


Abstract
Background Approximately 38,000 scoliosis surgery correction operations are performed annually in the United States; these operations are associated with considerable postoperative pain which can be difficult to manage. This is largely attributed to an incision spanning multiple vertebral segments with paraspinal muscle dissection and retraction to facilitate the implantation of segmental hardware and rods. Frequently utilized analgesic modalities include intravenous patient-controlled analgesia and epidural analgesia, often in combination. We sought to ascertain the feasibility and analgesic efficacy of continuous thoracolumbar dorsal ramus nerve (TDRN) block using surgically placed multiorifice catheters.
Methods Forty-two patients diagnosed with idiopathic scoliosis who underwent a posterior spinal fusion (PSF) were enrolled after consent was obtained. Patients were managed utilizing a standardized Enhanced Recovery After Surgery) protocol including a perioperative opioid-sparing regimen. Data were collected at specified time intervals during the recovery period. These data points included pain scores using the Numeric Rating Scale. Parenteral or both oral and parenteral opioid consumption doses were also collected every 4 hours. Any significant postoperative adverse events were recorded as well.
Results A total of 42 patients had surgically placed TDRN catheters, and 40 patients were included in this study. The patients all reported low to moderate pain scores with low opioid consumption postoperatively, while the TDRN catheter delivery of local anesthetic analgesics did not result in significant complications.
Clinical Relevance A regional technique utilizing TDRN catheters could be a valuable component of the postoperative pain management protocols for PSF surgery, and additional studies are warranted.
Conclusion This study evaluated the feasibility and analgesic efficacy of TDRN catheters for postoperative pain control following multilevel PSF for idiopathic scoliosis. Continuous local anesthetic delivery through TDRN catheters is a feasible and safe technique for postoperative pain control in these patients. Selective blockade of the dorsal rami might have benefits over epidural analgesia or other regional techniques.
Level of Evidence 3.
- Adolescent idiopathic scoliosis
- posterior spinal fusion surgery
- postoperative pain management
- thoracolumbar dorsal ramus nerve (TDRN) block
- multi-orifice catheter
- Enhanced Recovery After Surgery
Introduction
Posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) is aimed at preventing spinal curve progression, restoring spinal balance, and improving quality of life.1 Patients are deemed surgical candidates when their Cobb angle, the measure of the lateral curvature of the spine, is greater than 45 degrees.2 Corrective surgery for AIS is invasive, warranting a large linear incision over multiple spinal segments, the dissection of overlying erector spinae muscles, and the disruption of soft tissue and ligaments for hardware placement.3 Incisions can span 12 or more vertebral segments.4 Postoperative pain is one of the most concerning issues for patients and their caregivers, while inadequate treatment with an opioid-sparing regimen can lead to poor mobility after surgery. Conversely, overreliance on opioids can result in undesirable side effects and an increased length of stay.5
The traditional methods of postoperative management of pain include opioids (oral, intravenous, and intrathecal), acetaminophen, and anti-inflammatory drugs. Historically, opioids have been the mainstay of a postoperative pain management regimen, and only in recent years have we seen the introduction of regional techniques such as thoracic epidural,6 erector spinae plane block,7 and local wound infiltration.8 Over the past decade, there has been a growing trend to use more regional techniques as valuable contributing components of the analgesic regimen for spine surgeries.9 Largly due to the implementation of Enhanced Recovery After Surgery (ERAS) protocols, there is an emphasis on multimodal analgesic techniques in an effort to minimize opioid consumption and maximize patient satisfaction.10,11 Parenteral opioids come with significant side effects including sedation, respiratory depression, nausea, vomiting, and slowing of bowel function, including ileus.6 ERAS protocols in general, and those specifically designed for idiopathic scoliosis correction, promote evidence-based modalities to refine pain management while reducing potential surgical stress response.12,13 Interfascial regional anesthetic techniques, such as erector spinae plane block, thoracolumbar interfascial plane block, and quadratus lumborum block, have fewer side effects and carry less risk than epidural analgesia and have been studied and described as acceptable options to help alleviate postoperative pain associated with PSF.1
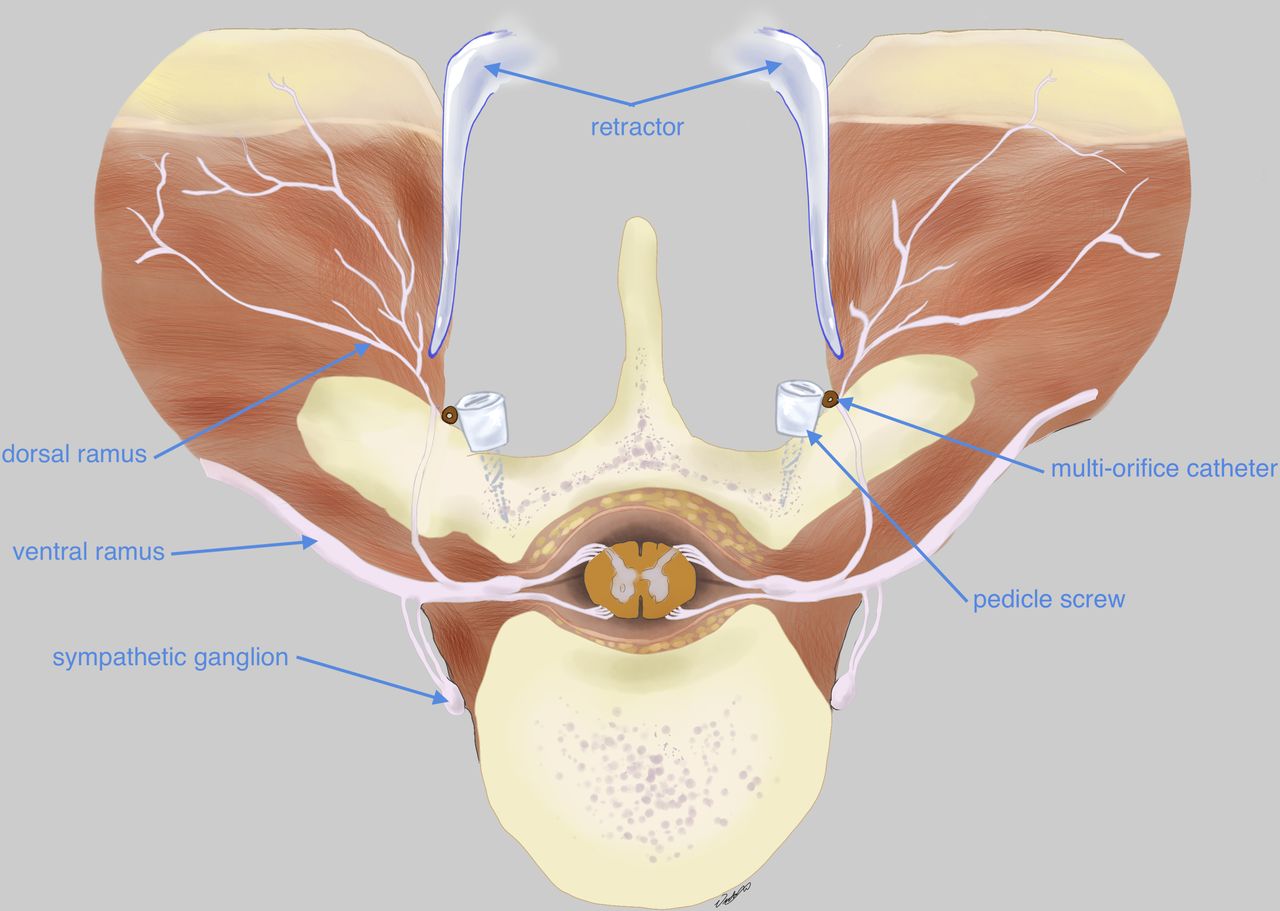
The main goal of our study was to investigate the feasibility, safety, and analgesic efficacy of surgically placed thoracolumbar dorsal ramus nerve (TDRN) catheters as a selective regional technique, targeting the dorsal sensory distribution of the spinal nerves. The dorsal ramus nerve is the posterior division of a spinal nerve, which provides motor innervation to the deep muscles of the back and sensory innervation to the skin of the back.14,15 By selectively blocking the dorsal rami of spinal nerves, a desirable, isolated somatic analgesic effect can be achieved in the back region. Of note, this technique should prevent side effects of neuraxial blockade such as urinary retention, hypotension, or decreased leg muscle strength. The TDRN catheters are placed under direct visualization in the surgical field lateral to the implanted pedicle screws and target analgesia of the area surrounding the root of the dorsal ramus nerve, which is located directly outside the intervertebral foramen and deep to the erector spinae musculature. Last, regional nerve blockade can reduce neurological inflammation through the reduction of cytokine production and aid in the prevention of a hyperalgesic state.16 Analgesia delivered via the TDRN catheter system may thus carry this additional advantage, although the exact mechanisms of the phenomenon are not well understood.16
Methods
This was a prospective, observational single-center study of 42 patients who had intraoperative placement of TDRN catheters for postoperative pain after spinal fusion for scoliosis surgery. This study was approved by the New York Medical College Institutional Review Board (Protocol Number 12672). Pediatric patients with AIS scheduled to have a PSF were enrolled with written consent from parent/guardian and patient assent. Patients receiving daily pain medications including chronic opioids or acetaminophen were excluded from the study. Patients who would have difficulty communicating a pain score, such as severely syndromic or intellectually challenged children, were also excluded. The mean age of the studied cohort of patients was 14.4 years with a range of 10 to 17 years.
ERAS protocol for pediatric PSF surgery was employed for all the study patients. Under this protocol, patients received an actual weight-based dose of oral acetaminophen of 15 mg/kg (maximum 1000 mg) and gabapentin of 15 mg/kg (maximum 600 mg) within the hour prior to surgery. Total intravenous anesthesia (propofol and remifentanil) was utilized to facilitate intraoperative neuromonitoring, including somatosensory evoked potentials, transcranial motor evoked potentials, and electromyography monitoring. At the end of the surgical correction and before wound closure, the surgeon placed 4 multiorifice catheters under direct visualization. Two catheters per side are placed in parallel fashion lateral to the newly implanted pedicle screw hardware near the dorsal ramus nerve root in order to cover the entire length of the surgical wound, with a catheter length overlap by a few centimeters to ensure uniform spread of the local anesthetic infusion along the fused segments (Figure 1). The catheters were named according to their placement, as follows: left upper catheter, left lower catheter, right upper catheter, and right lower catheter (Figure 2). On each side, catheters were tunneled out, secured externally with clear, occlusive, and sterile adhesive dressings near the posterior hip area, and attached to a splitter that connects to 1 common catheter at each side. Each single-catheter infusion was connected to a rate-adjustable flow device delivering 0.2% ropivacaine at a dose of 0.4 mg/kg/h. We used the Ambu ACTion BlockPump (Ambu Inc., Columbia, MD), a portable, rate-adjustable, disposable elastomeric pump. The pumps were primed, and all catheter and pump connections were performed under sterile conditions in the operating room. Aside from the weight-based preset continuous infusion rate, there was also an option to set additional ropivacaine dosage through a patient-administered bolus function, which has a lockout interval set for 1 hour. A patient-controlled analgesia (PCA) pump with intravenous hydromorphone was offered for breakthrough pain at a bolus dose of 0.004 mg/kg with a 20-minute lockout in addition to scheduled and staggered doses of acetaminophen and nonsteroidal anti-inflammatory drugs as part of the standard protocol order set.

Intraoperative placement of thoracolumbar dorsal ramus nerve catheter within the anatomy of the back. Published with permission from the International Journal of Spine Surgery.17

Thoracolumbar dorsal ramus nerve catheters in place prior to surgical closure. Published with permission from the International Journal of Spine Surgery.17
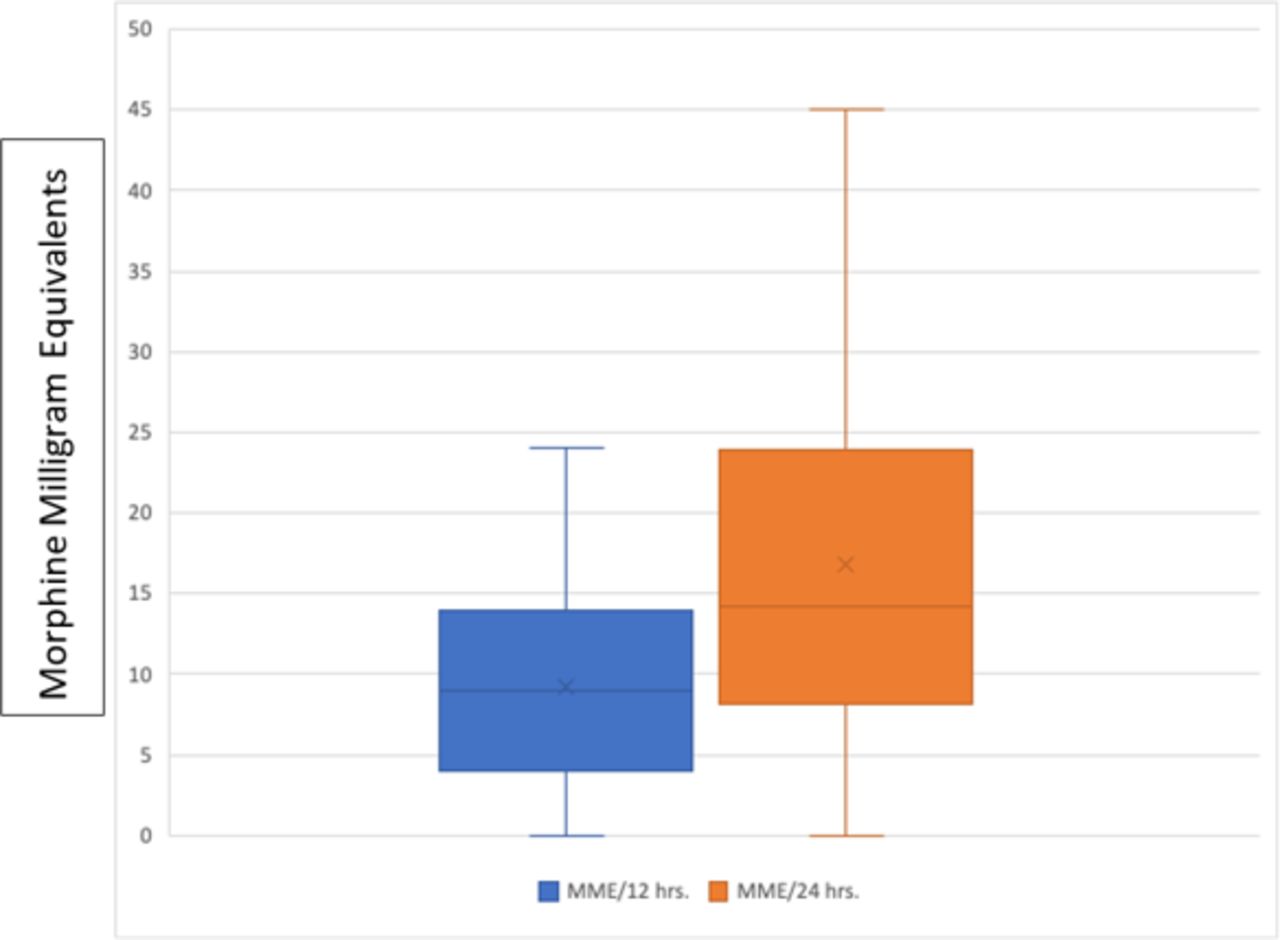
The patients were followed each day by the acute pain service and assessed for levels of pain and side effects, such as infection, catheter malfunction, hematoma, neurological damage/deficits, Horner’s syndrome, etc. The catheters were removed 48 hours postoperatively by the surgical team. The indwelling urinary and arterial line catheters were discontinued on postoperative day (POD) 0 or 1. The Numeric Rating Scale (NRS) was used by the nursing team to assess pain level at the postoperative hours 0, 0.5, 4, 8, 12, 16, 20, and 24. Opioid consumption was assessed by tallying the total amount of opioid medication, both oral and parenteral, at 12 and 24 hours after surgery and was converted to morphine milligram equivalents (MME). These 2 time points were chosen for analysis in order to best reflect cumulative opioid consumption in the setting of the regional blockade and their associated pain scores. Patients were seen within 2 weeks of surgery for an outpatient postoperative visit by the orthopedic surgeon, at which time they were assessed for ongoing analgesic needs and any postoperative sequelae.
Results
The study enrolled 42 patients with the diagnosis of AIS over 36 months. PSF surgery was performed by 1 surgeon. One patient had revision surgery for hardware failure. Two patients were excluded from the study: one due to catheter dislodgment on POD 0, and the second was excluded because of incomplete data collection. Ultimately, 40 patients were included in the data analysis. Demographic data, Cobb angle measurements, mean opioid doses, and mean pain scores at 12 and 24 hours are presented in Table 1. One of 40 patients experienced a pump leak on POD 1, which necessitated an immediate device replacement. This patient remained in the study analysis because the interruption was so brief and did not disrupt therapy or prevent us from collecting data. After discussion with the product manufacturers, the technical issues were addressed, and the anesthesia, nursing, and surgical teams were re-educated. Subsequently, for the remainder of the study, we encountered no further pump leakage or catheter dislodgment. None of the catheters had to be removed for any complications such as local anesthetic systemic toxicity, hypotension, surgical/catheter site infections, paresthesia, or poor motor function. Patients tolerated the TDRN catheters well and experienced low to moderateNRS pain scores (Figure 3). Opioid consumption was recorded and converted to MMEs within a 0- to 12-hour and 13- to 24-hour period as represented in Figure 4. Patients also resumed regular diet and engaged in physical therapy on POD 1. None of the patients had any postoperative side effects from the catheters at their 2-week follow-up visit. Routine follow-up postsurgical visits scheduled at 2 weeks, 3 months, 6 months, 1 year, and 2 years were reviewed. Six of the patients had not yet completed the 2-year mark, but their preceding visits were included in the evaluation. The following surgical complications were observed: 2 patients presented with asymptomatic pseudarthrosis, and 2 patients reported chronic postoperative pain issues. Among them, a 15-year-old girl was referred to rheumatology for suspected fibromyalgia 6 months after surgery, while another patient was referred to rheumatology due to persistent shoulder pain. One patient was lost to follow-up. No infectious complications were recorded in our patient cohort.

Box and whisker plot representing numeric rating scale pain scores at 0–12 and 13–24 hours postoperatively.

Opioid consumption represented in mean morphine milligram equivalents at 0–12- and 13–24-hour periods.
Patient demographic and basic clinical characteristics (N = 40).
Discussion
Patients who undergo PSF experience a challenging postoperative recovery in terms of the effectiveness of pain management.4 The nature of the surgery involves a large incision with extensive trauma to the surrounding muscles and tissues followed by the implantation of metal hardware into the bones in order to correct the spinal deformity.9 The application of a regional technique in addition to a multimodal pain regimen as utilized by ERAS protocols can help to improve outcomes.18 ERAS protocols, while not new, are still relatively uncommon in spine surgery.18 In this study, we demonstrate that the use of a TDRN catheter system is a feasible and effective strategy to help manage pain following PSF in adolescents undergoing scoliosis surgery. Continuous regional anesthetic techniques, such as epidural and local wound infiltration catheters, have been reported with demonstrated efficacy for both scoliosis and other types of spine surgery.6–8 TDRN catheters have several distinct advantages over other regional techniques. They are placed under direct visualization, facilitating a direct target for the local anesthetic to block sensory and motor innervation of the paraspinal muscles and soft tissue involved, sparing the blockade of ventral rami, thus potentially optimizing the efficacy of the modality. The use of the parallel, double catheter system ensures the ability to deliver local anesthesia throughout the span of fused vertebral segments, as discussed in a technical report.17 The specific use of a multiorifice catheter is thought to help distribute the local anesthetic more evenly over the adjacent dorsal rami of the spinal nerves, resulting in improved block characteristics.17 TDRN block has been reported to be an effective pain option after adult spine procedures in opioid-tolerant patients as well.19,20 The use of TDRN catheters can help reduce opioid requirements, preserve respiratory function, prevent hypotension as well as urinary retention, potentially decrease the surgical stress response, and reduce the inflammatory response.21
Our study is limited by the absence of our own control data. For comparison purposes, we reviewed studies with similar-sized samples with data from PSF patients who received PCA therapy. We noted that our TDRN catheter patients exhibited comparatively lower opioid usage in the first 24 hours after PSF. Four studies reported PCA cumulative dosage in historical controls prior to the initiation of alternative pain management modalities after PSF. Compared with 16.8 mg/24 h in our study, the 2016 study of Thomson et al22 showed a mean MME of 42.3 mg/24 h. In a 2017 study,23 the total mean PCA dose was reported as 35.8 mg/24 h MME. Another study in 201724 also reported a mean MME of 51 mg/24 h. In a 2019 study,25 PCA usage was reported as 0.703 MME/kg/24 h, while in our study, MME was 0.25 MME/kg/24 h (see Table 2). The patient demographic data in all 4 studies are similar and typical for adolescents undergoing PSF for AIS.
Since the completion of our study, we have continued to utilize TDRN catheters for our scoliosis surgical patients. As a result of their improved pain control and safety profile of continuous TDRN block technique, patients are no longer admitted to the intensive care unit and recover on the general pediatric nursing floor. Additionally, we no longer prescribe opioid PCA therapy in the immediate postoperative period, relying on intermittent bolus doses of opioids for breakthrough pain. While this study exclusively evaluated AIS patients. we have found the technique to be particularly beneficial for neuromuscular scoliosis patients, many of whom are nonverbal. Avoiding excess sedation and its side effects in a population that cannot effectively communicate is essential. While larger studies are needed, this study is promising in that it demonstrates that TDRN catheters are useful modality in the management of postoperative pain after PSF surgery for AIS.
Summary of similar studies comparing opioid consumption in scoliosis surgery.
Conclusion
In this study, we sought to assess the value of a selective, continuous regional anesthetic technique in the management of acute postoperative pain for PSF surgery. In AIS patients, a TDRN catheter appears to be a safe, feasible, and effective analgesic complement to a postoperative pain management protocol for PSF. This regional technique produces opioid-sparing effects. Further studies, including appropriately powered randomized controlled trials, are needed to recommend the use of dorsal rami blockade as a standard treatment option in adolescent scoliosis surgery.
Acknowledgments
We thank Elizabeth Drugge, PhD, for the data analysis and figure preparation and Marvin Medow, PhD, for his assistance in the data analysis.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors declare no conflicts of interest.
Ethics approval This study was approved by the New York Medical College Institutional Review Board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.