


Abstract
Background No prior work has explored whether the presence of degenerative spondylolisthesis impacts patient-reported outcome measurements (PROMs) after an anterior cervical discectomy and fusion (ACDF); therefore, the goal of the current study was to determine whether the presence of a spondylolisthesis affects PROMs after an ACDF.
Methods A retrospective cohort study was conducted on patients over the age of 18 who underwent a 1- or 2-level ACDF. All patients received preoperative standing lateral x-rays and were placed into 1 of 2 groups based on the presence of cervical spondylolisthesis from C2-T1: (1) no spondylolisthesis (NS) group or (2) spondylolisthesis (S) group. Preoperative, postoperative, and delta (postoperative minus preoperative) were recorded and compared between groups via univariate and multivariate analysis. Outcomes reported were the Physical Component Scores of the Short Form-12 (PCS-12), the Mental Component Scores of the Short Form-12 (MCS-12), the Neck Disability Index (NDI), and visual analog scale (VAS) Arm/Neck.
Results A total of 202 patients were included in the final analysis with 154 in the NS group and 48 in the S group. Both patient cohorts reported significant postoperative improvement in PCS-12, NDI, and VAS Arm/Neck. When comparing outcome scores between groups, only MCS-12 delta scores were different between groups, with the S group exhibiting a greater mean delta score (8.3 vs 1.3, P = 0.024) than the NS group after ACDF. Multiple linear regression analysis indicated having spondylolisthesis at baseline was a significant predictor of greater change in MCS-12 than the NS group (β = 4.841; 95% CI, 0.876, 8.805; P = 0.017).
Conclusion Both groups demonstrated significant postoperative improvement in PCS-12, NDI, or VAS Neck/Arm pain scores with no significant differences between groups. Patients with spondylolisthesis were found to have significantly greater improvement scores in MCS-12 scoring than those without spondylolisthesis after ACDF surgery.
- patient-reported outcome measurements (PROMs)
- physical component score of the SF-12 (PCS-12)
- mental component score of the SF-12 (MCS-12)
- neck disability index (NDI)
- visual analog scale neck pain (VAS Neck)
- visual analog scale arm pain (VAS Arm)
- anterior cervical discectomy and fusion (ACDF)
- cervical spondylolisthesis
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is commonly performed in the treatment of degenerative disorders of the cervical spine. Approximately 132 000 ACDFs are performed each year in the United States for cervical radiculopathy and myelopathy.1,2 Within the realm of degenerative cervical conditions, spondylolisthesis is a relatively common finding, with reports of up to 10% to 21% of patients undergoing surgical intervention related to symptomatic degenerative disc disease of the cervical spine and has received increased attention in recent years.3–7
Improvement of neurologic function and/or reduction in pain are key objectives of any spine surgery, though the impact of cervical spondylolisthesis on outcomes has yet to be clearly defined.5,7 The presence of anterolisthesis specifically has been reported to cause a greater degree of myelopathic symptoms in those patients with cervical spondylolisthesis, and prior literature describes an insidious progression of myelopathic disease with cervical spondylolisthesis.4 However, there is currently conflicting data on the clinical impact of correcting horizontal displacement and instability in patients with cervical spondylolisthesis.8 The data that do exist on the matter is sparse as it pertains to ACDF.
Furthermore, patient-reported outcome measures (PROMs) are becoming increasingly utilized in spine surgery as these scales tend to reflect the quality of surgical intervention.9–11 No prior work has explored whether the presence of degenerative spondylolisthesis impacts PROMs after an ACDF; however, considering the negative impact that the presence of cervical spondylolisthesis has on individuals suffering with myelopathy, it would be useful to determine whether ACDF surgery has any benefit in reducing the chronic burden of degenerative cervical pathology in the presence of cervical spondylolisthesis using PROMs as an objective measure of postoperative improvement. Hence, the purpose of this study was to determine the effect of degenerative cervical spondylolisthesis on a variety of commonly utilized cervical-spine–specific PROMs following ACDF for degenerative cervical radiculopathy and/or myelopathy.
METHODS
Patient Selection and Cohort Creation
Following Institutional Review Board approval, a retrospective database analysis was conducted on all available patients at a single institution who received either 1- or 2-level ACDF surgery between January 1, 2011, and December 31, 2016. Individuals were retained if they met the following inclusion criteria: (1) older than 18 years; (2) clinical symptoms of radiculopathy, myelopathy, or mixed radiculomyelopathy; (3) operative diagnosis of degenerative cervical pathologies including disc herniation, spinal stenosis, foraminal stenosis, spondylosis, etc. Anyone with the following characteristics was excluded from the final cohort: (1) less than 1 year of documented clinical follow-up; (2) evidence of greater than 1 level of cervical spondylolisthesis; (3) greater than 2-level ACDF surgery received; (4) surgical intervention to address tumor, infection, trauma, or revision of a prior instrumented cervical fusion surgery. Cervical spondylolisthesis was diagnosed by a group of 10 fellowship-trained, orthopedic spine surgeons by interpreting a discontinuity in the posterior vertebral line (from C2-T1) on standing, lateral x-rays obtained at preoperative office encounters (Figure). The present authors verified the clinical presence or absence of cervical spondylolisthesis through a manual chart review of operative records documenting the surgical diagnosis. Patients were then split into groups based on the presence or absence of cervical spondylolisthesis: (1) no spondylolisthesis (NS) group or (2) spondylolisthesis (S) group.

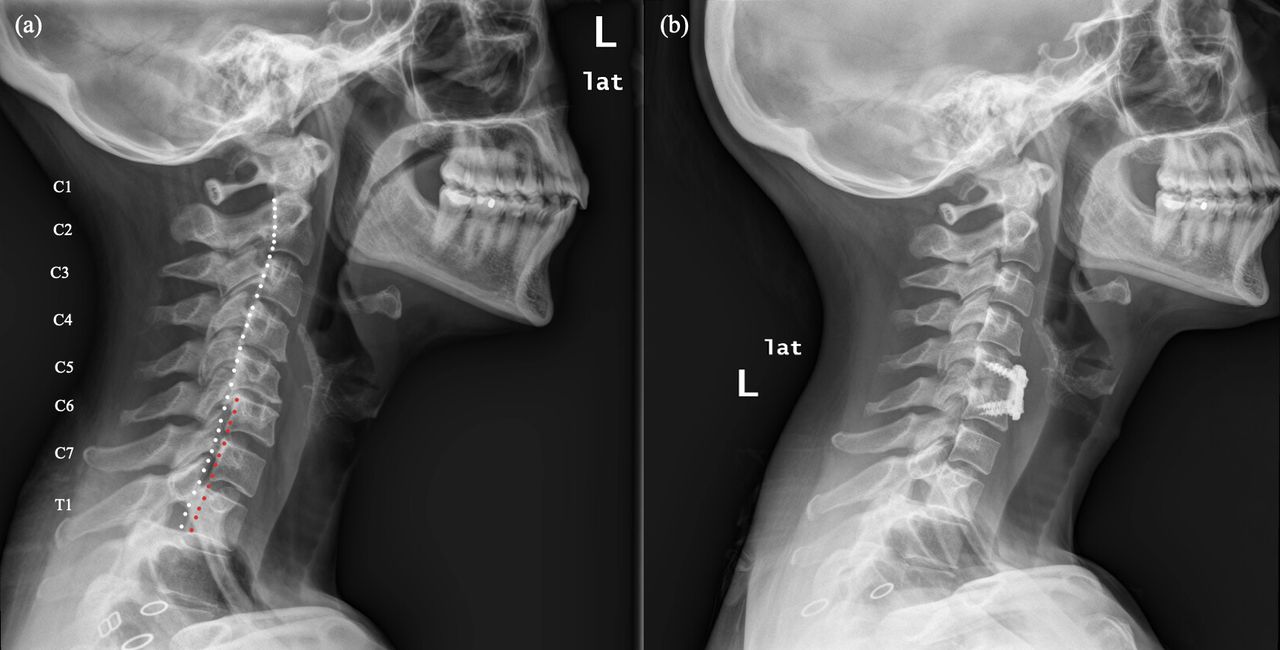
Radiographic interpretation and diagnosis of cervical spondylolisthesis. Cervical spondylolisthesis was diagnosed by a group of 10 fellowship-trained, orthopedic spine surgeons by interpreting a discontinuity in the posterior vertebral line (from C2-T1) on standing, lateral x-rays obtained at preoperative office encounters. (A) Preoperative, lateral film demonstrating discontinuity of posterior vertebral line between C5 and C6. (B) Postoperative, lateral film after single-level anterior cervical discectomy and fusion.
Outcomes
After the final cohort of patients was established, each individual health record was queried for various demographic factors, including age, sex, body mass index (BMI) (kg/m2), smoking status, and worker’s compensation status. For patients in the spondylolisthesis group, the level of spondylolisthesis was identified and recorded for each individual. Next, a thorough review of prospectively gathered pre- and postoperative PROMs from individual queries through OBERD (OBERD, Columbia, MO) was conducted, including the Neck Disability Index (NDI), the Physical and Mental Component Scores of the Short Form-12 Health Survey (PCS-12 and MCS-12), and the visual analog scale (VAS) neck and arm pain scores.
Statistical Analysis
A paired samples t test was used to assess change for each PROM within each group. A Mann-Whitney U test was used to compare continuous variables between groups and the Pearson’s  or Fisher’s exact test was used to compare categorical variables between groups. Multiple linear regression was performed to determine whether the presence of spondylolisthesis predicted worse improvement in PROMs adjusting for demographic and surgical variables. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS; IBM, Armonk, NY) version 24. Statistical significance was defined using a threshold of P < 0.05.
or Fisher’s exact test was used to compare categorical variables between groups. Multiple linear regression was performed to determine whether the presence of spondylolisthesis predicted worse improvement in PROMs adjusting for demographic and surgical variables. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS; IBM, Armonk, NY) version 24. Statistical significance was defined using a threshold of P < 0.05.
RESULTS
Demographics
A total of 202 patients were identified who met the inclusion criteria. Of those 202 patients, 154 (76.2%) were included in the NS group and 48 (33.8%) in the S group. The mean age of all included patients was 56.0 (95% CI, 54.0, 57.0), with the S group having a significantly older average age than the NS group (60 vs 54; P < 0.001). The total number of males included was 102 (50.5%), and the mean BMI was 30.1 (95% CI, 29.2, 31.0) kg/m2, with the S group having a significantly lower BMI than the NS group (28.7 vs 30.6; P = 0.046). There was a total of 15 smokers (7.4%), 29 (14.4%) patients with a clinical diagnosis depression, and 10 (5.0%) patients with a diagnosis of diabetes mellitus prior to surgical intervention. The average final follow-up was 14.6 months (range: 12–18 months). There were no other statistically significant differences in demographics between groups. All patients in the S group had anterolisthesis. One (2.1%) patient was found to have a spondylolisthesis at C2-C3, 12 (25.0%) at C3-C4, 13 (27.1%) at C4-C5, 11 (22.9%) at C5-C6, 1 (2.1%) at C6-C7, and 10 (20.8%) at C7-T1.
Patient-Reported Outcome Measurements
Both the NS and S groups demonstrated a significant change from baseline to postoperative measurements with regard to most PROMs. One notable exception was the NS group, which did not demonstrate any statistically significant postoperative change in MCS-12 scores. Comparing PROM between groups, the baseline, postoperative, and ΔPROMs were all similar with respect to NDI, PCS-12, VAS Neck, and VAS Arm pain scores. Alternatively, when considering MCS-12 scores, the S group demonstrated more disability at baseline (44.1 vs 48.0, P = 0.044); however, these individuals demonstrated greater Δ outcome scores (8.3 vs 1.3, P = 0.010) after surgical intervention. Multivariate analysis indicated that the presence of cervical spondylolisthesis was associated with greater improvement in MCS-12 scores at final follow-up (β = 4.841; 95% CI 0.876, 8.805; 0.017). No other PROMs appeared to significantly influence patient outcomes after multivariate analysis. PROMs between groups are shown in the Table.
Patient-reported outcome measurements between cervical spondylolisthesis groups.
DISCUSSION
Although ACDF for degenerative disease is a commonly performed  procedure with effective clinical outcomes, the impact of spondylolisthesis in the treatment of degenerative cervical spondylosis is not well studied. Increasingly, PROMs are relied upon as an evaluation of treatment quality in spine surgery.9–11 As the body of literature has grown, cervical spondylolisthesis has become a more common consideration in the treatment of degenerative cervical spine disorders. Considering the negative impact that the presence of cervical spondylolisthesis may have on perioperative myelopathy symptoms, it would be useful to determine whether the presence of this preoperative diagnosis influences surgical outcomes following ACDF to address degenerative cervical pathology.12,13 Therefore, the primary aim of this study was to evaluate the effect of cervical spondylolisthesis among patients undergoing ACDF for degenerative cervical radiculopathy and/or myelopathy utilizing cervical-spine–specific PROMs as objective criteria for postoperative improvement.
procedure with effective clinical outcomes, the impact of spondylolisthesis in the treatment of degenerative cervical spondylosis is not well studied. Increasingly, PROMs are relied upon as an evaluation of treatment quality in spine surgery.9–11 As the body of literature has grown, cervical spondylolisthesis has become a more common consideration in the treatment of degenerative cervical spine disorders. Considering the negative impact that the presence of cervical spondylolisthesis may have on perioperative myelopathy symptoms, it would be useful to determine whether the presence of this preoperative diagnosis influences surgical outcomes following ACDF to address degenerative cervical pathology.12,13 Therefore, the primary aim of this study was to evaluate the effect of cervical spondylolisthesis among patients undergoing ACDF for degenerative cervical radiculopathy and/or myelopathy utilizing cervical-spine–specific PROMs as objective criteria for postoperative improvement.
The results of the current study suggest that all patients have subjective improvement of pain and physical outcomes regardless of the presence of spondylolisthesis after ACDF, but those with cervical spondylolisthesis have a distinct improvement in mental health domains after anterior cervical fusion that is not experienced by patients without cervical spondylolisthesis. Both NS and S groups demonstrated a significant change over time for all PROMs included, except MCS-12 among the NS group. Specifically, with regard to MCS-12 scores, the S group demonstrated significantly greater baseline disability (44.1 vs 48.0, P = 0.044); however, they also reported greater Δ scores (8.3 vs 1.3, P = 0.010) than the NS group after surgical intervention. Furthermore, multivariate analysis demonstrated that cervical spondylolisthesis was associated with greater improvement in MCS-12 scores (β = 4.841 [0.876, 8.805], 0.017). Considering physical pain and functional parameters, there were no significant differences between groups in terms of baseline, postoperative, or delta outcome scores for NDI, PCS-12, VAS Neck, and VAS Arm pain scores. Finally, multivariate analysis indicated that the presence of cervical spondylolisthesis was not a significant predictor of greater improvement in any of these domains.
Previous studies have demonstrated that patient-reported outcomes and patient-reported satisfaction following ACDF are multifactorial. Andresen et al conducted a retrospective study evaluating PROMs in patients undergoing surgical treatment for cervical radiculopathy. The authors identified strong correlations between patient satisfaction and obtaining MCID in VAS Neck or SF-12 PCS.14 Godil et al conducted a prospective cohort study in patients undergoing ACDF to evaluate the relative responsiveness of PROMs to changes in pain and quality of life. They remarked that while NDI score is the most valid and responsive measure of improvement in pain and disability after cervical surgery, only the SF-12 PCS could accurately discriminate meaningful improvement in quality of life. Moreover, they identified SF-12 MCS as a poor discriminator after cervical surgery.15 These studies imply that improvements in the mental domain may not have a great clinical relevance to patient-perceived outcomes after ACDF. While this study did not evaluate satisfaction related to the spondylolisthesis, based on the observed PROMs, the aforementioned studies would suggest that similar satisfaction would be expected. Segar et al found that patients with a spondylolisthesis adjacent to an ACDF showed similar improvements in pain, disability, and function compared to those without.16
Limitations
To date, this is one of the first studies to compare PROMs between patients with and without spondylolisthesis; however, patient data and responses were not collected prospectively. Additionally, the smaller sample size of the cohort and uneven group numbers make the results of the present analysis prone to errors in variance; however, we wanted to include all available patients for the purpose of our analysis. Furthermore, this study classified spondylolisthesis in a clinical fashion and confirmed the presence of this diagnosis with a manual review of operative reports. The present study may have benefited from a radiographic outcome analysis utilizing various features described by previous authors, who subclassified severity of cervical spondylolisthesis and incorporated important modifiers. Woiciechowsky et al characterized spondylolisthesis into three categories according to radiographic findings such as facet joint degeneration and vertebral body degeneration.5 Kawasaki et al designated 2.0 mm or less displacement, 2.0 to 3.4 mm displacement, and 3.5 mm or more displacement as mild, moderate, and severe spondylolisthesis, respectively.6 Facet joint degeneration and subluxation as key features in degenerative spondylolisthesis and future studies may subcategorize the S group to better elucidate these initial findings, though the goal of this study was to establish the effect on PROMs by the presence of any spondylolisthesis.5,7,17,18 Finally, if the study group were divided, results from any subgroup would have been underpowered.
CONCLUSION
Patients with cervical spondylolisthesis reported similar improvement in all physical pain and functioning outcome surveys after ACDF than those without this diagnosis. While larger trials with more descriptive subclassifications for type and degree of cervical spondylolisthesis should be conducted to further elucidate this relationship, the present study suggests that patients with cervical spondylolisthesis should expect subjective improvement in pain and functionality following ACDF that is on par with those who do not have spondylolisthesis.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The author(s) report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
Ethics Approval This study was approved by the Institutional Review Board at the Thomas Jefferson University Hospital. Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Keywords
- patient-reported outcome measurements (PROMs)
- physical component score of the SF-12 (PCS-12)
- mental component score of the SF-12 (MCS-12)
- neck disability index (NDI)
- visual analog scale neck pain (VAS Neck)
- visual analog scale arm pain (VAS Arm)
- anterior cervical discectomy and fusion (ACDF)
- cervical spondylolisthesis