


Abstract
Background The fourth webinar in a 4-part series hosted by the International Society for the Advancement of Spine Surgery explored contemporary endoscopic spine surgery techniques. This session covered complex revision strategies, endoscopic management of grades 1–3 spondylolytic spondylolisthesis, cervical foraminotomy, and decompression techniques for cervical spondylotic myelopathy (CSM).
Objective The aim was to assess surgeon endorsement of the discussed endoscopic spine surgery techniques both before and after the webinar using polytomous Rasch analysis. Additionally, the analysis sought to determine how these insights might shape clinical guideline recommendations.
Methods Before the webinar, which was attended by 868 potential participants, a survey was distributed to collect data on the level of support for various techniques using a Likert scale. The polytomous Rasch model analyzed these responses by evaluating decision complexity relative to surgeon expertise. This approach helped develop a logarithmic scale to objectively analyze categorical responses, distinguish between congruent and incongruent items, and contribute to the enhancement of clinical guidelines.
Results Of the 868 surgeons, 263 accessed, 150 started, and 118 completed the prewebinar survey, with a completion rate of 78.7%. The participants were mainly orthopedic surgeons (59.3%) and neurosurgeons (34.7%) but also included residents (2.5%), fellows (1.7%), and interventional radiologists (1.7%). In the postwebinar phase, 298 participants accessed the survey, 169 started it, and 128 completed it, achieving a 75.7% completion rate. The demographics of postwebinar participants closely mirrored the initial group: 66.4% orthopedic surgeons, 23.4% neurosurgeons, 3.6% residents, 2.9% fellows, 0.7% medical students, and 2.9% interventional radiologists. The Rasch analysis confirmed high surgeon confidence for the posterior cervical foraminotomy and endoscopic treatment of spondylolytic spondylolisthesis grades 1 to 3 and posterior endoscopic decompression for CSM. Both pre- and postwebinar responses showed a good fit to the Rasch model for these endoscopic techniques, indicating minimal bias, supported by differential item functioning analysis. The application of the endoscopic surgery platform for procedures such as lumbar revision surgery for adjacent segment disease or failed interbody fusion cages and posterior decompression of CSM saw little shift in endorsement, as evidenced both in descriptive and the logarithmically transformed Rasch statistics.
Conclusion This webinar highlighted the evolving consensus on best practices in endoscopic spine surgery, displaying wide acceptance of endoscopic debridement of spondylolytic spondylolisthesis, cervical foraminotomy for herniated disc and bony stenosis, and posterior endoscopic decompression for CSM.
Clinical Relevance Assessing surgeon confidence and acceptance of endoscopic spinal surgeries using polytomous Rasch analysis.
Level of Evidence Level 2 (inferential) and 3 (observational) evidence because Rasch analysis provides statistical validation of instruments rather than direct clinical outcomes.
- endoscopic spine surgery
- polytomous Rasch analysis
- surgeon endorsement
- lumbar revision surgery
- spondylolytic spondylolisthesis
- cervical herniated disc
- cervical foraminal stenosis
- Cervical spondylotic myelopathy
Introduction
The International Society for the Advancement of Spine Surgery (ISASS) recently hosted the fourth in a 4-part series of webinars dedicated to the cutting edge of endoscopic spine surgery. This session focused on deepening the understanding of and fostering discussion around advanced techniques for treating complex spinal conditions. Key topics addressed included endoscopic spine surgery for complex revision strategies, such as adjacent segment disease or failed interbody fusion implants, endoscopic treatment of grades 1 to 3 spondylolytic spondylolisthesis, cervical foraminotomy for herniated disc and bony foraminal stenosis, and endoscopic decompression for cervical spondylotic myelopathy (CSM). The webinar utilized polytomous Rasch analysis to evaluate participant feedback on each discussed topic, providing a sophisticated framework based on item response theory (IRT).
Surveys conducted before and after the webinar captured valuable insights, which were analyzed using polytomous Rasch analysis. This approach assessed how well participants received each topic and procedure, highlighting the rapid advancements and robust evidence in favor of patient-centered minimally invasive surgery. This method offered a thorough examination of the attendees’ perceptions, experiences, and outcomes, providing a robust foundation for evaluating the efficacy of the discussed endoscopic techniques and the satisfaction levels of surgeons. These findings are instrumental in shaping clinical guidelines for endoscopic spine surgery.
The incorporation of the Rasch model, grounded in IRT,1–8 enhances this analysis by offering a sophisticated framework to interpret the data from this webinar series on spine surgery. It effectively addresses the probabilistic elements of decision-making by correlating task difficulty with individual proficiency,8 proving essential for analyzing agreement on various topics. Spine surgery, which depends heavily on a mix of experience, skill, and external factors, poses challenges inadequately addressed by traditional statistical methods focused on patient-reported outcomes or surgeon decisions. By applying mathematical precision to categorical data like Likert-scale responses, the Rasch model provides several significant benefits. It evaluates the complexity of decisions within the context of surgical expertise for a deeper understanding, converts ordinal data to a precise scale enhancing comparison accuracy, and ensures uniform measurement across varied surgical choices for reliable comparisons. Additionally, it identifies outlier items to refine evaluation tools and supports the development of educational content and guidelines by highlighting areas of strength and potential improvement, thereby improving surgical outcomes. By leveraging the polytomous Rasch model, this analysis aims to transform the expertise shared during the webinar into actionable insights for clinical evidence evaluation based on surgeon feedback.
Materials and Methods
Webinar and Surgeon Survey
The authors distributed an online questionnaire via www.typeform.com to 868 potential surgeons during an ISASS-sponsored Zoom webinar on 16 April 2024. Participants were invited to evaluate their level of support or importance for 4 discussed topics using a Likert scale from 1 (low) to 5 (high). This survey was administered both at the beginning and the end of the webinar to monitor any shifts in the participants’ endorsements due to the information presented. The topics assessed for support, each rated on the same 1 to 5 scale, included the following (Figure 1):
“Endoscopic Spine Surgery for Complex Revision Strategies” by Christian Morgenstern, MD, Center of Spine, Teknon Medical Center, Barcelona, Spain.
“The Endoscopic Treatment of Grades 1 to 3 Spondylolytic Spondylolisthesis” by Martin Knight, MD, FRCS, MBBS, Manchester University, The Spinal Foundation, The Weymouth Hospital, London, UK.
“Cervical Endoscopy for the Treatment of Disc Herniation and Spinal Stenosis” by Yi Jang, MD, Beijing Haidian Hospital, Beijing, China.
“Clinical Efficacy of Spinal Endoscopy in the Treatment of Cervical Spondylotic Myelopathy” by Xifeng Zhang, MD, Department of Orthopedics, First Medical Center, PLA General Hospital, Beijing, China.

Left to right: Webinar moderator—Kai-Uwe Lewandrowski, MD, faculty who presented on the following topics: (1) Yi Jang, MD, Beijing Haidian Hospital, Beijing, China, presented “Cervical Endoscopy for the Treatment of Disc Herniation and Spinal Stenosis.” (2) Martin Knight, MD, Manchester University, The Spinal Foundation, London, UK, presented ”The Endoscopic Treatment of Grades 1 to 3 Spondylolytic Spondylolisthesis.” (3) Christian Morgenstern, MD, Morgenstern Center of Spine, Teknon Medical Center, Barcelona, Spain presented “Endoscopic Spine Surgery for Complex Lumbar Revision Strategies.” (4) Xifeng Zhang, MD, Department of Orthopedics, First Medical Center, PLA General Hospital, Beijing, China, presented “Clinical Efficacy of Spinal Endoscopy in the Treatment of Cervical Spondylotic Myelopathy.”
Additionally, participants were asked to provide details about their postgraduate education and years in practice.
Statistics and Rasch Analysis
The data were exported to Excel and analyzed using IBM SPSS (version 27) and Jamovi (version 2.3). Descriptive statistics were used to summarize responses and calculate means, ranges, SDs, and percentages. The χ 2 test assessed the relationship between variables, while the Rasch analysis was conducted using the IRT module in Jamovi. A P value less than 0.05 was considered statistically significant, and a 95% confidence interval was applied to all statistical tests. The polytomous Rasch model, as detailed by Andrich and discussed in Part 1 of the report, was utilized in this survey analysis. This model suggests that the characteristics of both the individual and the item determine the probability of a specific outcome in an empirical context. It models ordered response data by the likelihood of a response falling into categories such as “strongly agree,” “agree,” “disagree,” or “strongly disagree.” In the polytomous Rasch model, scoring x on an item indicates that an individual has surpassed x thresholds on a continuum while not surpassing the remaining m − x thresholds. Mathematically, the application of the Rasch model in this study is expressed as the log odds (or logit) of a person endorsing an item, reflecting the difference between the person’s ability or level of agreement and the item’s difficulty. The model uses χ 2 fit statistics, outfit, and infit to evaluate the data’s fit to the model. The findings from the polytomous Rasch analysis are visually presented in the Wright plot9 and through person-item map analysis.10
Sample Size
The Rasch model operates under a principle of balanced requirements; to achieve a stable measure of individuals, the number of items presented should match the number of participants required to calibrate those items accurately. This symmetry is critical in psychometrics, as it ensures the reliability of the measurements derived from the model. According to Azizan et al,11 administering a set number of items—say, 30—to an equal number of participants, when done under conditions of appropriate targeting and good model fit, is likely to produce statistically stable measurements. Specifically, measures obtained in this setup are expected to be stable within ±1.0 logits at a 95% confidence level.
Bias Detection
Rasch analysis excels at identifying disturbances in data, including biases, by analyzing residuals—the differences between observed and model-predicted responses. It generates fit statistics for each item to gauge their alignment with Rasch model expectations. The outfit mean square error statistic, sensitive to outliers, measures deviations from model predictions as a ratio of observed to expected variance, where a value of 1.0 signifies perfect fit, values above 1.0 indicate noise, and values below 1.0 suggest overfit. In contrast, infit is a weighted version that lessens the impact of less informative responses. Misfitting items, indicated by infit and outfit statistics, may function differently across respondent subgroups and could signal bias, known as differential item functioning (DIF).12 This bias can appear when individuals with equivalent abilities but different backgrounds respond inconsistently to an item. The difNLR() and difORD() functions are used for detecting DIF in dichotomous and ordinal data, respectively. The difNLR() applies a nonlinear regression model for binary responses, while the difORD() uses logistic models suitable for ordinal data, both employing likelihood ratio tests to confirm the presence of DIF.13
In this study, graphical tools, such as person-item interaction maps, Wright maps, and item characteristic curves, were used to visually assess how items performed across different groups and to detect bias by examining infit and outfit statistics. Acceptable ranges for infit and outfit values, generally between 0.6 and 1.4, indicate a lack of distortion in the data. Additionally, the authors utilized the MAPQ3 methodology, a technique based on IRT analysis, where values of 0.3 or less also indicate an absence of data distortion. These tools assist in identifying items that may disproportionately affect certain subgroups. Given its focus on measuring latent traits and identifying item bias,13 Rasch analysis was deemed more effective than regression or analysis of variance in detecting biases within this study.
Results
The fourth part of the webinar series titled “Current and Emerging Techniques in Endoscopic Spine Surgery,” hosted by ISASS on 16 April 2024, attracted 868 surgeons, of whom 263 accessed, 150 started, and 118 completed the prewebinar survey, with a completion rate of 78.7%. The participants were mainly orthopedic surgeons (59.3%) and neurosurgeons (34.7%) but also included residents (2.5%), fellows (1.7%), and 2 interventional radiologists (1.7%). In the postwebinar phase, 298 accessed the survey, 169 started it, and 128 completed it, achieving a 75.7% completion rate. The demographics of postwebinar participants closely mirrored the initial group, with 66.5% orthopedic surgeons, 23.4% neurosurgeons, 3.6% residents, 2.9% fellows, 0.7% medical students, and 2.9% others (interventional radiologists). The polytomous Rasch analysis conducted on the responses from participants of the fourth webinar provided insightful data on endorsing various endoscopic procedures before and after the webinar. The procedures analyzed included the following:
endoscopic spine surgery for complex revision strategies, including adjacent segment disease and removal of failed cages, and endoscopic revision interbody fusion with re-grafting, expandable cages, and adjacent segment disease
endoscopic debridement of grades 1 to 3 spondylolytic spondylolisthesis
cervical endoscopic foraminotomy disc herniation and bony stenosis
posterior endoscopic single and multilevel decompression of CSM
Descriptive Statistics of Learning Curve Assessment, Clinical Outcomes, and Endoscopic Techniques
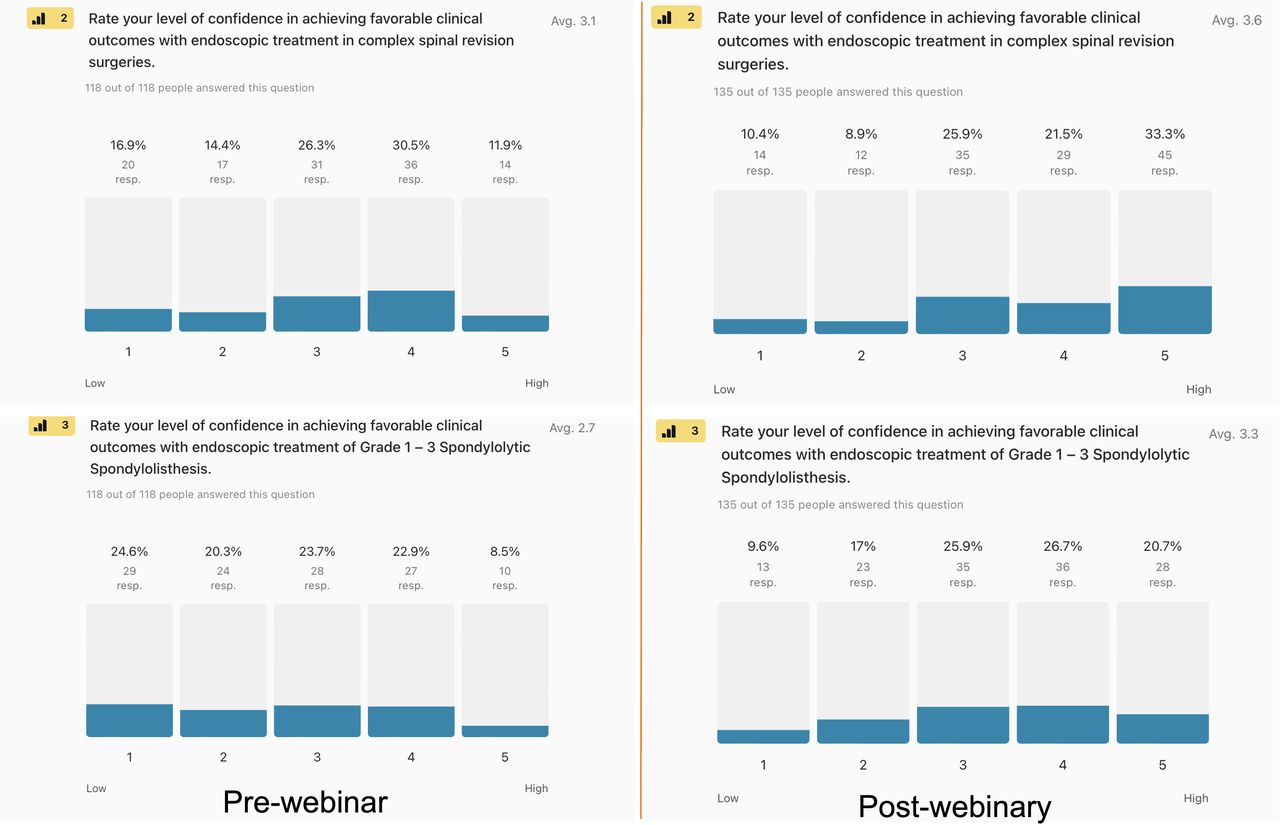
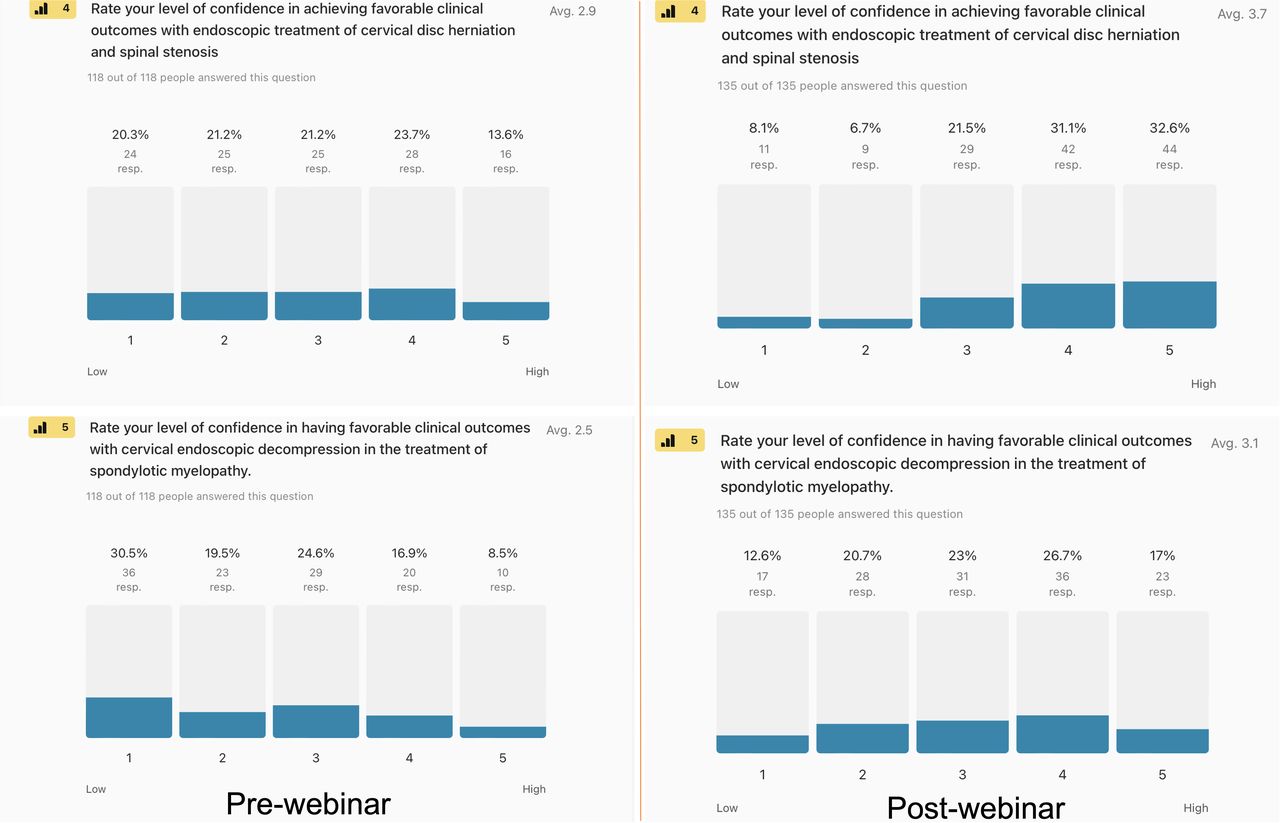
The descriptive statistics illustrated in Figures 2–3 reveal the changes in surgeons’ perceptions and endorsements of various endoscopic spine surgery techniques before and after the webinar. Figure 2 reveals a notable increase in surgeons’ confidence in performing endoscopic revision surgeries on patients with failed lumbar spine surgeries due to cage-related issues and adjacent segment disease. Confidence levels, as rated on a Likert scale, increased from 42.4% prewebinar to 54.8% postwebinar for the highest confidence categories (4 and 5). Additionally, the perceived advantage of debriding lumbar spondylolytic spondylolisthesis (grades 1–3) improved significantly after the webinar, rising from 31.4% to 47.7%. Figure 3 further demonstrates the webinar’s effectiveness, with a significant boost in confidence for performing posterior percutaneous endoscopic cervical foraminotomy from 34.4% prewebinar to 63.3% postwebinar. Confidence in treating CSM using endoscopic surgery increased from 25.4% to 37.4%. These descriptive statistic results revealed subtle changes in professional attitudes and confidence concerning different endoscopic spine surgery methods. Such shifts might reflect the potential of educational programs such as the ISASS webinar series to influence surgical practice choices and perceived effectiveness. The Rasch model was utilized to scrutinize these shifts in endorsement in greater detail, aiming to isolate those outcomes that consistently received strong support from surgeons to exclude biases or anomalies within the data.

Pre- and postwebinar descriptive statistics of the level of confidence in achieving favorable outcomes with endoscopic revision surgery in previously operated patients with failed lumbar spine surgeries due to cage nonunion, cage subsidence or expulsion, or adjacent segment disease: (2) Only 42.4% of surgeons gave it the highest endorsement by selecting options 4 or 5 on a Likert scale from 1 to 5 before the webinar vs 54.8% after the webinar. (3) Only 31.4% of prewebinar respondents thought debriding lumbar spondylolytic spondylolisthesis grades 1 to 3 was advantageous. However, after the webinar based on Dr Knights’s presentation, this number increased to 47.7%.

Pre- and postwebinar descriptive statistics of (4) the level of survey respondents’ confidence in achieving favorable clinical outcomes with posterior percutaneous endoscopic cervical foraminotomy for herniated disc or bony stenosis at a high level (survey response options 4 or 5) was 34.4% before and rose to 63.3% after the webinar, and (5) the same confidence numbers for effectively treating single or multilevel cervical spondylotic myelopathy with the endoscopic surgery platform were 25.4% and 37.4%, respectively.
Polytomous Rasch Analysis
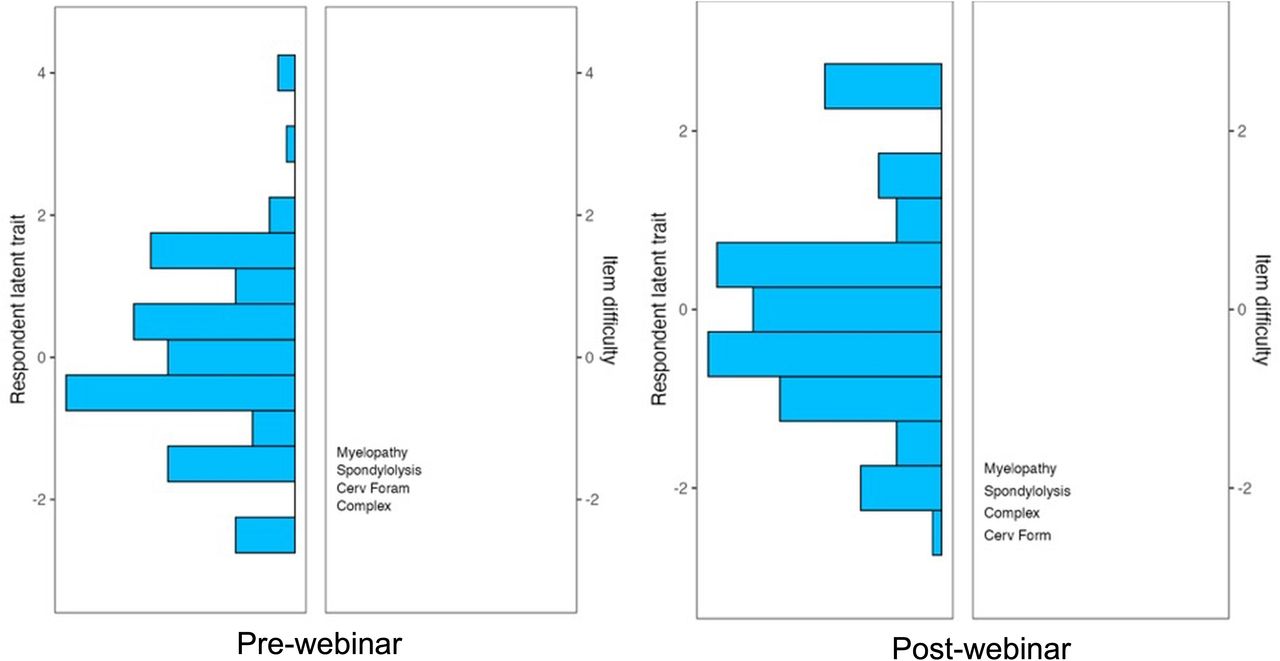
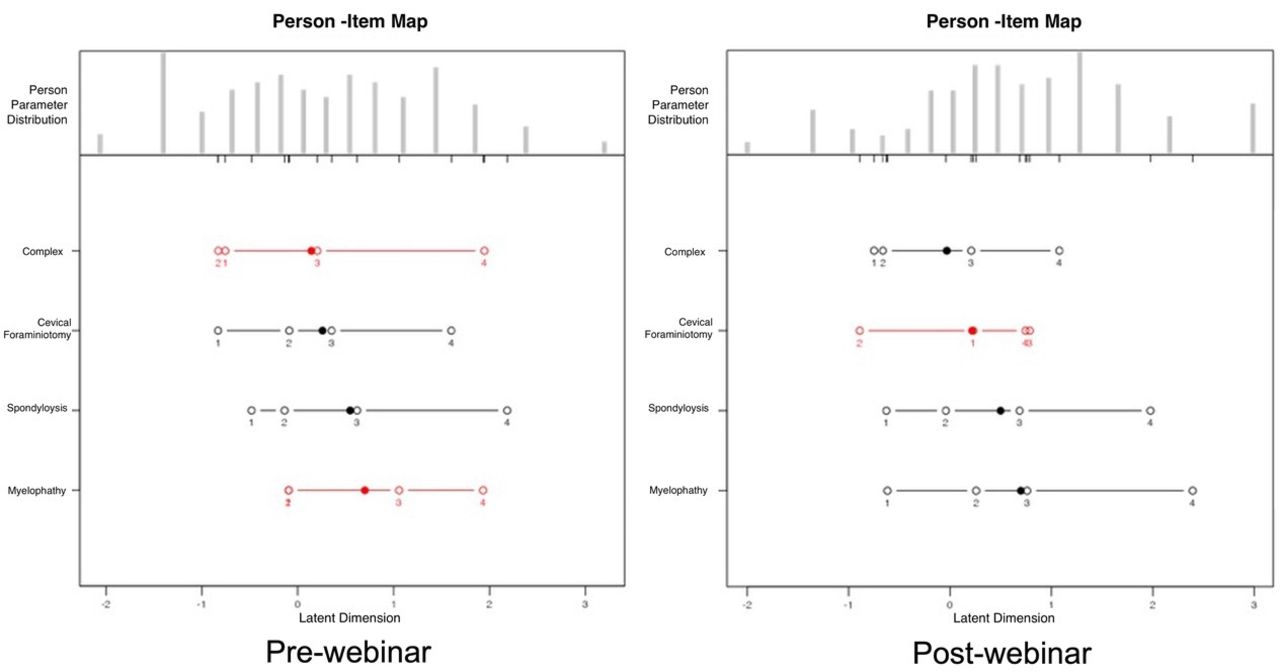
As demonstrated in Figure 4 through 5, the polytomous Rasch analysis offered a nuanced understanding of surgeons’ intensity of endorsements of various procedural techniques, demonstrating the interaction between the surgeons and the various endoscopic surgeries tested. Figure 4 presents Wright plots from pre- and postwebinar assessments, showcasing a shift in surgeons’ latent traits and the reduction in assessment gaps from 3 to 1, indicating a substantial educational impact on participants. The analysis identified that the most challenging items regarding agreement remained those involving complex lumbar spine revision surgeries and CSM. Figure 5 uses a person-item map to graphically depict the logit-transformed positions of surgeons and test items along a unified continuum. This Rasch model analysis indicated a more orderly progression in the ranking of item difficulties postwebinar, especially in the context of surgical debridement of lumbar spondylolytic spondylolisthesis, cervical foraminotomy, and posterior endoscopic decompression of CSM with all mean logits shifted to the right and being greater than 0; that is, greater than 50% chance of endorsing the test items, and a wider logit spread indicating better differentiating between the categories of these test items. However, the complex lumbar spine revision scenarios showed disorderly threshold progression, suggesting ongoing challenges in achieving consensus on these topics. It remained a lower-intensity item with logit locations shifted to the left (between 0 and 1) and a narrower logit spread.

The item response theory polytomous Rasch partial agreement analysis was employed to obtain Wright plots of prewebinar (left panel) and postwebinar (right panel) survey responses regarding the surgeons’ confidence level in achieving favorable clinical outcomes with the clinical application of the endoscopic spinal surgery platform in the treatment of painful posterior foraminal stenosis, symptomatic cervical spondylotic myelopathy (CSM), the surgical debridement of grades 1 to 3 lumbar spondylolytic spondylolisthesis, and in complex lumbar spine revision surgery scenarios due to cage failure, such as cage subsidence or expulsion, nonunion, or adjacent segment disease. On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability and intensity of partial agreement. The surgeons, represented by horizontal bars at the top, represented the highest level of endorsement capable of performing these difficult operations with favorable outcomes. On the right of the Wright plot, the harder-to-agree-on items are listed at the top vs the easier-to-agree-on ones at the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item (neutral response). There were 3 assessment gaps on the prewebinar survey and 1 on the postwebinar survey. This observation highlights the beneficial training effect of this webinar regarding filling knowledge gaps in participating spine surgeons. There was no redundancy between any of the test items. However, successfully treating patients suffering from CSM and those from persistent lumbar pain due to spondylolytic spondylolisthesis with endoscopic decompression was considered the hardest.

The person-item map of prewebinar (a) and postwebinar (b) survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts person and item positions (in logits) along the x axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Disordered items are shown in red, and ordered ones are in black. Examining the order and location of these test items reveals an orderly progression of the ranked order of item difficulties or intensities along the logit continuum for prewebinar responses regarding the surgeons’ confidence level in achieving favorable clinical outcomes with the clinical application of the endoscopic spinal surgery platform in the treatment of painful posterior cervical foraminal stenosis and the surgical debridement of grades 1 to 3 lumbar spondylolytic spondylolisthesis. The prewebinar test items CSM and complex lumbar spine revision surgery scenarios due to cage failure, such as cage subsidence or expulsion, nonunion, or adjacent segment disease generated disorderly threshold progression, suggesting a poor fit to the Rasch model with a statistically significant difference between the observed values and the values predicted by the model (Tables 1 and 2). In the postwebinar survey, the test item surgical debridement of grades 1 to 3 lumbar spondylolytic spondylolisthesis generated an orderly threshold progression following Dr Knight’s presentation. The complex lumbar spine revision surgery scenarios due to cage failure, such as cage subsidence or expulsion, nonunion, or adjacent segment disease, continued to generate postwebinar disorderly threshold progression.
Prewebinar survey model fit analysis and item statistics of the rating scale model.
Postwebinar survey model fit analysis and item statistics of the rating scale model.
Fit and DIF Bias Statistics
Infit and outfit statistics showed that all calculated values were between 0.8 and 1.3 before and after the webinar. These numbers suggest that both the outlier-sensitive statistics (outfit) and the inlier-sensitive or information-weighted fit statistics, which are more sensitive to the pattern of responses to items targeted on the person, fit the Rasch model well (Tables 1 and 2). The authors also employed the MAPQ3 methodology rooted in IRT analysis with 0.167 (P < 0.001) calculated for the prewebinar survey and 0.121 (P = 0.028) for the postwebinar survey—less than 0.3 corroborating the absence of data distortion. The DIF statistics for the prewebinar survey DIF detection procedure showed no statistically significant difference between orthopedic (reference group) and neurosurgeons (focal group; Tables 3 and 4) in item response characteristics curves. However, the DIF statistics for the postwebinar survey DIF detection procedure showed a statistically significant difference between surgeons residing outside China (reference group) and surgeons from China (focal group; Table 4), regarding the items “complex revision strategies” statistics of 11.9786 and a P value of 0.003, therefore indicating data distortion suggestive of bias for these test item in the postwebinar survey (Table 4, Figure 6).
Prewebinar survey DIF detection procedure for ordinal data based on adjacent category logit model with orthopedic surgeons as the reference and neurosurgeons as the focal group.
Postwebinar survey DIF detection procedure for ordinal data based on adjacent category logit model with surgeons from outside China as the reference vs those from China as the focal group l.

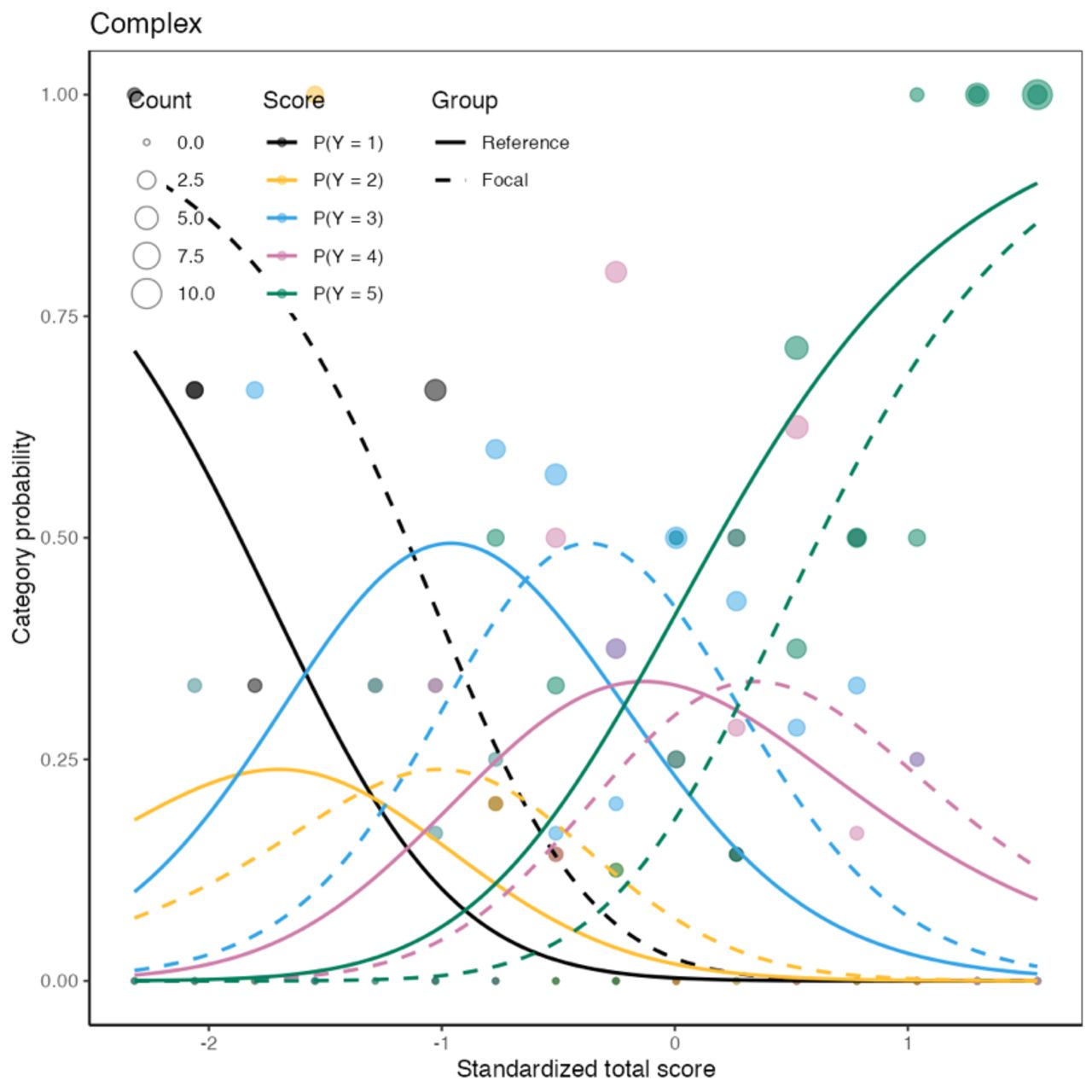
Item characteristic curves generated from postwebinar survey responses on test item “complex lumbar spine revision surgery” scenarios due to cage failure, such as cage subsidence or expulsion, nonunion, or adjacent segment disease” as part of a differential item functioning (DIF) detection process to detect item bias between surgeons from Europe and the Americas and Chinese spine surgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (non-Chinese surgeons) and another for the focal group (Chinese surgeons). The groups were tested for bias because Chinese participants comprised the largest contingent in the postwebinar survey. Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level, which showed a significant difference between non-Chinese surgeons (reference group) and Chinese surgeons (focal group) with the statistics for prewebinar DIF detection of 2.5379 and a P value of 0.281 (Table 3) and postwebinar DIF detection of 12.111 and a P value of 0.002 (Table 5). There were statistical differences between non-Chinese and Chinese surgeons in how they perceived the test item “complex lumbar spine revision surgery,” suggesting bias. All the other test items did not show any evidence of bias between the Chinese and non-Chinese surgeons.
Postwebinar survey DIF detection procedure for ordinal data based on adjacent category logit model with orthopedic surgeons as the reference and neurosurgeons as the focal group l.
Discussion
The “Current and Emerging Techniques in Endoscopic Spine Surgery” webinar series, hosted by the ISASS, highlights the growing interest and evolving practices in endoscopic spine surgery. The last installment of the 4-part series notably impacted spine surgeons’ perceptions of mastering different endoscopic techniques and their endorsement of various procedures such as cervical foraminotomy and transforaminal debridement of spondylolytic spondylolisthesis. The series has drawn significant online participation, as evidenced by the high number of webinar participants and the high rates of survey completion. This engagement spans various specialties and levels of experience throughout these 4 webinars, demonstrating widespread interest in these techniques, with orthopedic surgeons consistently more involved than neurosurgeons.
Descriptive Opinion Statistics
The descriptive statistics reveal significant changes in surgeons’ perceptions and endorsements of various endoscopic spine surgery techniques before and after the fourth ISASS webinar on endoscopic surgery techniques. The data show a notable increase in surgeons’ confidence in performing endoscopic revision surgeries on failed previous lumbar spine operations, such as cage-related issues and adjacent segment disease. Specifically, confidence levels on the Likert scale rose from 42.4% to 54.8% for the highest confidence categories, 4 (agree) and 5 (strongly agree). Additionally, there was a significant improvement in the perceived advantage of debriding lumbar spondylolytic spondylolisthesis, with endorsements increasing from 31.4% to 47.7% postwebinar. Employing the same criteria, there was also a significant boost in confidence for performing posterior percutaneous endoscopic cervical foraminotomy, with confidence levels surging from 34.4% prewebinar to 63.3% postwebinar. Confidence in managing CSM using endoscopic surgery similarly increased, rising from 25.4% to 37.4%. The ISASS webinar series “Current and Emerging Techniques in Endoscopic Spine Surgery” appears to have successfully influenced participants, enhancing their skills and knowledge in specific endoscopic procedures. The Rasch model was employed to ensure that these observed shifts in endorsement were not influenced by biases or anomalies within the data. This statistical approach allowed for detailed scrutiny of the changes, isolating outcomes that consistently received strong support from surgeons. This rigorous analysis confirms that the improvements in surgeon confidence were substantial and likely to influence their clinical practices moving forward.
Rasch Survey Analysis
The Rasch analysis provided a nuanced evaluation of the shifts in endorsements across various surgical techniques, enabling us to differentiate between authentic changes in clinical opinion and those that might be due to statistical anomalies or biases within the survey responses. The analysis demonstrated that most of the survey items were effective discriminators, aligning well with the predictions of the Rasch model. The majority of outfit statistics hovered around 1, with some variations between 0.8 and 1.3, except for the items related to complex revision strategies. Outfit statistics below 1 indicate that the data are less variable than expected by the model, suggesting a high predictability (as detailed in Tables 1 and 2). While values near 1.0 are considered optimal, a range of 0.7 to 1.3 generally signifies a robust model fit. Notably, we did not observe very low outfit values; these would typically raise fewer concerns than higher values, as they do not suggest the presence of outlier-driven noise. The infit and outfit values indicated that the survey questions were effective, demonstrating the efficiency of the survey instrument employed by the researchers.
The authors gained insights from pre- and postwebinar Wright plots, indicating that endoscopic posterior single- and multilevel decompression for CSM and endoscopic debridement of grades 1 to 3 spondylolytic spondylolisthesis elicited strong, albeit divided, opinions, reflecting these as the most contentious issues. In contrast, posterior cervical endoscopic foraminotomy for disc herniation and bony stenosis achieved a higher consensus. This aligns with numerous clinical studies validating the efficacy of the posterior endoscopic cervical foraminotomy technique.14–23 The person-item maps demonstrated disordered threshold responses prewebinar for endoscopic surgery in complex revision surgeries and CSM. Such disorder suggests category confusion or inversion, where participants may have found it challenging to distinguish between different levels of agreement clearly. This type of response distribution, characterized by sharp divides between agreement and disagreement, typically occurs when the response categories do not form a clear, progressive sequence. This confusion may arise from ambiguous category definitions or the inherent complexity of the question, leading to diverse interpretations among participants. Additionally, the response scale might need to be finely tuned enough to capture nuanced differences in attitudes, potentially causing reversals using categories. These findings underscore the necessity for further examination and refinement of survey questions to improve clarity and address the issues with disordered responses. Despite the lack of external “right” or “wrong” criteria to guide recalibration or refinement of potentially redundant or predictable items, the authors employed the Rasch model to analyze the survey data meticulously. They focused on identifying shifts in endorsement that demonstrated a structured threshold arrangement. After the webinar, a more organized logit progression was noted in the responses for endoscopic debridement of grades 1 to 3 spondylolytic spondylolisthesis and posterior endoscopic decompression for single- or 2-level CSM.24 For posterior cervical foraminotomy, the orderly progression in logits indicated a solid consensus among surgeons regarding their confidence in achieving positive clinical outcomes with this technique.
Limitations and Bias Detection
High item complexity and a lack of scale sensitivity were notable constraints in our Rasch analysis. As detailed in the publication of the second ISASS webinar about contemporary endoscopic spinal surgery techniques, the authors opted for the difORD() functions to identify biases instead of the traditional analysis of variance and regression analyses. These traditional methods can be problematic when based on external criteria, assuming these criteria are unbiased measures. The challenge of creating an unbiased external criterion underscores the necessity of relying solely on internal criteria derived from the test responses. The Rasch logistic response model addresses this challenge effectively by evaluating responses using internal criteria. This approach allows for maximum likelihood estimation techniques, integral to the Rasch model, producing valuable asymptotic variance estimates in parameter estimates. This methodological choice facilitates the identification of biased tests, distinguishing them from items that misfit for other reasons and defining the expected magnitude of residual variance when both items and person responses align with the measurement model. Our analysis of surgeon responses, a crucial aspect of our research, is an unbiased reflection of prevailing trends. This is particularly true for most items, except for those related to “complex revision surgery.” In this case, the DIF statistics from the postwebinar survey revealed a statistically significant bias between non-Chinese surgeons (reference group) and Chinese surgeons (focal group). This indicates a clear distortion in the data for these items in the postwebinar analysis, as evidenced by specific figures and tables in the documentation, highlighting a potential bias in the survey’s findings for these particular test items. While different opinions on surgical spine care may exist in various countries as a reflection of different training standards and managing styles, we did not observe any bias in the response to the endoscopic treatment of CSM, spondylolytic spondylolisthesis, or foraminal cervical stenosis.
Conclusions
The findings from the third ISASS webinar on Contemporary Endoscopic Spinal Surgery Techniques highlight the profound influence of targeted educational programs on surgical practices. These programs are pivotal in shaping future clinical guidelines and training frameworks to better align with the latest surgical techniques and evolving confidence levels among surgeons. Key outcomes from the webinar’s surveys and analyses include a strong, unbiased interaction between surgeons’ experience of favorable clinical outcomes with endoscopic debriding lumbar spondylolytic spondylolisthesis, posterior percutaneous endoscopic cervical foraminotomy, and treating CSM.
Acknowledgments
This webinar and special issue were supported with an education grant to ISASS from Lange MedTech.
Footnotes
↵† International Society for the Advancement of Spine Surgery, Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI), International Intradisccal Therapy Society
↵‡ Minimally Invasive Spine Surgery Section of the Chinese Orthopedic Association (COA)
↵§ Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI)
↵¶ International Society for the Advancement of Spine Surgery
Funding ISASS received funding for the webinar and the publication of this special issue from Lange MedTech. Funding was paid directly to the organization. No formal funding by private, government, or commercial funders was received by the authors.
Declaration of Conflicting Interests The authors volunteered their time and internal resources to support the design and conduction of this research study. All authors aided in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The authors declare no conflict of interest relevant to this research, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone.
Disclosures Christian Morgenstern reports royalties/licenses with Signus GmbH and Hoogland Spine Products GmbH; consulting fees from SpineArt SA and UniTech GmbH; and support for attending meetings and/or travel from Hoogland Spine GmbH and Signus GmbH.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.