


ABSTRACT
Background: In 2014, inpatient spinal fusion surgery had the highest aggregate cost of any inpatient surgery performed in the United States, costing 12 billion dollars. As the national health care system seeks to improve value-based care, there is increased motivation to perform surgery on an outpatient basis. To ensure improved patient outcomes with this transition, patient selection has become increasingly important to identify who would most benefit from outpatient spine fusion, for example. This demands an improved understanding of the demographics of patients who have been receiving outpatient spine fusion on which the spine surgery community can build to improve cost-effective care delivered.
Methods: The Healthcare Cost and Utilization Project, State Ambulatory Surgery Databases, and Agency for Healthcare Research and Quality databases were queried for demographic data regarding all-cause outpatient spine surgery between 2012 and 2014. Outpatient surgery volume was compared with inpatient surgery volume—which was provided by the State Inpatient Databases.
Results: A total of 1,164,040 spine fusion procedures were identified between 2012 and 2014, of which 132,900 procedures were performed as outpatient surgery (11.4%). Of all fusion procedures amongst 18- to 44-year-old patients, 18.4% were outpatient. A larger proportion of white patients, rather than black or Hispanic patients, underwent ambulatory procedures (12.14% vs 9.53% vs 7.46%, respectively); 16.54% of spinal fusion procedures for patients with private insurance was performed on an outpatient basis. Based on patient income, 76% of all outpatient fusions were performed on patients who live in “not low” income ZIP codes.
Conclusions: There has been a gradual trend toward performing more outpatient spinal fusion procedures over the studied period. This study has also revealed unique trends in the demographics of patients who have received outpatient spine fusion during this time.
Level of Evidence: 3.
INTRODUCTION
Cervical and lumbar spinal fusion may be indicated for a number of diagnoses including the following: cervical spondylotic myelopathy, cervical radiculopathy, lumbar spinal stenosis, lumbar spondylolisthesis, scoliosis, and spinal fractures.1,2 Several lumbar fusion techniques, for example, have been shown to be safe when performed in an outpatient basis including the following: anterior lumbar interbody fusion, transforaminal lumbar interbody fusion, lateral lumbar interbody fusion, and posterior lumbar interbody fusion.3 These are performed using minimally invasive surgery (MIS) techniques. The potential benefits of MIS include the following: less muscle disruption, decreased blood loss, shorter hospital stay, decreased surgical site infections, and more cosmetically appealing surgical incisions.3 Additionally, anterior cervical discectomy and fusion (ACDF) has also been safely performed in an outpatient setting given that strict criteria are maintained to identify appropriate candidates for outpatient spinal fusion.4 Surgeons may recommend an outpatient spinal fusion for younger patients who have a body mass index less than 35, no medical comorbidities, and an adequate support network.5 The increase in outpatient spinal fusion may help to decrease health care expenditures in all-cause adult spinal fusion surgery.
Although previous studies have identified that outpatient spinal fusion procedures are increasing in the United States, very few have described the demographics of the patients undergoing this procedure.6,7 These data address gaps in the literature and provide demographics on patients who underwent outpatient spine fusion between 2012 to 2014. For example, certain patient factors, such as younger age, have been associated with early postoperative discharge after outpatient MIS.5 Thus, a better understanding of the demographic breakdown of these patients may improve our predictive ability to identify prospective discharge times. Further, it will allow surgeons and health care teams to provide more personalized care. Additionally, our findings may aid health care professionals and policy makers in providing further insight on important population variables associated with the growing presence of outpatient spinal fusion.
MATERIALS AND METHODS
Data Source
Data were collected from the corresponding State Ambulatory Surgery Database (SASD) from the Healthcare Cost and Utilization Project (HCUP) and the Agency for Healthcare Research and Quality (AHRQ) between 2012 and 2014. These ambulatory surgery statistics are totals of all surgeries in state databases and do not represent national estimates. In total, the data comprise approximately two-thirds of the US population across 29 states. In the current study, the terms “ambulatory” and “outpatient” are used interchangeably as defined by HCUP.
Patient Selection and Characteristics
A combination of SASD information from HCUP and AHRQ databases were queried for spinal fusion from 2012 to 2014 using the Clinical Classification Software (CCS) code 158 for spinal fusion. There were no additional exclusion criteria for patients.
Demographic and economic data were obtained for outpatient spinal fusion surgeries between the ages 1 and 85. Insurance types included Medicare, Medicaid, private, self-pay, and other. The “other” category included worker's compensation, TRICARE/CHAMPUS, CHAMPVA, Title V, and other government programs. The number of annual surgeries, sex of patient, patient race and ethnicity, patient age, insurance type, median income of patient ZIP code, and patient residence were all recorded. Median income of patient ZIP code includes the categories “low income” and “not low income.” Low income is defined as the lowest earning quartile of Americans for that year. Patient race and ethnicity was defined as white, black, Hispanic, Asian/Pacific Islander, Native American, or other. These data were acquired by comparing annual average data that were acquired from the aforementioned databases. Standard error analysis was used to determine if data were reliable. All data reported had standard error below 0.3 to confirm reliability.
Incidence was determined by comparing the volume of cases to the US population by using population values provided by the US Census Bureau.
The SASD, HCUP, and AHRQ databases are all de-identified and were therefore deemed exempt by our institutional review board.
Source of Funding
No funding was necessary for completion of this study as the SASD, HCUP, and AHRQ databases are all publicly available.
RESULTS
An estimated 1,164,040 spinal fusions were completed between 2012 and 2014 across 29 states included in the SASD. Over this period 132,900 spinal fusions were completed in an outpatient setting. In 2012, 11% of all spinal fusions were performed in an ambulatory setting. This increased to 12% in 2014 (Table 1).
Annual number of spinal fusion surgeries in the United States between 2012 and 2014.
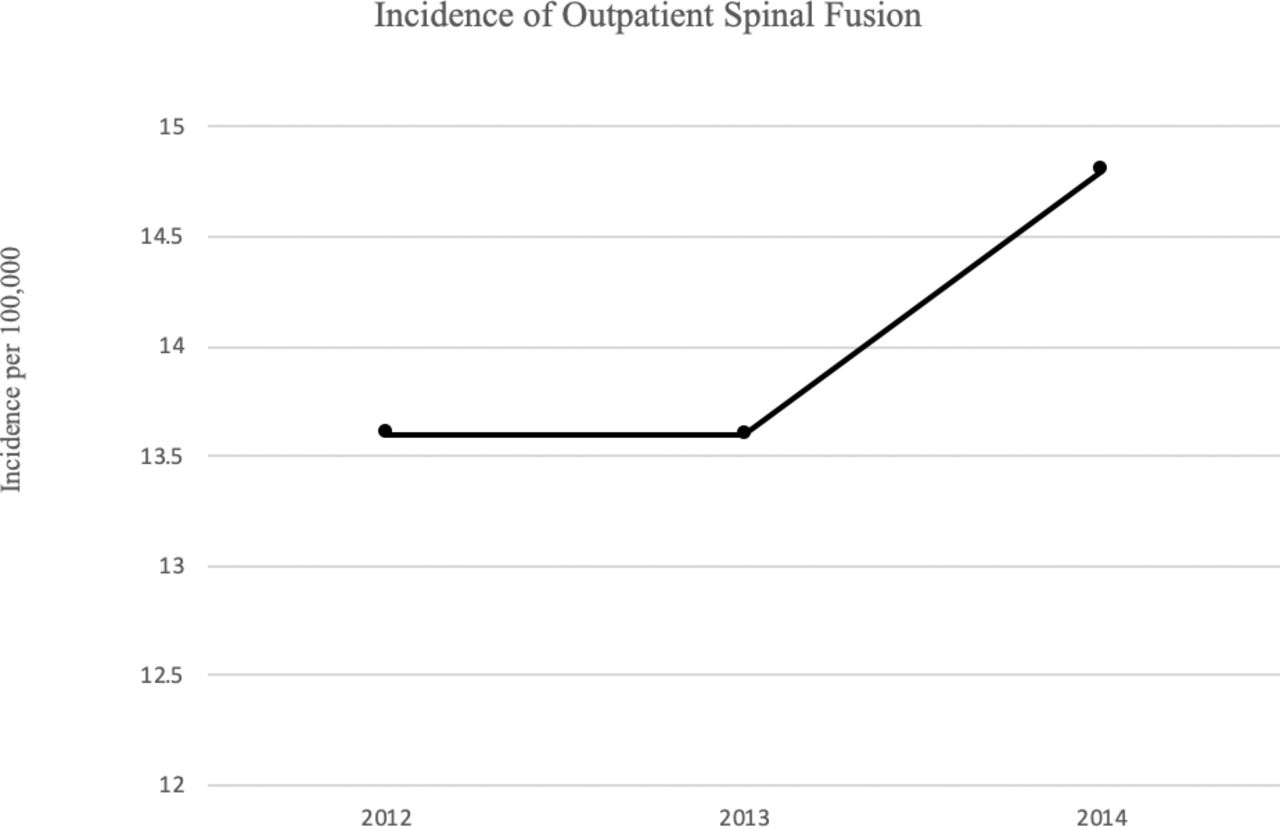
The incidence of outpatient spinal fusion in the United States for 2012 and 2013 were the same at 13.6 per 100,000 people. In 2014, incidence increased nearly 10% to 14.8 per 100,000 people (Figure 1).

Incidence of outpatient spinal fusion per 100,000 people based on US population estimates from the US Census Bureau.
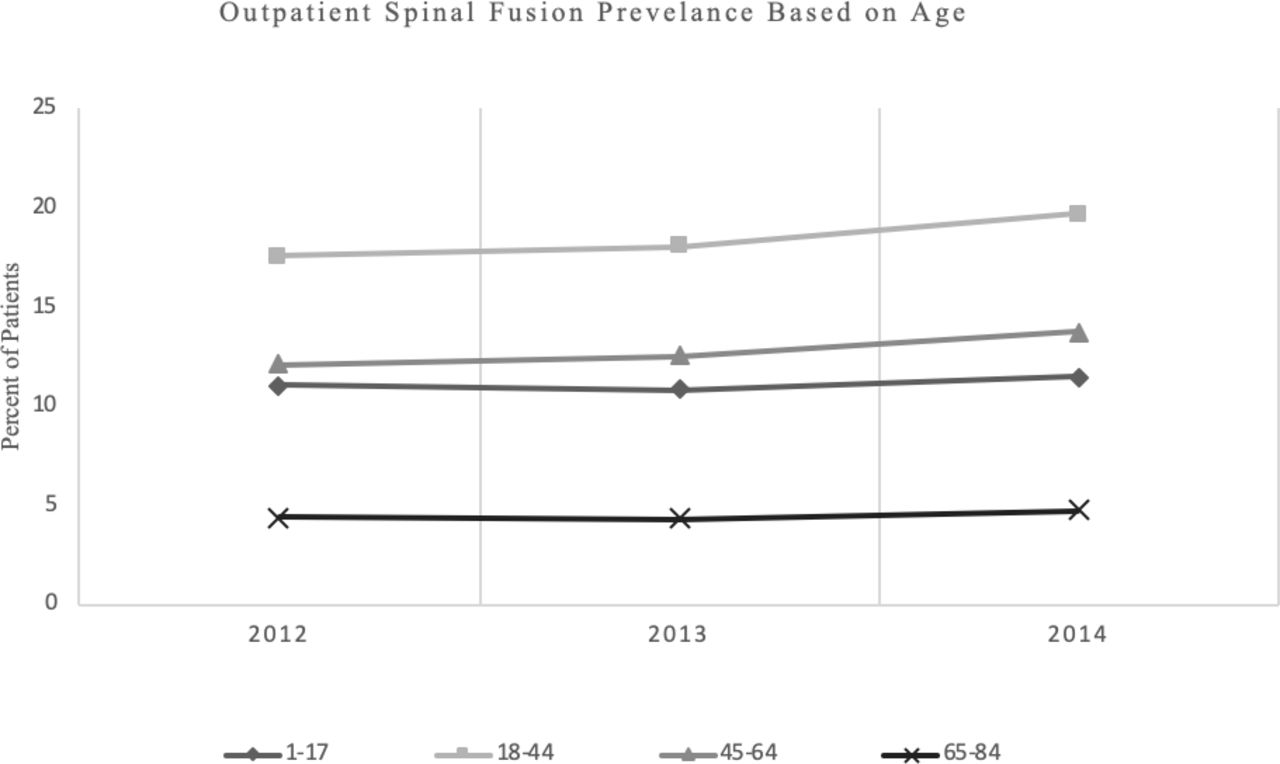
The highest rates of patients who underwent spinal fusion (by age) on an outpatient basis were observed in cohorts of patients between 18 and 44 years of age. In 2012, there were 17.54% of spinal fusions performed on patients aged between 18 and 44 were on an outpatient basis (Figure 2). By 2014, the percentage increased to 19.65%. Patients aged 45 to 64 had the second highest incidence of outpatient fusion with 12.13% in 2012 to 13.76% in 2014. Patients aged 65 to 84 had the lowest rate of outpatient spinal fusion surgery with 4.38% across the study period and 4.74% in 2014.
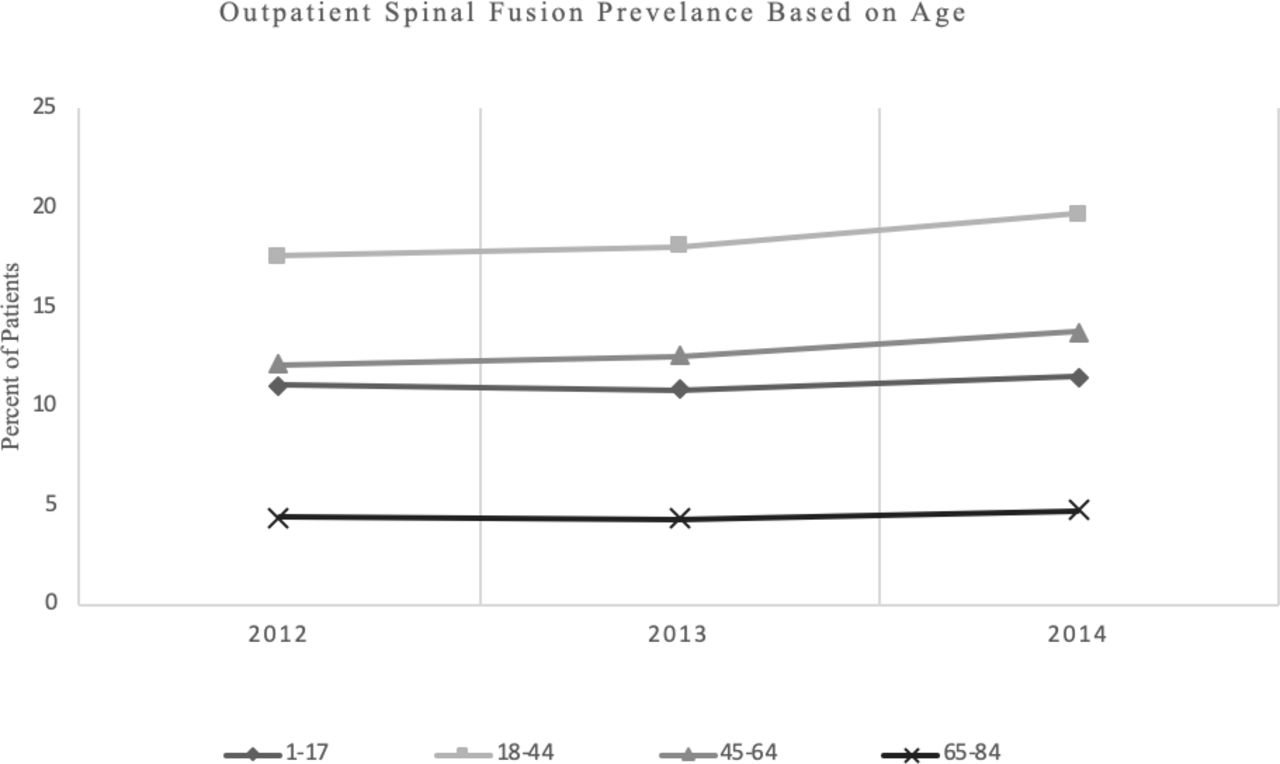
Composition of patients who underwent outpatient spinal fusion from 2012 to 2014 in the United States based on age.
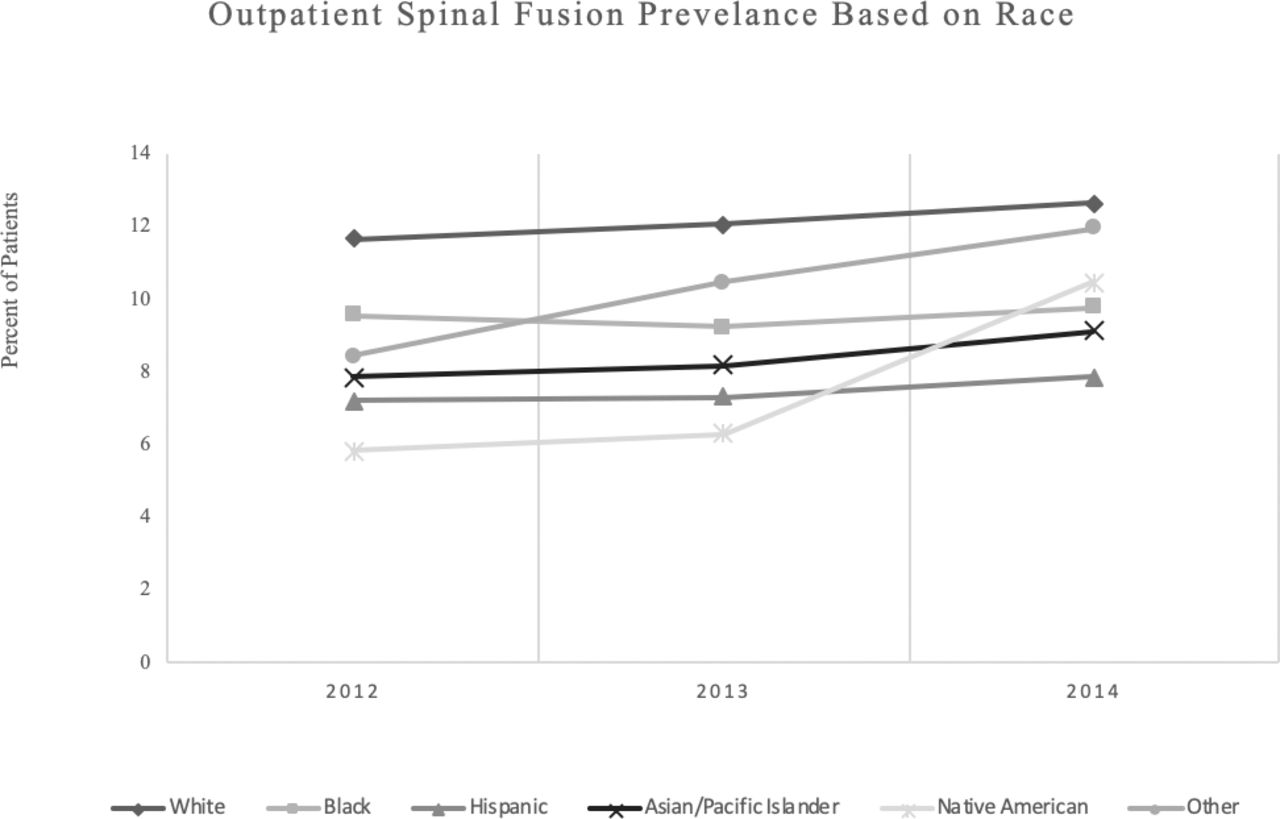
The National Inpatient Sample (NIS) showed that a larger proportion of white patients underwent outpatient spinal fusion surgery than any other race. In 2012, there were 11.68% of spinal fusion surgeries performed on white patients as outpatients, which increased to 12.67% in 2014. In comparison, there were only 7.21% of ambulatory spinal fusions performed on Hispanic patients in 2012, with a small increase to 7.87% in 2014. For the black population, there were 9.58% of outpatient spinal fusions performed in 2012 and 9.78% in 2014. There was a 4.63% increase in the percent of outpatient spinal fusion surgeries performed on Native American patients from 2012 to 2014 (5.85% to 10.48%) (Figure 3).

Composition of patients who underwent outpatient spinal fusion during the study period by race and ethnicity.
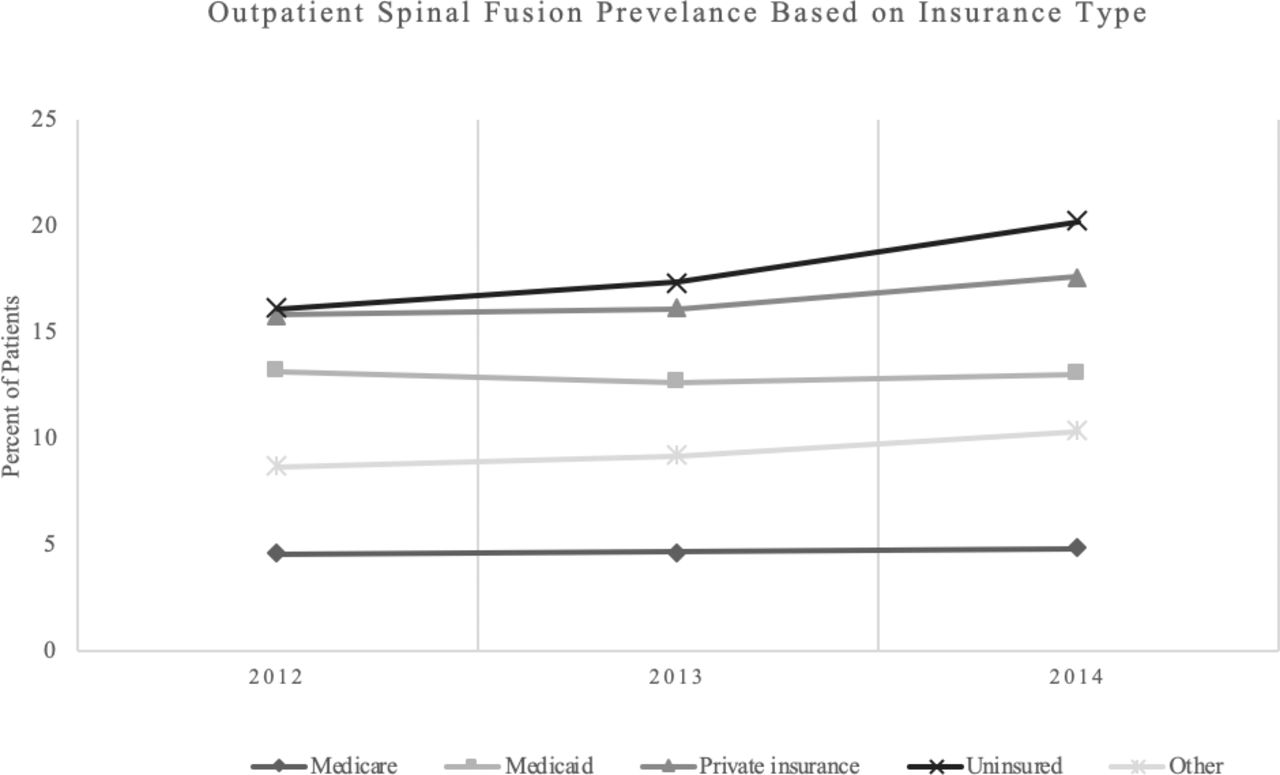
Patients who had private insurance or self-pay had the highest proportion of outpatient spinal fusion surgery throughout the study period. The rate of ambulatory spinal fusions performed on self-pay from 2012 to 2014 increased from 16.12% to 20.28%, whereas it increased from 15.85% to 17.62 for private insurance patients over the same time period. Patients insured with Medicare were the least common patient group—based on payer. Between 2012 and 2014, the percent of outpatient spinal fusions performed on Medicare beneficiaries increased from 4.62% in 2012 to 4.84% in 2014 (Figure 4).

Percentage of spine fusions cases treated in ambulatory surgery setting stratified by insurance type of patients.
Over the study period, women had a consistently higher prevalence of outpatient spinal fusion surgeries compared with men. The rate of outpatient spinal fusions performed on women increased from 11.84% in 2012 to 12.57% in 2014. There was a corresponding increase in the percent of outpatient spinal fusion surgeries performed on males from 2012 to 2014 (9.98% to 11.06%).
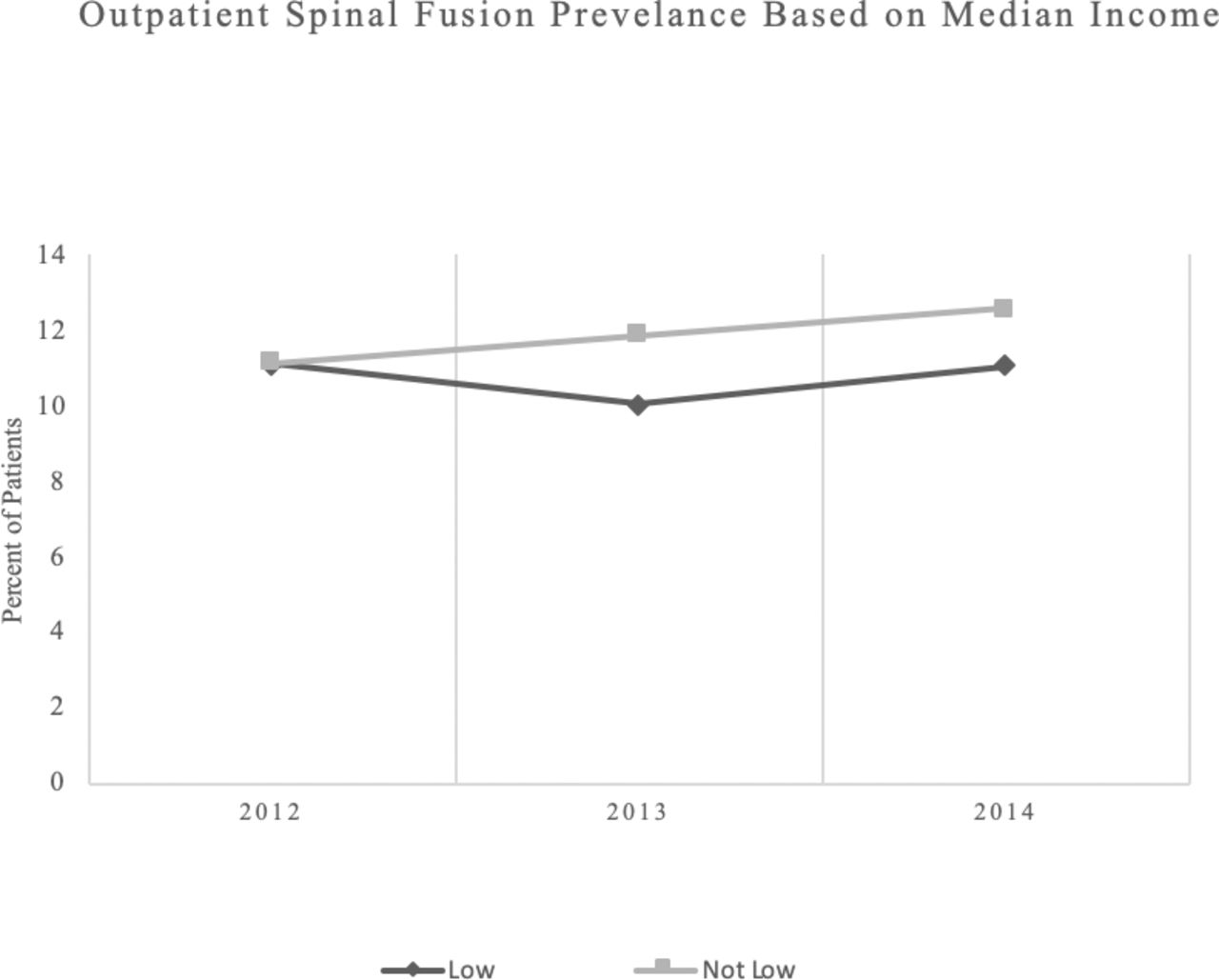
In terms of socioeconomics, there was a large difference in the number of outpatient spine fusions in patients in the “low” versus “not low” median ZIP code income. Specifically, only 24% of all outpatient fusions were performed on the “low” income cohort, whereas 76% were performed on the “not low” cohort (Figure 5). Of the population who received outpatient spine fusion, the “not low” income group represented over 3 times the representation of the “low” income group.
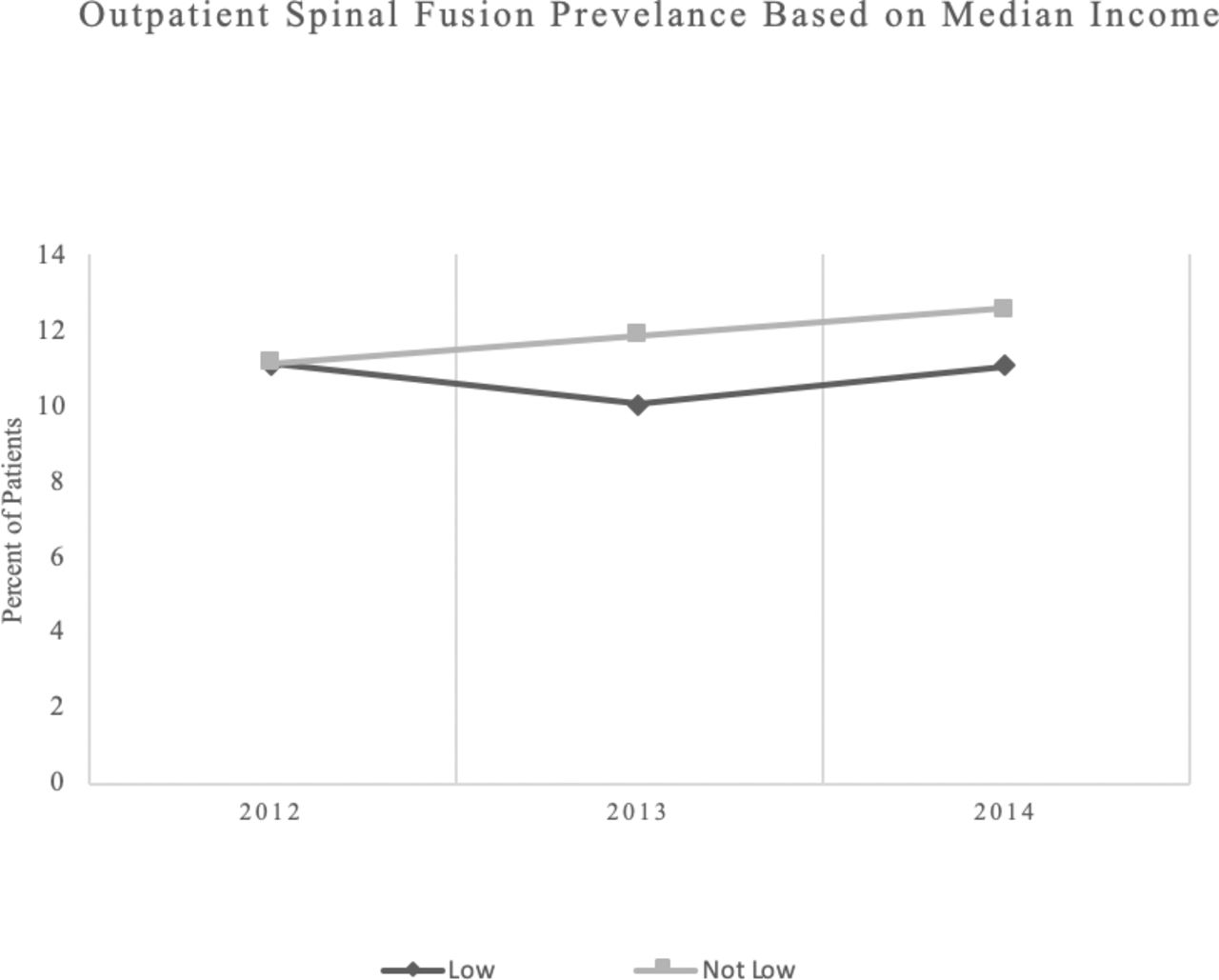
This figure shows the number of total spine fusions stratified by “low” vs “not low” median income based patient ZIP code.
DISCUSSION
Outpatient spinal fusion is safe and efficacious in the appropriately indicated patient.4 Anterior and posterior lumbar interbody fusion techniques as well as ACDF have been successfully used in outpatient settings. Minimally invasive lumbar interbody fusion techniques may cause less tissue disruption and surgical insult, thus quicker recovery and may be better suited for the outpatient arena.3,4,6 The present study identifies demographic and socioeconomic trends among patients who underwent outpatient spinal fusion surgery between 2012 and 2014.
There are multiple reports of decreased cost and higher patient satisfaction with outpatient spine surgery compared with the inpatient setting.8–12 Specifically, outpatient ACDF is associated with fewer complications than inpatient surgery.3 Pugely et al8 showed that outpatient single-level discectomy has lower overall short-term complication rate than those performed as inpatient.9 Total complications, deep wound infection, urinary tract infection, rate of blood transfusion, and duration of operation were all significantly higher in inpatient lumbar discectomy compared with the same procedure in an outpatient setting. The authors attributed lower complication rates to improved postoperative mobilization, decreased rate of urinary catheterization, and shorter duration of exposure to pathogens. Developing an understanding of the demographic breakdown of patients receiving this surgery can drive further investigation into understanding how postoperative outcomes can be improved in specific patient populations.
In the current study, the incidence of outpatient spinal fusion increased from 13.6 to 14.8 per 100,000 people in 2012 to 2014. The increase in incidence may be attributed to the aforementioned potential benefits of outpatient spinal fusion, such as decreased complication rate as well as decreased cost. Additionally, there may be a financial or social incentive for surgeons to perform the cases in an ambulatory setting. It is possible that the role of spine implant billing may be involved as well. Because payment and reimbursement for spine fusion implants can vary widely between insurance contracts, if the cost of implants is prohibitively high and unable to be reimbursed, this may cause fewer patients to receive fusion in an ambulatory setting. Therefore, implant reimbursement trends in the ambulatory setting may also affect trends in ambulatory spine fusion. Although these suggestions may play a role, further investigation is required to determine causation.
The results of our study are comparable with the existing literature. In the current study, the percentage of spinal fusion surgeries performed on an outpatient basis was slightly higher in women than in men in all 3 years of the study period. Similarly, Arshi et al13 investigated trends in outpatient posterior lumbar fusion from 2007 to 2015 and also found that women underwent slightly more outpatient spinal fusion than do men (54.4% vs 45.6%). Moreover, McGirt et al14 found similar data with 50.7% females receiving inpatient fusion and 49.3% were males (P = .04).
We report that over the study period that 81% of all outpatient fusions were performed on white patients and only 8.6% on black patients. McGirt et al14 found a similar, though greater distribution, with 87% of outpatient fusions being performed on white patients between 2005 and 2011.15 Lad et al16 reported that African Americans who underwent surgery for spinal stenosis regardless of setting were more likely to experience postoperative complications of any kind and higher costs. Equity and equality in access is a challenge to the health care system, and these data suggest that it is also present in the world of ambulatory spine surgery. These data clearly show that the white patient population received ambulatory spine fusion greater than 9 times more than the Black and African American population. This distribution is inconsistent with the ethnic and racial composition of the US population. These data show that there are clearly racial disparities associated with spinal fusion; however, determining the etiologies will require further investigation.
Moreover, patients who are either privately insured or self-pay undergo outpatient spinal fusion at a higher rate than do other patients with different insurance types. Considering that “not low” income patients and privately insured patients were more likely than the rest of each of their respective cohort to receive outpatient surgery, one may speculate that this may represent a financial barrier that might prevent certain patients from accessing outpatient care. Further investigation into the cost and access to outpatient spinal fusion is necessary to fully understand this phenomenon.
Baird et al6 showed similar findings regarding age distribution for outpatient fusions. The authors reported that patients aged 20 to 50 were more likely to undergo outpatient spinal fusion surgery than elderly patients, likely suggesting that younger patients might be more commonly recommended for outpatient procedures because they are less likely to have the comorbidities associated with old age. Increased age has been associated with increased risk of hemorrhagic complication, infection, and refusion in adult spinal fusion.17 These patients are less suited to outpatient spinal fusion than younger patients and may benefit from the monitoring offered by an inpatient hospital admission.
There are several limitations to this study. The database used for this study includes information from 29 states and therefore cannot be used for national estimates, as there may be geographical variance. Furthermore, the granularity of the CCS codes used for data extraction prevents an accurate delineation between diagnoses that could have precipitated the need for surgery. This could be further complicated by inaccuracies in the CCS billing record, errors in transferring hospital records to the NIS database, and a lack of data about revision surgeries. Additionally, we were unable to clearly differentiate between cervical and lumbar fusion cases. Because outpatient fusion was captured on the NIS using a specific CCS code, it is also possible that coding issues may have prevented the capture of all spinal fusions. These data are further limited by the fact that the NIS database only includes information between 2012 and 2014 for ambulatory spine fusion. Another limitation of this study is the inability to study patient outcomes from the databases used. Future prospective studies are indicated to provide further data surrounding ambulatory spinal fusion.
CONCLUSION
The present study defines demographic information and trends surrounding outpatient spinal fusion surgery by using data from 3 large databases. Overall, patients with private insurance, white patients, and patients between the ages of 18 and 44 years old were the most common groups to undergo an outpatient spinal fusion. A better understanding of the demographic trends related to outpatient spine fusions may allow health care providers and policymakers to establish and improve care in the outpatient setting, possibly, by specifically identifying those patients who would benefit the most and thus optimizing their outcomes. Further investigation into why these trends are observed is necessary will be necessary to implement changes within the health care system that will further improve patient care.
Total number of outpatient spinal fusion surgeries distributed by age in the United States.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}