


Abstract
Background The biomechanical behavior of total disc replacement (TDR) and anterior cervical discectomy and fusion (ACDF) incomplex multiplanar motion is incompletely understood. The purpose of this study was to determine whether ACDF or TDR significantly affects in vitro kinematics through a range of complex, multiplanar motions.
Methods Seven human cervical spines from C4-7 were used for this study. Intact cervical motion segments with and without implanted TDR and ACDF were tested by use of unconstrained pure bending moment testing fixtures in 7 mechanical modes: axial rotation (AR); flexion/extension (FE); lateral bending (LB); combined FE and LB; combined FE and AR; combined LB and AR; and combined FE, LB, and AR. Statistical testing was performed to determine whether differences existed in range of motion (ROM) and stiffness among spinal segments and treatment groups for each mechanical test mode.
Results ACDF specimens showed increased stiffness compared with the intact and TDR specimens (P < .001); stiffness was not found to be different between TDR and intact specimens. ACDF specimens showed decreased ROM in all directions compared with TDR and intact specimens at the treated level. For the coupled motion test, including AR, LB, and FE, the cranial adjacent level (C4/C5) for the intact specimens (2.7°) showed significantly less motion compared with both the TDR (6.1°, P = .009) and ACDF (6.8°, P = .002) treatment groups about the LB axis. Testing of the C4/C5 and C6/C7 levels in all other test modes yielded no significant differences in ROM comparisons, although a trend toward increasing ROM in adjacent levels in ACDF specimens compared with intact and TDR specimens was observed.
Conclusions This study compared multiplanar motion under load-displacement testing of subaxial cervical motion segments with and without implanted TDR and ACDF. We found a trend toward increased motion in adjacent levels in ACDF specimens compared with TDR specimens. Biomechanical multiplanar motion testing will be useful in the ongoing development and evaluation of spinal motion–preserving implants.
Anterior cervical discectomy and fusion (ACDF) comprise a common surgical treatment for degenerative disc disease involving the cervical spine. Despite excellent short- and long-term clinical results, concern about the development of adjacent-segment disease (ASD) has prompted a surge in the development of motion-sparing treatments, such as total disc replacement (TDR).1–13 Numerous biomechanical, radiographic, and clinical reports have confirmed the increased rate of ASD and altered adjacent- level kinematics in patients treated with ACDF.1–6 Hilibrand et al3 reported an ASD rate of 2.9% per year after fusion, and Baba et al4 found that new dynamic spinal canal stenosis had developed in 25% of patients after a mean 8.5-year follow-up.
Several theories have been proposed regarding the development of ASD after ACDF, including the development of compensatory motion and load in adjacent segments to achieve motion and alignment similar to preoperative levels. Whereas biomechanical and radiographic differences between ACDF and TDR have been identified, clinical outcomes and patient satisfaction remain similar,13–15 although some emerging evidence has indicated that TDR may show clinical benefit over ACDF over longer-term follow-up.16
Although TDR maintains motion and may preserve more “natural” kinematics at the surgical and adjacent levels, there are several reasons why ACDF continues to remain the more widely used method of treatment. Whereas ACDF has been used for decades with positive results, the use of TDR in the cervical spine is a relatively new approach, with a comparative lack of long-term data on factors such as the accumulation of wear debris, fatigue failure, and heterotopic ossification.17–19 Previous studies have shown that TDR may not completely restore native motion parameters because of loss of lordotic alignment and variations in the center of rotation,6, 20, 21 although conflicting evidence indicates that TDR may closely simulate intact motion.6
In vivo and in vitro studies have been performed to analyze the differences in cervical kinematics and kinetics in the setting of ACDF and TDR; however, most of these studies have observed simple arcs of motion in a single plane (flexion-extension or lateral bending).6, 20 A previous investigation has examined complex, multiplanar motion of the lumbar spine,22 but a similar study has not been performed in the cervical spine with implanted TDR and ACDF. Examining multiplanar motion may provide an improved understanding of in vivo behavior of spinal motion–preserving implants. The objective of this study was to determine whether ACDF or TDR significantly affected in vitro kinematics compared with the intact human cervical spine through a range of complex, multiplanar motions.
Methods
Seven human cervical spine specimens were used for this study. The mean age of the specimens was 61.4 ± 13.8 years. Each specimen was radiographically screened for anatomic defects or prior surgery before initiation of the study. The specimens were maintained in a freezer at −20°C until approximately 24 hours before testing. They were thawed to room temperature, and all residual musculature was removed by careful dissection. Care was taken to preserve all ligamentous attachments. Throughout preparation and testing, the specimens were kept moist with a wrapping of saline solution–soaked gauze. For each spine, the C4-7 segment was used for potting. The cephalad and caudad vertebrae were rigidly embedded in a urethane potting compound (Smooth On, Easton, Pennsylvania). The segments were potted so that the mid plane of the central (C5/C6) disc space was horizontal.
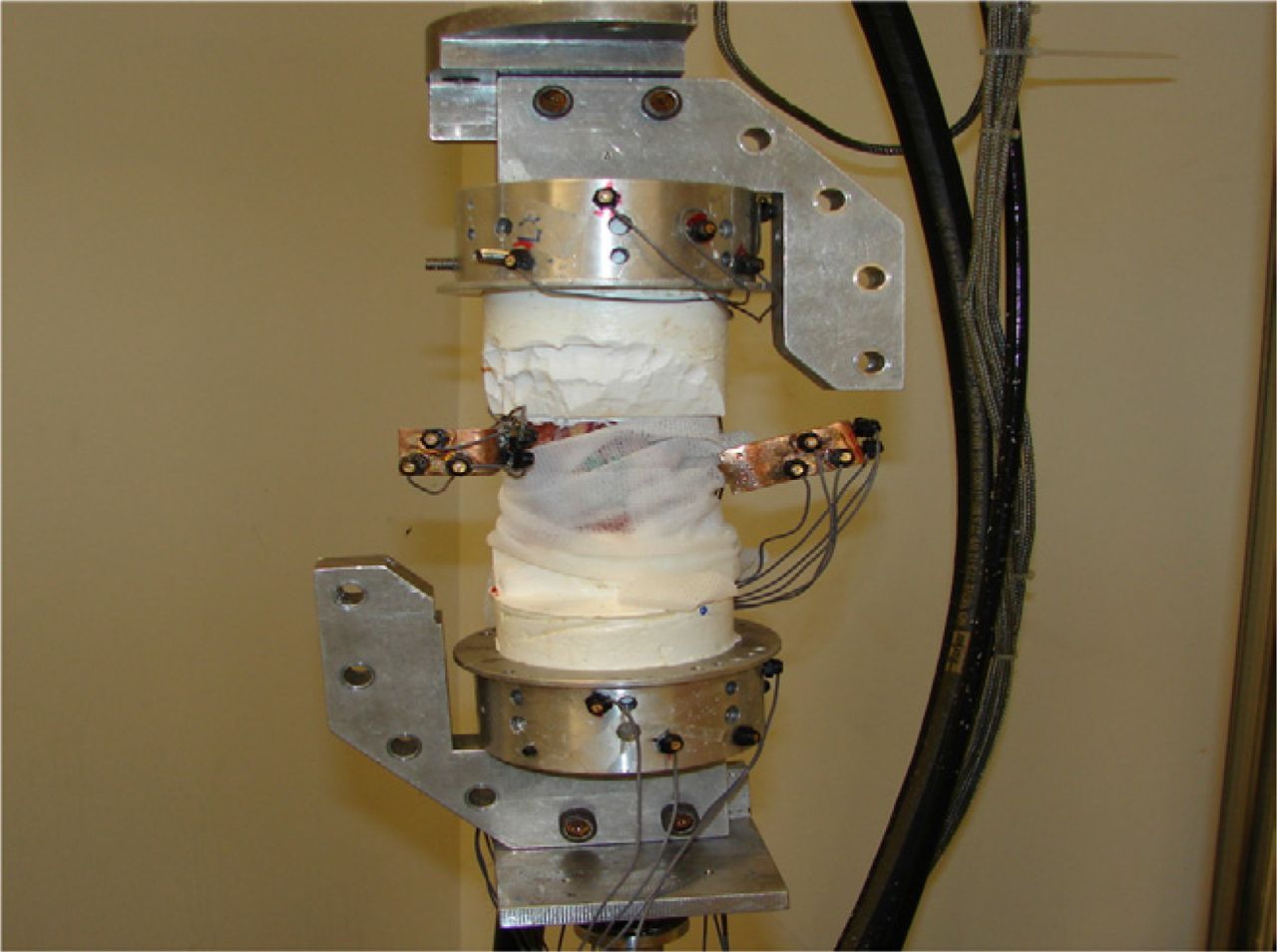
The cervical motion segments were tested by use of a standard flexibility protocol with custom, unconstrained fixtures in an Instron 8521S servohydraulic load frame (Instron Corp., Canton, Massachusetts) (Fig. 1). The 7 mechanical test modes were as follows: left and right axial rotation (AR); flexion/extension (FE); left and right lateral bending (LB); combined FE and LB; combined FE and AR; combined LB and AR; and combined FE, LB, and AR.22 For the intact cases, moments of 0 ± 1.5 Nm were applied sinusoidally at a constant frequency of 0.1 Hz for a total of 6 cycles. The relative 3-dimensional motion of the C4, C5, C6, and C7 vertebral bodies was measured by an OptoTrak motion tracking system (Northern Digital, Waterloo, Ontario, Canada), and these data were synchronized with the load/moment data from the Instron electronics. To determine global changes in motion, the relative difference in position among the C4/C5, C5/C6, and C6/C7 vertebral bodies was analyzed along the applied motion axes. Range of motion (ROM) was calculated as the total rotation along the axis of interest for the same cycle. Subsequent treatments were tested in displacement (rotation) control by use of a hybrid testing protocol. For the hybrid protocol, the intact ROM was calculated and the 2 treatment groups were displaced until the total ROM equaled that of the intact specimen.
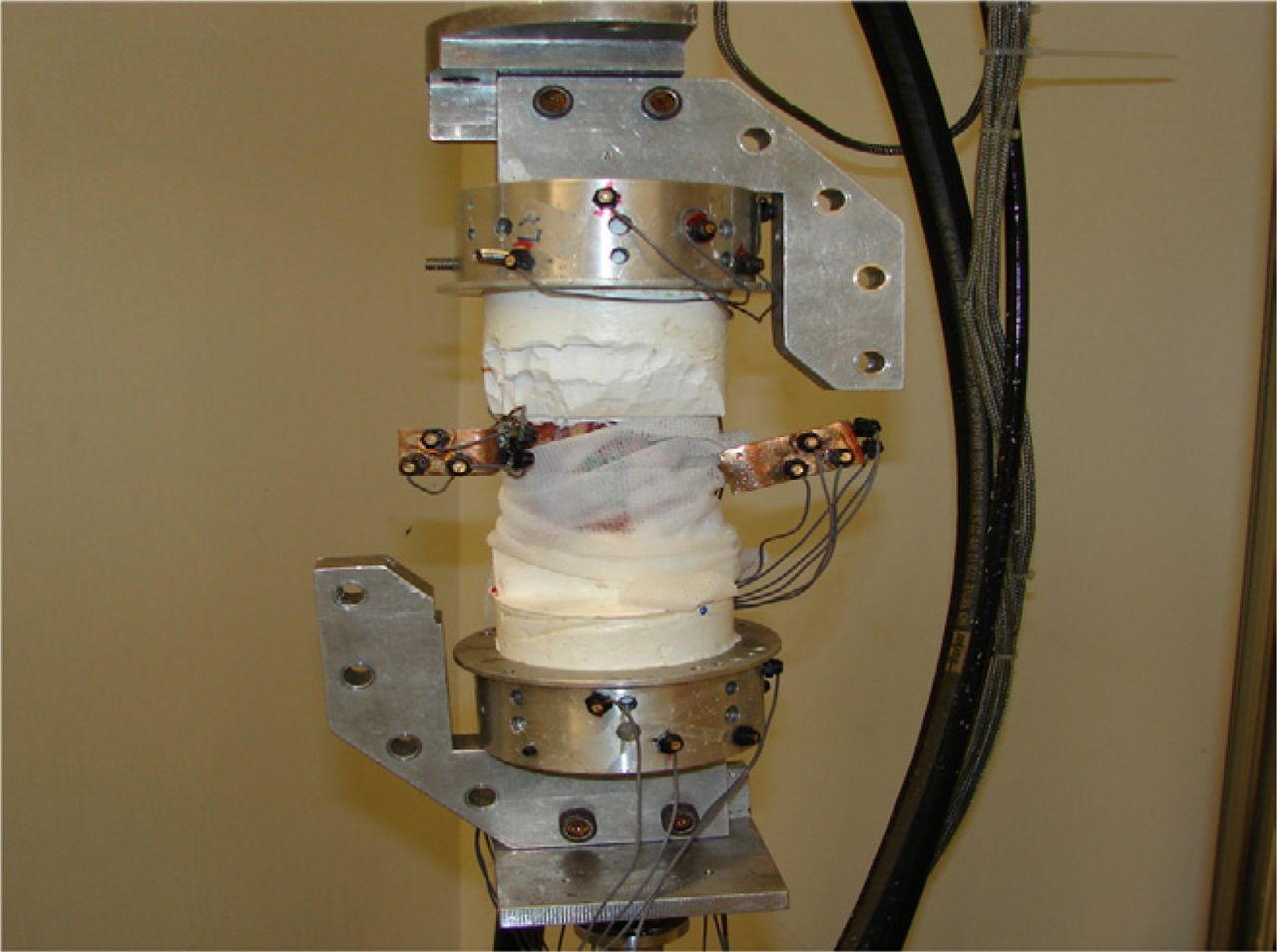
Test apparatus in combined FE-AR test mode.
After testing of intact specimens, a Globus Medical Secure Cervical TDR (Globus Medical, Inc., Audubon, PA) was placed at the C5/C6 level according to the manufacturer's instructions, and specimens were retested under the same testing protocol. On completion of TDR testing, a simulated ACDF was performed with the Globus Medical Assure anterior plating system along with a rigid interbody spacer, and again, specimens were tested using the same testing protocol.
A 2-factor repeated-measures analysis of variance (ANOVA) was performed to determine whether significant differences existed in ROM among spinal segments and treatment groups for each mechanical test mode. In all cases the level of statistical significance was set to .05 a priori. A Holm-Sidak post hoc test was performed to identify statistical significance between variables.
Results
Kinematics of treated C5/C6 level
In the FE test mode (P = .011, ANOVA), the ACDF treatment group exhibited significantly less motion (6.6° ± 4.0°) at the treatment level compared with the intact group (10.5° ± 4.4°, P < .001) and the TDR group (9.2° ± 2.9°, P = .014) (Fig. 2A). In the AR test mode (P = .006, ANOVA), the ACDF (4.7° ± 3.0°, P < .001) and TDR (5.9° ± 2.7°, P = .028) treatment groups showed significantly less motion at the treatment level compared with the intact group (7.6° ± 3.1°) (Fig. 2B). In coupled motion consisting of FE with LB (P = .006, ANOVA), the ACDF treatment group (2.9° ± 1.9°) exhibited significantly less motion compared with both the intact (7.1° ± 3.6°) and TDR (6.5° ± 3.8°) groups about the FE axis of rotation (P < .001 for both comparisons) (Fig. 2C). Specimens treated with ACDF showed statistically less motion compared with intact specimens with regard to motion along the FE axis in the AR and FE coupled motion test mode (2.7° ± 2.4° vs 6.8° ± 3.6°, P = .003). Within the ACDF treatment group, for FE with LB coupled motion, the treated level (C5/C6) exhibited significantly less motion (2.9° ± 1.9°) compared with the cranial adjacent levels (7.3° ± 3.4°, P = .004) and caudal adjacent levels (8.0° ± 4.0°, P = .012) about the FE axis.
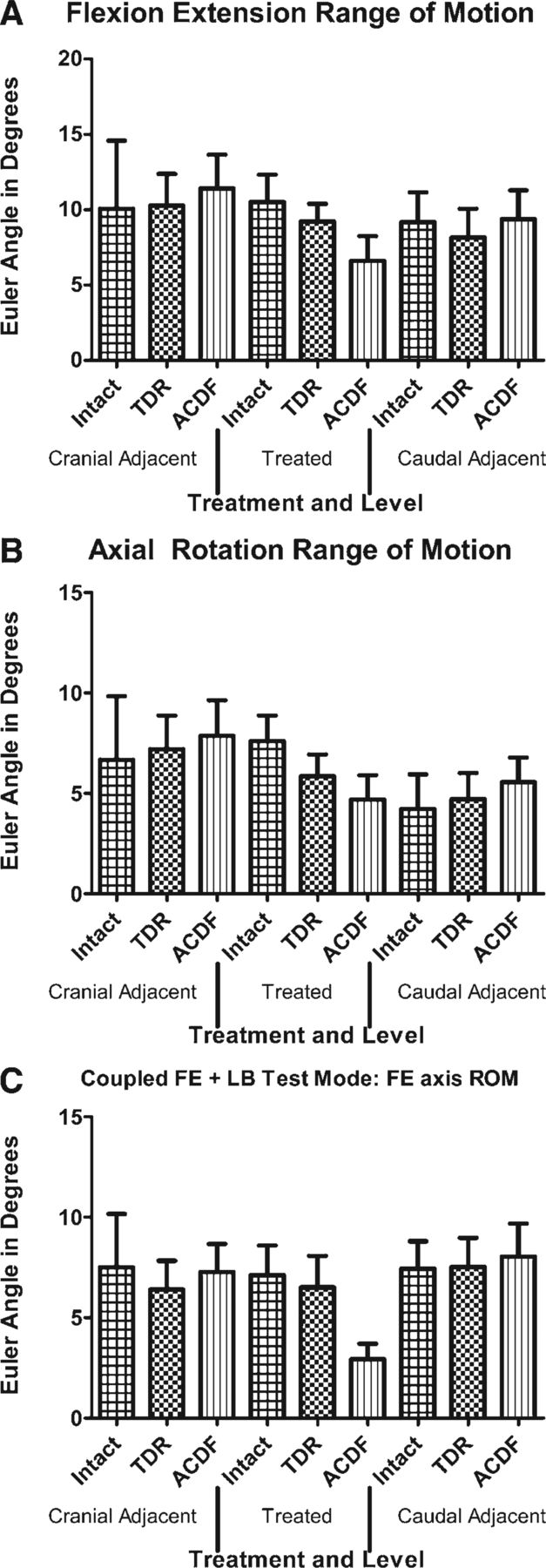
(A) ROM data for FE test mode. (B) ROM data for AR test mode. (C) ROM data for coupled FE-LB mode.
Kinematics of cranial adjacent level (C4/C5)
For the tests performed in FE, the mean ROM at the cranial adjacent level (C4/C5) was 10.1° ± 4.5° for the intact specimens. ROM did not increase with TDR (10.3° ± 5.2°) and increased by 1.3° (11.4° ± 4.5°) in specimens treated with ACDF; significant differences were not found (P = .188) (Fig. 2A). For LB, mean ROM at the cranial adjacent level was 8.0° ± 5.2° for the intact group and increased by approximately 1.5° (TDR, 9.5° ± 6.8°; ACDF, 9.6° ± 6.2°) for each treatment group (P = .272). AR showed mean ROM at C4/C5 of 6.7° ± 3.2° for intact specimens, 7.2° ± 4.1° for those treated with TDR, and 7.9° ± 4.4° for those treated with ACDF (P = .374) (Fig. 2B). For the coupled motion test including AR, LB, and FE, the cranial adjacent level (C4/C5) for the intact specimens (2.7° ± 2.1°) showed significantly less motion compared with both the TDR (6.1° ± 4.8°, P = .009) and ACDF (6.8° ± 4.7°, P = .002) treatment groups about the LB axis (Fig. 2C).
Kinematics of caudal adjacent level (C6/C7)
At the caudal adjacent level (C6/C7), the mean FE ROM was 9.2° ± 4.9° for intact specimens, 8.2° ± 4.7° for those treated with TDR, and 9.4° ± 4.7° for those treated with ACDF about the primary axis of motion (P = .159) (Fig. 2A). In LB the mean ROM was 5.6° ± 4.4° for intact specimens. ROM did not increase (5.8° ± 3.8°) with TDR and was 6.6° ± 3.9° in specimens treated with ACDF (P = .533). Tests performed in AR produced mean ROM of 4.2° ± 4.2° for intact specimens, 4.7° ± 3.2° for those treated with TDR, and 5.6° ± 3.0° for those treated with ACDF (P = .132) (Fig. 2B). All other test modes yielded no significant differences in ROM comparisons.
Stiffness summary
The mean stiffness for the FE test mode at the treated level (C5/C6) was 0.34 ± 0.18 Nm per degree for intact specimens, 0.36 ± 0.13 Nm per degree for those treated with TDR, and 0.94 ± 0.71 Nm per degree for those treated with ACDF. ACDF treatment significantly increased stiffness compared with both intact and TDR specimens at the treated level in the FE test mode (P < .001 for both). For the FE with LB test mode, the mean stiffness was 0.58 ± 0.43 Nm per degree for intact specimens, 0.56 ± 0.26 Nm per degree for specimens treated with TDR, and 1.63 ± 0.92 Nm per degree for specimens treated with ACDF; ACDF treatment significantly increased stiffness compared with intact and TDR specimens at the treated level (P < .001 for both). Stiffness values between treatment groups in all other test modes yielded non–statistically significant differences.
Discussion
This study compared multiplanar motion under loaddisplacement testing of subaxial cervical motion segments with and without implanted TDR and ACDF. We found that TDR specimens exhibited significantly more motion at the level of reconstruction compared with ACDF specimens in FE testing and coupled motion testing, but there was no significant difference in AR, although substantial motion in the ACDF group was observed. We also described the complex, multiplanar motion of the cranial and caudal adjacent levels with and without implanted ACDF and TDR.
Our objective was to determine whether biomechanical differences existed between reconstruction techniques about multiple directions of motion. ACDF statistically significantly increased stiffness at the level of reconstruction (C5/ C6) compared with intact specimens and specimens with implanted TDR for FE and for FE with LB. Though not statistically significant in other test modes, stiffness values after ACDF treatment were generally more than twice as high compared with the intact and TDR treatment. A larger sample size may potentially indicate more statistically significant differences in specimens treated with ACDF compared with TDR and intact specimens.
For AR, the cranial and caudal adjacent levels showed increased motion, though not significantly, for both the TDR and ACDF interventions compared with the intact specimens, with the most motion observed in the ACDF specimens. There is currently no definitive evidence that increased adjacent-segment motion leads to ASD, although clinical studies have found increased levels of ASD after ACDF. In addition, the development of ASD may be a function of the natural history of spondylotic disease. In a clinical study examining adjacent segments after TDR or ACDF, Kim et al7 reported that at a mean of 19 months after surgery, ACDF patients were 3.5 times more likely to have radiographic adjacent-segment degeneration on radiographic examination than TDR patients, although the patients did not show differences in symptomatology. Whether radiographic adjacent-segment degeneration is less common in TDR patients than in ACDF patients long-term will be determined by studies with longer follow-up.
Comparing our results with clinical data yields interesting observations. Differences in motion at adjacent segments has been examined at 12 months’ follow-up in 454 patients undergoing either ACDF or TDR by Park et al,6 who showed no change in ROM at adjacent segments for TDR patients but significantly increased FE motion at the cranial adjacent level after ACDF. In our study we found the ROM of the cranial adjacent segments of intact specimens to be 10.1°, which increased to 11.4° after ACDF. Although the difference was not significant in our study, our values closely match the values reported by Park et al of 9.6° before ACDF and 11.0° after ACDF, supporting the validity of our methods and results.
We did not use an axial preload (follower load) for testing in this experiment. Previous studies suggest that the application of a cervical follower load decreases motion, bending moments, and shear forces of functional spinal units.23, 24 If we used a follower load, our results may have been more clinically relevant, although the biomechanical differences between ACDF and TDR would likely decrease. We chose to perform testing with more aggressive bending moments and shear forces to provide a rigorous basis for comparison.
The motion found through the “fused” segment of the ACDF samples ranged from 2° to 8° depending on the plane of motion. Hypothetically, a fused segment should have no motion; thus the motion observed in this study may represent incomplete “fusion” of the motion segment (time 0 test), motion of the sensor-specimen interface, or variability in sizing the graft for ACDF. Specifically, motion in the ACDF group may be attributed to the wooden dowel rigid interbody spacer used. On the basis of the motion detected in this study, we may have undersized the grafts. A wedged graft may have provided a more complete fusion.24 Another possible explanation for the motion may be the fact that the ACDF group was tested after intact and TDR testing. With a small sample size, we wanted to perform a repeatedmeasures test to obtain the highest statistical power within this small group, yet repeated testing may have damaged the specimens. Similarly, the effect of the keel in the endplates from TDR may have provided a surface difficult to match with the fusion block and thus allowed some motion. Performing posterior stabilization may have reduced the motion at the ACDF segment. The accuracy of the OptoTrak system is validated and was not likely to be the source of variation.
The differences in motion found between intact specimens and those treated with TDR may be due to resection of small osteophytes that limit ROM. The tested cadaveric specimens used in this study had a mean age over 61 years, which may not represent the optimal age for patients receiving cervical TDR because of the extent of spondylosis in this age group.
One limitation of this study was the relatively small sample size. Although this study may have been underpowered to find significant differences in motion, it does describe a useful protocol for investigating multiplanar motion in the cervical spine, and our findings—though not statistically significant—are of interest. Future research may investigate multiplanar motion in living patients with implanted TDR versus ACDF. In addition, studies performed using different TDR designs and other motion-preserving technology may lead to different motion patterns in adjacent- segment motion. In this study we tested only the subaxial spine and did not include the axial spine or skull. This testing protocol may thus be an unnatural motion situation because compensatory motion in living patients may also occur at the occipital-cervical and atlanto-axial joints, yet testing the entire cranial-cervical motion segment is a technical challenge.
This study analyzed complex multiplanar motion of intact specimens and adjacent levels as compared with specimens with implanted TDR and ACDF. We found significantly increased stiffness of the ACDF versus TDR specimens at the treated level, as well as a trend toward an increase in ROM at the adjacent levels in ACDF specimens compared with intact specimens and specimens with implanted TDR.
Footnotes
Globus Medical, Inc., provided funding for this study.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.