


Abstract
Background The clinical outcome of anterior cervical decompression and fusion (ACDF) correlates with fusion rates. There is a debate about how patients with symptomatic pseudarthrosis should be managed. In this study, a treatment plan is developed based on the surgical results of 95 patients and the recent literature.
Methods A retrospective study to evaluate the long-term results after surgical treatment of symptomatic pseudarthrosis after ACDF. Between 1994 and 2015, 95 patients underwent surgery due to symptomatic pseudarthrosis after ACDF. The diagnosis was confirmed with dynamic radiographs and computed tomography scans. The approach used was anterior in 62 (65.1%), posterior in 13 (13.7%), and combined anterior and posterior in 20 (21.2%) patients. The operative details and the radiological and clinical results were analyzed.
Results The primary operation was fusion using cages in 70, bone graft and plate in 16, and bone graft only in 9 patients. The revision was performed after a mean of 27 months. After a mean follow-up of 52 months, the mean Visual Analog Scale improved from 7.5 to 2.3 (P = 0.001), and the mean Neck Disability index improved from 26.4 to 8.7 (P = 0.034). Fusion was achieved in all patients after a mean of 7.8 (SD 2.9) months. Reoperation was indicated in 4 patients, all of whom were in the anterior-only group, and was due to retropharyngeal hematoma in 1 patient and cage sinking with kyphosis in 3 patients.
Conclusions Solid arthrodesis significantly improves the symptoms of cervical pseudarthrosis patients. The presence of adjacent segment disease, implant migration, residual stenosis, and segmental kyphosis plays an important role in decision-making. A treatment recommendation plan has been suggested.
Level of Evidence 4.
INTRODUCTION
Anterior cervical decompression and fusion (ACDF) was first described in 1950 by Smith and Robinson.1 In the past 2 decades, several modifications were introduced in the surgical technique. Furthermore, implants’ use to support fusion and restore and preserve the cervical sagittal profile during healing is introduced.2–7 The fusion rate after ACDF varies between the different fusion techniques with a wide range of fusion rates between 30% and 90%. The rate of pseudarthrosis increases in multisegmental fusion.8–10
The definition of pseudarthrosis is still debatable, with recent literature recommendation to use the dynamic lateral cervical spine views as a diagnostic method. A change of more than 1 mm in the distance between the spinous processes’ tips between the 2 adjacent vertebrae is an indicator of pseudarthrosis.11 A computed tomography (CT) scan with a lack of bridging trabecular bone between the 2 fused vertebrae and radiolucency between the graft or the implant and the vertebral endplates is an indicator of the failure of fusion.11,12
Diagnosis of symptomatic pseudarthrosis can be based on nonunion being observed radiographically and on clinical symptoms after the exclusion of other causes for the symptoms.9–14 Some pseudarthrosis patients have a stable, tight fibrous nonunion, whereas others have an unstable mobile nonunion.15 In patients with recurrent or persistent neck pain, however, pseudarthrosis is a possible cause of neck symptoms. Therefore, an accurate diagnosis is essential for the management of pseudarthrosis.16
The surgical management of symptomatic cervical spine pseudarthrosis can be through anterior, posterior, or combined anterior and posterior approaches.17–20 Decision-making should be based on the pathology and the presence of implant failure or a concomitant adjacent segment disease (ASD).19Despite the availability of many papers discussing the management of the cervical spine pseudarthrosis, an organized plan for the surgical approach is lacking.
In this study, the surgical treatment of symptomatic cervical pseudarthrosis after ACDF was analyzed to develop a plan for this pathology’s surgical treatment based on the results obtained in this work and the current literature.
MATERIAL AND METHODS
Data Collection
All data of the surgically treated patients in our department were prospectively recorded, including preoperative data, operative profile, and the regular postoperative follow-up. In this study, a retrospective analysis of this prospectively collected data was performed. Between 1994 and 2015, 95 patients were operated on for symptomatic cervical spine pseudarthrosis after ACDF. The clinical presentation, together with the Neck Disability Index (NDI) and the visual analog scale (VAS), was collected. The time lapse between the index operation (the first fusion procedure) and the revision surgery, the radiological examinations, the duration of symptoms, the surgical approach, the intraoperative findings, and the postoperative clinical and radiological outcomes were analyzed. Acceptance from our institutional ethical review board was obtained before conduction of this analysis (Number 2019-213)
Inclusion Criteria
The index operation was performed for a cervical spine degenerative disease (cervical spondylosis). The duration of symptoms was more than 12 months, with the conservative treatment’s failure to adequately reduce the symptoms. The diagnosis of pseudarthrosis was based on radiological and clinical examination. Radiologically, a cervical spine lateral view in flexion and extension was performed, and a preoperative CT scan was performed. Magnetic resonance imaging (MRI) examination was performed to evaluate the adjacent segments and exclude other causes of the symptoms. An independent radiologist evaluated all cases before the surgical intervention. Clinically, the VAS was 5 or more despite the conservative treatment. Patients operated due to fractures, tumors, or spondylodiscitis were excluded from this study.
Surgical Technique
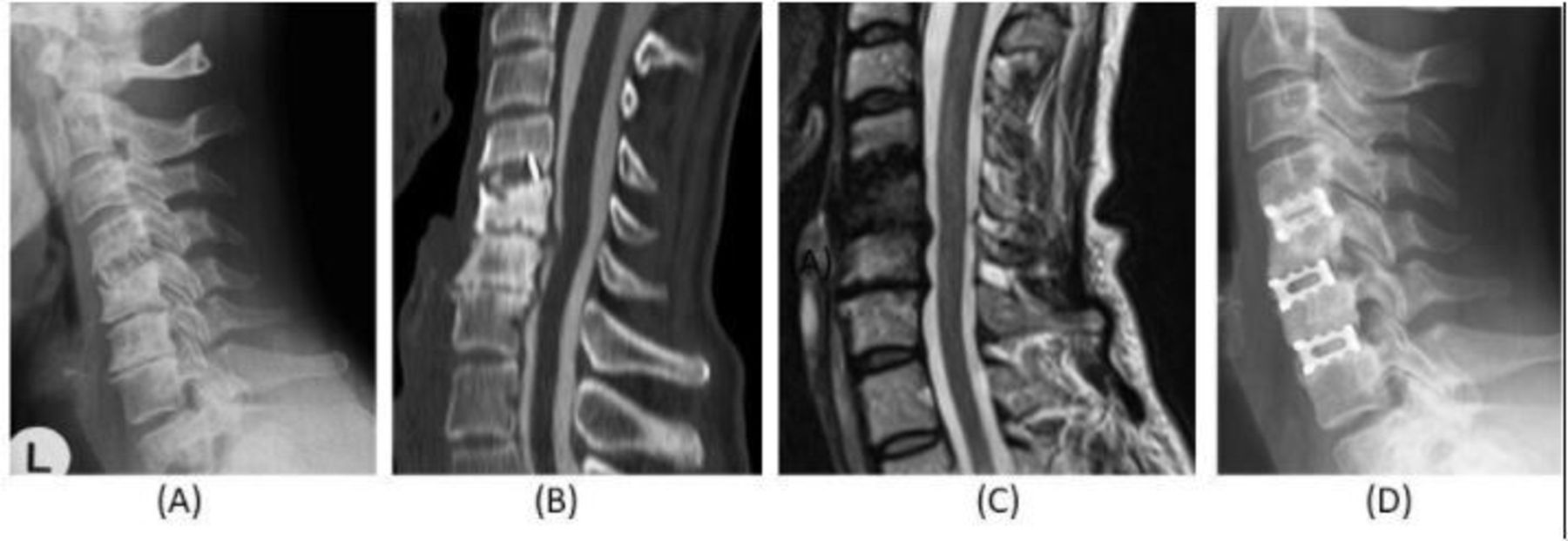
Three surgical approaches were applied. The anterior approach was used in 62 patients (Figure 1). A standard right-sided anterior cervical approach was used, followed by removal of the implants and excision of the fibrous pseudarthrosis tissue. Re-fusion was then performed using titanium cages filled with iliac bone graft. In cases with ASD, the adjacent segments were concomitantly decompressed and fused. A cervical orthosis was used for 3 to 6 weeks postoperatively.

(A) Plain x-ray, (B) preoperative computed tomography, and (C) preoperative magnetic resonance imaging of a 52-year-old male patient presenting with symptomatic pseudarthrosis C4/5 18 months after anterior cervical decompression and fusion (ACDF). The preoperative workup showed an additional adjacent segment disease, C5-7. He was treated by anterior revision and ACDF C5-7 and achieved solid arthrodesis at the final follow-up (D).
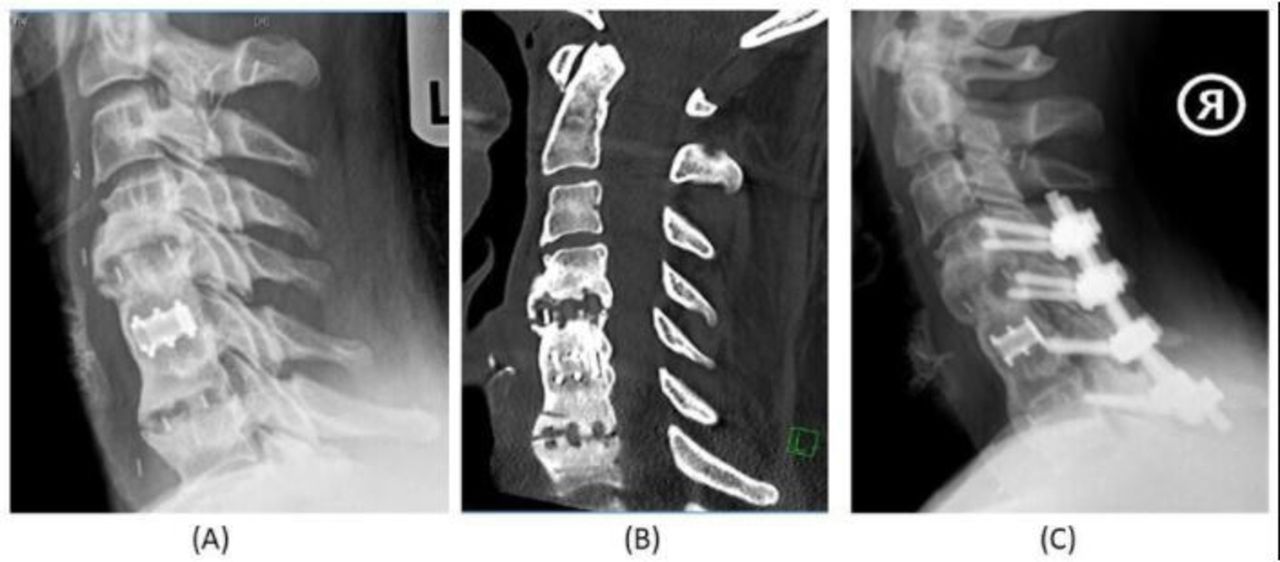
The posterior approach was applied in 13 patients (Figure 2). A posterior midline cervical approach was used, followed by posterior instrumentation using a lateral mass screw-rod system or reconstruction plates combined with posterior fusion using an iliac bone graft. These patients had a preserved cervical spine lordosis and had no ASD or anterior implant failure.

(A) Plain x-ray and (B) preoperative computed tomography of a 45-year-old female patient presenting with symptomatic pseudarthrosis C4/5 and C6/7 3 years after anterior cervical decompression and fusion. She was treated by posterior fusion and achieved solid arthrodesis 2 years postoperatively (C).
The third group included 20 patients undergoing a combined approach. Anteriorly, the pseudarthrosis was excised, and a re-fusion was performed using cages and bone graft. Posteriorly, a posterior midline incision with the lateral mass screw-rod system or a reconstruction plate and fusion using iliac bone graft was used. This group of patients had either a long segment fusion (3 levels or more) or a bad bone quality with osteoporosis (proved after a preoperative dual-energy x-ray absorptiometry [DEXA] scan).
Outcome Assessment
All patients had a scheduled postoperative follow-up after 3, 6, and 12 months for an x-ray imaging as well as clinical examination; follow-ups then occurred yearly. NDI and VAS were used to assess the clinical outcome. Postoperative dysphagia was assessed using the Bazzaz score.21 Any graft-related complications were recorded. Bony fusion in the follow-up visits was used as the radiological outcome of the procedure using x-rays with functional lateral views and CT scans. The measurement of the cervical lordosis between C2 and C7 in the lateral x-rays was measured. The duration until the fusion was recorded, and the causes for revision were analyzed.
Data Analysis
The data were analyzed using SPSS statistical software on an IBM-compatible computer. The mean and the standard deviation were used to calculate the numerical variables. The student t test was used to compare numerical values, and the  test was used to compare the nominal values.
test was used to compare the nominal values.
RESULTS (Table 1)
Summary of the clinical and surgical data during the study period (N = 95).
Preoperative Data
There were 47 females and 48 males with a mean age of 54.3 ± 12.2 years. The index surgery was a 1-level fusion in 20 patients, 2-level fusion in 40 patients, 3-level fusion in 26 patients, and 4- or more-level fusion in 9 patients. The applied surgical techniques in these index ACDFs consisted of using cervical fusion cages in 70 patients, bone graft and plate in 16 patients, and bone graft only in 9 patients. In 75 patients, a single-level pseudarthrosis was operated on, and in the remaining 20 patients, the revision was on 2 levels. In 16 patients, an ASD was present at the pseudarthrosis surgery time and was simultaneously managed. Fifty-five patients had the index operation in our department, and 40 patients were referred to our department for the revision surgery, but the index operation was performed elsewhere. This study did not analyze the causes or the rates of pseudarthrosis. Many patients were managed elsewhere, and only the revisions were performed in our department.
All patients had persistent neck pain and cervical instability symptoms. In 46 patients, cervical radiculopathy in 1 or more cervical levels was recorded. Mixed radiculopathy and myelopathy were present in 18 patients, and 5 patients had cervical myelopathy without radiculopathy. The mean preoperative NDI was 26.4 (SD 5), and the mean VAS was 7.5 (SD 2). The mean time lapse between the index operation and the revision surgery was 27 (SD 11.6) months (minimum 12 months and maximum 50 months). All patients had a preoperative MRI examination, 85 patients had a preoperative CT scan to confirm the pseudarthrosis, and in 10 patients, the diagnosis was based only on plain x-ray examination with dynamic views without CT examination. The mean preoperative lordosis measured from C2-C7 on a neutral lateral x-ray was 8.75 (SD 5.4) degrees. Cage sinking was present in 42 patients (44%), while plate and screw loosening was present in 12 patients (12.6%).
Operative Data
The mean operative time was 143 (SD 70) minutes (range, 35–310 minutes). For the anterior-only group, the mean operation time was 130 (SD 60) minutes (range, 35–285 minutes). For the posterior-only group, the mean operative time was 123 (SD 68) minutes (range, 40–285 minutes). For the combined anterior and posterior group, the mean operative time was 193 (SD 74) minutes (range, 100–310 minutes). The difference between the anterior-only and the posterior-only group was statistically insignificant (P = 0.08), whereas the combined anterior and posterior group had a significantly longer operation time (P = 0.01).
The mean blood loss was 577 (SD 440) mL (range, 20–1500 mL). The mean blood loss for the anterior group was 208 (SD 150 mL) (range, 20–650 mL). For the posterior group, the mean blood loss was 710 (SD 560) mL (range, 250–2800 mL). For the anterior-posterior group, the mean blood loss was 1070 (SD 850) mL (range, 200–4000 mL). The anterior group had significantly less blood loss (P = 0.03), whereas the posterior group did not differ significantly from the combined anterior and posterior group (P = 0.07), the posterior approach being responsible for the main blood loss. There were no intraoperative complications in any of the 3 groups.
Postoperative Data
The mean postoperative follow-up was 52 (SD 28) months (minimum 24 and maximum 120 months). Fusion was achieved in all cases after a mean of 7.8 (SD 2.9) months (range, 6–12 months). The mean cervical lordosis improved significantly from 8.75 (SD 5.4) degrees preoperatively to 12.6 (SD 4.4) degrees at the final follow-up (P = 0.01). However, the mean lordosis angle improvement in the posterior-only group (13 patients) from 10.4 (SD 2.3) preoperatively to 11.7 (SD 3.2) degrees at the final follow-up did not reach the statistical significance level (P = 0.07). Clinically, at the end of the follow-up period, the mean NDI improved to 8.7 (SD 3.2), and the mean VAS reached 2.3 (SD 1.7). The changes in both being statistically significant. (P = 0.034 and 0.001). At the end of the follow-up, 3 patients (3.3%) still had mild dysphagia and 5 (5.2%) patients had graft site pain.
After the revision surgery, reoperation was necessary for 4 patients (4.2%); all were in the anterior-only approach. In 1 patient, the revision was due to a retropharyngeal hematoma presented with postoperative dysphagia after 2 days postoperatively and was revised without any persistent symptoms. The revision was due to cage subsidence and partial loss of lordosis in the remaining 3 patients after an anterior-only revision. The 3 patients had a long segment fusion (3 levels in 2 patients and 4 levels in 1 patient). These patients had a DEXA scan and proved to have osteoporosis. They were managed by a posterior lateral mass fixation and fusion and achieved a solid fusion after a mean of 4.5 months. Patients who underwent a posterior-only approach and had a combined anterior and posterior approaches did not have reoperations.
DISCUSSION
ACDF is a widely used surgical method for the treatment of cervical degenerative disease. Pseudarthrosis is a possible complication of this procedure, with rates up to 50% in multilevel constructs, and is sometimes related to unsatisfactory postoperative results. However, pseudarthroses are not always symptomatic and often do not require surgical intervention.20 Treatment of symptomatic pseudarthrosis can be accomplished by anterior revision procedure or posterior or a combination of both. To date, there remains considerable debate in the literature as to the optimal method for the management of pseudarthrosis.10,22
Diagnosis of Pseudarthrosis
Determining the fusion status after ACDF can be challenging for both surgeons and radiologists. Ghiselli et al analyzed the different radiological methods to diagnose pseudarthrosis and recommended the measurement of the segmental Cobb angle in the dynamic views to predict pseudarthrosis.20,22 Cannada et al proved that a motion exceeding 1 or 2 mm between the spinous processes of the involved segments on maximal flexion-extension views is more accurate than the Cobb angle method proposed by Ghiselli et al, and their technique has been applied in the current work.15 However, this method has an important limitation, as patients with symptomatic pseudarthrosis suffer from neck pain and might not be able to perform maximal flexion and extension to get trustable measurements in the dynamic views. That is why most patients in this series received a CT examination (85/95), including sagittal and coronal reconstructions, to establish pseudarthrosis diagnosis in doubtful cases. This fact had been confirmed by Ploumis et al, who compared CT scans with flexion/extension radiographs to determine pseudarthrosis. They found pseudarthrosis rates on CT scans to range up to 31%, with a lower rate of pseudarthrosis detected by radiographs using 2 mm of spinous process displacement as the criteria.23
Surgical Approach
The surgical approach in terms of anterior vs posterior must be decided upon in planning the revision surgery.10 Each approach has its advantages and disadvantages. Proponents of the anterior approach highlight the lower rates of wound complications, access to anterior pathology and graft or implant migration, and the pseudarthrosis site’s exploration.24,25 Furthermore, the anterior approach offers biomechanical advantages, allowing for better restoration of normal cervical lordosis and is associated with less postoperative stiffness and pain.18,24
Contrary to these reports, several studies support using the posterior approach for the revision procedure, avoiding scar tissue and anterior wound complications.10,22 Additionally, a posterior revision provides new soft tissue planes and a native fusion bed.10 A meta-analysis conducted by McAnany et al indicated that the posterior approach offers a statistically higher and largely reproducible fusion rate than the anterior approach. However, posterior cervical fusion has been associated with more considerable intraoperative blood loss and a more extended hospital stay.22 This coincides with the results obtained in the current work, where the amount of blood loss was significantly more in the group undergoing posterior revision. On the other hand, the anterior approach applied in our patients demonstrated 2 types of complications. The first was retropharyngeal hematoma in 1 patient necessitating anterior reoperation, and the second was a mechanical complication with cage subsidence, necessitating posterior surgery. A similar result was obtained by Philips et al, who applied the anterior approach in 16 cases of symptomatic pseudarthrosis. Two patients in their series did not fuse and went on to undergo posterior fusions to achieve arthrodesis.26
Treatment Recommendations
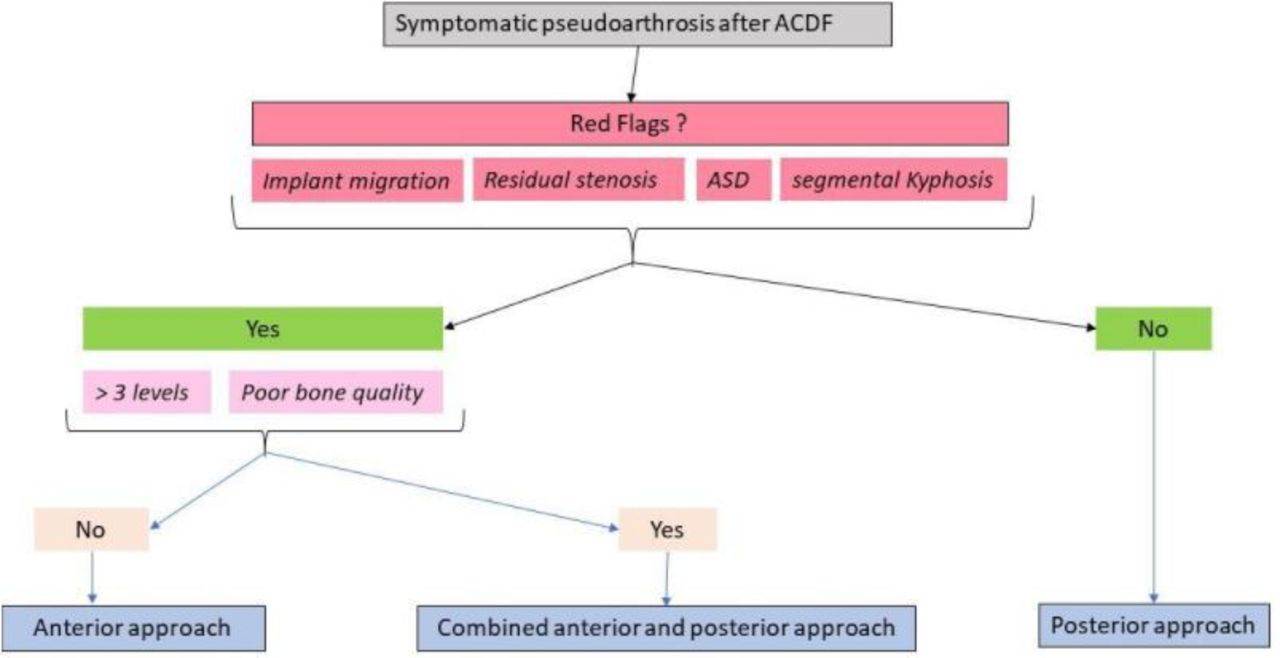
In the current case series, all patients had a significant improvement regardless of the used surgical approach; revisions and complications occurred only in patients with the anterior-only approach who had either a long segment fusion or osteoporosis (Figure 3).
Based on the results obtained in this work as well as on the literature mentioned above, a recommendation plan for the treatment of symptomatic pseudarthrosis after ACDF is suggested. Four findings were identified to help in decision-making: implant migration, residual stenosis, ASD, and segmental kyphosis. In the absence of these findings, the posterior approach is recommended to achieve solid arthrodesis. The presence of 1 or more of these findings necessitates anterior surgery. Once the decision for anterior surgery is taken, an additional posterior stabilization should be considered if the addressed pseudarthrosis extends for more than 3 levels or in case of low bone quality (DEXA scan). The suggested treatment recommendation plan is shown in Figure 3. Nevertheless, prospective randomized studies are needed to test the reproducibility of this plan.
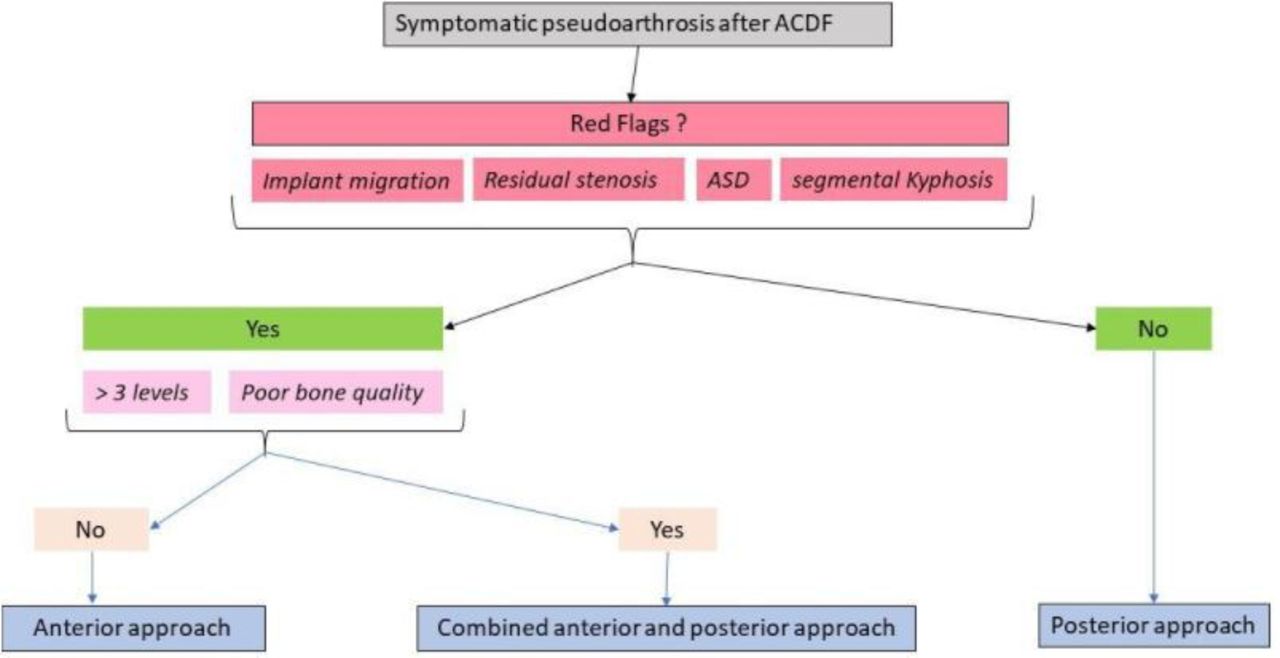
Treatment plan for symptomatic pseudarthrosis after anterior cervical decompression and fusion (ACDF). ASD, adjacent segment disease.
Despite the availability of many papers discussing the management of cervical spine pseudarthrosis, an organized plan for the surgical approach is lacking. This work’s primary goal is to combine the experience gathered over the years to manage cervical pseudarthrosis with the recent literature to produce a suggested plan for the surgical approach. In this work, an algorithm for the proper selection of the approach is introduced. Moreover, the current study with 95 patients represents one of the largest case series dealing with cervical pseudarthrosis’s surgical management (Table 2).
The number of studied patients and the mean follow-up in literature dealing with cervical spine pseudarthrosis.
Limitations
The study has some limitations. First, the study was a retrospective data analysis. Second, the presence of ASD in some patients may have been the cause of the symptoms and not only the radiological pseudarthrosis. Third, there was an unequal number of patients in each group.
CONCLUSIONS
Solid arthrodesis significantly improves the symptoms of cervical pseudarthrosis patients. The posterior approach is associated with more blood loss but a lower reoperation rate. Four findings have been identified, namely the presence of implant migration, residual stenosis, ASD, and segmental kyphosis. In the absence of these findings, the posterior-only approach is recommended. The presence of any of these red flags necessitates anterior revision. A combined approach should be considered in the presence of low bone quality and/or multilevel pseudarthroses.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.