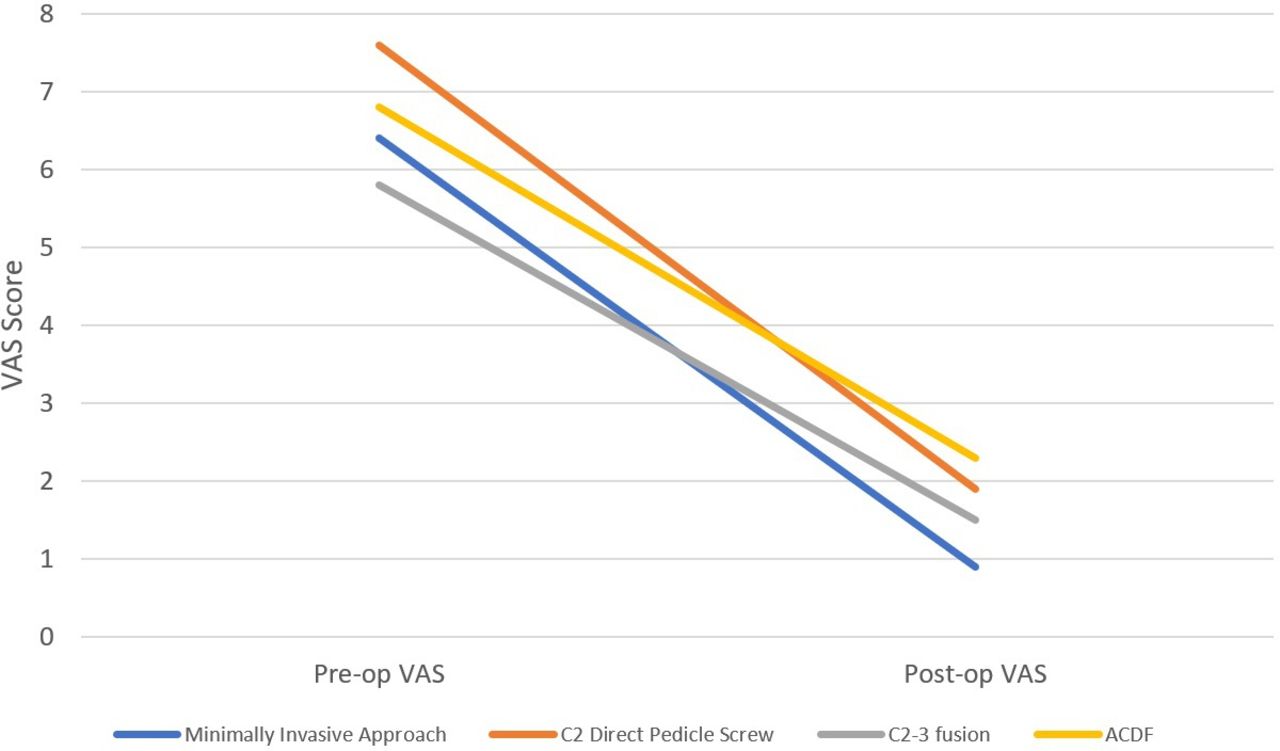
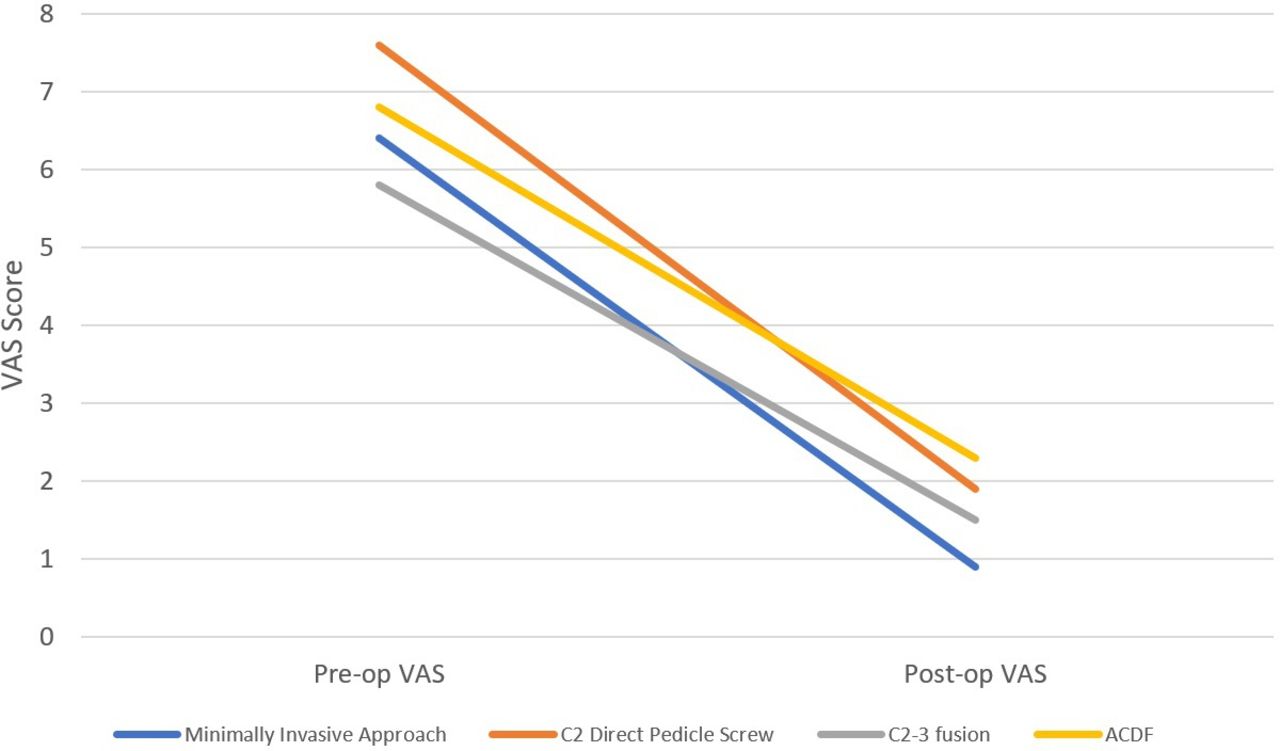
Pre- and postoperative visual analog scale (VAS) scores by surgical techniques displayed as line graph. ACDF, anterior cervical discectomy and fusion; pre-op, preoperative; post-op, postoperative.
Functional outcomes were reported in a variety of ways by different authors—the most popular tool used was the VAS score, which is a simple numerical scale asking the patient to rate their pain from 0 to 10. Other scores used include Odom’s criteria and the Japanese Orthopaedic Association score. Authors measuring pre- and postoperative VAS scores were included and mean scores are summarised in Table 2 and Figure 6. Preoperative VAS score averages ranged from 5.8 to 7.6—the C2 DPS approach caused the steepest fall in VAS score of 5.7, and MIS had the lowest postoperative VAS at 0.9. Both these methods attempt to cause minimal disturbance to surrounding structures, with MIS avoiding excess soft tissue dissection and the C2 DPS method avoiding instrumenting other vertebrae. ACDF had the highest postoperative VAS, while C2-C3 fusion showed the smallest improvement of 4.3.
Pre- and postoperative VAS scores by surgical techniques.
Other authors expressed the functional results through text, and generally across all surgical techniques, the results were positive. Chowdhury and Haque found that all 6 patients who had C1-C3 lateral mass fusion were leading a normal life with no symptoms by final follow-up11; Singh et al reported that all 10 patients treated with C2-C3 fusion had preserved neck rotation15; Li et al reported that all 38 patients treated with ACDF had normal neck movement at final follow-up50; and Man Kyu et al reported that all 7 patients who had MIS DPS fixation had a full range of motion in the neck within 6 months.41
Complication Rates
The complication profile of the different approaches was very different—the anterior approach, in particular, produced dysphagia and voice alterations. However, of the 16 cases of dysphagia, only 1 was permanent, and the rest resolved spontaneously within 3 months (Table 3). Jain et al reported that in 44 patients who underwent ACDF, all had dysphagia that resolved spontaneously within 2 to 3 days.49 This finding implies that this complication may be far more common than reported as different authors may use different thresholds of duration of dysphagia before reporting it as a complication.
Complications reported by surgical approach.
The complication profile of the posterior approach appears to be influenced by the greater soft tissue damage required whilst dissecting muscle from bone, leading to 3 instances of metalwork-related infection and increased intraoperative bleeding. There were no reported complications in 21 patients undergoing the MIS posterior approach.
No authors reported instrumentation-related injuries to the spinal cord; 1 author reported severe intraoperative bleeding during pedicle drilling suspected to be due to vertebral artery injury, but there were no neurological deficits postoperatively.33 No author reported early loss of fixation with any technique.
Operation Time
Given that a combined approach involves both anterior and posterior approaches, it was expected that the operation time for a combined approach would be longer than other procedures. Of note, multilevel vertebral fixation via the posterior approach was the slowest of the remaining operation types (Table 4).
Mean operating time by operation type.
Blood Loss
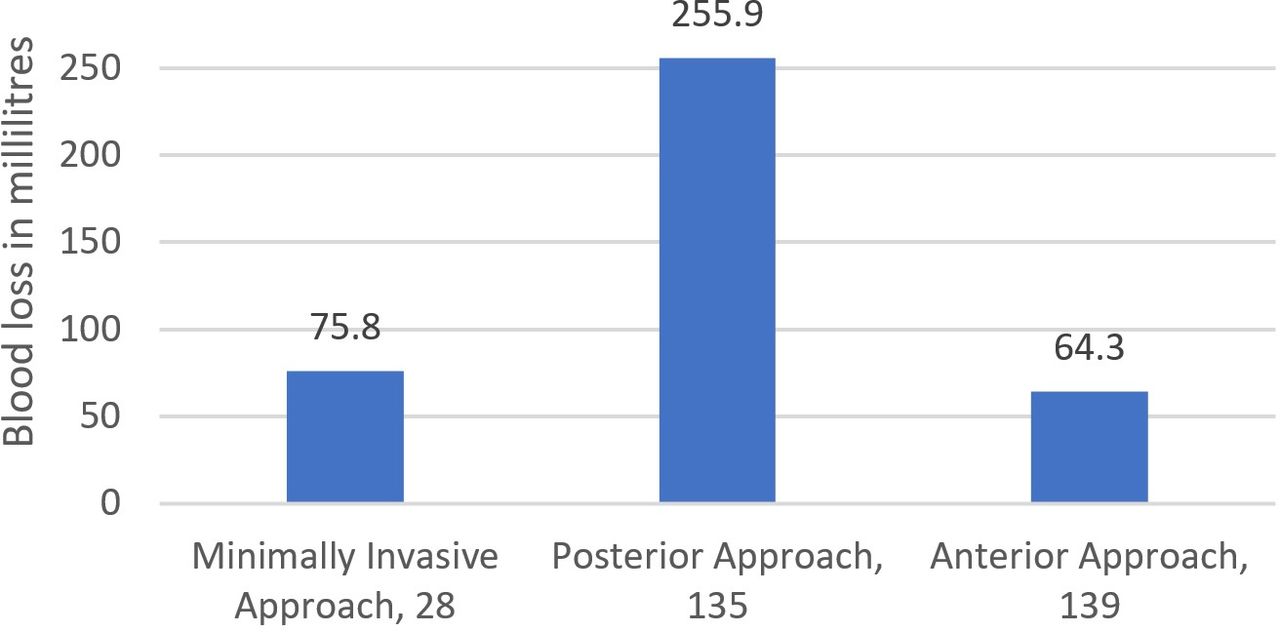
Blood loss varied by surgical approach. C2 DPS and multilevel fusions were combined to show posterior approaches together. The posterior approach caused the most blood loss and the MIS approach resulted in much less blood loss, but the anterior approach produced the smallest amount of blood loss (Figure 7).

Blood loss in milliliters by surgical approach, number of patients.
Fusion and Neurology
Reported fusion rates were excellent throughout all techniques. Hur reported 1 case of nonunion among 17 patients treated with ACDF44; there was otherwise a 100% fusion rate.
There were 487 patients in these articles who described symptoms of neurological deficits; 131 of these patients had neurological deficits. Only 7 of these patients failed to improve: 3 were due to confounding factors, such as mortality and concomitant head injuries; 2 were from Hur’s ACDF article; and 2 were from Liu’s 25 patients who underwent DPS.42,44
DISCUSSION
The inherent issues with conservative management have made surgery an increasingly viable treatment option for hangman’s fracture. Nonoperative methods, including traction, have been associated with axial pain, anterior dislocation, angulation, and nonunion. Associated bed sores, pulmonary infections, and delirium are common, particularly in the elderly. Accurate reduction cannot be achieved through traction alone if there is displacement; after removal of traction, the patient will have to wear a halo vest for 3 to 6 months, which can cause great discomfort. Thus, the potential for surgery to avoid these problems has caused a general shift in literature to use surgery as a primary treatment option rather than deal with conservative treatment that has failed.12,17,44,49,52 Various radically different surgical techniques may be employed via the anterior, posterior, or combined approach, and their indications, complications, and outcomes must be better understood to guide surgeons as surgical fixation becomes more commonly used in managing unstable hangman’s fractures over conservative management.
It remains widely accepted that type I fractures may be managed conservatively—only 14 patients of the 627 included in this review who were given a Levine-Edwards classification were type I, as they had excellent union rates nonoperatively.23 In 2000, Samaha et al noted that most authors reserved surgery for patients in whom conservative management failed, yet they recognized the need for early surgery in unstable fractures and suggested displacement of 3 mm and kyphosis >15° or lordosis >5°.53
ACDF has been used to treat hangman’s fractures since at least 1968.54 Several approaches have been described, including a transoral approach, which provides excellent exposure of the vertebral bodies and disc; however, it is associated with high infection rates.55 This technique appears to enjoy little popularity, with none of the articles included in this study employing it. Authors describing the approach in this systematic review referred to a transverse skin incision at the midpoint between the angle of the jaw and thyroid cartilage17,32,44,45,56,57; others included in this review18,31 and in the wider literature58 described a “high retropharyngeal,” “submandibular,” or “high anterior cervical” approach, which may involve an incision closer to the mandible; others described a more longitudinal skin incision from the angle of the jaw to the hyoid bone.46,48,49 After skin and platysma incision, all authors used the fascial planes of the neck to retract the sternocleidomastoid and carotid sheath laterally and enter the retropharyngeal space to expose the prevertebral fascia.58 Structures at risk via this approach include the carotid sheath, recurrent laryngeal nerve, esophagus, trachea, hypoglossal, and facial nerves; however, the majority of the approach relies on opening fascial places and minimizing the soft tissue and muscle damage.44 Where a submandibular approach is employed, some authors have advocated excising the submandibular nerve rather than retracting it, which avoids injury to the marginal mandibular nerve.59
This approach retracts the esophagus and surrounding neurovascular structures, and dysphagia and voice alterations were the main reported complications here. Precise incidence is difficult to estimate, as while Jain et al reported a degree of dysphagia and donor site pain, many authors reported neither.49 This is largely self-limiting, with only 1 case of permanent dysphagia.
Once exposed, patients undergo C2-C3 disc excision, which is replaced either with a bone graft, commonly from the ilium, or a synthetic bone substitute50; Heneghan and McCabe noted in a questionnaire from 52 patients who had undergone iliac crest grafting that 90% experienced pain and 7% had infection; they advised the use of more recently developed synthetic materials.60 Following discectomy and reduction, the fracture may be fixed with either a cage with or without a short plate and screws construct. The construct created by ACDF with plate and screws is shown in Figure 8. Wei et al compared 21 patients who underwent ACDF with a polyetheretherketone cage with 28 patients who underwent ACDF with iliac crest graft and plating; they found blood loss and operative time were significantly less in the cage group, and all achieved solid fusion. Furthermore, the graft required can be taken through a smaller donor site, and thus donor site morbidity is reduced.46
While the anterior approach provides excellent access to the intervertebral disc, it does not allow direct access to the facet joints; this may be required in type III injuries involving facet joint dislocations. Techniques to reduce facet joints include closed preoperative traction, which many authors in this systematic review found to be sufficient. Open anterior techniques included using distractor pins with or without a posterior force; using a Cobb elevator in the intervertebral space following discectomy to move the dislocated facet away; and using vertebral spreaders to open the intervertebral space and then angle the spreaders rostrally.61,62 Facet joint dislocations may be described as subluxed, perched, or locked; particularly in locked facet joints, reduction may be difficult and require a combined approach.63 Hur et al described 2 type III injuries treated with ACDF, 1 being subluxed and 1 locked; the patient with the locked facet joint was the only patient in the systematic review who had nonunion and later required a posterior fusion44; no other authors described the type of facet joint dislocation. Kong et al performed ACDF on 46 patients, including 7 with type III injuries. Three had poor reduction, with anterior displacement of the C2 vertebral body and local kyphosis at C2-C3 and postoperative mild occipital and neck pain. All 3 cases were in type III fractures, and they suggested this was due to the difficulty of reduction due to locked facets, ultimately concluding that while a combined anterior-posterior approach may be required to achieve better reduction, a single anterior approach produced acceptable clinical results.12
While ACDF had the worst postoperative VAS scores in the present review, it is difficult to tell whether the findings are significant, as this review also noted that ACDF is particularly used in type IIA fractures, characterized by severe angulation of the anterior fragment with PLL injury. These are along with type III fractures that are particularly unstable, which may cause worse functional outcomes. The anterior approach is useful in this regard to provide access to the disc, ALL, and PLL. In cases of disc instability, instrumenting the vertebrae from a posterior approach may cause anterior displacement of the anterior fragment, thus the anterior approach may avoid iatrogenic injury.39
A clear advantage of the anterior approach is the greatly reduced blood loss—the results of this review show that on average, the open posterior approach produced 4 times the blood loss of the anterior approach, although with MIS, these are almost equalized. Patel et al compared 12 ACDF and 9 posterior fusions and found that the blood loss in the anterior group was half, which was statistically significant.18 Patel et al were clear that the anterior approach was safer, simpler, and faster and was associated with less blood loss and soft tissue damage. Comparing 24 ACDF and 14 posterior fusions, Ge found that ACDF produced significantly less intraoperative bleeding, less postoperative drainage, and shorter operation time.45
The posterior approach encompasses a range of methods. Traditional open approaches are made via a vertical midline incision and exposure of the posterior surface of the vertebrae to allow insertion of screws across the fracture site. To expose the posterior aspect of the vertebrae, the deep cervical muscles must be retracted—care should be taken to avoid damaging the facet joint capsule, and a subperiosteal dissection is advised to minimize bleeding. Nevertheless, greater bleeding due to muscle and posterior venous plexus damage and use of a drain is more common than the anterior approach18,45; however, others prefer this to avoid the major neurovascular structures encountered anteriorly.11
There are several types and combinations of fixations that can be provided from the posterior approach, including DPS, C2-C3 fusion with a rod and screws construct, or fusions involving C1 or even C4. Pars or pedicle screws may be used, which have different entry points and trajectories; however, both require accuracy to avoid damage to the vertebral artery and nerve roots.
C2 DPSs are a controversial method—they provide a physiological fixation by preserving movement at the C1-C2 and C2-C3 motion segments; however, they do not address discoligamentous instability. In a comparison of 4 patients with DPSs of C2-C3 fusion, Dalbayrak et al concluded that DPSs are a feasible method, but only in the absence of discoligamentous injury.25 ElMiligui et al reported that this technique provided an excellent functional outcome in 12 type II and 3 type IIA patients; although they reported 1 case of heavy bleeding during drilling, there was no neurological deficit or postoperative issues, they determined this to be an overall effective method.33 Hakalo and Wroński concluded they are safe, cheap, and feasible.64 Prost et al, however, dismissed this method as having no indication, only being indicated in minimally displaced, stable fractures, which could otherwise be managed conservatively.16 This conclusion is reflected in the present review, with it being used far less than multilevel posterior fusion or ACDF and almost exclusively in type II fractures. Other authors have expressed concerns regarding the narrow, angulated pathway of the screw through the vertebrae, which is lined by the vertebral artery and spinal cord—a rate of 11% to 66% neurovascular complications has previously been reported, although this is based on its earlier application and results in the 21st century appear to show far improved safety.29,45,65
This technique has the potential to be augmented with MIS and navigation techniques. Although only 13 patients in this review included complications or functional outcomes of patients undergoing MIS, they reported no complications, the best postoperative VAS, and far lower blood loss than open fusion. The protection of soft tissues afforded by MIS and improved screw accuracy in the cervical spine under navigation provides an impetus to expand these operations.15,20,66
Most operations performed by the posterior approach involved multilevel fixation, mainly C2-C3. The multilevel posterior fusion is the strongest biomechanical fixation14,19; it is more resilient than DPS yet may not prevent collapse of the C2-C3 space in the presence of disc damage.67 C2 pedicle or pars screws are usually used alongside C3 lateral mass screws, which are safer to instrument. C1-C3, C1 and C3 fusion, and occipitocervical fusion have also been described. For example, Chowdhury and Haque described 6 patients with unstable hangman’s fractures treated with C1 and C3 lateral mass screws, which provided good stability, good outcomes, and reduced intraoperative risk of vertebral artery injury; however, they conceded that due to the elimination of C1-C2 rotation, this was a last case resort.11 Posterior C2-C3 fusion is the only appropriate method for fixing atypical hangman’s fractures. ACDF cannot directly fix the posterior arch to the vertebral body, potentially leaving large fracture gaps26 and DPSs require an intact PLL complex, which is usually damaged in atypical fractures.68
Limitations
Although this systematic has several strengths, it is not without limitations. The following are its key limitations:
Most studies were retrospective; therefore, reliability may be questioned as it relies on previous documentation; as such, frequency of observed outcomes may differ between different authors.
Few studies compared 2 or more methods of fixation to allow direct comparison between outcomes.
Few studies displayed results by patient; therefore, it was difficult to break down results by category, such as complication rates by age or by Levine-Edwards classification.
These factors meant a meta-analysis was deemed likely to be unreliable; however, the synthesis of data to provide comparisons did powerfully display differences.
CONCLUSION
Hangman’s fracture results from a hyperextension injury of the neck, most typically seen in road traffic accidents. Levine-Edwards produced the most used classification; progressive grading represents increased instability due to damage to the C2-C3 discoligamentous complex; modern advances in surgery mean patients can be given rapid, stable fixation and avoid prolonged pin traction. Surgical approach may be anterior, posterior, or a combination.
Discectomy may be performed through the anterior approach if there is disc herniation or PLL injury—this approach is associated with reduced blood loss and soft tissue injury; however, it may cause dysphagia, but this usually resolves. We found that ACDF had the worst postoperative VAS; however, this approach was used most in the unstable IIA fracture, so the significance of the VAS is uncertain.
Direct C2 pedicle screw fixation preserves all motion segments, but it does not provide sufficient support in discoligamentous injury. It is used predominantly in type II fractures deemed to be sufficiently stable. The use of MIS significantly reduces blood loss, limits soft tissue damage, and is associated with the best postoperative VAS.
Posterior fusion provides the strongest biomechanical fixation and is best in atypical fractures. It produced the smallest decrease in VAS, and the muscle dissection needed for exposure causes greater soft tissue damage and blood loss.
Oveall, all surgical approaches are broadly safe and provide excellent fusion and improvements in neurology, with literature supporting their use; surgeons must be familiar with all techniques to select the best in given circumstances.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- Received September 13, 2022.
- Revision received November 19, 2022.
- Accepted January 21, 2023.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.