


Abstract
Background There is a paucity of data examining anterior lumbar interbody fusion (ALIF) with pedicle-screw fixation (ALIF-PSF) or without (standalone, sa-ALIF) for the treatment of low-grade isthmic spondylolisthesis (IS). Treating pathology with sa-ALIF reduces costs, operative times, and posterior access morbidity. This study aimed to investigate the clinical and radiographic outcomes of sa-ALIF for the management of low-grade IS compared with an ALIF-PSF cohort.
Methods Retrospective analysis of prospectively collected data. Consecutive patients from 1 senior spine surgeon performing sa-ALIF or ALIF-PSF for management of low-grade IS. Patient-reported outcome measures (PROMs) were collected at baseline, then postoperatively at 6 weeks, 6 months, 12 months, and a final follow-up timepoint. Computed tomography was conducted at 6 months, 12 months, or until interbody fusion was confirmed.
Results Two cohorts comprised 51 patients (sa-ALIF 22 and ALIF-PSF 29). Both cohorts’ PROMs improved from baseline to 12 months postoperatively. There were no significant differences (P = 0.05) in PROMs between the 2 cohorts at 6 months postoperatively, 12 months postoperatively, or at a final follow-up timepoint. There were no significant differences in mean fusion rates 12 months postoperatively (sa-ALIF 82% and ALIF-PSF 88%). Compared with preoperative measurements in sa-ALIF and ALIF-PSF cohorts, listhesis and segmental lordosis showed no significant changes, while disc height significantly increased (P = 0.0001). There were no significant differences in disc L5/S1 radiographic measurements between the cohorts at 12 months. There were 12 complications (sa-ALIF 2 and ALIF-PSF 10). Only 1 patient in the ALIF-PSF cohort required revision surgery.
Conclusions In appropriately selected patients with normal bone density, sacral slope <40°, and a body mass index <35, sa-ALIF is a safe and effective treatment option for grade I IS. The additional morbidity and cost of PSF may not be justified given the satisfactory clinical and radiographic outcomes of sa-ALIF for grade I IS.
Clinical Relevance Clinically, this research continues to suggest that sa-ALIF is a safe and effective method of treatment for low grade IS.
Level of Evidence 4.
Introduction
Isthmic spondylolisthesis (IS) is an anterior translation of a vertebral body over the subadjacent vertebrae secondary to bilateral defects of the pars interarticularis, with L5/S1 being more common than L4/L5. The majority of IS is asymptomatic with a prevalence of approximately 4.4% to 6%.1,2 However, when symptomatic, IS can lead to severe mechanical low back pain, lumbar radiculopathy, or both.3
The degree of anterolisthesis is categorized by the Meyerding classification system, where a higher grade is associated with increased listhesis.3 This system is used to stratify patients and inform clinical management.4
When conservative management for low-grade (I/II) IS is unsuccessful, spinal fusion is indicated.5 Fusion techniques used to manage IS include posterolateral bone graft with or without posterior pedicle-screw/rod fixation (posterior lumbar fusion [PLF]), with or without the addition of interbody cages (posterior lumbar interbody fusion [PLIF]), and anterior column interbody fusion either oblique (oblique lumbar interbody fusion) or direct anterior (anterior lumbar interbody fusion [ALIF]). ALIF is advantageous as it enables the impaction of a wide-footprint lordotic interbody cage with the restoration of disc height and segmental lordosis while indirectly increasing the circumferential diameter of the foramen.6,7 ALIF spares posterior musculoligamentous damage and retraction of cauda equina nerve roots.8 Supplementary posterior fixation may be added, involving PLF, open or percutaneous pedicle-screw fixation (PSF), or a combination. A recent large multicenter retrospective cohort suggested supplemental posterior fixation to ALIF-enhanced fusion rates without increasing the risk of adjacent segment disease.9 This was consistent with prior studies that have shown combined 360° approaches may provide superior fusion rates.7,9 However, the cost and morbidity of posterior fixation must be considered. Concerns regarding paraspinal muscle damage induced by iatrogenic denervation caused by posterior fixation remain contentious.10–12
There is a paucity of clinical and radiographic outcomes comparing standalone ALIF (sa-ALIF) without posterior fixation9,13–15 to ALIF with PSF for the management of IS. In contrast to ALIF-PSF, treating IS with sa-ALIF reduces costs, operative times, blood loss, and posterior access complications but may risk higher rates of nonunion.
We aimed to investigate the clinical and radiographic outcomes of sa-ALIF for the management of low-grade IS compared with an ALIF-PSF cohort and consider the cost effectiveness of each.
Methods
Study Design and Patient Population
For the present study, we conducted a retrospective analysis of prospectively collected data of consecutive patients undergoing either sa-ALIF or ALIF with PSF between November 2012 and October 2021. All operations were performed by a senior spinal fellowship-trained neurosurgeon. Treatment groups were not randomized.
The sa-ALIF cohort from 2014 to 2018 comprised a separate cage and buttress plate; then from 2018 to 2022, the sa-ALIF cohort comprised an integrated cage-plate-screw construct. The integrated sa-ALIF was adopted after 2018 when this construct became commercially available, accounting for the shorter follow-up time.
All patients enrolled in the study reported worsening mechanical low back pain, severe radicular lower extremity pain, or both (not responsive to physical therapy, opiate analgesia, and targeted steroid injections) and/or development of lumbar radiculopathy. Indications for sa-ALIF were symptomatic grade I isthmic anterolisthesis with mechanical low back pain, lumbar radiculopathy, or both. Additional posterior fixation was indicated for (i) grade I isthmic anterolisthesis with reduced bone density and/or high sacral slope (>40°) or (ii) grade II isthmic anterolisthesis. Bone density was assessed in high-risk patients.16 Patients with osteopenia or osteoporosis were referred to a consultant endocrinologist for preoperative optimization. The minimum follow-up period was 12 months. Patient demographics were recorded at baseline. The inclusion criteria were adults aged 18 years or older; patients with IS at L4/L5 or L5/S1 that had not responded to conservative management for a minimum of 6 months; and patients who agreed to attend all follow-up visits and imaging. All patients underwent a focused duplex scan to screen for vascular abnormalities, and if any were detected, they proceeded to computed tomography (CT). Exclusion criteria for surgery were disc disease across 3 or more levels, grades III to IV spondylolisthesis, significant iliac artery or aortic pathology, morbid obesity (body mass index [BMI] >35 kg/m2), previous complex/extensive retroperitoneal surgery, and abdominal/pelvic radiotherapy. Prior lumbar spine surgery was not an exclusion criterion.
Clinical Outcomes
Patient self-reported outcome measures (PROMs) were evaluated preoperatively and at 6 weeks, 6 months, 12 months, and final follow-up postoperatively. PROMs included visual analog scale (VAS) back and leg scores, Oswestry Disability Index (ODI) scores, and physical (physical component summary) and mental (mental component summary) 12-Item Short Form Survey (SF-12) scores. Ottawa decision regret scale scores (0–100) were evaluated at the final follow-up, with lower scores indicating higher satisfaction.17
Radiographic Outcomes
CT was performed on postoperative day 2 for instrumentation positioning, then at 6- or 12-month follow-up for interbody fusion status. If fusion was confirmed, no further CTs were undertaken to reduce patient radiation exposure. CT images were assessed using the Bridwell criteria.18 Fusion was assessed by a third-party radiologist from another institution. Segmental lordosis and disc height were measured, and anterolisthesis was reported using the Meyerding classification system (Table 1).
Meyerding classification system.
Adverse Events
Clinical adverse events recorded included persistent mechanical and radicular pain, surgical site infection, and re-operations at the index and adjacent levels. Acute complications were defined as ≤6 months, and chronic complications were defined as >6 months postoperatively.
Surgical Technique
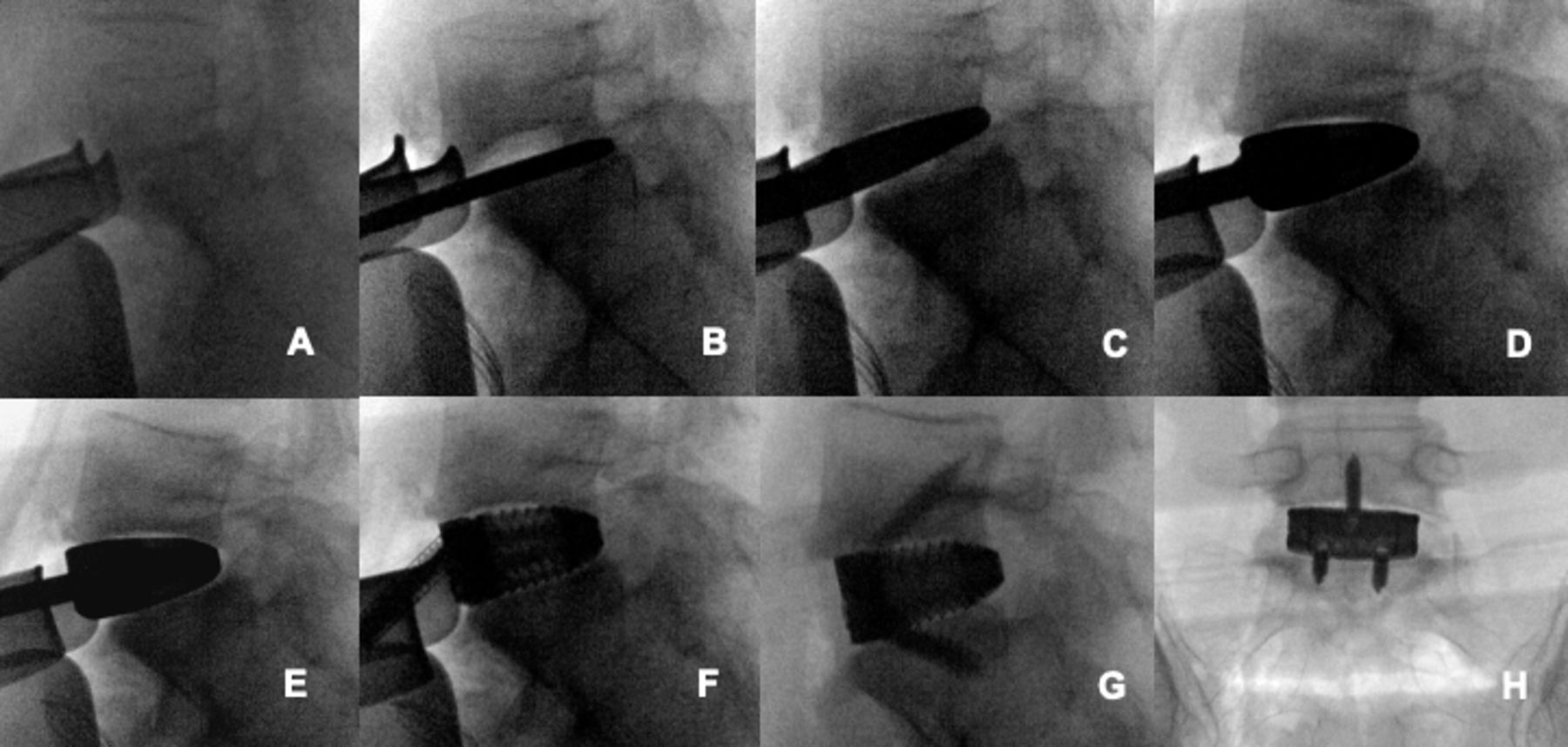
The anterior approach by a vascular access surgeon comprises a transverse or longitudinal skin incision, followed by a retroperitoneal dissection with retraction of the visceral structures, and exposure, mobilization, and retraction of the vessels. The target disk was confirmed by image intensifier and then resected, endplates were curetted/rasped, and sequential trials were used to distract and reduce the slip before a definitive cage was inserted along with a buttress plate (Perimeter, Medtronic PLC, Dublin, Ireland; 2014–2018) or a combined cage with integrated plate-screw fixation (Independence, Globus Medical, PA; 2018–2022; Figure 1). All ALIF cage types were polyetheretherketone. Procedures included were single-level (L4/L5 and L5/S1) or 2-level ALIF (L4/L5 + L5/S1). The interbody cage bone substitute used was recombinant human bone morphogenic protein 2 (rhBMP-2) from 2012 to 2020. rhBMP-2 (Medtronic PLC, Dublin, Ireland) was delisted by the TGA (Therapeutic Goods Administration—Federal Government Authority and Regulator) in Australia in March 2020;19 thereafter, a demineralized bone allograft (DBA, Australian Biotechnologies, Sydney, Australia) was used instead. A hybrid procedure consisted of a disc replacement at the superior L4/L5 and corresponding ALIF at inferior L5/S1 level.

Fluoroscopic images of anterior lumbar interbody fusion. (A) Anterior L5/S1 disc exposure. (B) Seven-millimeter paddle distractor (not rotated) to posterior apophyseal ring. (C) Nine-millimeter paddle distractor (rotated) to posterior apophyseal ring. (D) Large 13 mm, 15° trial. (E) Large 15 mm, 15° trial. (F) Large 15 mm, 15° cage. (G) Cage with screw fixation (lateral). (H) Cage with screw fixation (anteroposterior).
Ethical Statement
This study was a review of cases collected under a standard privacy disclosure to patients whose information will be used for ongoing evaluation of outcomes, and their identity will be protected in any publication arising from this. The project was reviewed by an independent expert in Human Research Ethics and classified as a low-risk research project in accordance with section 5.1.19 of the National Statement on Ethical Conduct in Human Research (2007). Institutional approval was granted by Epworth HealthCare (EH2024-1153). The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Statistical Methods
Counts and percentages were reported for categorical data, means, and SDs for continuous data. Proportions tests were used to compare categorical data between both cohorts (sa-ALIF and ALIF-PSF). Normal distribution was checked using Shapiro-Wilk tests. Paired sample t tests were used to compare PROMs and radiographic parameters from baseline to final follow-up. Independent t tests were used to compare patient demographics, operative statistics, clinical outcomes, and radiographic outcomes between both cohorts (sa-ALIF and ALIF-PSF). Statistical significance was assessed at P = 0.05, 2-tailed. Analyses were performed in Stata 18 (Stata Corporation, College Station, Texas).
Results
The cohort consisted of 51 patients (sa-ALIF 22 and ALIF-PSF 29) with similar demographics (Table 2). Mean age and BMI of sa-ALIF were 43.3 ± 14.1 years (54.5% men) and 24.1 ± 2.0 kg/m2 vs 48.7 ± 11.4 years (62.1% men) and 27.9 ± 3.4 kg/m2 for the ALIF-PSF cohort. Only 4 patients were current smokers (sa-ALIF n = 1). All patients were privately insured (except for 1 patient in the sa-ALIF cohort who received workers’ compensation). There were 43 grade I IS (sa-ALIF 22 and ALIF-PSF 21) and 8 grade II IS (ALIF-PSF 8) patients. There were 4 two-level procedures at L4/5 and L5/S1, 2 involving an L4/L5 total disc replacement and L5/S1 ALIF (sa-ALIF 1 and ALIF-PSF 1), and 2 involving a 2-level ALIF at L4/L5 and L5/S1 (sa-ALIF 1 and ALIF-PSF 1).
Patient demographics and operative data.
Only 6 patients (sa-ALIF 1 and ALIF-PSF 5) received an interbody cage with a separate buttress plate, with the remainder receiving integrated cage-plate-screw constructs. rhBMP-2 was used in 22/29 (92%) of the earlier ALIF-PSF cohort but only 4/22 (19%) of the more recent sa-ALIF cohort.
All PROMs significantly improved from baseline to final follow-up in both sa-ALIF and ALIF-PSF except SF-12 MCS (Table 3). Mean VAS leg values were lower in the sa-ALIF cohort preoperatively (sa-ALIF 7.2 vs ALIF-PSF 8.1, P < 0.05) and 6 weeks postoperatively (sa-ALIF 2.7 vs ALIF-PSF 4.9, P < 0.001), while mean SF-12 physical component summary scores were greater in the sa-ALIF cohort 6 weeks postoperatively (sa-ALIF 39.9 vs ALIF-PSF 36.8, P < 0.05). There were no other significant differences (P < 0.05) in baseline PROMs and PROMs at all follow-up time points. The decision regret scores were extremely low, indicating low regret in both cohorts.
Clinical outcomes.
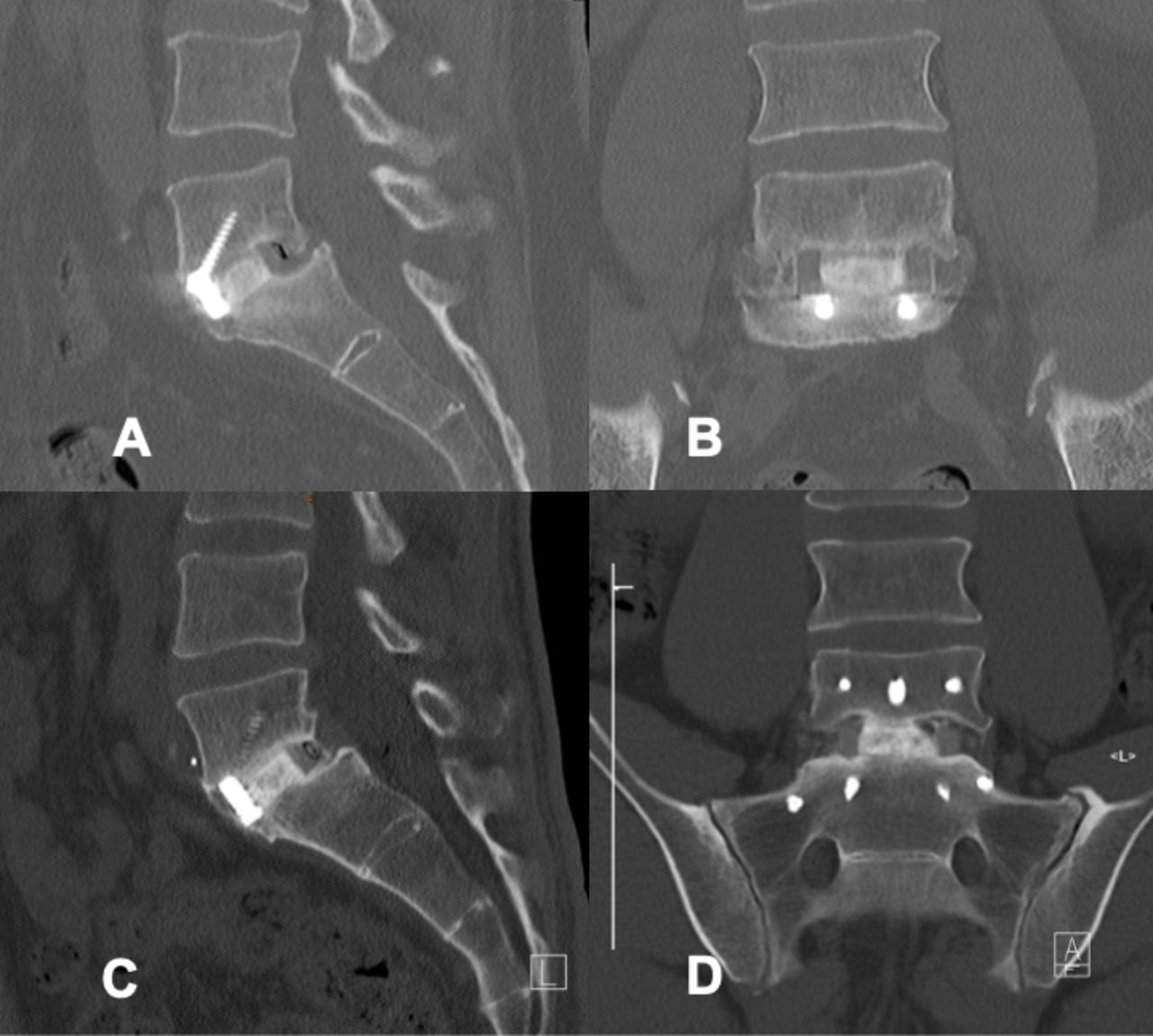
[td][td][td]Table 4 shows our radiographic fusion results with example fusion in Figure 2. At 6 months postoperatively, fusion rates (Bridwell interbody fusion grade 1 or 2) were 36.4% and 50.0% in the sa-ALIF and ALIF-PSF cohorts (P = 0.34), respectively, increasing to 81.8% and 88.5% 12 months postoperatively (P = 0.52). The mean fusion rates were not significantly different between the sa-ALIF cohort and the ALIF-PSF cohort at 6 and 12 months postoperatively. None of the sa-ALIF patients required subsequent supplemental posterior fixation.
Computed tomography fusion outcomes at 6- and 12-month follow-up.

Example fusion on 12-month postoperative computed tomography for standalone anterior lumbar interbody fusion (ALIF) (A) sagittal and (B) coronal view and for ALIF with pedicle screw fixation (C) sagittal and (D) coronal view.
There was no significant change (P > 0.05) in the degree of anterolithesis or segmental lordosis in either cohort (sa-ALIF and ALIF-PSF) comparing preoperative to 12-month measurements. Conversely, disc height improved in sa-ALIF (P = 0.0001) and ALIF-PSF (P = 0.0001) cohorts comparing preoperative to 12-month postoperative scores. The mean disc height in the sa-ALIF cohort was significantly greater than in the ALIF-PSF cohort 6 months postoperatively (sa-ALIF 12.1 mm vs ALIF-PSF 10.4, P < 0.05; Table 5). There were no other significant differences in radiographic parameters between both cohorts at baseline, 6 months postoperatively, and 12 months postoperatively.
Radiographic parameters at pre- and postoperative timepoints.
There were 12 adverse events (Table 6), 2 of which occured in the acute postoperative period (ALIF-PSF 2) and 10 of which (sa-ALIF 2 and ALIF-PSF 8) were chronic (>6 months). The superficial wound infections were in the ALIF-PSF cohort. Of the 8 patients with persisting back and lower extremity pain, only 1 patient required revision surgery for nerve root decompression. This reoperation was not due to the failure of the ALIF cage. No patients experienced retrograde ejaculation. There were no vascular complications.
Adverse events to final follow-up.
Discussion
This retrospective cohort study was conducted over the past decade to evaluate whether sa-ALIF is effective for the treatment of low-grade IS, avoiding the added cost and morbidity of posterior fixation. In our study, we reported a shorter mean follow-up time in the sa-ALIF cohort (2.1 years) vs ALIF-PSF (3.9 years). This was accounted for by the availability of integrated cage-plate-screw fixation in the sa-ALIF group from 2018 and a change in surgeon preference, away from potentially unnecessary PSF.
The majority of ALIF-PSF patients received rhBMP-2 compared with the sa-ALIF cohort where the majority received DBA. This was accounted for by the regulatory withdrawal of rhBMP-2 in March 2020 in Australia. Despite the difference in biological use between the sa-ALIF and ALIF-PSF, there were no significant differences in CT interbody fusion rates between the 2 cohorts.
Clinical Outcomes
In our study, both sa-ALIF and ALIF-PSF had significant improvements in all PROMs from baseline to final follow-up. ALIF with posterior fixation has been reported as effective in improving patients’ PROMs.6,7,20–23 Few studies have reported PROMs for sa-ALIF.13–15
VAS leg scores were significantly lower in the sa-ALIF cohort both preoperatively and 6 weeks postoperatively. This may be partially attributed to heterogeneity in patient demographics, as the sa-ALIF group had lower BMIs, fewer smokers, and no cases of Meyerding grade II. The added morbidity from posterior fixation may also contribute to the higher VAS leg scores and lower SF-12 physical component summary scores in the ALIF-PSF cohort at 6 weeks postoperatively. No other statistical differences were observed between the 2 cohorts across the recorded timepoints. This suggests, in appropriately selected patients, that sa-ALIF is effective in treating IS and avoiding the associated disadvantages of the additional instrumentation.
Mean decision regret scores were extremely low in both cohorts. This may reflect our study’s low number of workers’ compensation patients (n = 1), who are associated with lower postoperative satisfaction (RR = 2.10) according to a meta-analysis from 2021.24
Sa-ALIF Outcomes
Aunoble et al13 presented 20 adults with low-grade spondylolisthesis with a similar mean follow-up (2.2 years) compared with our study (2.1 years). In their study, comparing preoperative PROMs to final follow-up, ODI scores decreased from 57% (28.5) to 21% (10.5), VAS back pain decreased significantly from 6.5 to 2.7, and VAS leg decreased from 6.2 to 3.4. Our study demonstrated superior improvements in VAS leg with similar improvements in ODI and VAS back.
Kim and Lee14 presented outcomes of 40 patients with low-grade IS (sa-ALIF 20, posterolateral fusion + PSF 20) and conducted from 1977 to 1994 with an average follow-up of 3.6 years. In the sa-ALIF group, 17/20 patients had excellent or good outcomes, supporting the use of sa-ALIF for low-grade IS.
Likewise, a recent study by Jesse et al15 of 34 patients who received sa-ALIF for low-grade IS at L5/S1 reported 12-month postoperative PROMs (VAS back 1.9, VAS leg 1.7, ODI 10.2) that were similar to our findings.
A systematic review that reported PROMs following sa-ALIF for varying indications showed similar improvements in VAS back (7–2.9) and inferior improvements in VAS leg (5.6–2.3) and ODI (26.1–12.5) postoperatively.25
Our results suggest a clinical benefit of using sa-ALIF in IS, consistent with the positive results previously reported in the literature.
ALIF-PSF Outcomes
Studies comparing ALIF-PSF to T/PLIF for IS have shown that ALIF-PSF is safe and effective for low-grade IS.20–23 Ould-Slimane et al21 compared ALIF with posterior fixation to posterior approaches (transforaminal lumbar interbody fusion [TLIF]/PLIF). Compared with posterior approaches, circumferential fusion provided greater improvements in VAS leg, VAS back, ODI, and SF-12 physical component score at mean 46-month follow-up. However, a systematic review by Alhammoud et al20 with a total of 397 patients with IS (198 ALIF-PLF, 199 TLIF/PLIF + PLF) found no significant difference in clinical outcomes or fusion rates between combined anterior-posterior approaches and posterior-alone approach.
Likewise, Prost et al22 investigated 89 patients with IS who received ALIF-PSF (n = 71) vs TLIF (n = 18), and Kim et al23 reported 78 patients who received circumferential ALIF (n = 46) vs TLIF (n = 32). Both reported improvements in VAS back and VAS leg comparable to our study.
Adverse Events
Anterior retroperitoneal approaches are associated with complications including incisional hernias, ileus, retrograde ejaculation, and vascular injury,26–28 while posterior approaches risk paraspinal muscle denervation, neurological injury, dural tears, hardware failure, and nonunion.28–30
There are concerns regarding the morbidity associated with supplemental posterior fixation in ALIF. However, a recent multicenter retrospective cohort study of 1377 ALIF patients found no significant difference in adjacent segment disease rates between sa-ALIF and ALIF with posterior fixation.9 Our complication rate for sa-ALIF was 9% which is comparable to literature reports, ranging from 10% to 35%.14,15,25,31 But our complication rate for ALIF-PSF was 34%, higher than reported rates of 4.2% to 18.6%21,22,32 accounted for by our inclusion of persisting mechanical and lower extremity pain, not included in most other studies.
The higher rates of complications seen in our ALIF-PSF cohort may be attributed to morbidity associated with posterior fixation, supporting sa-ALIF for appropriately selected patients. Heterogeneity between the sa-ALIF and ALIF-PSF cohorts may also influence this discrepancy.
Radiographic Outcomes
Reported interbody fusion rates for ALIF-PSF range from 88% to 100%,21,23,32,33 higher than sa-ALIF fusion rates, which range from 60% to 95%,13–15,34,35 supported by a recent multicenter retrospective review of 1377 IS patients,9 reporting nonunion rates of 2.4% for sa-ALIF vs 0.5% for ALIF-PSF.
The nonunion rates in our study were also comparatively low, with high fusion rates in both cohorts with no significant difference between sa-ALIF (81.8%) vs ALIF-PSF (92.0%). No patients in the sa-ALIF group needed subsequent supplemental posterior fixation. The trend to higher and earlier fusion rates found in our ALIF-PSF cohort may be secondary to the added stability of the PSF construct.
Disc height was significantly better at 12-month follow-up in both cohorts, which was not the case for segmental lordosis or the degree of anterolisthesis. It is unclear if these radiological outcomes impact the clinical findings. Studies on IS patients have reported greater increases in segmental lordosis in their sa-ALIF25 and ALIF-PSF cohorts.6,22,32 Reasons for this are multifactorial and may include varying surgical techniques, noting that in this study, a 15° lordotic cage was used. The mean increase in disc height postoperatively in our sa-ALIF cohort (4.7 mm) and ALIF-PSF cohort (3.8 mm) is consistent with literature reports on sa-ALIF25 and ALIF-PSF (3–8.7 mm).6,22,32,36 In this study, both cohorts experienced a nonsignificant reduction in anterolisthesis. This is consistent with some literature reports22,25 and not others.6,32,36 This discrepancy may reflect alternate surgical technique or the greater degree of anterolisthesis seen in some cohorts.
At the 12-month final follow-up, there were no significant differences between the cohorts in radiographic scores. This suggests that the addition of pedicle screws to and ALIF construct may not enhance the final radiographic outcomes.
Cost
Our study demonstrates comparable clinical outcomes and fusion rates between sa-ALIF and ALIF-PSF for low-grade IS spondylolisthesis. The avoidance of supplemental posterior fixation reduced patient morbidity and cost. Studies report up to a 22% increase in cost for supplemental posterior fixation with Goz et al reporting the average cost for ALIF as $75,872 compared with $92,249 in ALIF with posterior fixation.37 We recently published mean operative charges of AUD$2500 per hour.38 Quoted in this study, the average cost of our single-level sa-ALIF was AUD$25,053. The cost of posterior fixation would approximate to AUD$6644 for the implants and AUD$3750 for an additional 90 minutes of operative time on average.
The difference in the cost of each bone graft (rhBMP-2 and DBA) is small, with the DBA costing AUD$6193 per 8.5 mg used and rhBMP-2 costing AUD$6000 per 8.4 mg used (in 2014).
Strengths and Limitations
This was a retrospective analysis of prospectively collected data with a limited sample size. Cohorts were compared in a nonrandomized fashion. All operations were conducted by a consultant spine surgeon at a single center. These data were collected over a 12-year period, which adds unavoidable heterogeneity to the surgical technique. We note that the sa-ALIF surgeries were performed more recently than the group of ALIF-PLF patients. Additionally, most ALIF-PSF patients received rhBMP-2, while most sa-ALIF patients received DBA due to a regulatory change. It would be prudent to follow up with this DBA cohort long term to assess concerns such as infection risk. Further randomized, controlled, and larger comparisons between sa-ALIF and ALIF-PLF are needed to definitively evaluate the statistical difference in clinical and radiographic outcomes.
Conclusion
In appropriately selected patients with normal bone density, sacral slope, and a BMI <35, sa-ALIF is a safe and effective treatment option for grade I IS without the need for supplementary posterior fixation. The additional morbidity and cost of PSF may not be justified given the satisfactory clinical and radiographic outcomes of sa-ALIF for grade I IS.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures All authors have completed the ICMJE uniform disclosure form. G.M.M. has disclosures of Globus Medical (consultancy), Device Technologies (travel), Life Healthcare (consultancy, travel), Australian Biotechnology (consultancy), National Surgical (travel), Medtronic (consultancy), and SeaSpine (travel).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.