


Abstract
Background There is an increasing acceptance of conducting minimally invasive transforaminal lumbar interbody fusion (TLIF) in ambulatory surgical centers (ASCs). The Centers for Medicare and Medicaid Services (CMS) introduced the Hospitals Without Walls (HWW) program in March 2020. This program granted hospitals regulatory flexibility to offer services and procedures in nontraditional locations, including ASCs. However, implementation hurdles persist.
Methods A survey was sent to 235 surgeons regarding the use of ASCs for performing TLIF surgeries on elderly patients. Multiple-choice questions covering various aspects of TLIF practice preferences, including surgical indications, decision factors for choosing ASCs over hospitals, implementation hurdles, reimbursement concerns, staffing issues, and the impact of CMS rules and regulations on TLIF in ASCs, particularly concerning physician ownership and self-referral conflicts governed by the Stark law, were asked.
Results The survey completion rate was 25.8% (Figure 1). The most common surgical indications for TLIF in ASCs were spondylolisthesis (80%), spinal stenosis (62.5%), and low back pain (47.5%). Most surgeons (78%) believed TLIF could be safely performed in ASCs. Streamlined workflow, lower infection rates, and cost-effectiveness were advantages listed by 58.5% of surgeons. Patient’s medical history (75.8%), followed by ASC resources and capabilities (61%) and surgeon preference (61%), were relevant factors. Higher efficiencies at ASCs (14.6%), contractual issues (9.8%), and ownership issues (7.3%) were less relevant to surgeons. About 65.9% of surgeons reported lower reimbursement in ASCs, and 43.9% said it was an implementation hurdle. Lower direct costs were reported by 53.7% of surgeons. Other hurdles included a lack of trained staff (24.4%), inadequate staffing (22.0%), cost overruns (26.8%), high Joint Commission or the Accreditation Association for Ambulatory Health Care credentialing costs, and surgeons feeling uncomfortable performing TLIF in ASCs (22.0%). Only 17.1% listed medical problems as a reason their patient was considered unsuitable for the ASC environment. A majority (53.7%) stated that their ASCs complied with strict Stark requirements by disclosing physician ownership interests. However, 22% of surgeons reported self-referrals under the “In-Office Ancillary Services Exception” allowed by the Stark law.
Conclusion Our survey data show that surgeons’ perceptions of current CMS rules and regulations may hinder the transition into the ASC setting because they think the reimbursement is too low and the regulatory burden is too high. ASCs have disproportionally higher initial acquisition and ongoing costs related to staff training and maintenance of the TLIF technology that CMS should consider when determining the appropriate financial remuneration for these complex procedures.
Clinical Relevance ASC offers a viable and attractive option for their TLIF procedure with the advantage of same-day discharge and at-home recovery.
Level of Evidence 3.
INTRODUCTION
In response to the COVID-19 pandemic, the Centers for Medicare and Medicaid Services (CMS) introduced the Hospitals Without Walls (HWW) program in March 2020. This program granted hospitals regulatory flexibility to offer services and procedures in nontraditional locations, including ambulatory surgical centers (ASCs), while still receiving Medicare payments. This unprecedented situation provided a unique opportunity to evaluate the safety and effectiveness of minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) in ASCs for Medicare beneficiaries. However, despite the potential benefits, the implementation of TLIF in ASCs has faced certain hurdles,1 prompting the question of whether there are medical or infrastructure-related challenges beyond reimbursement concerns.
While recent evidence suggests that MIS-TLIF procedures yield comparable 2-year clinical outcomes to open TLIF surgeries and offer superior cost-effectiveness, relatively few surgeons currently perform these procedures in ASCs.2–4 The advantages of minimally invasive spine surgery, such as reduced blood loss, decreased postoperative pain, lower infection risk, decreased reliance on pain medication, and faster return to daily activities, align well with the advantages of performing the operation in ASCs.4 The clinical benefits and procedural efficiencies of performing minimally invasive fusion procedures such as TLIF in the ASC setting are becoming increasingly well established, suggesting a growing recognition of the viability and effectiveness of ASCs for these types of surgical procedures.5 Comparative studies evaluated differences in perioperative baseline characteristics, operative efficiency, and 30-day safety events for patients undergoing MIS-TLIF in a hospital vs an ASC and highlighted similar safety profiles and clinical outcomes in ASC compared with traditional hospital settings.6–9 There is also a growing acceptance of performing MIS-TLIF in ASCs, indicating a shift in surgical practices toward more cost-effective and patient-friendly environments. This trend is partly facilitated by certain technological advancements, such as navigation and robotics, which facilitate MIS-TLIF in outpatient settings.10
Patients generally tend to have higher satisfaction rates in ASCs due to the overall better experience attributed to streamlined workflows, improved efficiency with reduced waiting times, the perceived cost advantage resulting from limited preoperative testing that is often required at hospitals, and concentrated access to specialized expertise.4 Furthermore, ASCs are designed to provide outpatient care with a more personalized and patient-centered approach, allowing patients to undergo TLIF surgery and return home on the same day.
In this survey study, the authors aimed to better understand surgeons’ perspectives as the ultimate decision-makers in determining where to perform TLIF on elderly patients—whether in an ASC or a hospital setting. The study explored factors that drive surgeons’ decisions, including reimbursement adequacy, regulatory and legal considerations, and medical reasons. By examining these factors, the authors sought to provide insights into the decision-making process surrounding TLIF procedures in the elderly population in an ASC vs hospital setting.
METHODS
The authors conducted an online survey to gather information from prospective respondent surgeons regarding their utilization of ASCs for performing TLIF surgeries on elderly patients. The survey, hosted on www.typeform.com, was distributed to 235 surgeons through email, social network chat groups, and messenger apps like WhatsApp. The surgeons were presented with multiple-choice questions covering various aspects of TLIF practice preferences, including surgical indications, decision factors for choosing ASCs over hospitals, implementation hurdles, reimbursement concerns, staffing issues, and the impact of CMS rules and regulations on TLIF in ASCs, particularly concerning physician ownership and self-referral conflicts governed by the Stark law.
The survey questions were designed by a team of authors with expertise in CMS rules and regulations related to TLIF in ASCs. The survey questions were meticulously crafted based on a literature review and expert consultations among the authors, many of whom are experts in the ASC environment. This process ensured that the questions were relevant, clear, and capable of eliciting the desired information. Additionally, the questions were reviewed and refined in consultation with reimbursement experts, enhancing their validity in the context of our study. Before the launch of the main study, a pilot test was conducted with a smaller subset of the target population. The feedback obtained was instrumental in making necessary adjustments to the survey’s wording and structure, improving its clarity and reducing potential biases. While a formal validation process was not conducted, survey research shows that the survey data do not come in at random.11–15 The authors, therefore, consider our survey results sufficiently reliable for our research purposes. The authors applied this methodology in multiple survey studies.16–24
The survey was conducted from 30 May 2023 to 28 June 2023, ensuring that the authors remained blinded to the identity of the responding surgeons. Once the survey concluded, the responses were downloaded in an Excel file format and imported into IBM SPSS (version 27) statistical software for further analysis. Descriptive statistics were calculated, including response counts, mean values, ranges, SDs, and percentages. Additionally, χ 2 statistics were used to assess the strength of associations between factors. Missing answers were included in percentage calculations and indicated at the top of each data table. A significance level of 0.05 or less (P ≤ 0.05) was considered statistically significant, and a confidence interval of 95% was employed for all statistical tests.
RESULTS
Response Rate
Two hundred thirty-five spine surgeons accessed the online survey on the typeform.com website. Forty-one submitted a valid survey at a completion rate of 25.8% (Figure 1). The average time to complete the online survey was 5 minutes and 54 seconds.

Two hundred thirty-five spine surgeons accessed the online survey; 41 submitted a valid survey at a completion rate of 25.8%.
Surgical Indication and Technique
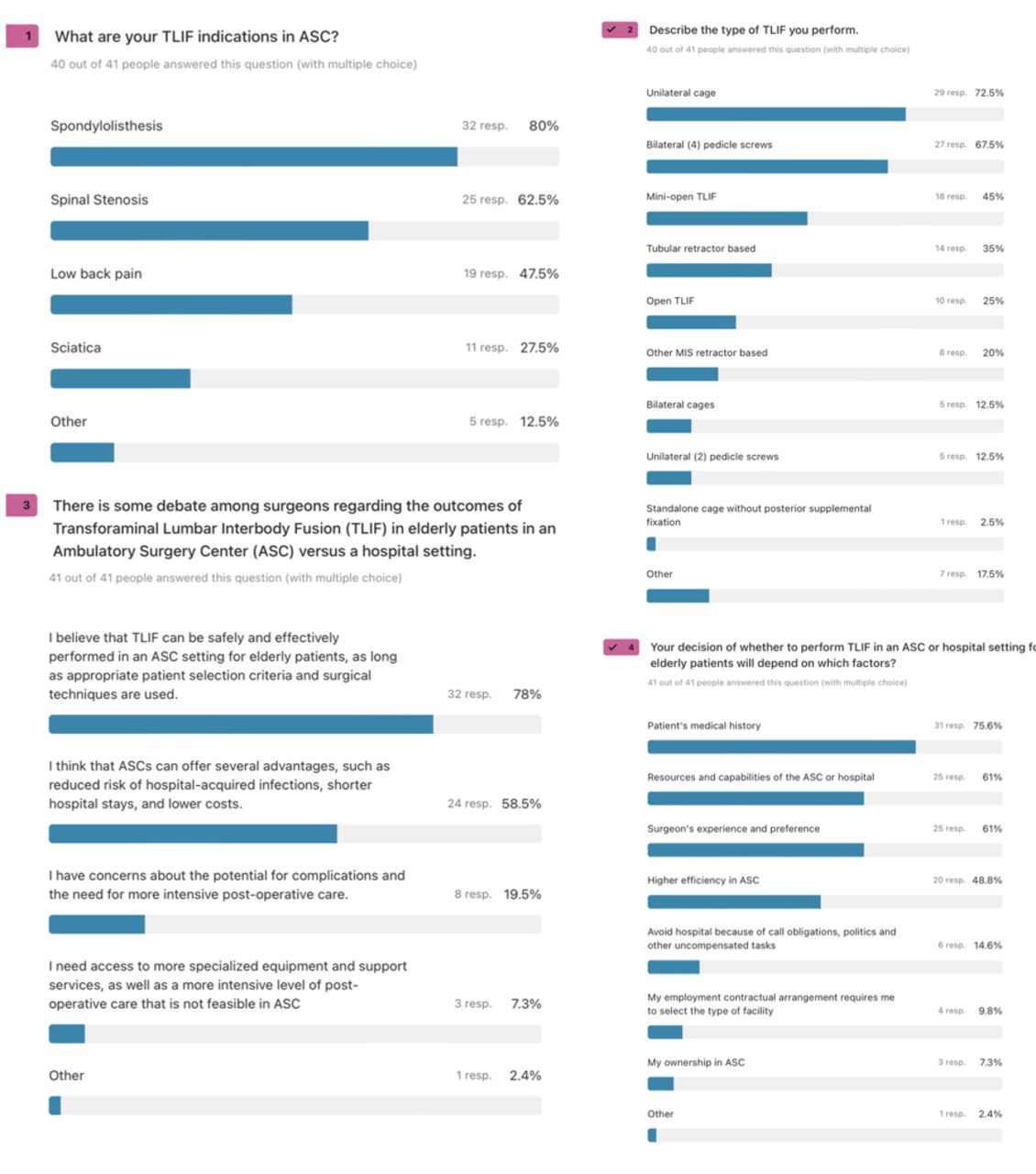
The most common surgical indications for TLIF in ASCs were spondylolisthesis (80%), spinal stenosis (62.5%), and low back pain (47.5%; Figure 2). The preferred surgical approach involved unilateral cages (72.5%) and bilateral pedicle screws (67.5%). Only a small percentage of surgeons (12.5%) used bilateral TLIF cages, while another 12.5% stabilized the spine using a unilateral pedicle screw construct. Among the surgical techniques used, the mini-open approach was favored by 45% of surgeons, followed by tubular retractor (35%), open TLIF (25%), and other minimally invasive retractor-based (20%) surgeries.

Respondents indicated that the most common surgical indication for transforaminal lumbar interbody fusion (TLIF) in ambulatory surgical centers (ASC) was spondylolisthesis (80%), spinal stenosis (62.5%), and low back pain (47.5%). Unilateral cages (72.5%) with bilateral (4) pedicle screws (67.5%) were preferred by most surgeons. Only 12.5% of surgeons placed 2 (bilateral) TLIF cages, and another 12.5% stabilized the spine with a unilateral pedicle screw construct. The mini-open approach was used by 45% of surgeons, followed by tubular retractor (35%), open TLIF (25%), and other minimally invasive retractor-based (20%) surgeries. Most surgeons (78%) believed TLIF could be done safely in an ASC in appropriately selected patients, and 58.5% indicated that ASC is attractive because of streamlined workflow, lower infection rates, and cost. Only 19% of surgeons were worried about having complications in an ASC. When booking a patient for TLIF in an ASC vs hospital, 75.8% of surgeons indicated the patient’s medical history being the most relevant factor, followed by ASC resources and capabilities (61%) and surgeon preference (61%).], higher efficiencies at an ASC (14.6%), contractural issues (9.8%), or ownership issues (7.3%).
Perceived ASC Advantages
Most surgeons (78%) believed TLIF could be safely performed in ASCs when appropriate patient selection criteria were met. Additionally, 58.5% of surgeons found ASCs attractive due to their streamlined workflow, lower infection rates, and cost-effectiveness. Only 19% of surgeons expressed concerns about complications in an ASC setting. When considering whether to book a patient for TLIF in an ASC or a hospital, surgeons identified the patient’s medical history as the most relevant factor (75.8%), followed by ASC resources and capabilities (61%) and surgeon preference (61%). Factors such as higher efficiencies at ASCs (14.6%), contractual issues (9.8%), and ownership issues (7.3%) were also considered.
Reimbursement
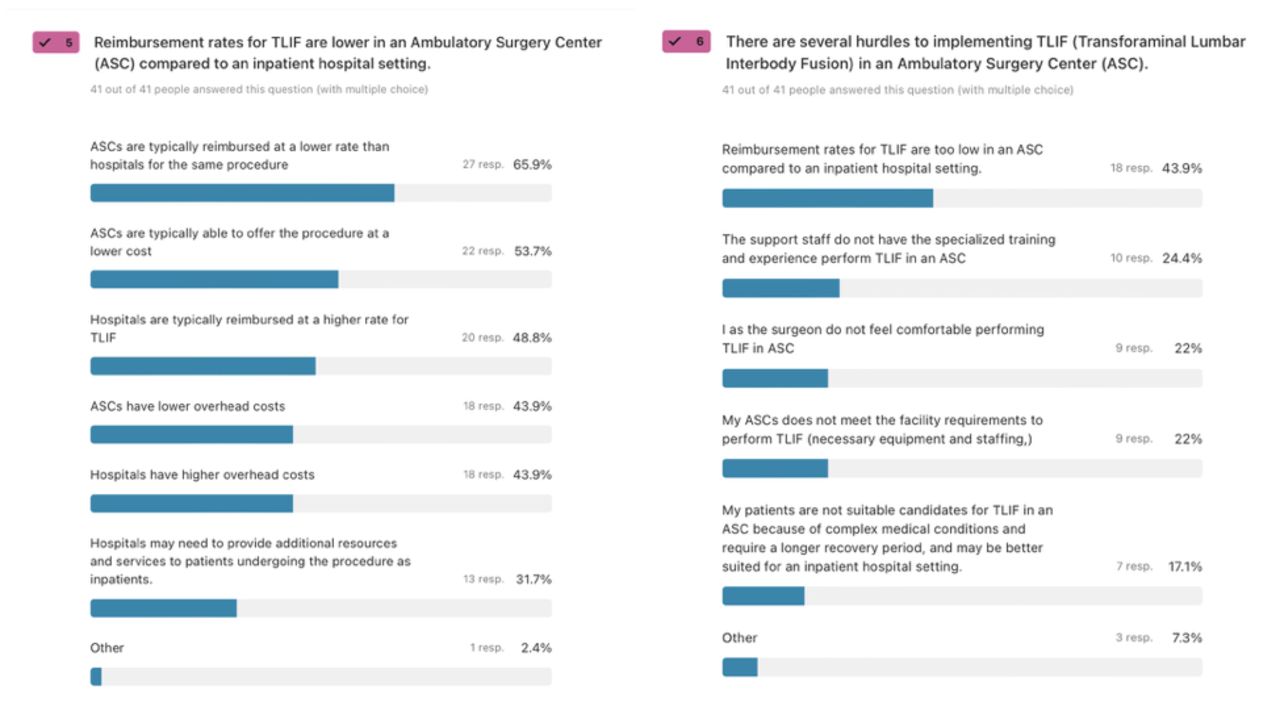
Regarding reimbursement, 65.9% of surgeons believed that ASCs were reimbursed at a lower rate, while 48.8% believed hospitals received higher payments for TLIF procedures (Figure 3). More than half of the surgeons (53.7%) believed that ASCs could provide surgical services at a lower cost due to lower overhead expenses (43.9%). In contrast, hospitals were seen as having higher costs due to the provision of additional services. Among the challenges associated with TLIF implementation in ASCs, 43.9% of surgeons identified low reimbursement as a barrier, while 24.4% noted the need for more trained support staff. Additionally, 22% of surgeons expressed discomfort with performing TLIF in ASCs, and another 22% considered the ASC staffing inadequate. Only 17.1% of respondents believed TLIF patients with complex underlying medical problems were unsuitable for the ASC environment.
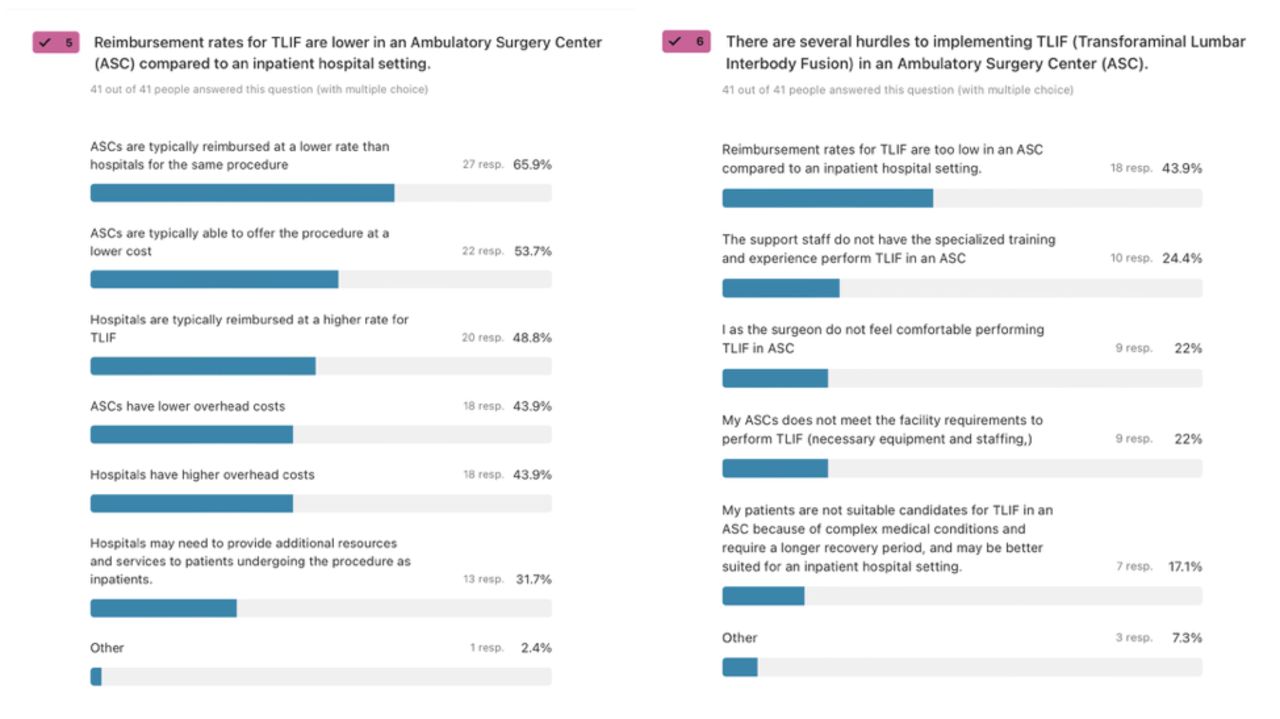
Most respondents (65.9%) believed that ambulatory surgical centers (ASCs) were reimbursed at a lower rate, and 48.8% thought hospitals get paid at a higher rate for transforaminal lumbar interbody fusion (TLIF). More than half of surgeons (53.7%) thought that ASC could provide surgical services at a lower cost because of lower overhead (43.9%). Hospitals were believed to have higher costs because they must provide additional services. When asked about TLIF implementation hurdles in an ASC, 43.9% of surgeons believed the reimbursement was too low, 24.4% needed more trained support staff, 22% were uncomfortable performing TLIF in an ASC, and 22% considered the ASC staffing inadequate. Only 17.1% of responding surgeons thought that their TLIF patients were not a good fit for the ASC environment because of the complexity of their underlying medical problems.
Implementation Hurdles
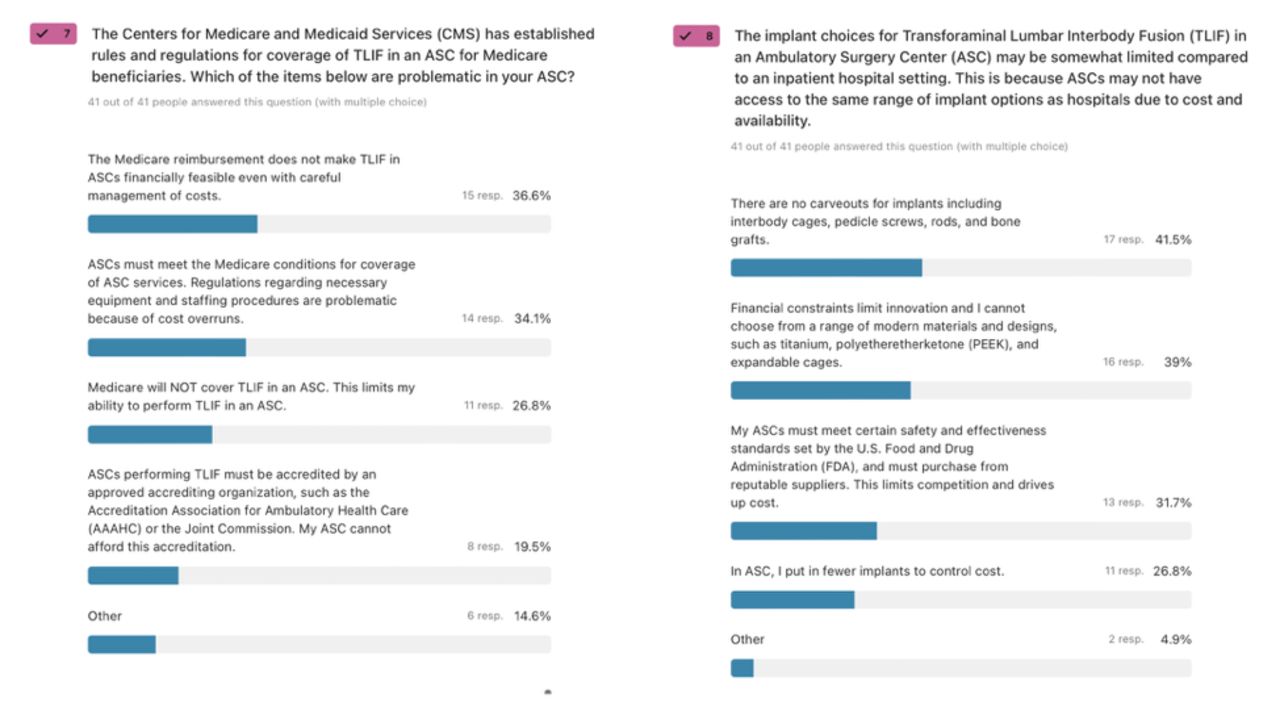
Respondents had varied opinions when asked about the rules for TLIF coverage in ASCs established by the CMS (Figure 4). Around 36.6% of surgeons did not believe that CMS reimbursement was sufficient to perform TLIF in ASCs, even with careful cost management. Similarly, 34.1% of surgeons felt the CMS-mandated staffing and equipment requirements resulted in cost overruns. A smaller group reported that their local CMS administrator did not cover TLIF in ASCs (26.8%), and 19.5% felt that the credentialing costs through organizations like the Joint Commission or the Accreditation Association for Ambulatory Health Care were too high.

Among the survey respondents, 36.6% of respondents did not think that Centers for Medicare and Medicaid Services (CMS) reimbursement was adequate to perform transforaminal lumbar interbody fusion (TLIF) in ambulatory surgical centers (ASCs) even with careful cost management; 34.1% opined that the CMS-mandated staffing and equipment requirements were creating cost-overruns. A smaller group of surgeons (26.8%) reported that their local CMS administrator does not cover TLIF in ASC, and another 19.5% indicated that the credentialing cost through the Joint Commission or the Accreditation Association for Ambulatory Health Care was too high.
Compliance Issues
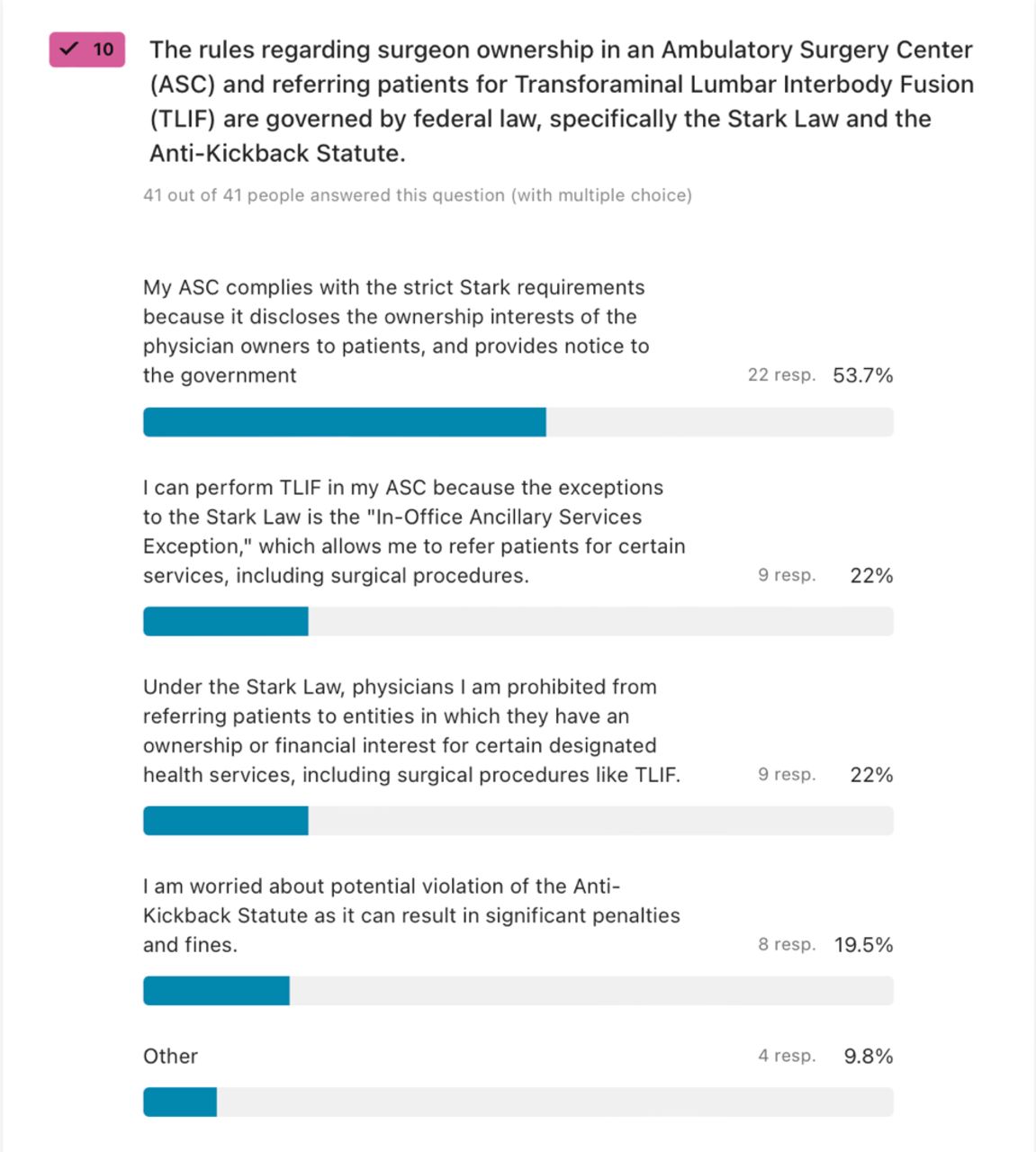
Responding surgeons expressed relatively less concern regarding compliance with Stark Law and Anti-Kickback statutes (Figure 5). A majority (53.7%) stated that their ASCs complied with strict Stark requirements by disclosing ownership interests of physician owners to patients and providing notice to the government. However, 22% of surgeons reported self-referrals under the “In-Office Ancillary Services Exception” allowed by the Stark law. At the same time, an equal percentage acknowledged that they were prohibited from referring patients to entities in which they held an interest. Furthermore, 19.5% of surgeons worried about potential Stark violations and the associated penalties and fines.

Compliance with Stark Law and Anti-Kickback statutes was a lesser concern to responding spine surgeons. The majority (53.7%) indicated that their ambulatory surgical center complies with strict Stark requirements because it discloses ownership interests of the physician owners to patients and provides notice to the government. Self-referrals under the “In-Office Ancillary Services Exception” were reported by 22% of surgeons. However, the same percentage of surgeons indicated that under the Stark law, they were prohibited from referring patients to entities they were interested in. Another 19.5% were worried about potential Stark violations and the potential for significant penalties and fines.
DISCUSSION
Before the implementation of CMS’s HWW program, fusion procedures such as MIS-TLIF performed in ASCs were limited to commercially insured patients, while Medicare beneficiaries were restricted to undergoing these procedures in traditional hospital settings. This situation created a catch-22 situation in which CMS required evidence of procedural safety in the Medicare population to expand the list of ASC-payable services to include TLIF procedures.25 Still, Medicare did not reimburse for ASC surgeries, making it challenging to gather the necessary data regarding older patients. The HWW initiative resolved this dilemma and facilitated the comparison of intraoperative variables and short-term safety outcomes between Medicare-age patients treated in ASCs and those treated in hospitals.
Surgeon survey data showed that the primary indication for TLIF was spinal stenosis and instability-related problems. Most (78%) believed TLIF could be safely performed in ASCs, taking advantage of the streamlined workflow, lower infection rates, and cost-effectiveness, generally resulting in higher patient satisfaction. When considering whether to book a patient for TLIF in an ASC or a hospital, surgeons were more concerned with medical comorbidities than with handling complications in the ASC setting, highlighting the importance of appropriate patient selection. Contractual or ownership issues were the lowest priority when selecting the place of service. Only 7.3% of surgeons indicated that their ownership of an ASC influenced their decision regarding where to perform the TLIF.
Implementation hurdles caused by insufficient reimbursement were the number one perceived concern of responding surgeons (65.9%). Surgeons (53.7%) believed that ASCs could provide surgical services at a lower cost due to lower overhead expenses (43.9%). A recent report by Shahi et al highlighted the procedural and cost inefficiencies of performing MIS-TLIF procedures in hospitals.26 Among 71 eligible patients, only 4% were discharged on the same day their surgeries were conducted in hospitals. The median length of stay was 27 hours, similar to the current study’s findings for in-hospital patients (approximately 24 hours). Delayed physical therapy evaluation and clearance were among the factors contributing to discharge delays in the hospital setting. The authors concluded these patients could have been managed more efficiently in ASCs without surgical technique or protocol modifications.
Implementation hurdles inherent to ASCs include a lack of trained staff, which was noted by 24.4%. Some 34% of surgeons believed the CMS-mandated staffing and equipment requirements resulted in cost overruns in part (19.5%) due to the added cost of the Joint Commission or the Association for Ambulatory Health Care Accreditation. Noncoverage by their local CMS administrator was reported by 26.8% of responding surgeons. Violating Anti-Kickback statutes was less of a concern as the majority (53.7%) stated that their ASCs complied with Stark requirements by disclosing ownership interests of physician owners to patients and providing notice to the government. Another 22% of surgeons reported self-referrals under the “In-Office Ancillary Services Exception” as allowed by the Stark law. Contractual obligations with their employer (22%) and perceived risk of Stark violations (19%) were also reported. Updated policy statements by professional surgeon societies should highlight the shifting trends in CMS regulations and reimbursement rulings to improve surgeons’ knowledge and patients’ access to the ASC setting for more complex spinal surgeries such as TLIF.
The present study was limited by low power dictating descriptive statistics. The survey’s primary objective was to gather exploratory insights and qualitative trends rather than perform quantitative hypothesis testing. Calculating percentages was an appropriate method to present data clearly and intuitively, facilitating an understanding of the distribution of responses among the surveyed surgeons. This approach is particularly relevant in surveys where the intent is to capture attitudes, opinions, or practices, which are inherently qualitative. The survey was designed to provide preliminary insights and not to establish broad generalizations. With 45 of 238 responding surgeons submitting a completed survey, our opinion research successfully captured diverse perspectives, ensuring that a breadth of experiences and opinions of the limited number of surgeons presently performing MIS-TLIF in ASCs were represented. While a larger sample size might offer more generalizable data, the responses received from these 45 surgeons provide a focused snapshot of opinions and practices in this specific field. The survey’s findings should be considered current benchmark numbers for further research rather than conclusive evidence. Our exploratory survey identified surgeon perceptions that allowed us to articulate hypotheses that can be tested on a larger scale in subsequent research when more surgeons perform MIS-TLIF in ASCs. Therefore, despite the limitations in sample size, the survey’s results offer meaningful insights and contribute to the ongoing dialog in this area of surgical practice and may facilitate future research.
CONCLUSIONS
While advancements in techniques, technologies, and efficiencies have enabled complex spinal procedures like TLIF to be performed safely in ASCs, the surgical intensity has increased. Current minimally invasive approaches, utilizing small access portals, require precise microscopic techniques and real-time fluoroscopic guidance for instrumentation. While the procedure may be more efficiently executed in ASCs, it is not inherently safer or less challenging. The risks, such as neurological injury and technical demands of the procedure, remain, albeit performed in a shorter timeframe. Surgical teams must still be prepared to handle common intraoperative complications such as dural tears, implants, instrumentation failure, or bleeding-related problems. Consequently, ASCs have disproportionally higher initial acquisition and ongoing costs related to staff training and maintenance of the TLIF technology that CMS should consider when determining the appropriate financial remuneration for these complex procedures. Our survey data show that surgeons’ perceptions of current CMS rules and regulations may hinder the transition into the ASC setting as they believe the reimbursement is too low and the regulatory burden is too high.
Footnotes
↵† Kai-Uwe Lewandrowski and Abduljabbar Alhammoud are joint first authors.
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests This manuscript is not intended to endorse any products or push any agenda other than the associated clinical outcomes with TLIF spine surgery in ASC or hospital settings. None of the authors received anything of value in return for this publication. None of the authors are paid consultants of Wenzel Spine.
IRB approval This study was approved through a central IRB (Pearl IRB, Indianapolis, USA)
Disclaimer The views expressed in this article represent those of the authors and no other entity or organization. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.