


ABSTRACT
Atlantoaxial rotatory dislocations (AARDs) are common in the pediatric population and rarely seen in adults. We describe a case of neglected AARD and subsequent management. A 25-year-old man developed a Fielding type 1 AARD following a road traffic accident. He was managed conservatively for 1.5 months before being referred to us. The patient underwent surgery 1.5 months after the accident. Closed reduction failed and C1-2 fixation with the Harms technique was performed after intraoperative reduction resulting in correction of deformity. Delay of treatment makes intraoperative reduction more difficult and increases the possibility of the chronic permanent change of neck muscles and ligaments. Hence, a high index of suspicion with a thorough clinical examination and judicious use of radiological investigations is paramount to the appropriate management of such cases.
- atlantoaxial dislocations
- atlantoaxial rotatory dislocations
- atlantoaxial rotatory fixation
- Fielding type 1 AARD
INTRODUCTION
Atlantoaxial rotatory dislocation (AARD) is the rotational subluxation of C1 over C2. The pathoanatomy of AARD is related to the transverse alar ligament's (TAL) integrity. These dislocations occur more commonly in children and adolescents in whom there is a high degree of rotational behavior of C1 and C2,1 owing to weakness and malleability of periarticular soft tissue and increased mobility of the articular joints. In adults, they result from extreme rotation and distraction trauma of the cervical spine.
Atlantoaxial rotatory dislocation is defined as excessive movement and loss of facetal continuity between C1 and C2 as delineated by abnormal motion curves.2 Presentation is with neck pain and limited range of cervical spine motion with torticollis occurring towards the side of the dislocated facet joint. Radiographs with open-mouth views are often helpful in delineating the pathology. Dynamic computed tomography (CT) is the “gold standard” in the diagnosis of AARD, though patients' non-cooperation due to severe pain is the limiting factor in performance of the same.
Closed reduction with traction should be instituted immediately to avoid the serious consequences of chronic AARD. Recurrent dislocation and incomplete reduction should be treated with posterior C1-2 fusion in the best achievable alignment.3 Occasionally they are seen in adults, especially when preexisting C1-2 instability is present or with high-energy trauma.1
CASE REPORT
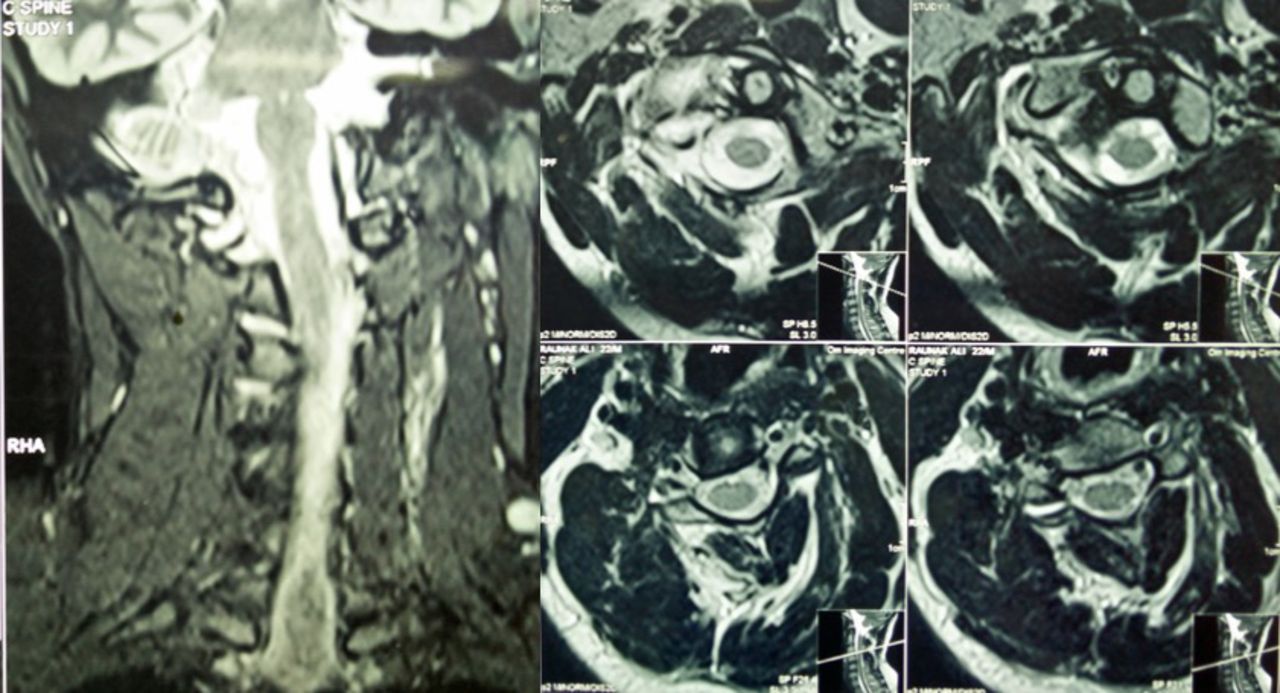
A 25-year-old man was involved in a road traffic accident while riding a 2-wheeler. He is alleged to have run into a stationary vehicle, after which his helmet fell off. He regained consciousness a few minutes later and helped his pillion rider. He was taken to the emergency department in another center and evaluated. Non-contrast CT of the head was normal. The patient could not move his head from its position, tilted to the right (“cock robin” position; Figure 1). He had clear consciousness and no motor paralysis or sensory disturbances. An MRI of the cervical spine was done at this time, showing atlantoaxial rotational subluxation with an intact TAL (Figure 2). A CT of the cervical spine was not done at this time. The patient was treated with conservative measures that included nonsteroidal anti-inflammatory drugs and cervical traction for 3 days. He was later discharged and advised bed rest and symptomatic measures. The head continued to be in a tilted position.

(a) Preoperative clinical photograph showing “cock robin” position and (b) immediately postoperative clinical photograph showing resolution of neck tilt. (c–e) Postoperative images at 2 years show no residual deformity and minimal restriction of rotation.

Preoperative MRI: (a) Coronal scans showing lateral tilt. (b) T2 weighted axial scans showed intact transverse alar ligament.
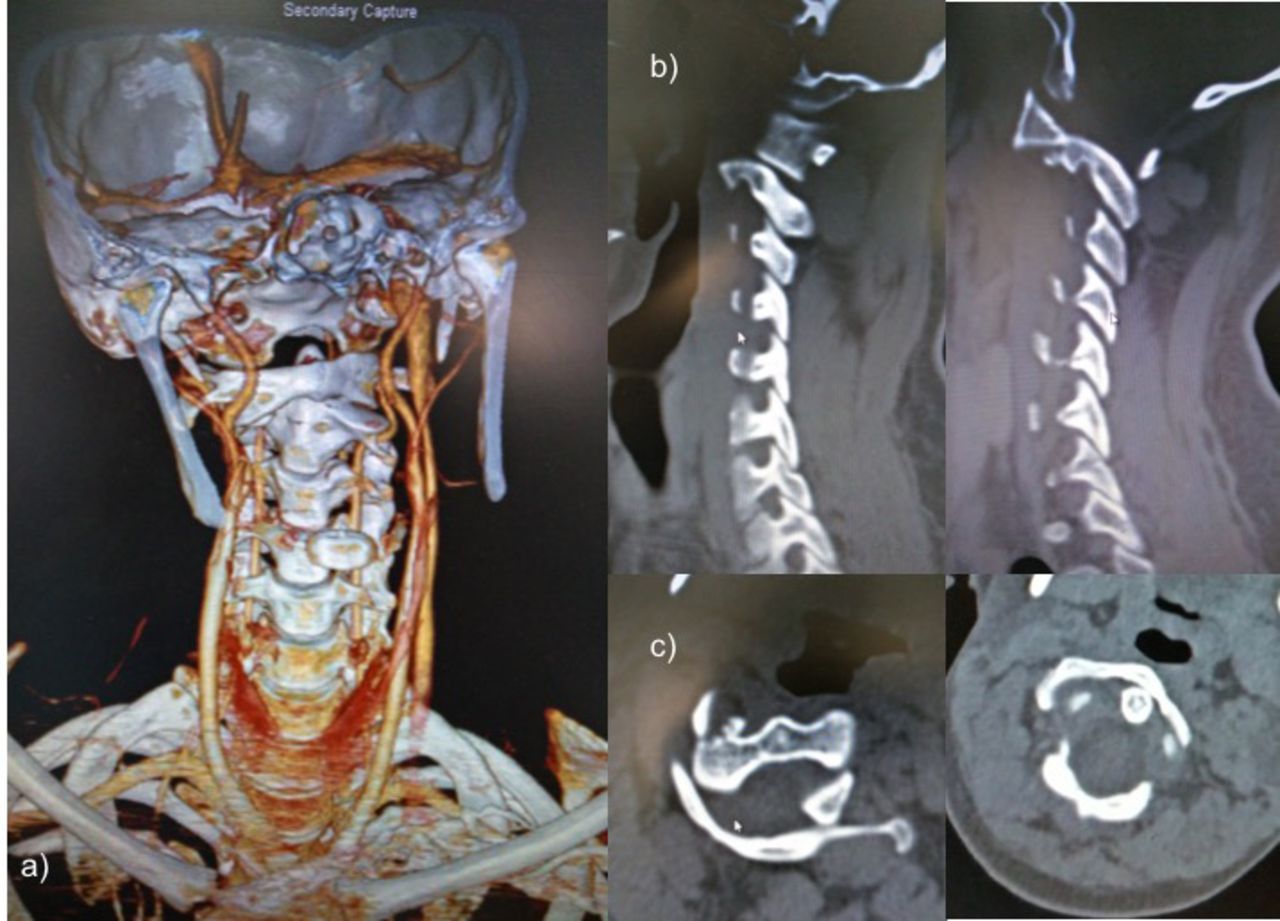
The patient presented to our center after 1.5 months of having failed various treatments for the injury. At presentation, he had pain in the left C2 distribution and tilted cock robin position of the head but no motor deficits. An x-ray and a plain CT of the cervical spine showed the atlas rotated to the right, centering on the dens of the axis, with no increase in atlanto-dental interval (Figures 3 and 4). No developmental deformities were observed. The CT angiography showed normal course of vertebral arteries. This corresponded to a diagnosis of Fielding type 1 AARD4 or White and Panjabi unilateral combined anterior and posterior dislocation.5 The C1-2 rotation angle was around 40°.

Preoperative x-ray: (a) Note eccentric position of the odontoid. (b) Lateral x-ray showing rotation at C1-2 with elliptical appearance of the C1 arch.

(a) Preoperative computed tomography angiography with 3-dimensional recon showing atlantoaxial rotatory dislocations. (b) Parasagittal view showing dislocation of facet joints. (c) Axial view showing maintained atlanto-dental interval with rotatory atlanto-axial dislocation.
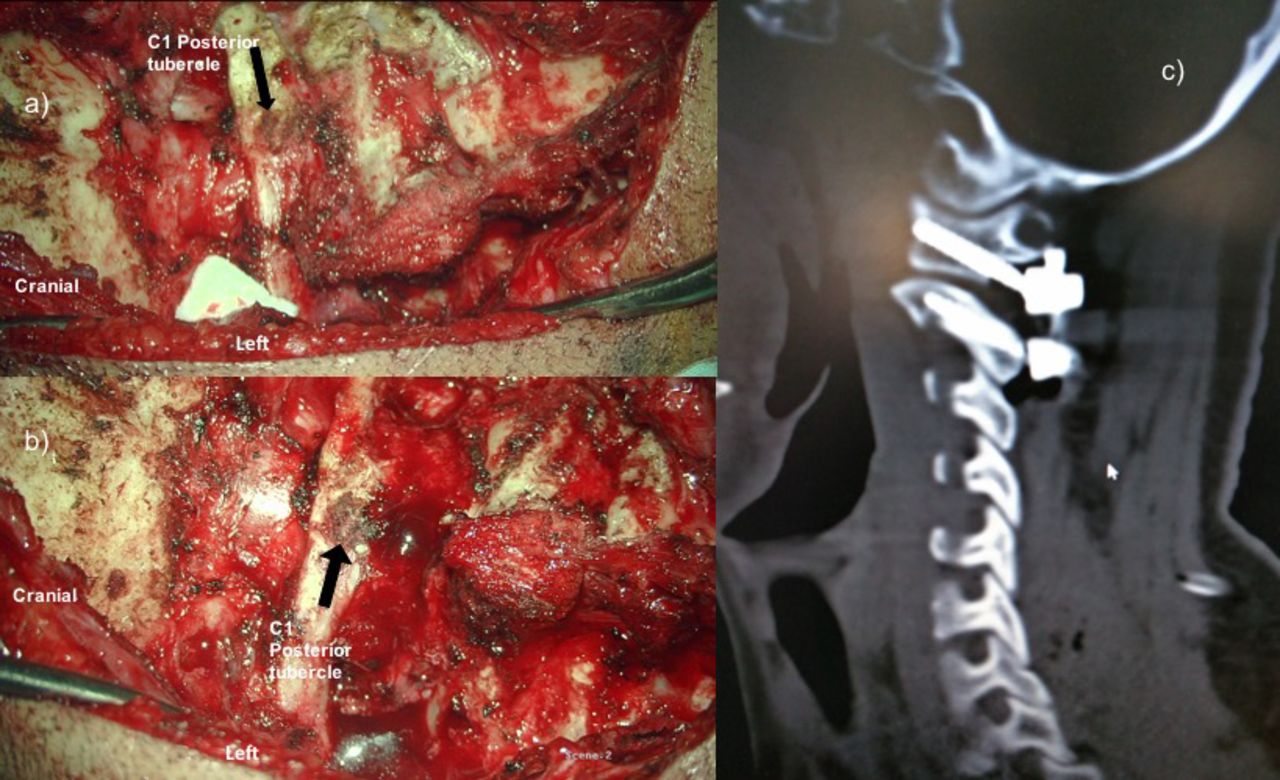
Awake manipulation and attempts at correction of the deformity failed due to neck pain and associated muscle spasm. The patient was taken for surgery, and after induction the patient's head was fixed on a Sugita 4-pin head clamp and again closed reduction was attempted under general anesthesia, but it failed. The patient was placed in a slightly reversed Trendlenberg position to allow the body weight to provide traction. Consequently, we proceeded with open reduction and fixation. After muscle dissection, the sub-axial cervical spine was seen to be rotated to the left. The C1-2 posterior atlantoaxial membrane was cut and the atlantoaxial joints were traced. The right C1 lateral mass was found to be perched anterior to the C2 pars. The rotational deformity had severely stretched the left C2 nerve, which was divided to expose the C1-2 interval. The C1 arch was found resting upon the C2 pars on the right side. A periosteal elevator was inserted into the space between the arch of the atlas and the C2 pars and rotated to achieve a distraction effect and release the perched C1 facet. This resulted in spontaneous derotation and correction of the deformity. The C1-2 joint spaces were then denuded of cartilage in preparation for fusion. Posterior fixation was done using the Goel-Harms C1-2 fixation technique.6 Following the surgery, the patient's neck pain subsided and the normal neck alignment was restored (Figure 5–7).

(a) Initial exposure depicting severe rotation of sub-axial spine in relation to C1. (b) Following opening of joint spaces C1-2 realignment noted. (c) Postoperative computed tomography scan.

Postoperative x-ray images at 2 years in extension, neutral, and flexion.

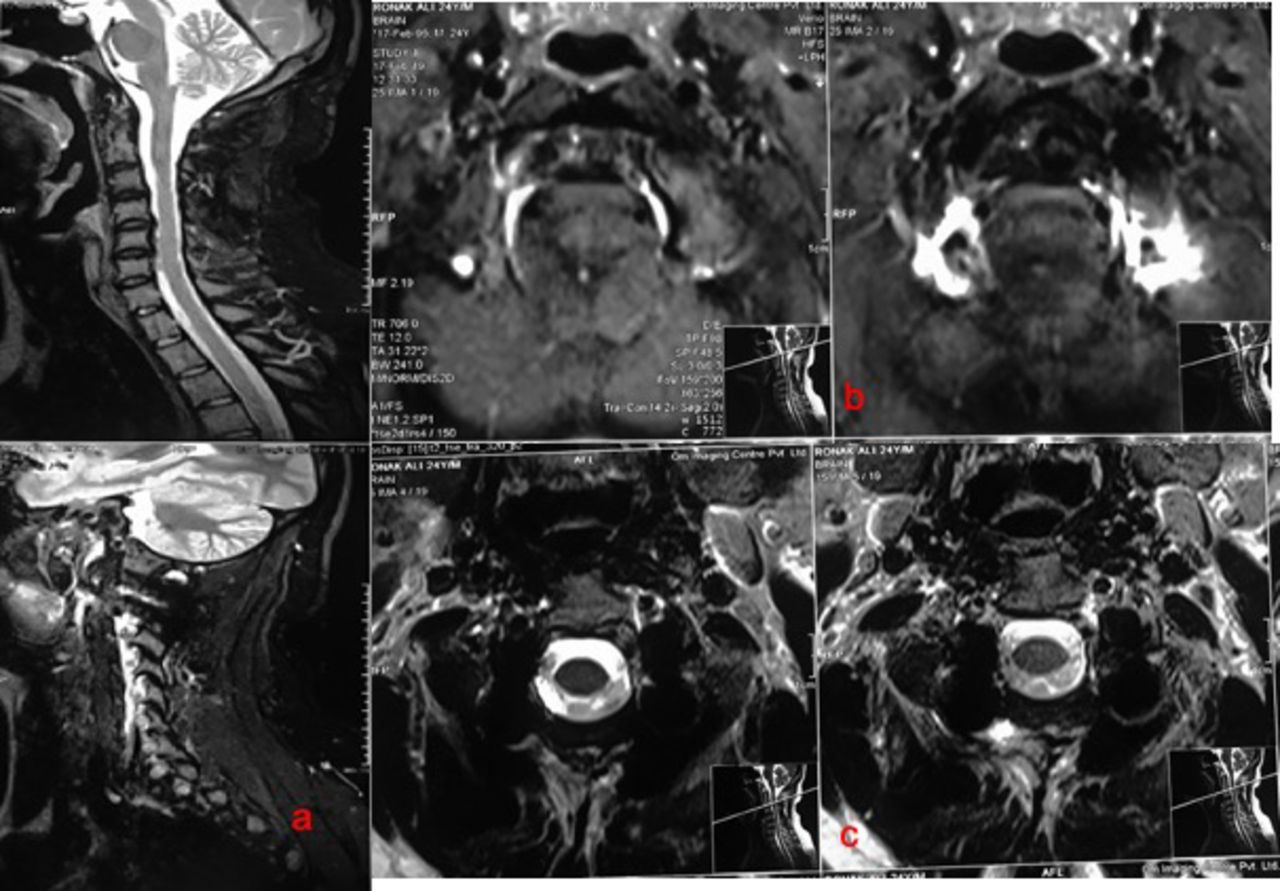
Postoperative MRI images at 3 years: (a) Sagittal scans of brainstem. (b) T2 weighted axial scans at foramen magnum level. (c) T2 weighted axial scans at C2 level.
DISCUSSION
Atlantoaxial rotatory dislocations are posttraumatic pathologies resulting from rotatory trauma at C1-2 bone-ligament complexes. Physiologically, the C1-2 joint is responsible for as much as 60% of the total rotation of the neck, behaving as the main rotational pivot of the cervical spine. The stability of the C1-2 joint is ensured by the atlas transverse ligament having high resistance against flexion and extension, by the alar ligaments limiting lateral flexion movements, and by the joint capsules limiting rotatory movements. In the absence of an intervertebral disc between atlas and axis, any rotational stress is transmitted through the articular facets and O-C1 joints. Excessive rotational forces may lead to capsular distraction and subsequently, AARD. In children, this condition is responsive to conservative measures and traction in view of the more elastic and slack joints ligaments and also weak periarticular soft tissue.7
AARDs are rare in adults and often the result of high-energy trauma.8 The small number of cases described in the literature may be attributable to the lethality of injuries producing traumatic AARDs. Mazzarra and Fielding9 have showed that the relative atlantoaxial rotation beyond 63° results in narrowing of the spinal canal and neural injury. However, cases have been described as a result of seizure,10 Grisel syndrome,11 and cervical dystonia.12 Diagnosis of AARD is often delayed as a result since it is an uncommon occurrence and manifests as subtle findings on conventional x-rays.4,13 Unilateral atlantoaxial subluxations are possible with a ruptured TAL. The ligament is intact in bilateral subluxations. On a lateral view, the rotational dislocation of the atlas leads to an elliptical appearance of the arch. Eccentric position of the odontoid process will be seen on true anterior-posterior view on plain radiographs. In a patient with persistent posttraumatic torticollis, a high index of suspicion of AARD must be maintained. A 3-dimensional CT scan must be performed to diagnose and classify the dislocation and evaluate C0-1 and C1-2 joints.2,14 An MRI scan is needed to evaluate transverse and alar ligaments, the articular facets, and periarticular edema. In addition, CT or MR angiography is needed to evaluate the exact status of vertebral arteries.
Most cases of adult posttraumatic AARD have been managed nonoperatively,8,15–22 whereas 2 cases having associated odontoid fractures23,24 and 1 having articular facet fracture25 were managed with open reduction and posterior fixation. For irreducible AARD, open reduction and fixation may become mandatory. Many surgical approaches are described for the treatment of AARDs. The posterior approach with the Harms fixation is the gold standard in fixed luxations, achieving a complete realignment and a robust stabilization. It allows intraoperative manipulation and reduction. Other authors26 have described reduction and fixation using extreme lateral approach. Weißkopf et al27 have used transoral reduction followed by temporary transoral fixation or definitive fusion in their series of pediatric and adult AARD.
Delay in reduction of more than 1 month in an adult results in a more difficult intraoperative reduction and could have clinical consequences. The delay in reduction and the cervical muscle spasm caused permanent changes that set the fixation. It would explain the failure of conservative treatment. Goel et al28 have discussed the detrimental effects of a delayed diagnosis of AARD and the success of facetal manipulation, distraction and realignment with fixation under surgical vision in the same. The abnormal degree of atlantoaxial rotation in our case and the failure of initial conservative approach to the same necessitated the surgical intervention.
Weißkopf et al27 showed that when fixation between C1 and C2 is demonstrated, the success rate of conservative treatment decreases in proportion to the delay in treatment. In our case too, the delay in diagnosis and treatment necessitated the need for operative intervention. Unless the CT imaging demonstrates fusion between the subluxated elements, a posterior approach for operative reduction and stabilization of the deformity is fairly simple and straightforward. The sacrifice of the stretched C2 root is often necessary for access to the luxated atlantoaxial joints. Possibly, the demonstration of a perched C1 facet may predict the failure of conservative management and attempts at closed reduction.
CONCLUSION
Atlantoaxial rotatory dislocations are rare in adults. Early diagnosis and treatment can allow closed reduction and bracing as an optimal treatment. High success rates have been reported with conservative therapy in patients with promptly diagnosed, stable, rotatory atlantoaxial dislocation not associated with transverse ligament disruption. When reduction is not possible, it is advisable to perform surgery as soon as possible to reduce the dislocation and stabilize the joint. Delay in treatment is associated with worse outcome and permanent changes in muscle and ligaments. We would like to stress the importance of evaluation of posttraumatic torticollis in adults by specialists and the need to maintain a high index of suspicion for AARD.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.