


ABSTRACT
Background: Pedicle screw instrumentation of the posterior cervical spine is the most secure form of fixation available to surgeons. It has not achieved widespread use yet in the Middle East, mostly due to concerns regarding its feasibility in the target population. A detailed morphometric analysis of the lower cervical spine pedicles using computerized tomography (CT) was proposed to address this issue.
Methods: Two hundred and seventy patients were enrolled in the study. CT scans were reviewed by two experienced assessors, and measurements of pedicle width (PW), height (PH), and transverse angle (TA) were recorded for all patients. Interobserver and intraobserver reliability were calculated using the kappa statistic. Sex differences were also recorded and analyzed. The t test was used to assess for any significant differences in measurements due to sex (P < .05).
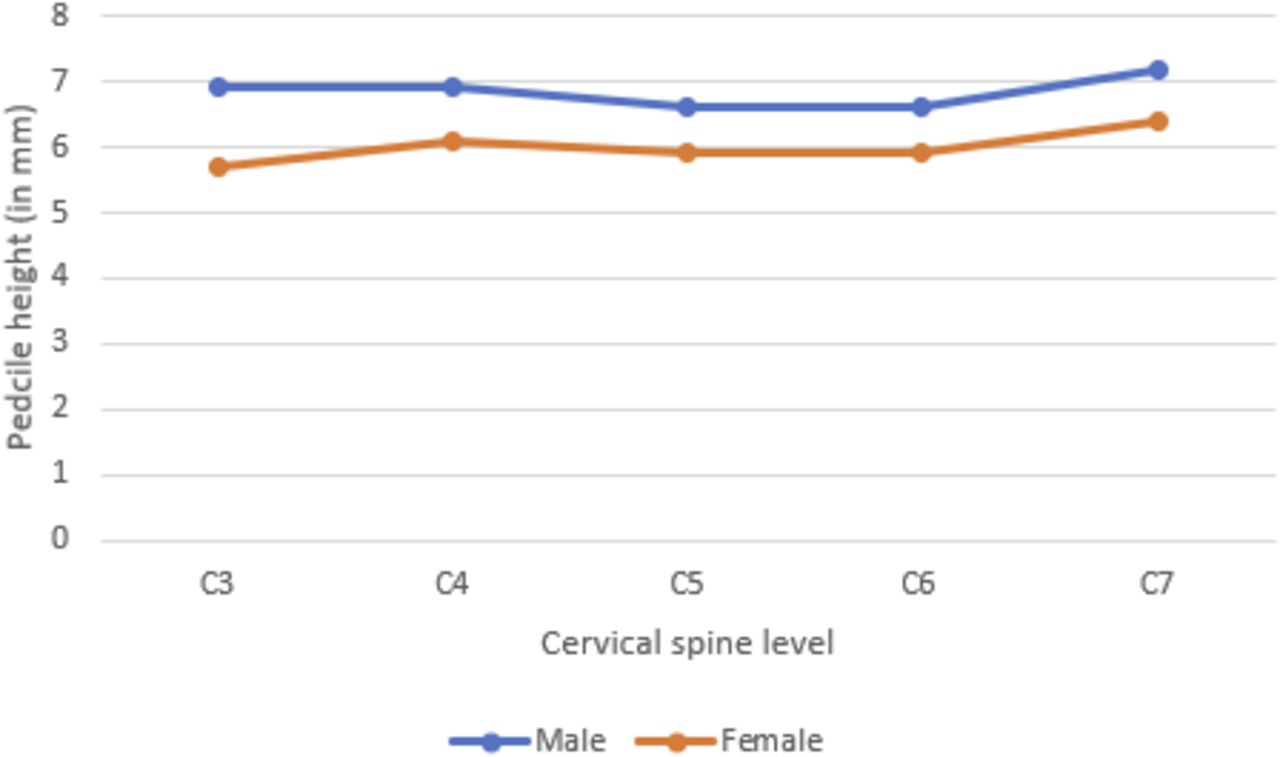
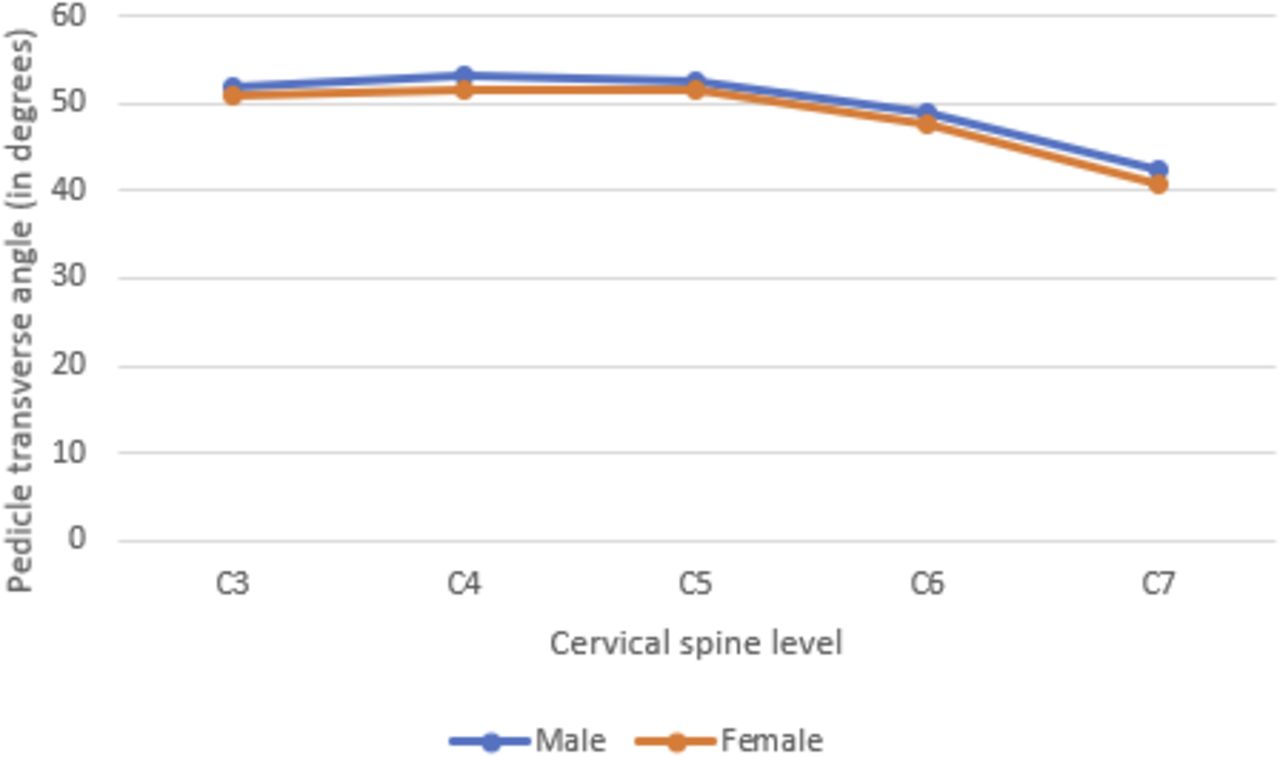
Results: The mean PW varied from 4.4 mm in C3 to 6.1 mm in C7. The mean PH was 6.4 mm in C3 and 6.8 mm in C7. Pedicle TA varied from 42 to 51 degrees between the different levels. Sex differences were observed and were statistically significant for PW and PH. Interobserver reliability was high for PW and PH, but was low for TA. Intraobserver reliability was 0.99 for both assessors.
Conclusion: This study provides reliable PW and PH measurements and demonstrates that cervical pedicle screw instrumentation is feasible in our local population. Significant variability exists, however, and each patient must be addressed individually for best results.
Level of Evidence: 3.
Clinical Relevance: This study shows that the morphology of the subaxial cervical pedicle permits instrumentation in a majority of cases of our target population.
INTRODUCTION
Posterior instrumentation of the subaxial cervical spine has evolved over the past few decades. Wiring techniques were superseded by lateral mass screws by the end of the 20th century. Cervical pedicle screw instrumentation was first described in 1994 by Abumi et al.1 Biomechanically, the cervical pedicle screw is far stronger than any lateral mass screw.2,3 Widespread use of this technique, however, has not been achieved. Variability in the cervical anatomy and risks to the neurologic and vascular structures are well documented in the literature.4,5
Ethnic variability in cervical pedicle anatomy was established by several previous reports.6–9 Cervical pedicle screw instrumentation is rarely used in our region, with reluctance usually attributed to the small size of cervical pedicles in our population. Given the scarcity of published data accurately representing our target population, it is difficult to support this argument. We aim in this study to quantify the cervical pedicle width, height and transverse angulation in our target population and compare it with existing data from other reports.
MATERIALS AND METHODS
Computerized tomographic (CT) scans of 300 consecutive adult patients (over 18 years of age) undergoing cervical spine imaging for various indications in our institution (located in Riyadh, Saudi Arabia) were included for the purpose of this study. Institutional research ethics board approval was granted before starting the study. Patients with congenital abnormalities, previous surgery, infections, neoplastic lesions, or trauma to the cervical spine were excluded. Expatriates and other noncitizens were excluded to allow for a better representation of our target population.
The CT scans were performed on 64-slice multidetector scanners; SOMATOM Definition (Siemens Healthcare; Erlangen, Germany), Discovery 750HD, and Lightspeed VCT (GE Healthcare) using the following parameters: helical acquisition, 120 kVp, 70–80 mAs, 512 × 512 × 16 matrix, 0 gantry tilt, and a slice thickness of 0.625 mm. Images were retrieved using the institution picture archiving and communication system (Centricity 4.2, GE Healthcare).
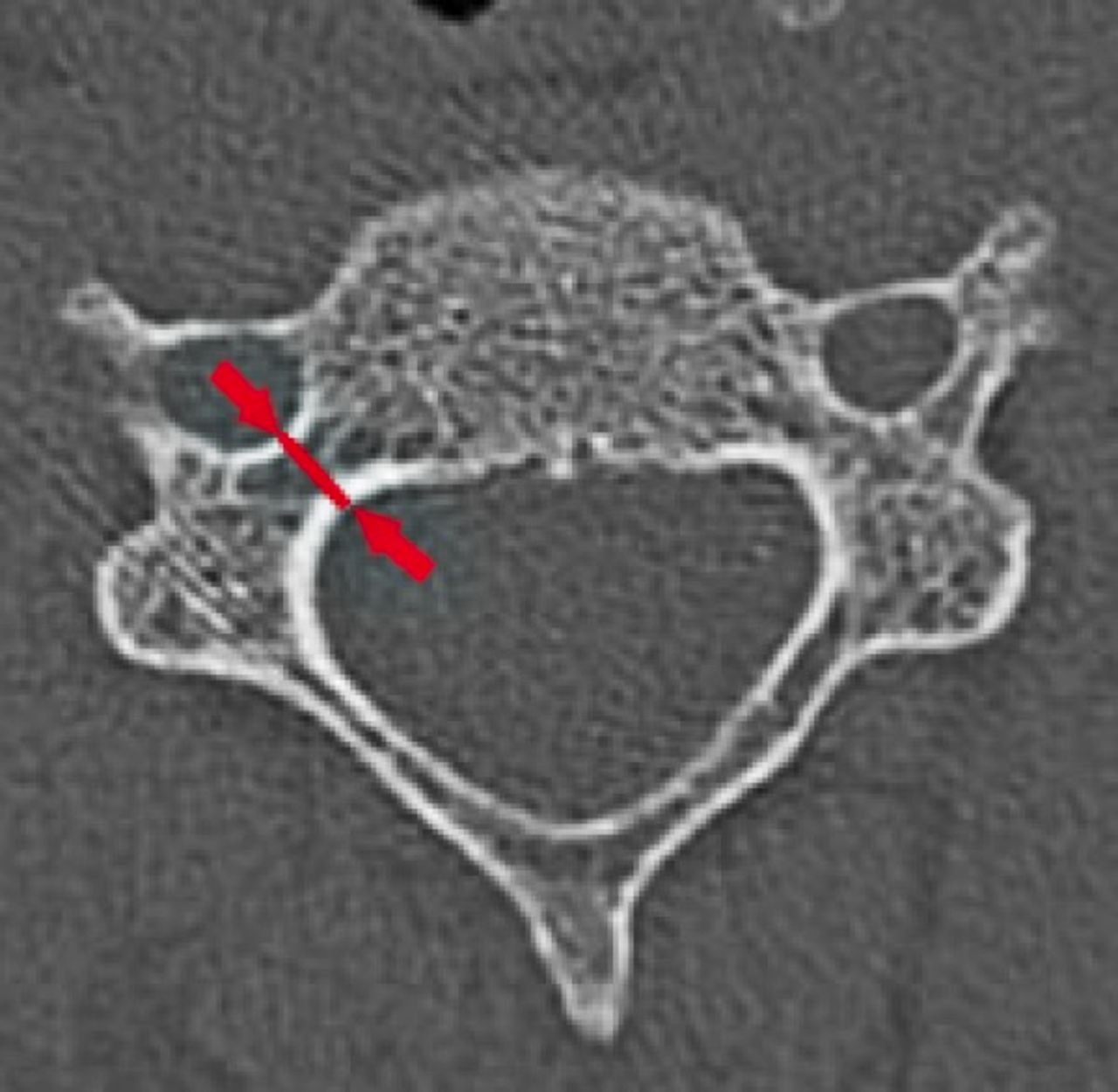
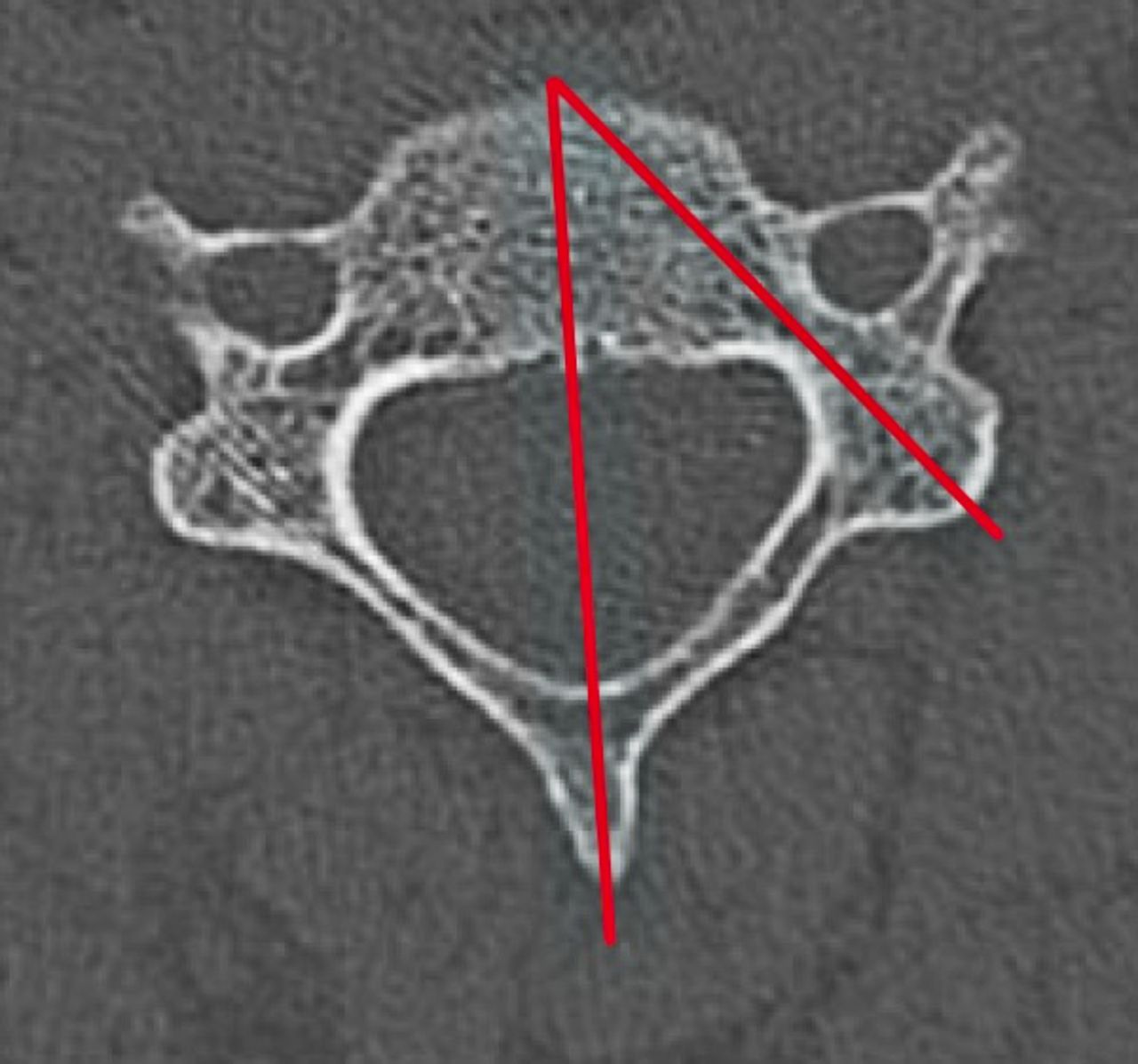
Measurements taken included pedicle width, pedicle height, and pedicle transverse angle from C3 to C7 unilaterally. The pedicle width was defined as the largest medial to lateral measurement of the pedicle isthmus taken in the axial view, including the cortex. The pedicle height was defined as the largest superior to inferior measurement of the pedicle isthmus taken in the sagittal view, including the cortex. The pedicle transverse angle was defined as the angle between the mid-sagittal axis (line from the midpoint of the anterior cortex to the tip of the spinous process) and the pedicle axis on the axial view (Figures 1–3). The measurements were taken independently by a consultant orthopedic surgeon (KA) and a consultant radiologist (FE) using the previously agreed upon criteria for measurement. The data were then analyzed for interrater reliability using the kappa statistic. A random sample of 20 patients had repeat measurements done 1 month later for measurement of intrarater reliability, again using the kappa statistic. The mean and standard deviation were calculated for all measurements. The t test was used to assess for any significant difference in pedicle measurements due to sex (P < .05). Statistical analysis was performed using SPSS software (version 24, IBM Corp., Armonk, New York).

Pedicle height.

Pedicle width.
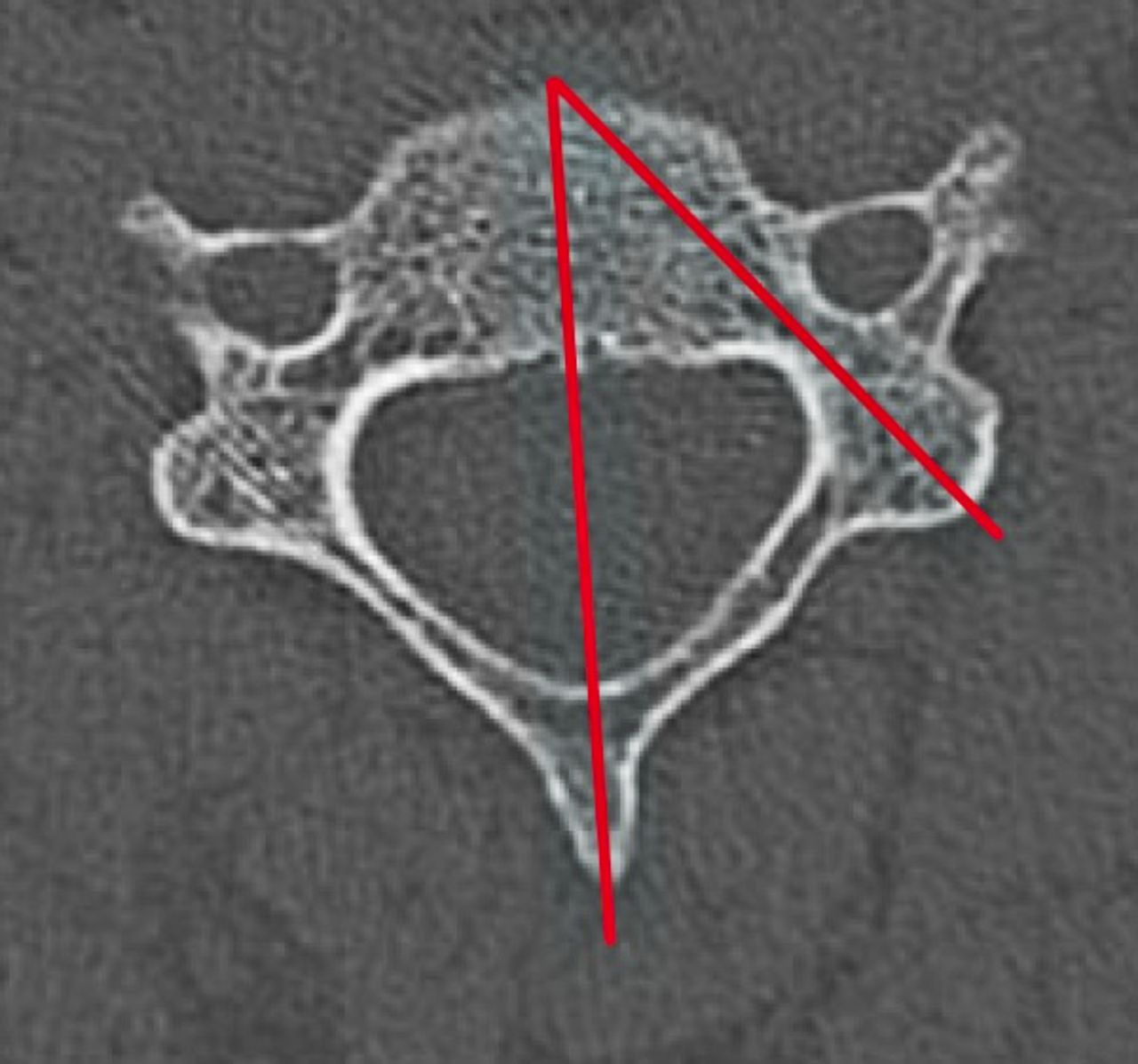
Pedicle transverse angle.
RESULTS
Three hundred consecutive patients who underwent cervical spine CT were included into the initial sample. After application of exclusion criteria, 270 patients made the final sample for analysis. A total of 1350 pedicles were measured to obtain 4050 measurements. The sample was composed of 154 males and 116 females. The average age was 40 years old (range, 18–92). The pedicle measurements and interobserver reliability are shown in Tables 1–3. Intraobserver reliability was 0.99 for both assessors. Sex differences were observed for all three measurements (Figures 4–6).
Pedicle width measurements.
Pedicle height measurement.
Pedicle transverse angle measurement.

Pedicle width measurement by sex (P < .05 for all measurements).
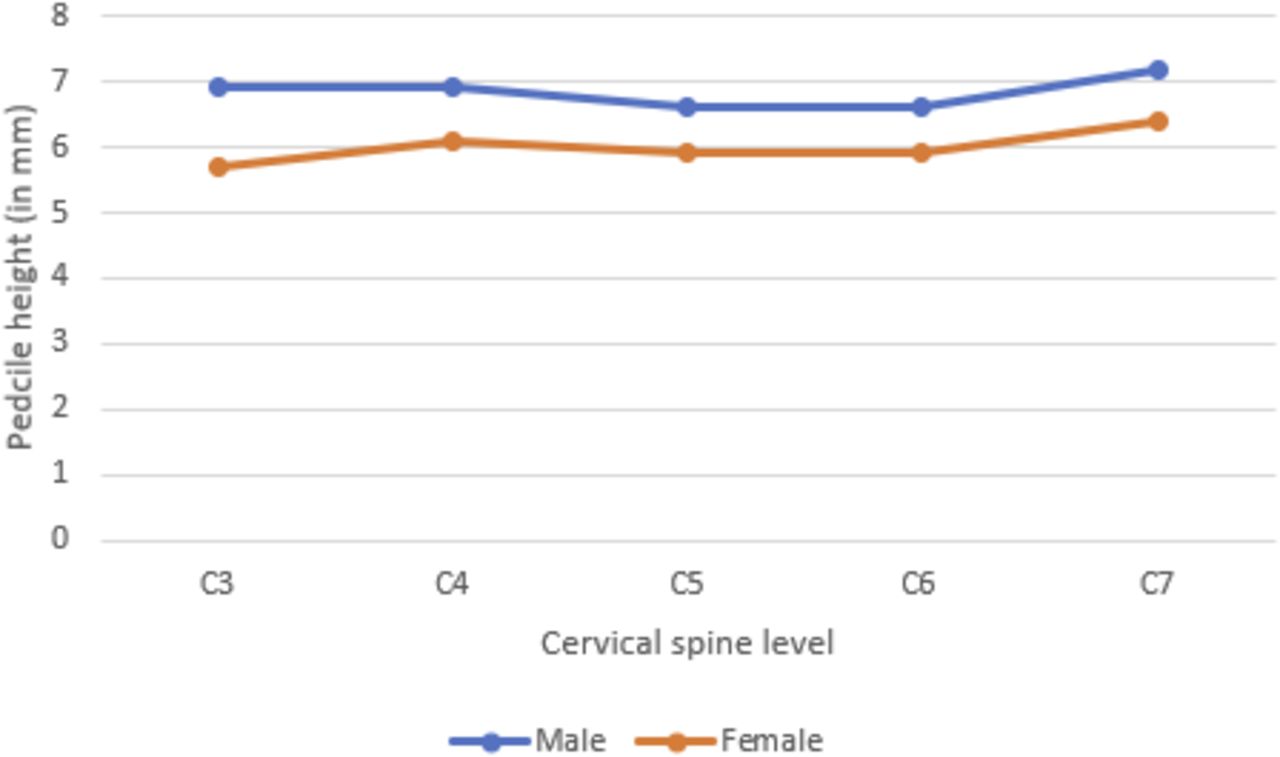
Pedicle height measurement by sex (P < .05 for all measurements).

Pedicle transverse angle by sex (P < .05 for C3–C5 only).
DISCUSSION
The first report on cervical pedicle measurements was published in 1991 by Punjabi et al.10 His study was done on cadavers, and pedicle measurements were done in addition to other anatomical landmarks of the cervical spine. The first CT-based morphometric analysis of the subaxial spine was reported in 1997 by Ebraheim et al.11 In the same year, Karaikovic et al12 published a similar study, but validated the CT measurements by manual measurement of cadaver specimens and found that the measurements correlated well. Several other reports came about afterwards that showed that sex- and ethnic-based variations existed.6,8,9,13–21 Chazono,22 an author of one of the aforementioned reports, reviewed some of these publications and found that the reported ethnic differences were within 10%–15% of each other.
Al-Saeed et al20 reported on cervical spine pedicle measurements from Kuwait. This study, while well planned and conducted, had a smaller sample size than our study. Given that our target population, supposedly, is of the same ethnicity, we found significant variability between our measurements and theirs, where their data were 0.5–0.7 mm larger in both pedicle height and width. That could be because their included patients, although “citizen of an Arab country”, were probably not natives of the country, as a large expatriate Arab population populates their country. Our study was limited to Saudi citizens and, as such, is probably more representative of an Arab/ Middle Eastern population.
The measurements presented in this study are similar to other Asian countries.8,9,16,19,23–25 Taking into account the thickness of the cortex, 0.5 mm for most levels, cannulation and instrumentation of C5, C6, and C7 with a 3.5-mm screw is certainly feasible in our population, but more so in males than in females. The transverse angle decreasing as we go into the lower levels also helps the starting point be within reach within the operative field.
This study is the largest CT-based morphometric analysis of human cervical spine pedicles done to date; however, this study may be limited as its measurements were limited to the three mentioned above, while other reports had more extensive data points collected. The authors believe that, from a clinical application perspective, these measurements are all that is needed to understand pedicle morphology and plan surgical treatment.
CONCLUSION
Cervical spine pedicle instrumentation is a useful tool in the armamentarium of spine surgeons. Although difficult in some cases, this current study shows that the morphology of the pedicle permits it in most levels and most cases. Nevertheless, a detailed review of each patient's CT results before surgery should be performed as significant anatomical variability exists, and the risk of neurovascular complication cannot be underestimated with this technique. More widespread availability of intraoperative CT imaging and navigation could help this technique gain more proponents in our region.
Footnotes
Disclosures and COI: The authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.