


Abstract
Background Posterior cervical foraminotomy (PCF) and anterior cervical discectomy and fusion (ACDF) are 2 commonly used surgical approaches to address cervical radiculopathy. Demonstrating superiority in clinical outcomes and durability of one of the approaches could change clinical practice on a large scale. This is the largest reported single-institutional retrospective cohort of single-level PCFs compared with single-level ACDFs for cervical radiculopathy.
Methods Patients undergoing either ACDF or PCF between 2014 and 2021 were identified using Current Procedural Terminology codes. Medical records were reviewed for demographics, surgical characteristics, and reoperations. Statistical analysis included t tests for continuous characteristics and c2 testing for categorical characteristics.
Results In total, 236 single-level ACDFs and 138 single-level PCFs were included. There was no significant difference in age (51.0 vs 51.3 years), body mass index (BMI; 28.6 vs 28.1), or Charlson Comorbidity Index (1.89 vs 1.68) between patients who underwent ACDF and those who underwent PCF. There was no difference in the rate of reoperation (5.1% vs 5.1%), time to reoperation (247 vs 319 days), or reoperation for recurrent symptoms (1.7% vs 2.9%) for ACDF vs PCF. Hospital length of stay (LOS) was longer for ACDF compared with PCF (1.65 vs 1.35 days, P = 0.041), and the overall readmission rate after ACDF was 20.8% vs 10.9% after PCF (P = 0.014).
Conclusions Overall reoperation rates or reoperation for recurrent symptoms between ACDF and PCF were not significantly different, demonstrating that either procedure effectively addresses the indication for surgery. There was a significantly longer LOS after ACDF than PCF, and readmission rates at 90 days and 1 year were higher after ACDF.
Level of Evidence 3.
- posterior cervical foraminotomy
- anterior cervical discectomy and fusion
- radiculopathy
- readmission
- reoperation
Introduction
Posterior cervical foraminotomy (PCF) and anterior cervical discectomy and fusion (ACDF) are 2 approaches commonly used to address cervical radiculopathy that has been refractory to conservative treatment. Posterior decompression of the affected nerve roots has the benefit of preserving cervical mobility while avoiding the subsequent possibility of adjacent segment disease (ASD), pseudarthrosis, and hardware failure associated with ACDF.1 While ACDF carries a higher risk of dysphagia and other complications relating to the anterior structures of the neck, PCF requires dissection of the posterior cervical musculature, which is associated with greater postoperative pain.2–4 Due to difficulties in accessing the disc space posteriorly and the lack of stabilization, recurrence of symptoms and need for additional surgery are considered greater risks with a posterior approach, according to some studies.5
While both approaches have their inherent risks, ACDF has increased nationally by 184% and continues to rise, compared with the 5.6% increase in PCF procedures, making up 80% of interventions for cervical disc herniations.6 In fact, in large database studies, ACDF frequency exceeds PCF by nearly a factor of 10 in the United States.7 Furthermore, ACDFs have been recognized as having as much as a 89% higher cost than PCF,7–9 particularly with indirect costs.10 These data, however, do not take into account reoperations and readmissions associated with both procedures.
Demonstrating superiority in clinical outcomes, health care costs and long-term durability of one of the approaches could potentially change clinical practice on a large scale for spine surgeons. While there are clinical and radiographic reasons that a surgeon may select ACDF vs PCF, given clinical equipoise, it has not yet been determined which, if either, is clinically superior or more cost-effective. The present study is the largest retrospective study to date comparing outcomes, reoperation rates, and readmission rates of single-level ACDF vs PCF.
Methods
Sample
A retrospective study of patients at a tertiary care institution who underwent single-level open PCF or open ACDF between C3 and C7 from 2014 to 2021 for radiculopathy was conducted. After obtaining institutional review board approval from the University of Pennsylvania, electronic medical records were reviewed to identify qualifying patients. Data from 5 spine surgeons with at least 10 years of experience were included. Patients were excluded from the study if they were less than 18 years old, if the indication for surgery was myelopathy or myeloradiculopathy, and if the etiology was for anything other than degenerative disease. Reoperations were recorded at 30-day, 90-day, 1-year, and 2-year intervals. Readmissions were recorded at 30-day, 90-day, and 1-year intervals.
Patient data collected from the medical record included gender, age, race, mean BMI, American Society of Anesthesiologists (ASA) score, and smoking status. Other preoperative comorbidities were extracted, including chronic kidney disease (CKD), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), peripheral vascular disease (PVD), diabetes mellitus (DM), prior cerebrovascular accident (CVA), cognitive decline, rheumatologic disorders, human immunodeficiency virus, and prior myocardial infarction. Charlson Comorbidity Indices (CCIs) were calculated. Intraoperative data, including the number and levels fused and operative time, were included.
Statistics
Patients undergoing either ACDF or PCF between 2014 and 2021 were identified using Current Procedural Terminology codes. Medical records were reviewed for baseline patient characteristics, including age, gender, ethnicity, BMI, smoking status, and medical comorbidities; surgical characteristics, including operative level and procedure length; and perioperative outcomes, including length of stay (LOS), reoperation rates and indications, and readmission rates. Baseline demographic variables were compared between groups using t tests for continuous characteristics and c2 testing for categorical characteristics. Univariable analyses were performed using t tests for continuous variables (LOS and operative time), while χ2 analyses were performed for categorical outcomes (reoperation and readmissions). To further investigate the relationships between possible confounding variables and perioperative outcomes, linear regression models were performed, including demographic data and surgical details (type of procedure and spinal levels), with LOS as the dependent variable, and logistic regressions were performed with either readmission or reoperation as the dependent variable. All statistical analyses were performed on SPSS (IBM, Armonk, NY).
Results
Patient Characteristics
A total of 374 total patients were included in the study. Of those patients, 138 (36.9%) were single-level PCFs and 236 (63.1%) were ACDFs. With respect to preoperative characteristics, the only statistically significant difference between groups was ASA class, with a mean of 2.22 vs 2.11 in the ACDF vs PCF group (P = 0.031), respectively. Given this significant difference, stratified analyses were performed for the primary outcomes of reoperation, readmission, and LOS to assess and control for possible confounding and effect modification. There were no differences between ACDF and PCF groups with respect to smoking history at the time of surgery. Within the ACDF cohort, 48.5% were never smokers, 33.6% were former smokers, and 17.9% were current smokers compared with 54.9%, 29.3%, and 15.8%, respectively, within the PCF cohort (P = 0.501). BMI (28.6 vs 28.1), CCI (1.89 vs 1.5), and age (51.01 vs 51.30) were not statistically different between ACDF and PCF (Table 1). With respect to specific comorbidities, 9% of the cohort had DM, 2% had CKD, 2.5% had CHF, 16.6% had COPD, 5% had PVD, and 4.8% had a prior CVA. There was no statistically significant difference between the ACDF and PCF groups in rates of preoperative comorbidities (Figure 1).
Perioperative patient characteristics.
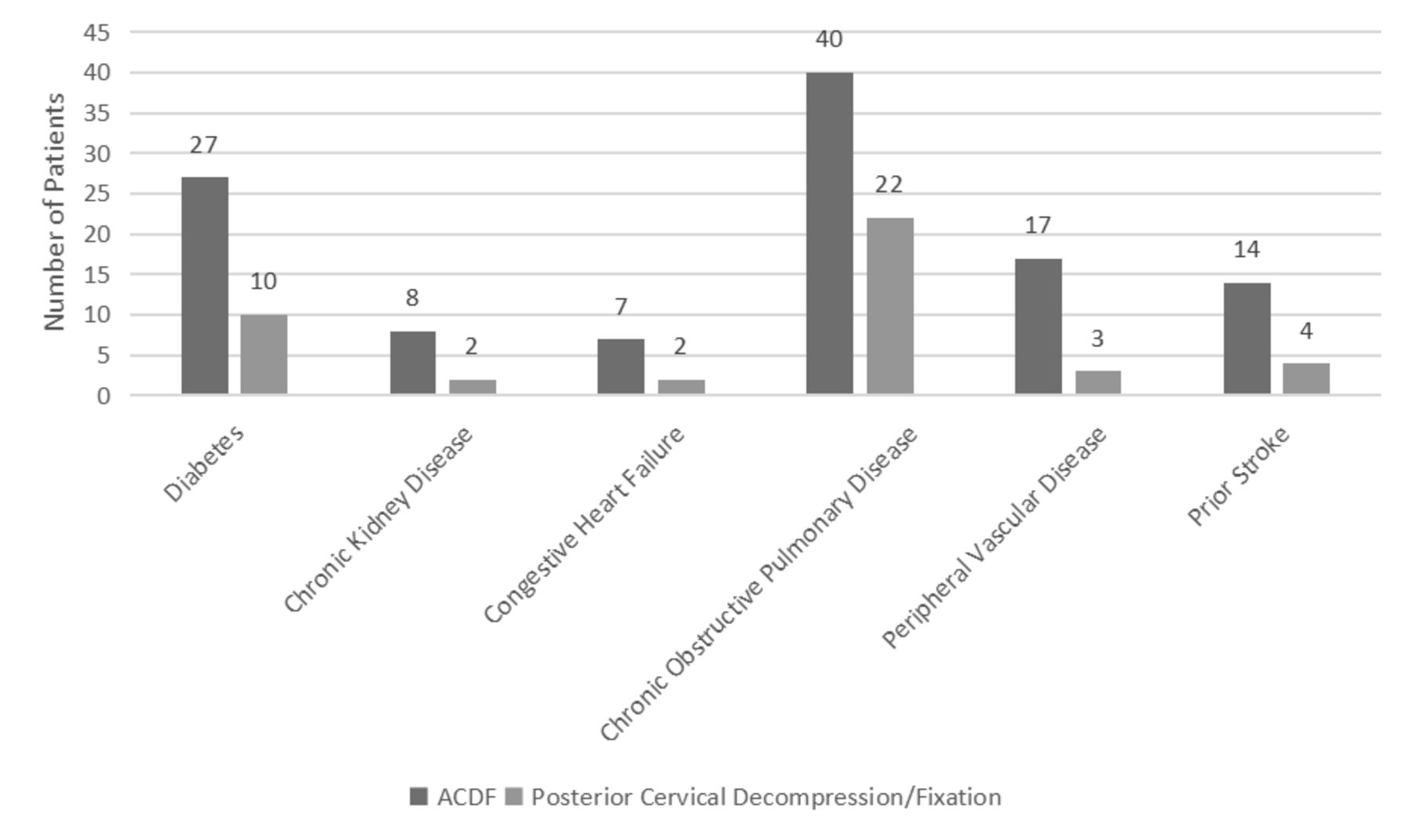
Comorbidities by surgery type. There was no significant difference between groups in preoperative comorbidities. The most commonly observed comorbidities were chronic obstructive pulmonary disease and diabetes mellitus in both groups. ACDF, anterior cervical discectomy and fusion.
Surgical Details
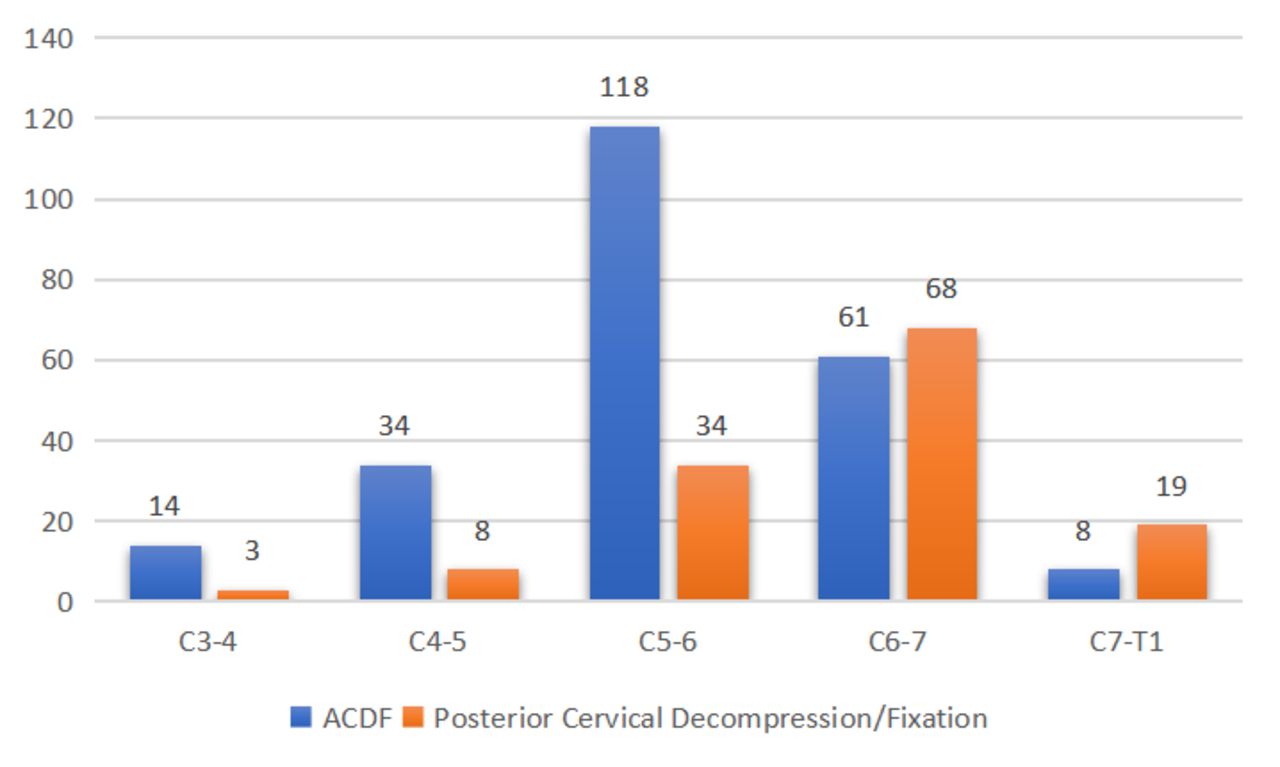
Procedure time was not significantly different between ACDFs and PCFs (124.78 vs 124.79 minutes). On χ2 analysis, there was a significant difference between the levels treated in the ACDF vs PCF groups (P < 0.001). Within the ACDF group, patients most often underwent surgery at the C5-C6 level (n = 118, 50.2%) followed by C6-C7 (n = 61, 26.0%) in contrast to the PCF group, which more frequently underwent decompression at C6-C7 (n = 68, 51.5%) followed by C5-C6 (n = 34, 25.8%) (Figure 2).
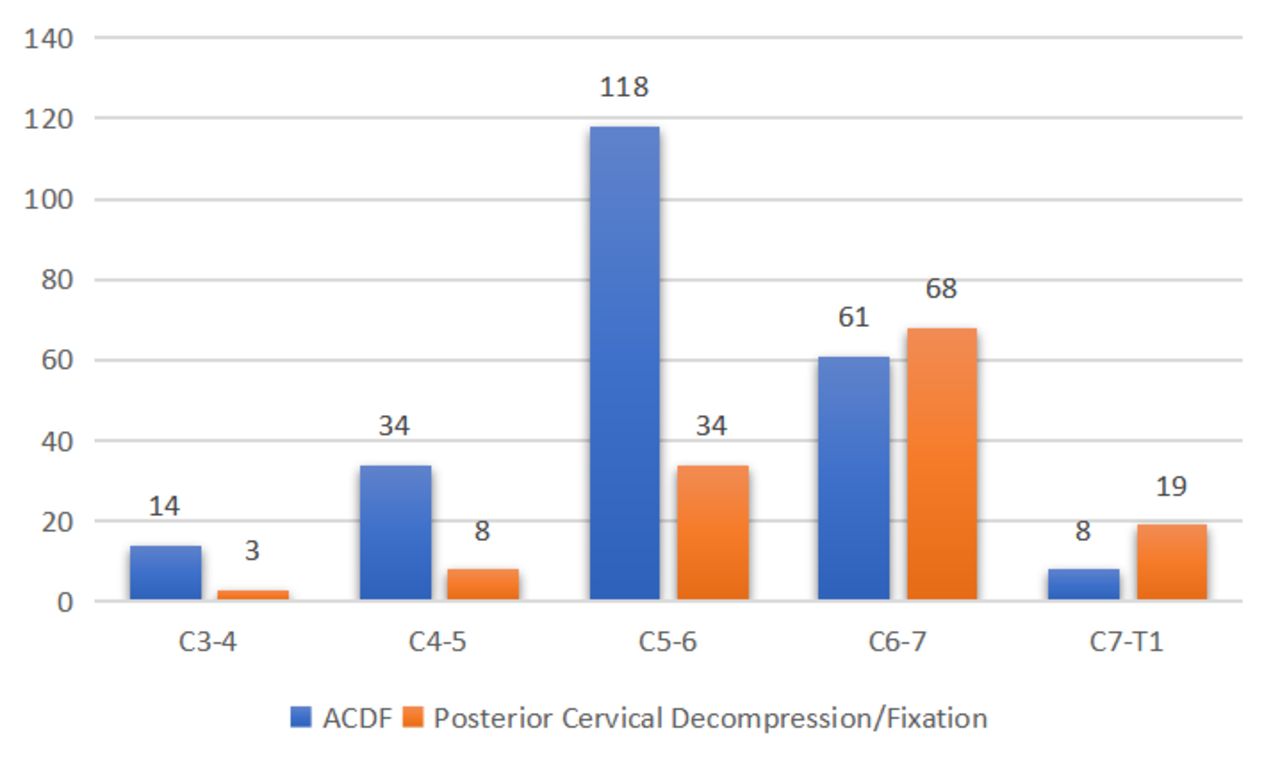
Cervical levels treated by surgery type. There was a significant difference between groups in the levels most commonly treated. Within the anterior cervical discectomy and fusion (ACDF) group, patients most often underwent surgery at the C5-C6 level followed by C6-C7 vs the posterior cervical foraminotomy group that more frequently underwent decompression at C6-C7 followed by C5-C6.
Hospital LOS was statistically different between ACDF and PCF (1.65 vs 1.35 days, P = 0.041). Upon stratification by ASA class, no significant differences were seen in LOS for patients with either ASA class 1 or 2. For patients with ASA class 3, there was a trend toward increased LOS following ACDF that did not reach statistical significance (1.98 vs 1.32 days, P = 0.06). This suggests that the association between LOS and surgical approach may be at least in part explained by confounding by ASA class. To predict LOS based on patient characteristics, a linear regression was performed, which revealed that increasing CCI score and female gender were predictive of increased LOS (P = 0.001 and P = 002, respectively). BMI, age, and procedure type did not contribute to LOS (Table 2). No specific comorbidity, including DM, CHF, COPD, CKD, PVF, or history of CVA, showed significantly increased rates of reoperation at any timepoint.
Linear regression of length of stay predictors.
Readmissions
The overall readmission rate at any timepoint after ACDF was 20.8% compared with 10.9% after PCF (P = 0.014). At 30 days, there was no statistical difference between groups (3.4% after ACDF vs 3.6% after PCF). However, at 90 days, there was a statistically significant higher rate of readmission after ACDF compared with PCF (5.9% vs 0.7%, P = 0.027). There was a trend toward reduction of odds of readmission with PCF relative to ACDF at 90 days (P = 0.067) and 1 year (P = 0.081). At 1 year, there again was a statistically significant higher rate of readmission in the ACDF group compared with the PCF group (14% vs 6.5%, P = 0.027). To again investigate the effect of ASA class on these results, similar analyses were performed for patients within each ASA class. This showed that for patients with ASA class 3, there was a significantly increased rate of readmission at any timepoint following ACDF compared with PCF (35.4% vs 8.7%, P = 0.015). No significant differences were seen at other timepoints or within other ASA classes.
Logistic regression showed that CCI was a significant predictor of odds of readmission at 90 days (P = 0.008) when controlling for surgical approach and at 1 year (P = 0.008) in a model controlling for age, BMI, and surgical approach. Specific comorbidities were analyzed separately with their relationships to readmission, including DM, CHF, COPD, CKD, PVD, and CVA. In respect to readmission at any timepoint, there was a significant association with PVD, COPD, DM, CHF, and CVA (P = 0.029, P = 0.018, P < 0.001, P = 0.028, and P = 0.012). Only PVD was associated with readmission at 30 days (P = 0.004) while CVA trended toward significance (P = 0.070). At 90 days, CHF and CKD were significantly associated with readmission (P < 0.001, P = 0.009). At 1 year, COPD, PVD, and DM (P = 0.008, P = 0.045, and P < 0.001) were associated with increased rates of readmission.
Reoperations
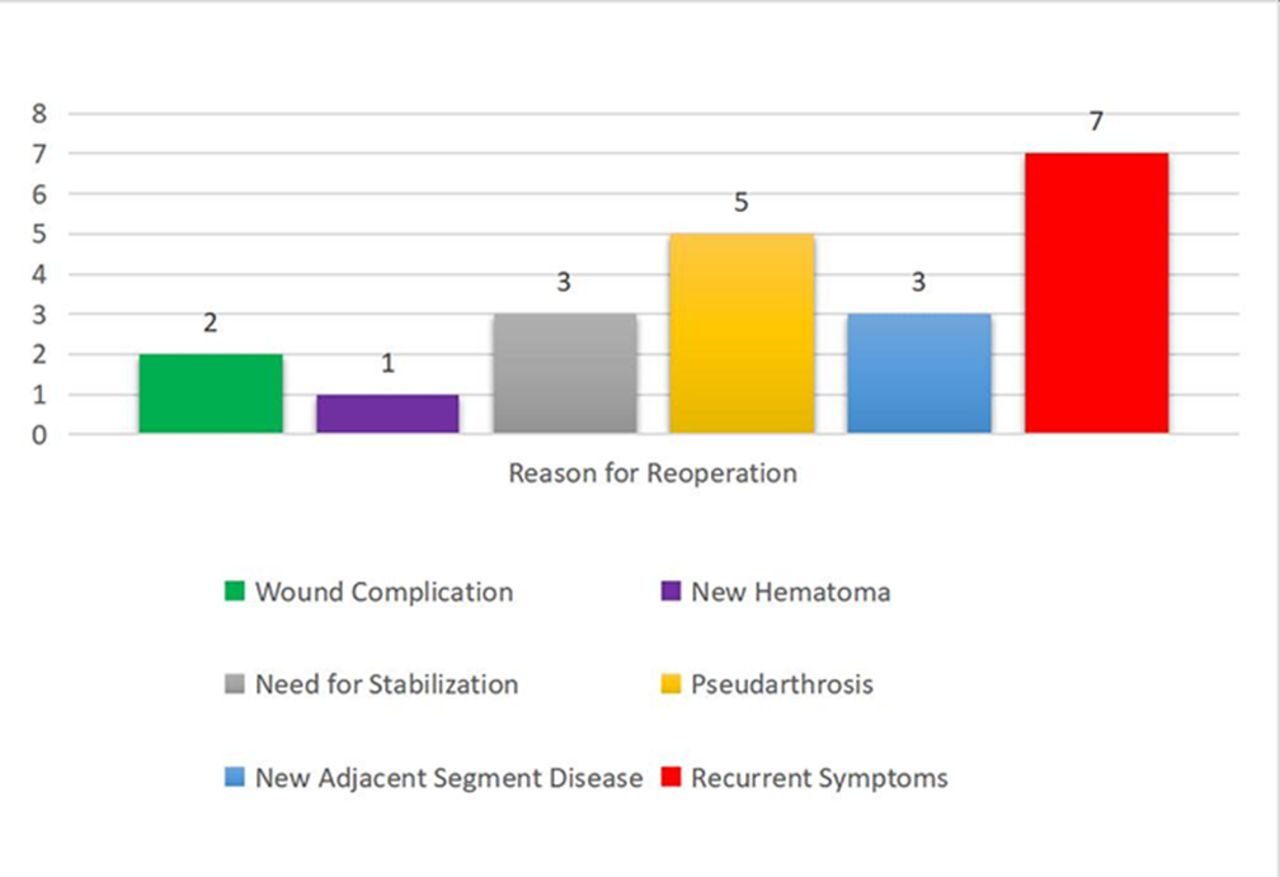
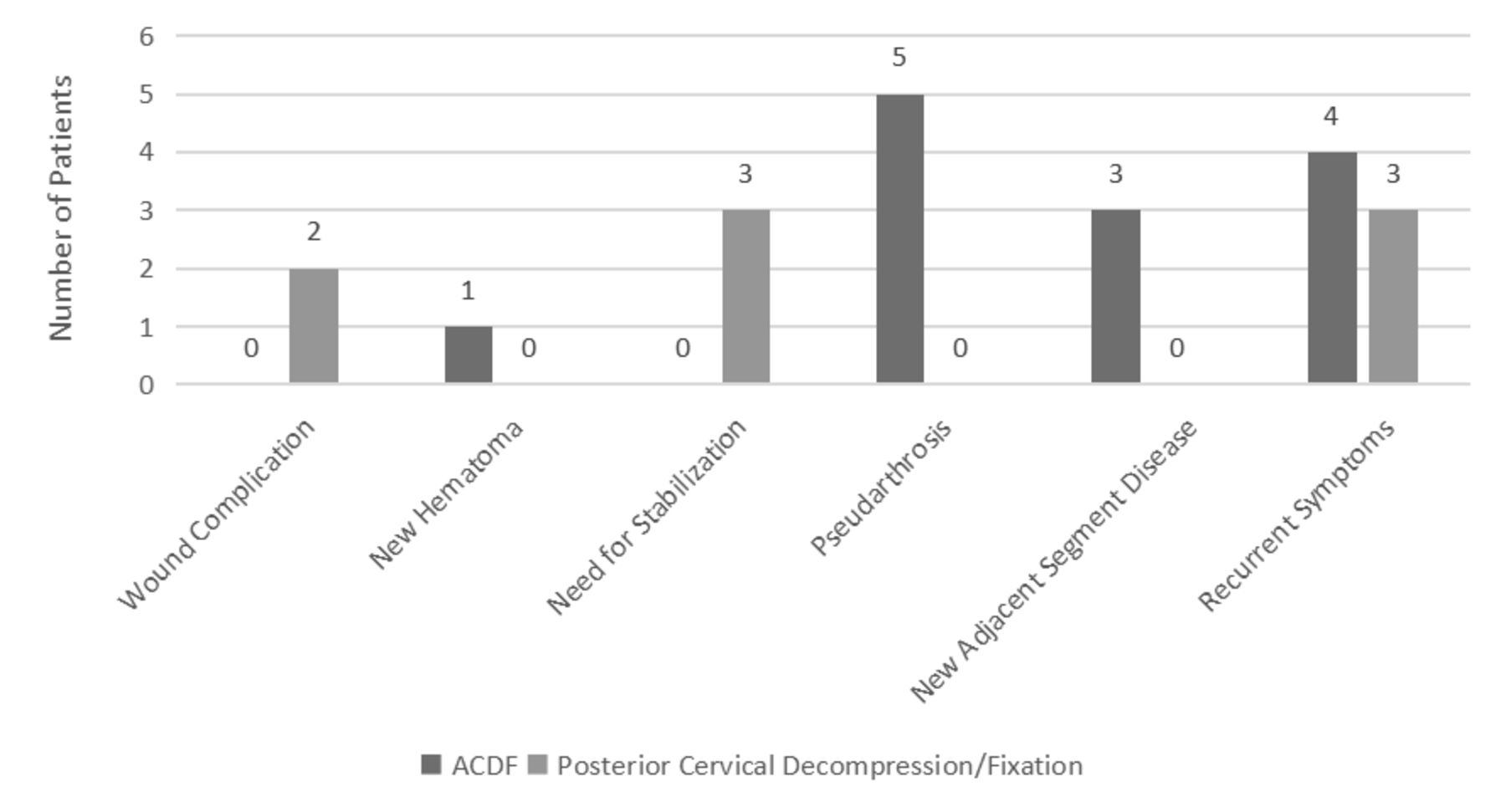
In both groups, the reoperation rate at 2 years was not significantly different between ACDF and PCF (12/236, 5.1% vs 7/138, 5.1%). The rate of reoperation did not show statistical significance based on the cervical level for the whole cohort or when stratifying by procedure type. Current smoking status was not significantly associated with rates of overall reoperation or reoperation for pseudarthrosis in linear regression. There was no significant association with any specific preoperative comorbidity and increased reoperation rate in either group. Reoperation was most frequently performed for recurrent symptoms (33.3% of the total cohort) (Figure 3). Reoperation for recurrent symptoms was not statistically different between ACDF and PCF groups (1.7% vs 2.9%, P = 0.438). This was true, regardless of the level treated for both groups. There was a trend toward significance in reoperation for wound infection more frequently occurring in the PCF group (1.4% vs 0%, P = 0.064). Reoperation for instability was significantly different between groups (0% in ACDF vs 2.2% in PCF, P = 0.023). As expected, reoperation for ASD was only seen in patients undergoing ACDF (1.3% vs 0%), but it was not significantly different between groups. Similarly, reoperation for pseudarthrosis was not seen in PCF patients but occurred in 2.1% of ACDF patients, which did not reach statistical significance (Figure 4). Of the 4 PCFs who underwent reoperation for recurrent symptoms, all had a subsequent ACDF. Of the 4 ACDFs with recurrent symptoms, 1 underwent redo ACDF, 1 had a PCF, and 2 had posterior decompression with fusion. Further evaluation with logistic regression was limited due to the small number of reoperations, preventing the effective evaluation of confounding variables.
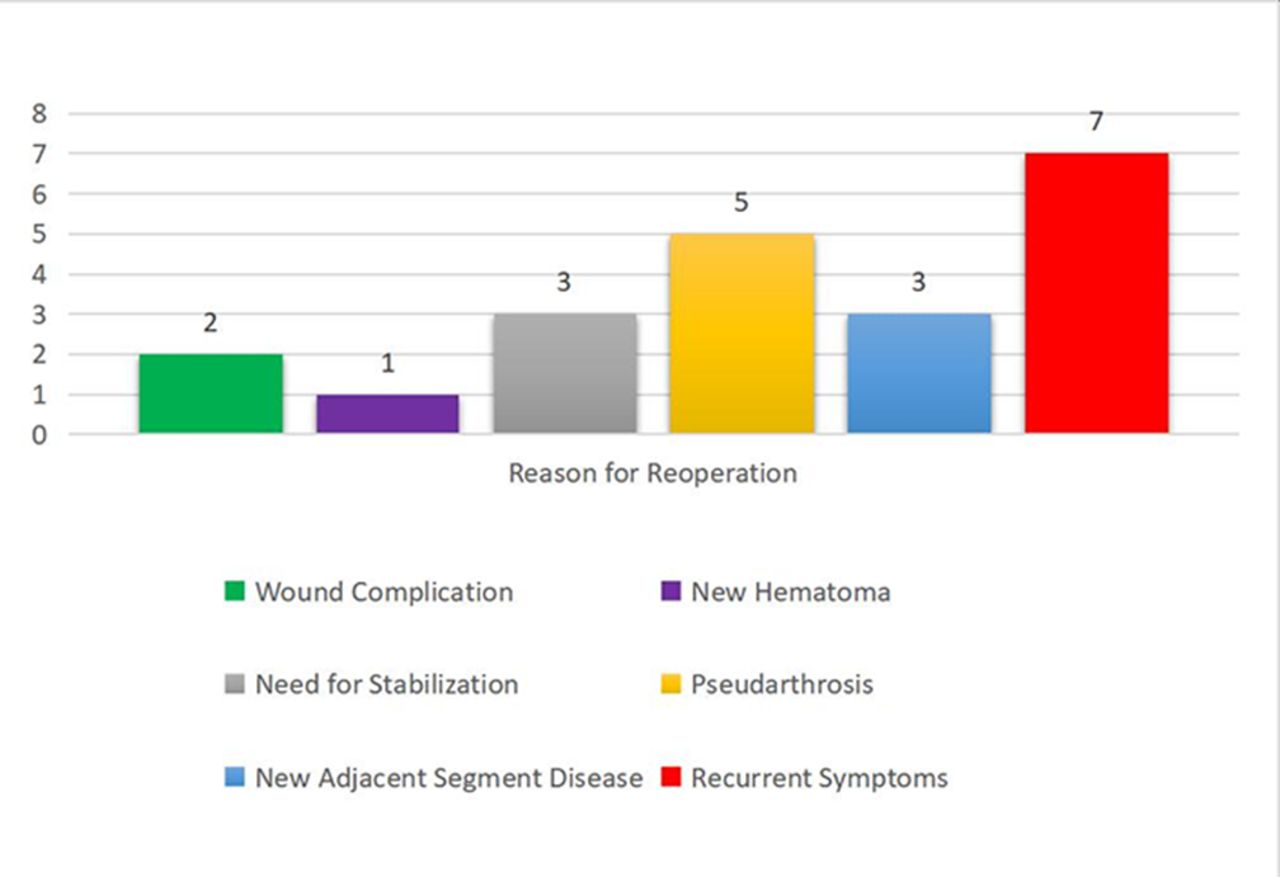
Reasons for reoperation of total cohort. Reoperation was most commonly performed for recurrent symptoms in both groups followed by instrumentation-related complications such as pseudarthrosis and adjacent segment disease.
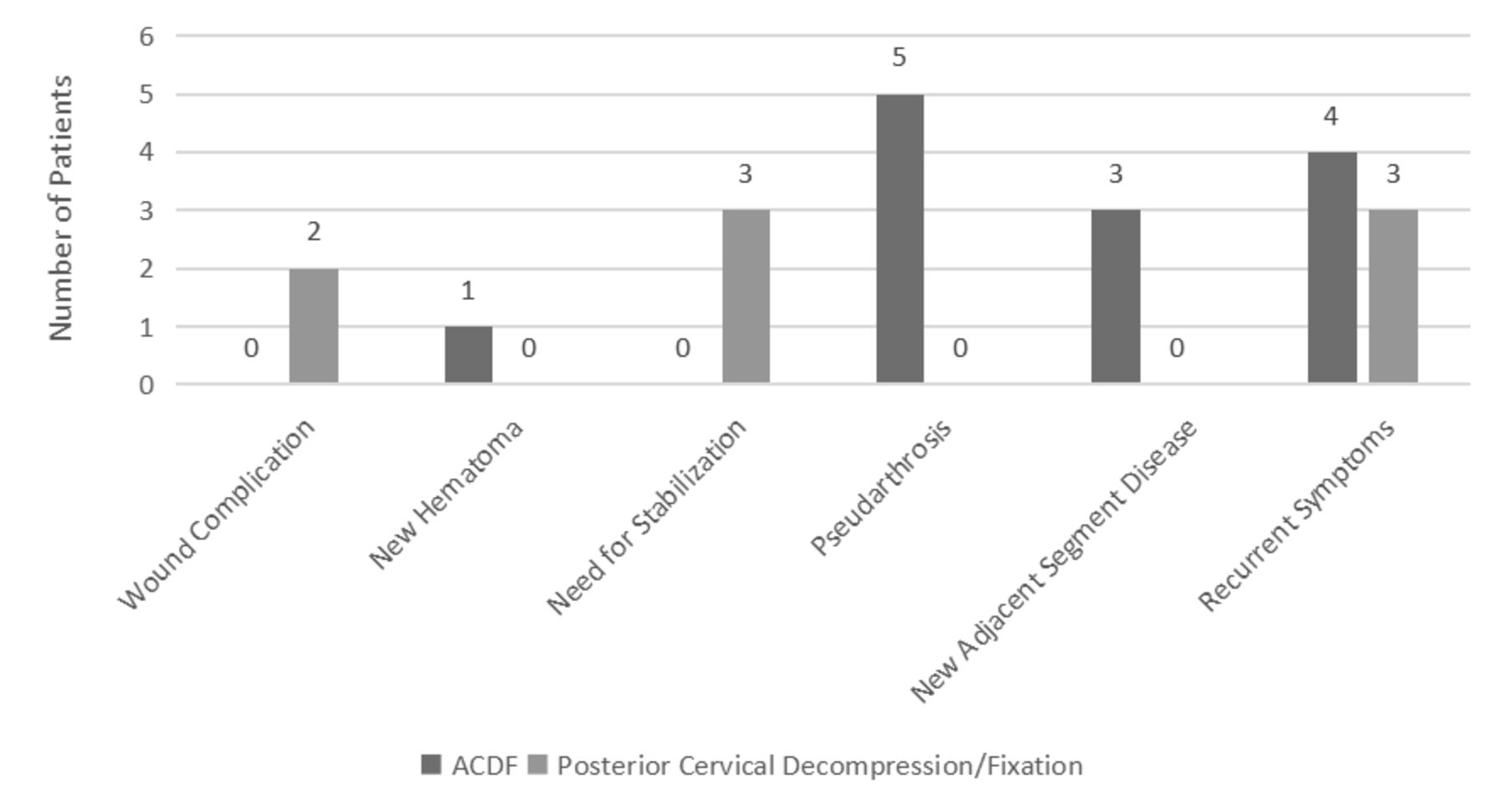
Reasons for reoperation by surgery type. Reoperation for recurrent symptoms was not statistically different between groups. There was significantly more reoperation for adjacent segment disease in the anterior cervical discectomy and fusion (ACDF) group. There were more reoperations for wound infections in the posterior cervical foraminotomy group.
Discussion
The US health care system is being charged with reducing costs while delivering quality care. Proxies for quality that have been adopted by regulatory bodies and individual health care systems include readmission rates, reoperation rates, and length of hospitalization. Prior studies have shown a longer LOS for single-level ACDFs vs PCF for radiculopathy, with PCFs most often discharging to home on the day of surgery, though a small randomized controlled trial (RCT) did not show any difference.7,11,12 Readmission after ACDF has been shown to cost approximately $6727 per patient admission.13 Though ACDFs have a lower 30-day readmission rate when compared with general neurosurgery, the sheer number of procedures performed means a high number of readmissions for a given hospital system.14 Prior studies have shown unplanned overall 30-day readmission rates after cervical surgery for degenerative disease to be 1.04%.15 Readmission at 30 days has been shown to be higher for patients undergoing PCF with a higher rate of postoperative wound complication.7,15 The 90-day readmission rates have ranged from 3.13% to 16.9% after posterior cervical approaches compared with 0.63% to 7.7% after anterior approaches.15
Reoperations are the greatest costs associated with a readmission.13,16 Reoperation rates in previous studies have ranged from 4% to 28% after ACDF and from 5% to 27% after PCF.5,10–12,16–19 Lubelski et al recently published the first propensity-matched retrospective analysis comparing 188 ACDFs with 140 PCFs at a single center with 2-year follow-up and found that the same-level reoperation rate was not significantly different, 4.8% compared with 6.4%, respectively. Unsurprisingly, reoperation rates for ASD are more common after fusion procedures as are reoperations for pseudarthrosis after PCFs. ASD and pseudarthrosis after ACDF have been cited at a rate of 3% and 3.1%.11,20 Wound infections have been cited to be the most common complication after PCF, ranging from 1% to 4.5%.5,11,21–23 Risk factors for reoperation in this population are younger age, male patients, preoperative diabetes, and lower BMI, which were not demonstrated using linear regression in our cohort.16,24,25 The subsequent surgical approach for recurrent symptoms has been shown to favor ACDF, regardless of the approach of the index surgery.26,27
Three randomized trials have been conducted to determine the superiority in ACDF vs PCF but are limited by small sample sizes. Herkowitz et al randomized 33 patients to ACDF or PCF and showed that 94% of patients who underwent ACDF reported an excellent or good outcome (as defined by relief of pain or improvement of pain requiring occasional analgesics without lifestyle restrictions) vs 75% of the PCF group.28 Ruetten et al compared endoscopic PCF with ACDF in an RCT with 175 patients suffering from lateral disc herniations and found no difference in reoperation between the groups (4.7% in the ACDF group and 6.7% in the PCF group). This study focused on revision surgery for same-level pathology not for ASD or pseudarthrosis, with more reoperations after ACDF at 12% than PCF at 2% to 3%.2 Another RCT by Wirth et al showed no difference in improvement from surgery in either ACDF or PCF in 72 patients nor a significantly different reoperation rate for recurrent symptoms (28% for ACDF and 27% for PCF).12
Previous studies that have attempted to compare these groups have been limited by their small sample sizes, particularly regarding the PCF cohort, have included a range of procedures and indications or have utilized national surgical databases, which are fraught with reporting errors and lack of clinical details. Given the clinical uncertainty, this study presents data from the largest single-center retrospective cohort comparing single-level ACDFs with PCFs. The groups are similar in preoperative characteristics, which strengthen the comparisons of postoperative outcomes. Additionally, we include a 90-day follow-up time for readmission, which is lacking in prior studies.29,30 Our study showed a statistically different LOS between ACDF and PCF (1.65 vs 1.35 days), with predictors being female sex and increasing CCI score. There was a significantly higher rate of readmission after ACDF overall, at 90 days and 1 year. Readmission at any timepoint was more common in those patients with preoperative PVD, COPD, DM, CHF, and CVA, regardless of the procedure type. We did not find any association with smoking status and readmission or reoperation, as has been previously reported in the literature with posterior cervical decompression and fusion procedures.31
The reoperation rate was 5.1% after both ACDFs and PCFs. Recurrent symptoms were the most common cause for reoperation in both groups (1.7% vs 2.9% in ACDF vs PCF, respectively) and were not significantly different. We found the rate of reoperation for pseudarthrosis and ASD was 2.1% and 1.3% in the ACDF group, which trended toward significance and reached statistical significance, respectively. We found that wound complications were associated with reoperation in 1.4% of the PCF group and in no patients undergoing ACDF with a trend toward significance.
Our data suggests that while both approaches effectively address the underlying pathology, PCF may result in a shorter hospitalization and fewer readmissions than ACDF. These factors in combination with the additional cost associated with instrumented fusions may lead surgeons to elect to perform PCF in situations of clinical equipoise.
The present study is limited by its retrospective study design and lack of patient-reported outcomes. Since the data are from a single center, this study’s findings may not be generalizable to other clinical settings and may inadvertently omit readmissions or reoperations outside of the University of Pennsylvania health care system. Additionally, while the 2-year follow-up time is sufficient to capture index-level failures and readmissions, longer-term follow-up would elucidate durability, long-term complications, and need for revision surgery, particularly due to ASD. Future studies should focus on prospective reduction of readmission rates within certain at-risk patient populations, taking into account the findings from the available retrospective literature, which will also limit the potential attrition bias. Additionally, with the increasing utilization of endoscopic approaches to the posterior cervical spine, a multicentered, prospective study comparing the 3 treatment modalities in terms of clinical outcomes and health care costs should also be conducted.
Conclusions
ACDFs and PCFs were performed for radiculopathy in similar patients with respect to demographics and preoperative characteristics. Overall reoperation rates between ACDF and PCF were not significantly different. Similarly, there was no statistically significant difference of reoperation for recurrent symptoms, demonstrating that either procedure effectively addresses the indication for surgery. However, LOS was significantly longer after ACDF than PCF. Additionally, the overall readmission rate at any timepoint was significantly higher after ACDF compared with PCF, which was seen at 90 days and 1 year postoperatively. These data suggest that PCF may be superior to ACDF in terms of LOS and readmission rates.
Acknowledgments
The authors would like to thank Jessica Nguyen, Zeena Jalal, Esther Jung, Gokul Karthikeyan, and Anthony Nguyen for their assistance with data collection and refinement. Additionally, we thank Eileen Maloney-Wilensky and Marie Kerr for providing logistic and administrative support to the research team at the department of Neurosurgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures David Casper reports grants/contracts from Cerapedics (paid to institution); consulting fees from Stryker Spine and Cerapedics; and serving as a Deputy Editor for Clinical Spine Surgery Journal. The remaining authors have nothing to disclose.
- Received February 7, 2023.
- Accepted February 22, 2023.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.