


Abstract
Background There has been increased interest in exploring methods to reduce postoperative pain without opioid medications. In 2015, a multimodal analgesia protocol was used involving the perioperative use of celecoxib, gabapentin, intravenous acetaminophen, lidocaine, and liposomal bupivacaine. Overall, the goal was to reduce the utilization of scheduled opioids in favor of nonopioid pain management.
Methods The results of a consecutive series of 1- to 2-level open primary lumbar fusions were compared to a cohort of patients after the implementation the perioperative multimodal pain management protocol. Primary endpoints included patient-reported pain scores and secondary endpoints included length of stay.
Results There were 87 patients in the preprotocol cohort and 184 in the protocol cohort. Comparing protocol and preprotocol patients, there were no significant differences in patient demographics. There was significantly average lower pain in the protocol group on postoperative day (POD) 1 (4.50 vs 5.00, P < 0.02) and POD2 (4.42 vs 5.50, P < 0.03). There was a lower pain score on POD0 (4.80 vs 5.00), but it was only clinically significant. There was a correlation between pain and duration of surgery in the preprotocol patients (POD0 R = 0.23, POD1 R = 0.02, POD2 R = 0.38), but not in the protocol patients (POD0 R = −0.05, POD1 R = −0.08, POD2 R = −0.04). There was a shorter length of stay in the protocol cohort (2.0 vs 3.0, P < 0.01). Finally, there was an approximately 35% reduction in morphine milligram equivalents of opioids in the protocol vs preprotocol cohorts (36.2 vs 57.0, P < 0.05).
Conclusion Our novel multimodal pain management protocol significantly reduced postoperative pain, length of stay, and opioid consumption in this patient cohort. Opioid usage correlated to pain in the protocol patients, while the preprotocol patients had no correlation between opioid use and pain medication.
Clinical Relevance In this study, we demonstrated that preoperative and intraoperative analgesia can reduce postoperative pain medication requirements. Furthermore, we introduced a novel concept of a correlation of pain with opioid consumption as a marker of effective pain management of breakthrough pain.
Level of Evidence 4.
- multimodal analgesia
- 1- to 2-level lumbar fusion
- reduced opioid consumption after lumbar fusion
- pain management
- lidocaine
- opioid
- narcotic
- morphine
- spine fusion
- gabapentin
- acetaminophen
- postoperative pain
INTRODUCTION
While 1- to 2-level open lumbar fusion surgeries have evolved into widely used treatments for spinal deformity and degenerative conditions, there is a delicate balance to controlling postoperative pain. To date, pain management techniques have heavily relied on opioid analgesics for adequate control in spine surgery patients; however, this is not without significant downsides. Opioids have been shown to have a wide range of adverse effects, including nausea, vomiting, respiratory depression, urinary retention, and constipation.1 Additionally, more significant and harmful complications of these agents may result in dependence, including tolerance, addiction, and possible abuse.2 Thus, opioid side effects may contribute to some common and long-term postoperative complications. The field of orthopedic surgery has become the third-highest prescribing specialty of opioid analgesia in the country, demonstrating a need for improved methods of pain control in this field.3
In general, spine surgery is considered to be significantly painful in comparison to other musculoskeletal surgeries, often requiring higher than average levels of analgesia.4 As a result, postoperative pain limits patient ambulation and activity after surgery, while those with less pain tend to mobilize earlier.5 Ultimately, the goal is to avoid complications of prolonged immobilization that can present as deep venous thrombosis, pulmonary embolism, atelectasis, decubitus ulcers, and ileus. As these consequences have significant effects on patient outlook and patient satisfaction, improved pain management strategies are critically important to successful patient safety and outcomes.
Multimodal pain protocols have become an area of interest in orthopedic spine surgery as a potential alternative therapeutic regimen for pain. Multimodal protocols exploit the therapeutic effect of various medications that are often effective at lower doses than the dose at which side effects become significant. Thus, for example, at high doses, nonsteroidal anti-inflammatory drugs (NSAIDs) can cause renal insufficiency and gastric ulcers.6 However, at low doses, NSAIDs can exert therapeutic effects. Additionally, having multiple analgesic medications with different mechanisms of action results in a synergistic therapeutic effect that is addictive. A short-term goal of such multimodal protocols is the reduction of opioid intake, whereas in the long term, such protocols may improve patient safety by accomplishing improved pain control with fewer side effects. Opioid-sparing multimodal protocols emphasize improved outcomes through a focus on the complexity of the pain pathways and concomitantly aim to decrease adverse medication side effects.7,8
In May 2015, a multidisciplinary team at our institution under the leadership of the senior author developed and implemented a multimodal analgesic protocol as an alternative to the historically utilized opioid protocol for postoperative pain control. This system was applied to patients who underwent 1- to 2-level open lumbar fusion surgeries and revolves around the administration of nonopioid medications spanning the perioperative period. As spinal surgery techniques and treatments continue to improve, implementing this protocol is believed to create an improved method for pain control—eliciting not only a better patient experience but also a better overall health status throughout the perioperative period.
The purpose of this study was to determine whether the use of an opioid-sparing multimodal pain protocol in the perioperative period caused a reduction in postoperative pain, shorter length of stay, and reduced opioid consumption in patients undergoing 1- to 2-level open lumbar spinal fusion surgeries.
MATERIALS AND METHODS
This was a retrospective cohort study centered on 271 patients (aged 23–86 years) scheduled for open 1- to 2-level primary lumbar fusion surgery between 2010 and 2017. All procedures were performed by 1 of 2 fellowship-trained orthopedic spine surgeons at 1 academic facility. Data were collected via medical record review from all physician and nursing documentation provided over the course of the patient’s stay. Those excluded from this study were patients who underwent spinal surgery secondary to trauma or those who had more than 2 levels of spinal fusion or decompression. Demographics, medical comorbidities, and preoperative medication histories did not exclude patients from the review.
Comparing both cohorts of patients, there were no statistically significant differences in mean age (64 vs 61 years), gender distribution (48% vs 52% male), BMI (30 vs 31), or duration of surgery (2:32 vs 2:31). There were no statistically significant differences in pain between 1- and 2-level surgeries (thus, the 1- and 2-level surgeries were combined).
Prior to May 2015, the pain management protocol predominantly included scheduled Oxycontin (10 mg per oral [PO] Q12h). Patients were given acetaminophen or tramadol for mild pain, oxycodone-acetaminophen (Percocet) for moderate to severe pain, and 2 mg intravenous (IV) hydromorphone for severe breakthrough pain. However, patients were not given scheduled steroids, ibuprofen, or gabapentin for prophylactic or analgesic purposes. For the purposes of this study, that pain management regimen was deemed the “preprotocol” group.
After May 2015, the multimodal pain protocol was uniformly administered to patients undergoing 1- to 2-level primary lumbar fusion surgeries. Patients were not informed of the multimodal protocol, nor did they know of any variations in postoperative management. In the “protocol” group, cohort patients received multimodal pain therapy, which included preoperative gabapentin 900 mg orally once and celecoxib 200 mg orally once (with the exception of renal risk). Intraoperatively, these patients received IV lidocaine 2 mg/kg/h, IV acetaminophen 1000 mg every 6 hours for 3 doses, and IV dexamethasone 10 mg once (for the prevention of postoperative nausea/vomiting). Patients also received an injection of 30 mL of liposomal bupivacaine mixed with 30 mL of bupivacaine with epinephrine. Postoperatively, patients were given gabapentin 300 mg orally 3 times per day for 5 days and celecoxib 200 mg orally for 5 days (Table). Patients were given oxycodone (Roxicodone) for moderate to severe pain and were given tramadol for mild pain. Patients were also given acetaminophen for mild pain (however, care was taken to avoid exceeding 4 g per day of acetaminophen) and were given 2 mg IV hydromorphone for severe breakthrough pain.
Perioperative multimodal pain protocol administered to protocol patients.
The patients’ measurements of pain were subjectively collected via nursing examination every 6 hours over the course of their stay. Patients were asked to rate their pain on a scale of 0–10 (10 being the worst pain) and to rank their acceptable pain level from 0 to 10 as well. Both absolute pain scores and the difference between patient-reported pain and acceptable pain level (to normalize for patient pain tolerances) were calculated for each postoperative day. Pain measurements were obtained over the course of 3 days, the first including the day of surgery, or POD0, followed by POD1 and POD2. Additionally, length of stay was noted and compared to determine whether improvements in pain decreased overall hospital stay in these patients. Length of surgery was taken from the nursing operative notes by comparing “surgery start” and “surgery end” times, which were recorded on all surgeries. All opioid medications taken by each patient in both preprotocol and protocol were also obtained and evaluated. Morphine equivalents were then calculated and compared to those in both cohorts to assess whether they were decreased in those receiving protocol therapy.
As this was a quality improvement project to improve patient care, institutional review board (IRB) approval was not sought prior to implementation of the protocol. IRB approval (an exemption) was obtained for the retrospective review of the medical records.
Statistical Analysis
Software utilized for statistical analysis includes R Studio (version 1.2.5033; RStudio, Inc.) and R (version 3.6.3; Vienna, Austria). The distributions of continuous variables were evaluated for normality by calculating the skew and kurtosis and plotting the histogram. Continuous data were summarized by the mean and SD or median and interquartile range for data with a normal or non-normal distribution, respectively. Independent-samples t tests and Mann-Whitney U tests were used to test for differences in demographics, surgical details, length of stay, reported pain, and opioid consumption between the 2 protocol groups, as appropriate. Spearman’s correlation coefficients were computed to test for correlations between average reported pain each day and (1) duration of surgery and (2) total opioid consumption. Statistical significance was set at P = 0.05.
RESULTS
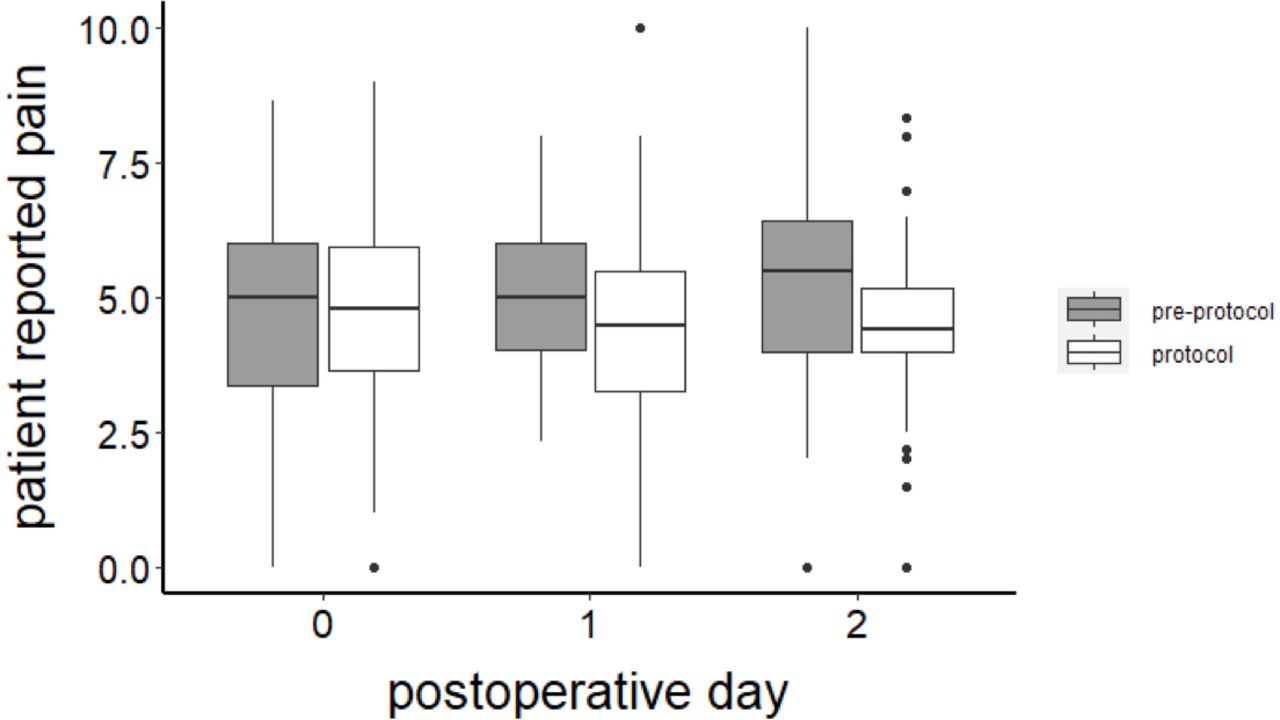
There were 87 patients in the preprotocol cohort and 184 patients in the protocol cohort. There was significantly average lower pain in the protocol group on POD1 (4.50 vs 5.00, P < 0.02) and POD2 (4.42 vs 5.50, P < 0.03) (Figure 1). There was an average lower pain score on POD0 (4.80 vs 5.00, P > 0.05), but it was only clinically significant. The difference between the patient-reported pain and their reported acceptable pain levels was also on average lower in the protocol patients on POD0 (0.98 vs 1.65) and POD1 (0.74 vs 1.25), but this was also only clinically significant.

Average pain scores in the preprotocol vs protocol cohorts by postoperative day.
There was a correlation between pain and duration of surgery in the preprotocol patients (POD0 R = 0.23, POD1 R = 0.02, and POD2 R = 0.38) but not in the protocol patients (POD0 R = −0.05, POD1 R = −0.08, and POD2 R = −0.04). Thus, the protocol was effective in controlling pain throughout the perioperative period. There was a statistically significant shorter length of stay in the protocol cohort (2.0 vs 3.0 days, P < 0.01).
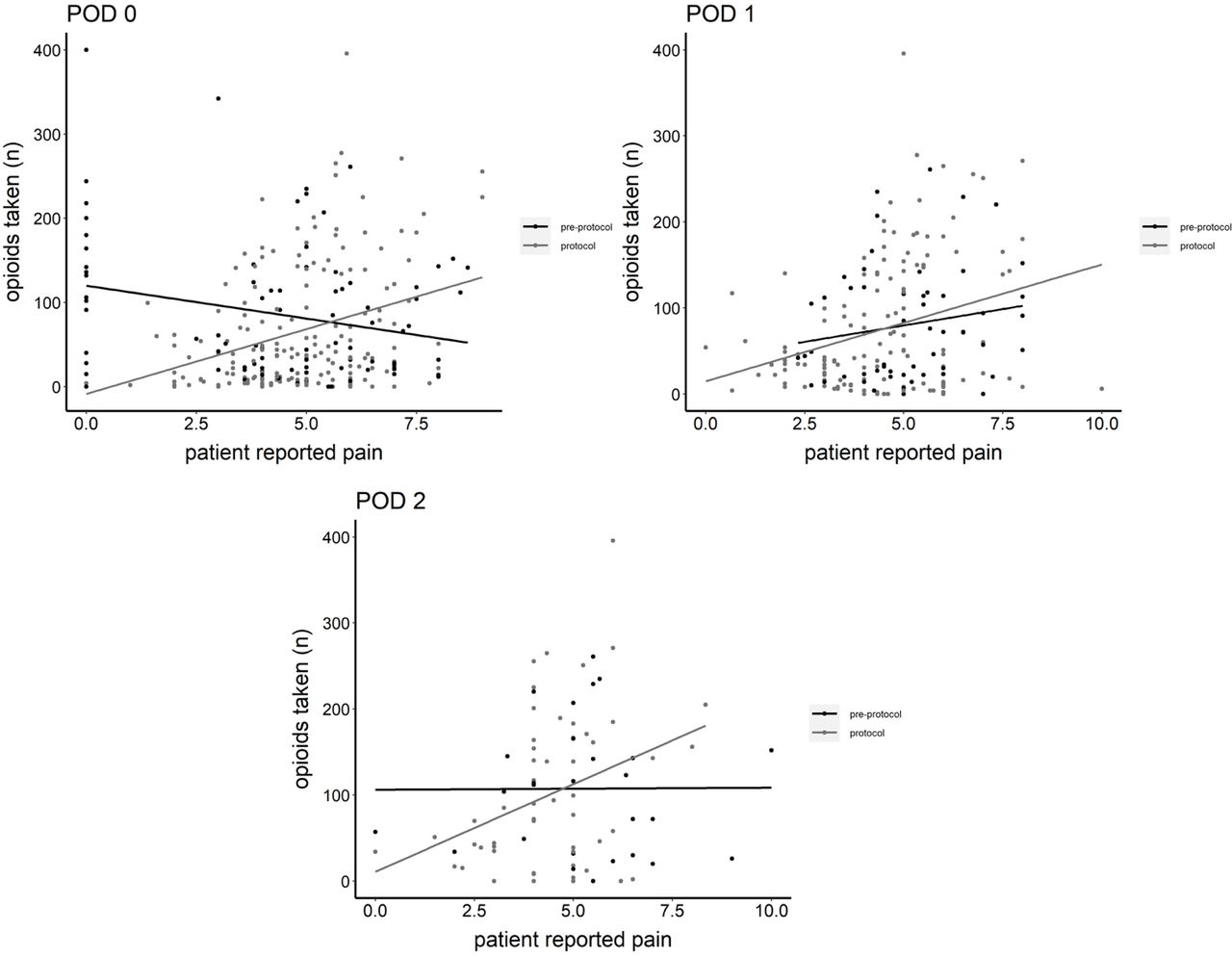
We found an approximately 35% reduction in morphine milligram equivalents of opioids in the patients in the first 3 hospital days in the protocol patients vs the preprotocol patients (36.2 vs 57.0 mg, P < 0.05). There was a correlation between pain and opioid consumption on POD0, POD1, and POD2 in the protocol patients (R = 0.34, R = 0.23, and P < 0.05), but not at all in the preprotocol patients (R = −0.12, R = 0.16, R = −0.07, and P > 0.2), suggesting that the patient’s pain in the protocol cohort correlated with an appropriate need for opioid analgesics (Figure 2). Overall, there were no specific complications attributed to those undergoing protocol therapy.

Correlation of patient-reported pain and morphine equivalent consumption over postoperative day (POD).
DISCUSSION
In the past, spine surgery success has been determined through objective measures such as fusion rates, deformity correction, and other clinician-based data; however, a new focus centers around patient-reported outcomes such as pain and its implications on hospital stay and long-term health.9 In this study, we have reported the results of a multimodal pain protocol in a population of patients undergoing 1- to 2-level open lumbar spinal fusion surgeries and compared them to a typical group of patients who underwent opioid pain therapy alone. In comparison to a preprotocol cohort, those who underwent protocol therapy had improved pain scores, reduced hospital stays, and decreased consumption of opioid medications.
Other studies have evaluated the success of multimodal pain protocols, and while they have been successful, it has been demonstrated over a smaller sample in a wide variety of spinal interventions. The strength of our study is that it includes a large number of consecutive, relatively homogenous patients who underwent similar single-level surgeries. By only analyzing the pain scores through POD2, we attempted to include the typical postoperative course (the average length of stay was 2.5 days). We expect that patients who remain in the hospital for nonpainful medical reasons (such as resumption of anticoagulation or atrial fibrillation) would confound the analysis of length of stay. We believe that the analysis of pain scores alone can be confounded by differences in patient pain tolerance and in acceptable pain levels. Thus, we included an analysis of the patient’s acceptable reported pain level (which did not differ between protocol and preprotocol groups) and the difference between the actual pain scores and the acceptable pain levels. We found that the protocol reduced the patient’s reported pain and the amount of pain exceeding the acceptable level and that the protocol reduced the overall opioid consumption. More importantly, we determined that a correlation existed between opioid consumption and pain scores in the protocol patients (as one would expect considering that opioids are in fact a pain medication). Surprisingly, there was no correlation between morphine milligram equivalent pain scores in the preprotocol patients. The lack of a correlation suggests that preprotocol pain medication use was either overmedicating or undermedicating patients on a systematic basis.
Again, while other studies exist reporting multimodal pain protocols, this protocol uses a unique combination of agents designed to focus on the main components of the complex pain pathways. The utilization of these medications has correlated with improved perioperative pain control and demonstrated ration use of opioids in protocol patients.
Components of the protocol, including NSAIDs, have demonstrated high utility in pain reduction in the perioperative period. They work via inhibition of inflammatory pathways activated by prostaglandins, a byproduct of arachidonic metabolism via cyclooxygenase-1 and 2 (COX-1,2), which increase in both local and cerebral spinal fluid (CSF)–promoting hyperalgesia.10 While the use of NSAIDs in spinal surgery has proven beneficial, it has been previously implicated to cause pseudoarthrosis and impaired bone formation. Dodwell et al reviewed NSAIDs for postoperative pain management through numerous retrospective studies and determined no increased risk of pseudoarthrosis over a 12-month period in postoperative spine patients.11,12 Additionally, it has been shown that high doses of nonselective NSAIDs, such as Ketorlac, in the acute postoperative period significantly decrease patient pain without demonstrating adverse effects on spinal fusion.13,14 With prolonged use, however, the inhibition of COX-1 receptors has been revealed to adversely affect bone healing.15 To avoid this, selective agents such as celecoxib, a COX-2 inhibitor, have gained increasing popularity. These agents not only avoid adverse effects on bone healing but, when used perioperatively, also have a beneficial reduction in central and peripherally generated inflammatory hypersensitivity as well as the necessity of opioid analgesia.12,15 These agents are not routinely used in patients with renal insufficiency or renal failure to reduce the risk of renal toxicity.
Gabapentin, originally developed as an anticonvulsant, works as an inhibitory analog in the central nervous system. The mechanism of action is the reduction of the release of several excitatory neurotransmitters responsible for nociceptive activation in the spine, thereby reducing pain.2 When given preoperatively, gabapentin has also demonstrated decreased requirements for opioid analgesia after spinal surgery.16,17 Additionally, gabapentin has been shown to act synergistically with NSAIDs, such as celecoxib, and can further decrease hyperalgesia when given concomitantly for spinal fusion patients.18 Gabapentin can cause a host of adverse events, including fatigue, somnolence, dizziness, and abnormal vision; additionally, although rare, when toxic systemic levels are reached, symptoms may progress to ataxia, nystagmus, and choreoathetosis.18 Gabapentin is not recommended in patients with a history of seizures. If patients are taking low-dose gabapentin (100 mg orally 3 times per day, for example) prior to surgery, we will increase the gabapentin dose up to the level described above (900 mg orally 3 times per day), but not above that.
Acetaminophen is a popular analgesic utilized for its low side-effect profile when given within therapeutic dosing. While the mechanism is not entirely clear, it has been proposed to have antinociceptive effects at the level of both peripheral and central nervous systems. When compared to its oral counterpart, IV acetaminophen has been shown to lower opioid requirements, decrease hospital length of stay, and reduce the risk of discharge to skilled nursing facilities.19 Ultimately, studies have demonstrated that when given in conjunction with NSAIDs, a statistically significant decrease in postoperative morphine equivalents was appreciated in patients undergoing spinal surgery.20
The use of IV lidocaine exerts its effects as an analgesic and anti-inflammatory agent through the inhibition of central nervous system excitatory pathways. Although the half-life of lidocaine is very short, ranging from 90 to 120 minutes, the nociceptive effect is long-lasting because it prevents activation of pain pathways.21 Farag et al demonstrated that IV lidocaine can decrease patient-reported pain scores and opioid requirements during the initial 48 hours after complex spinal surgery. It is believed that lidocaine and its metabolites not only act locally after soft tissue injury but can also remain in the CSF for extended periods exerting prolonged analgesic effects.21 Overall, each agent in our protocol has been selected to not only combat the complexities of the pain pathway but also ultimately decrease adverse outcomes from the preprotocol opioid analgesic administration. IV lidocaine is unfamiliar to many orthopedic surgeons. In general, orthopedic injections avoid IV injection to avoid systemic effects from a fracture hematoma block or joint injection. Systemic complications from IV lidocaine injection include but are not limited to hypotension, nausea, vomiting, pulmonary, and neurologic issues.21 In general, although there is a concern about lidocaine potentiating cardiac arrhythmias, lidocaine is actually a class 1B anti-arrhythmic medication. Obviously, in the operating room, lidocaine is administered carefully under continuous cardiac monitoring. While some other studies utilize IV ketamine instead of IV lidocaine, our multimodal group selected IV lidocaine to reduce the risk of delirium in elderly patients from ketamine, which has a lower risk of cardiac toxicity and arrhythmia. However, ketamine is known to cause substantial hallucinations in some patients.22
Total IV anesthesia (TIVA) is another component of our pain protocol. TIVA relies on the absence of inhaled gases for anesthesia. In general, TIVA is associated with a lower risk of postoperative nausea and vomiting compared to inhaled anesthetics. Additionally, TIVA is more compatible with spinal neuromonitoring.
Local anesthetics are injected at the time of surgery as well. We utilize both local anesthetics with epinephrine (to increase persistence in the surgical site) and local anesthetics in a liposomal format (to dissolve over 3 days). Some studies have demonstrated the benefit of liposomal injectables in spine surgery.23 Other studies have shown no benefit to liposomal injections in spine surgery. The maximum safe dose of local anesthetics is based on which is used and the body weight of the patient in question. Local anesthetic toxicity is a serious complication due to its inhibition of voltage-gated sodium channels in the central nervous system, and its effects are characterized by circumoral numbness, dizziness, tinnitus, blurred vision, and muscle twitching that can progress to tonic-clonic seizures and respiratory depression.24,25
We acknowledge that our study does have some limitations. First, we do not account for patient comorbidities in the assessment of our pain scores and morphine equivalent calculations. This study did not attempt to preoperatively evaluate whether patients required chronic opioid therapy for pain or other comorbidity but instead aimed to assess whether immediate perioperative management would elicit a difference in the hypothesized outcome measures. That being said, there were patients in the cohorts who demonstrated an increased need for opioid analgesia; however, these patients were advised to wean off all opioid analgesics as well as NSAIDs (to minimize bleeding risks) 2 weeks prior to surgery. Additionally, this provides an area for further analysis to identify whether or not our protocol is effective on opioid-tolerant vs opioid-naïve patients.
At the same time, with knowledge of the opioid epidemic, a conscious bias toward overall reduction in opioid administration has been pursued in these cohorts. Second, this study was not a randomized blinded study, though preprotocol and protocol patient data collection variables were well defined. Third, the collection of data was subjective from nursing evaluation of patients at inconsistent and varied times, but again, for our data collection, review of these records was taken at predetermined intervals for standardization. Finally, with an overall shift in decreased hospital admissions as a whole, patients who underwent operations in 2010, at the beginning of the study, may have experienced similar hospital admissions to those who underwent operations more recently under current guidelines. Furthermore, the retrospective comparison to a historical control group is less accurate than a concurrent, case-controlled study. These results also may not be applicable to a less painful surgery, such as a microdiscectomy. We deliberately selected the study population (1–2 level lumbar fusion) because it is a common, painful surgery. We also do not know the effect of pain protocol on readmission, reoperation, or long-term outcome
Overall, this study demonstrates the use of a unique multimodal pain protocol that aims to improve patient pain throughout the perioperative period. While a consensus on a universal protocol is yet to be determined for spinal surgery, this protocol provides additional positive support to an opioid-sparing pain regimen. Further studies into this protocol are underway to better assess its utility in multilevel spinal surgery in all regions of the spine and ultimately in all areas of orthopedics.
CONCLUSION
Our novel multimodal pain management protocol significantly reduced postoperative pain, length of stay, and opioid consumption in this homogenous group of patients. Our preoperative and intraoperative interventions appear to have reduced the effect of a long duration of surgery on pain in the protocol patients since there was no correlation between length of surgery and pain in the protocol patients; thus, opioid usage correlated to pain in the protocol patients suggesting rational use.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Institutional Review Board approval was obtained for review of patient medical records
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.