


Abstract
Background Intraoperative (IO) image guidance surgery using 3-dimensional fluoroscopic navigation methods, such as the O-arm system, has improved the accuracy of pedicle screw placement in instrumented spine surgery. IO and postoperative (PO) validation of the implant’s correct position from radiological images is a decisive step to ensure patient safety and avoidance of complications related to implant misplacement. In this prospective single-center study, the authors investigated the accuracy and agreement of assessment of pedicle screws from IO O-arm images in comparison to PO computed tomography images. This study aimed to determine whether final evaluation of pedicle screws can safely be conducted from IO images that supersedes the PO computed tomography control.
Methods A prospective single-center study was carried out at the Spine Unit in the Department of Orthopedics at Umeå University Hospital between 2019 and 2021. All patients enrolled in the study underwent instrumented thoracolumbar spine surgery using navigation. Imaging data were obtained from IO and PO examinations. Four reviewers—2 attending senior spine surgeons, 1 final year resident in orthopedics, and 1 attending neuroradiologist—classified pedicle screws using the Gertzbein and Robbins classification system. Agreement and accuracy of the reviewers were studied to evaluate the assessment of pedicle screws from IO and PO images.
Results A total of 70 patients (422 screws) were included in the study. There was high accuracy among surgeons both on IO and PO images (0.96–0.97, 95% CI [0.94–0.99] and 0.97, 95% CI [0.94–0.99], respectively), and the overall agreement between all raters was 92% to 98% (95% CI [0.90, 1.00]). The discrepancy in assessment between optimal (Group 1) and suboptimal (Group 2) screws between IO and PO images was as low as 1% to 1.7%, which indicates that very few suboptimal screws are missed in the assessment of IO images.
Conclusions The assessment of navigated pedicle screws using IO images is safe and reliable and may replace the need for further assessment using PO imaging.
Level of Evidence 3.
- pedicle screw
- navigation
- intraoperative imaging
- image-guided surgery
- O-arm
- postoperative imaging
- computer tomography
- Gertzbein and Robbins classification system
INTRODUCTION
Intraoperative (IO) image guidance using 3-dimensional (3D) fluoroscopic navigation such as O-arm technology has improved both precision and reliability of pedicle screw placement in instrumented spine surgery.1–5 These technologies are routinely used in many spine centers worldwide. IO and postoperative (PO) evaluation and verification of implant position on radiological images are an important and decisive step during and after surgery to ensure surgical safety and avoid complications due to implant misplacement.
Computed tomography (CT) is widely accepted as a standard diagnostic procedure because its high resolution allows for the evaluation of the pedicle screw position with higher accuracy than conventional radiology.6–10 Thus, CT is frequently used for PO evaluation of spine implant positions.
IO 3D fluoroscopy may be extended beyond navigation and employed for IO radiological control of implants. Hence, the need for PO CT would be limited and lead to less radiation exposure, facilitating PO patient care and lowering cost of hospitalization.
This prospective study evaluates the accuracy and agreement in rating the positions of pedicle screws in the thoracolumbar spine from IO and PO images using the Gertzbein and Robbins classification system for pedicle screws.11 This study investigates whether the assessment of accuracy from IO imaging performed by spine surgeons can supersede PO assessment from CT images.
MATERIALS AND METHODS
A prospective study enrolling a total of 70 patients (422 screws included) was carried out at the Spine Unit, Department of Orthopedics, at Umeå University Hospital between 2019 and 2021. Enrolled patients received thoracolumbar spine surgery with open, mini-open, or minimally invasive techniques using either Solera 5.5/6.0 Spinal System (CD Horizon, Medtronic) or Longitude II (CD Horizon, Longitude II Multilevel Percutaneous Fixation System) with IO O-arm imaging integrated with StealthStation S8 navigation system. All surgeries were executed according to a local navigation protocol with a 2-step navigation process of navigated pedicle probing followed by navigated pedicle screw placement. The inclusion criteria were patients aged 18 years or older with an American Society of Anesthesiologists physical status score ≤3. Patients were also required to understand oral and written information and to provide written consent to participate in the study. The study included pathologies of the thoracolumbar spine such as fractures, degenerative spine diseases, and tumors. Spine deformities were excluded from the study as scoliosis surgery often poses further challenges for the assessment of screw placement.
In accordance with the current radiological protocol in our unit at Umeå University Hospital, patients who receive surgery using the IO O-arm Imaging System with StealthStation navigation system should also undergo PO control CT imaging regardless of the IO control using O-arm.
Hence, patients included in the study followed the current radiological protocol and underwent both IO 3D O-arm (3Mpx 1.5 × 2 k resolution; IO) and PO CT (standard 64 slice; PO) radiological investigation. The IO radiology included 3D imaging at the start of the surgery when a reference frame for navigation had been mounted on the patient, allowing for the IO image to be navigated on. At least 1 additional IO 3D scan was performed at the end of the surgery when all pedicle screws had been placed. This IO image was used for the assessment of the pedicle screw positions. The radiological image data collected were anonymized and stored in the image viewing software (Sectra) for further assessment. The assessment and rating of the pedicle screw position from IO and PO images were performed by 3 spine surgeons–2 senior spine surgeons (1 orthopedic spine surgeon and 1 spine neurosurgeon) with more than 10 years of postresidency experience and 1 junior surgeon in the final year of residency in orthopedics (surgeon reviewers 1, 2, and 3). The control assessment and rating of screw position were performed by a senior neuroradiologist (neuroradiologist reviewer) using PO images. The assessment of radiological images and rating of pedicle screw position was carried out in random batches distributed individually among the reviewers at different time intervals.
Data Assessment
All pedicle screws were assessed and rated on IO and PO images according to the Gertzbein and Robbins classification system11 (Table 1). All data were anonymized to the reviewers. The reviewers were blinded to each other’s assessments. All radiological images were viewed in the image viewing software Sectra.12
The Gertzbein and Robbins classification system for pedicle screw accuracy.3
Statistical Analysis
Descriptive statistics were used to evaluate the ratings of pedicle screw position from both IO and PO radiological investigations among surgeon reviewers 1, 2, and 3 and the neuroradiologist reviewer. The accuracy was calculated in 3 distinctive and consecutive steps. First, the accuracy of the screw rating from IO and PO images was calculated for surgeon reviewers 1, 2, and 3. Second, the accuracy was calculated between the surgeon reviewers 1, 2, and 3 both for screw ratings from IO and PO images. Third, the agreement between screw ratings between surgeon reviewers 1, 2, and 3 from IO and PO images was evaluated using the first-order agreement coefficient (AC1). This agreement was also studied between IO and PO ratings by the surgeon reviewer and the neuroradiologist reviewer from PO images. Only the PO ratings of the neuroradiologist were compared with the IO and PO ratings of the reviewers as neuroradiologists mainly judge PO CT images. AC1 was preferred to the traditional adjusted Kappa because of symmetrical data imbalance.13 All statistical analyses were conducted using R version 4.2.1.14
RESULTS
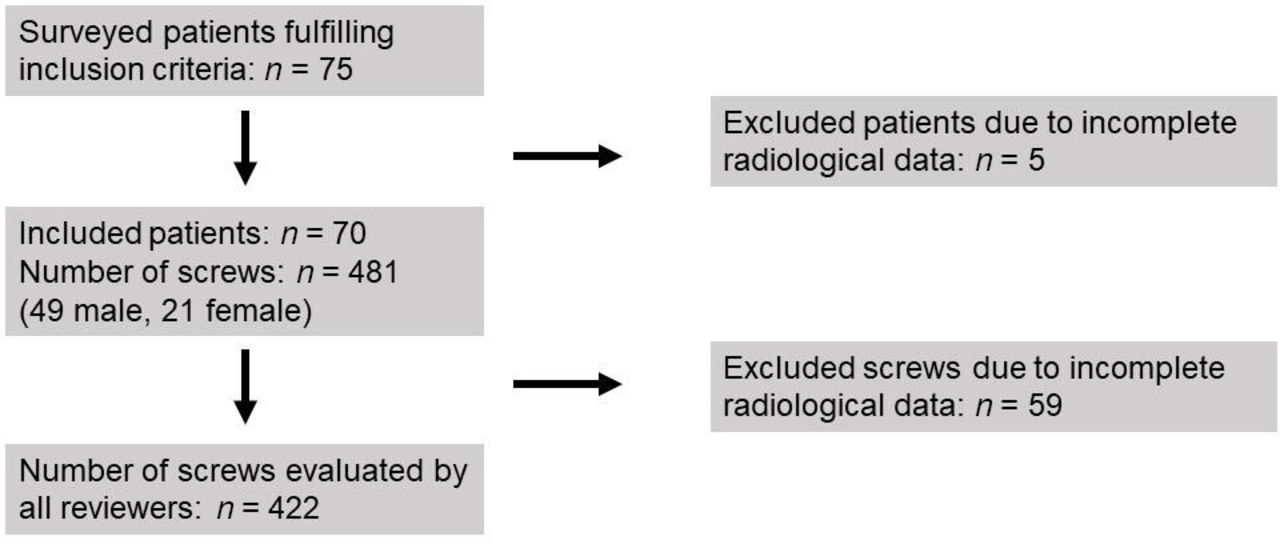
A total of 70 patients were enrolled in the study with 481 screws implanted; however, incomplete radiological imaging of 59 screws resulted in only 422 screws being classified by all reviewers (Figure 1).
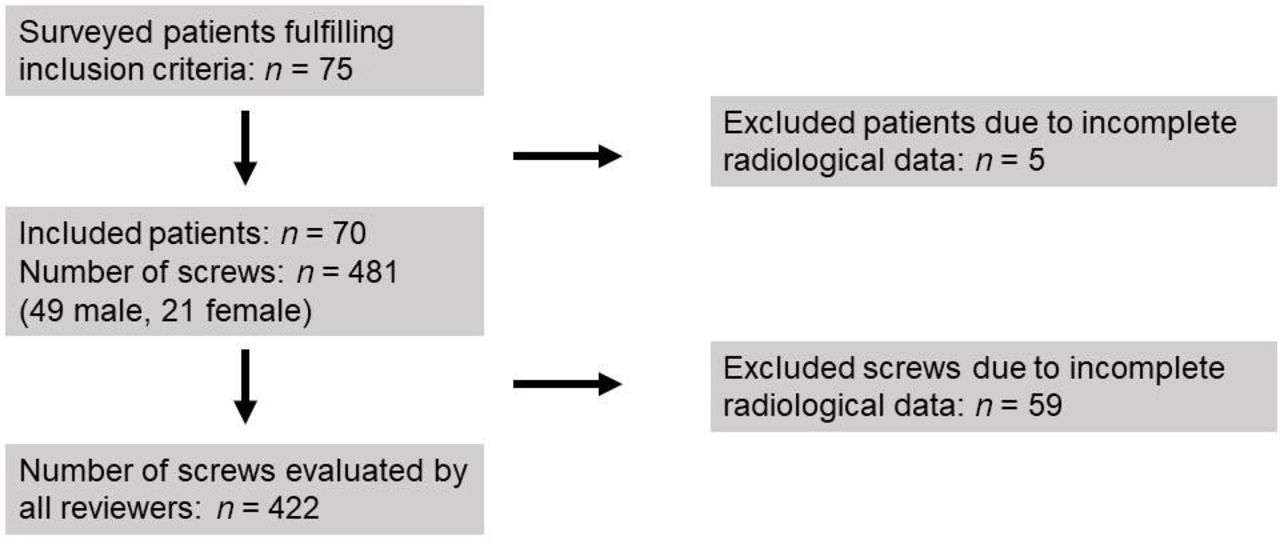
Flowchart of patient and screw inclusion.
Power analysis indicated a minimum sample size of 220 screws required to reach statistical significance (Supplemental Figure 1).15 The mean age was 61 years, and the ratio of men to women was 7:3. The indications for surgery were as follows: fractures (22 thoracic and 17 lumbar); tumor (11 thoracic and 8 lumbar); degenerative diseases (5 thoracic and 5 lumbar); and adjacent segment diseases (1 thoracic and 1 lumbar). The mean number of fused levels was 3, and the mean number of screws placed was 6. The surgery used either open, mini-open, or minimally invasive approaches, and all pedicle screws were placed using a 2-step navigation protocol (both pedicle probing and screw placement navigation). See Table 2 for more detailed description of demographics, including sex, age, and surgical indications for the patient group.
Overview of demographic distribution of study sample: gender and age distribution and indication for surgery (N = 70).a
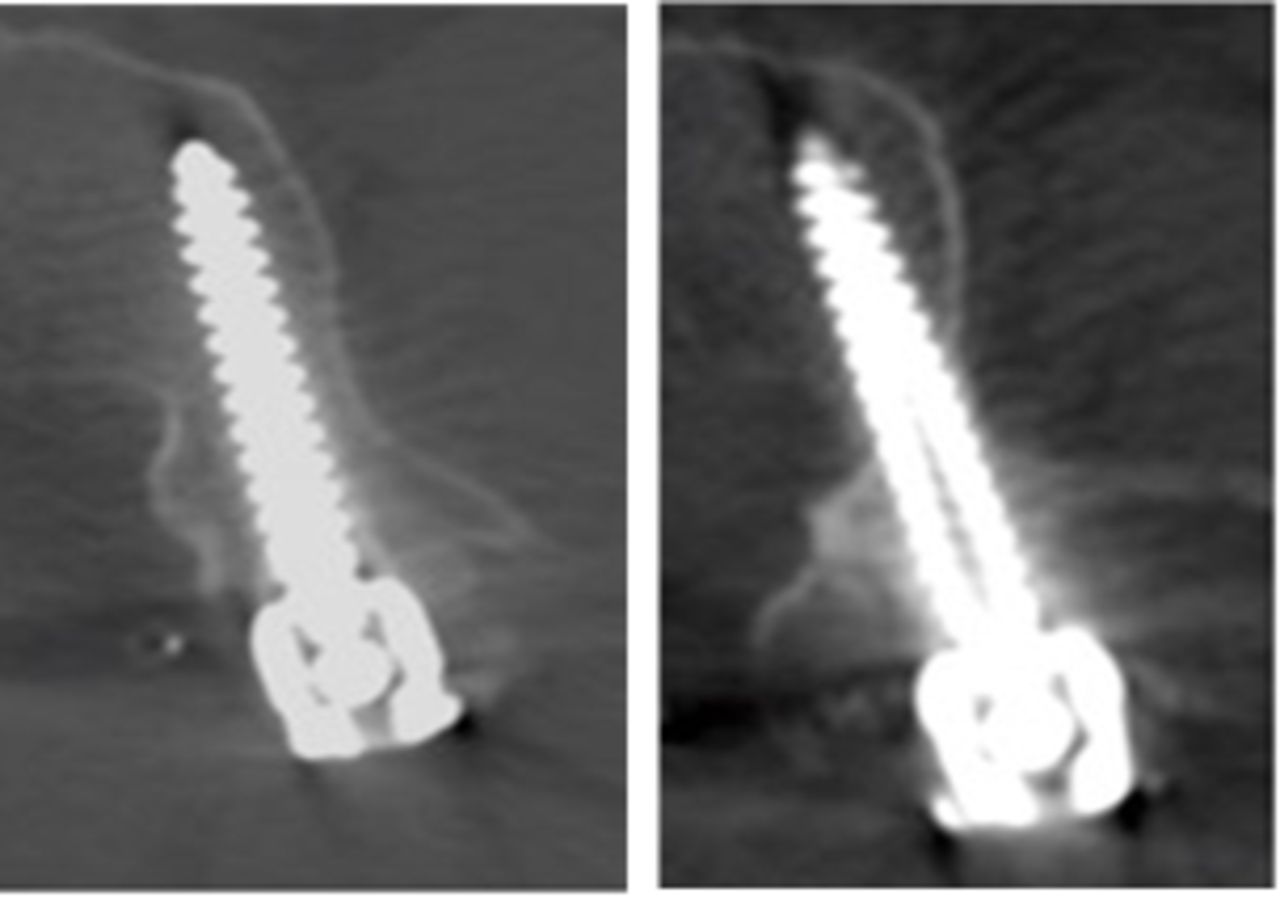
The pedicle screw placement assessment and rating were carried out according to the Gertzbein and Robbins classification system. The results were dichotomized and grouped as follows: Group 1: Grades A and B (0 to <2 mm breach) and Group 2: Grades C, D, and E (<4 to >6 mm breach; Figure 2). The 2 groups represent optimal placement (Group 1) and suboptimal placement (Group 2; Table 1).
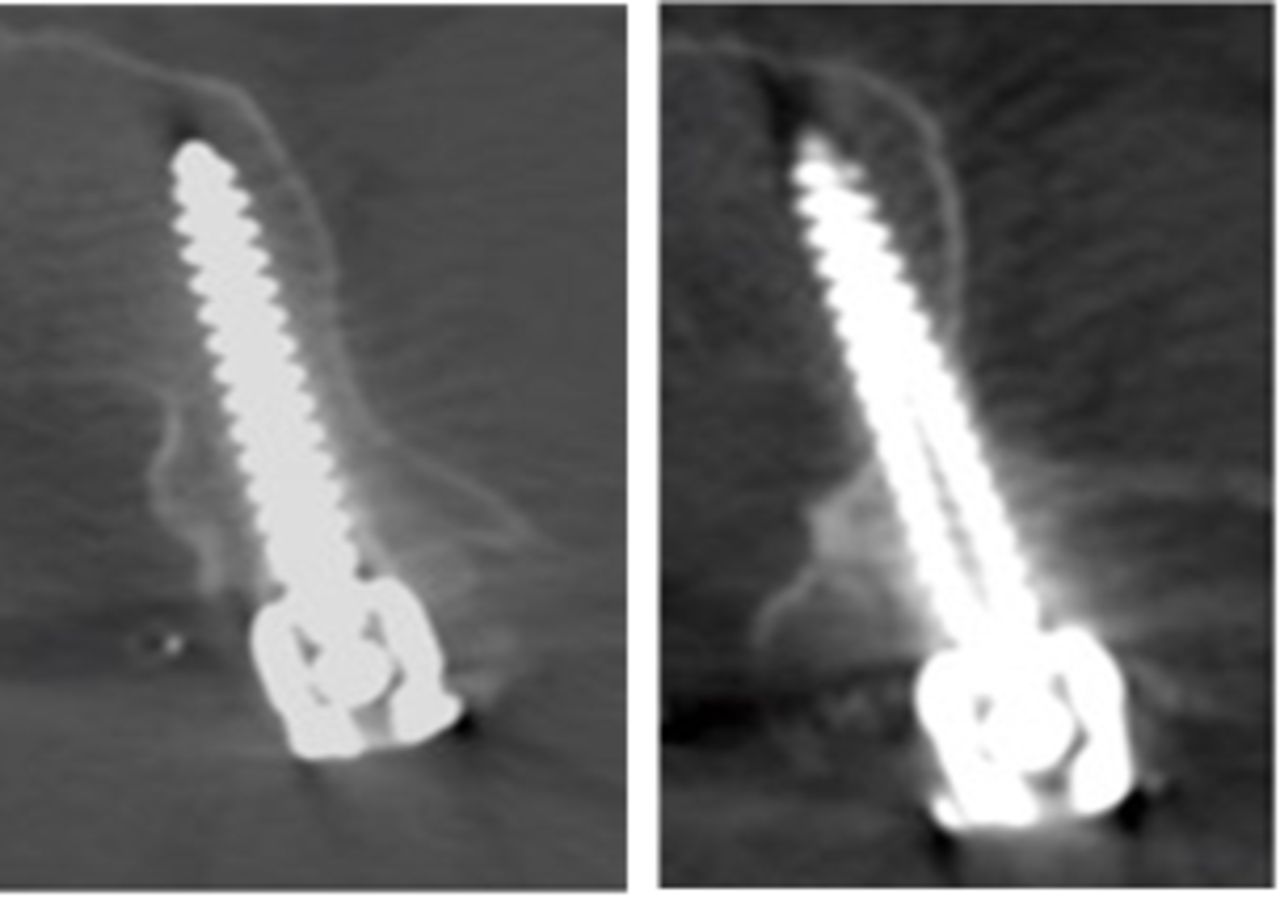
Example of screws rated as optimal (left; Group 1) or suboptimal (right; Group 2).
Table 3 provides a summary of the distribution of screws rated as Group 1 and Group 2 by all reviewers. The accuracy between the classifications of pedicle screws on IO and PO images by each reviewer was consistent and high: reviewer 1: 98% (95% CI [0.96–0.99]); reviewer 2: 99% (95% CI [0.97,0.99]); reviewer 3: 95% (95% CI [0.97,0.99.]; Table 3). Supplemental Table 1 provides an overview of the comparison of pedicle screw assessed in Group 1 and Group 2 by all 3 reviewers from IO and PO images and their compared accuracy (96%–97% for PO images and 97% for IO images).
Data distribution between optimal (Group 1) and suboptimal (Group 2) screw placement and accuracy (95% CI) of each surgeon reviewer’s assessment of IO (O-arm) and PO (CT) images.
The analysis of agreement, which was performed by AC1, compared ratings between surgeon reviewers from IO images and PO images; 96% to 98% (95% CI [0.94–1.00]) of the surgeon reviewers’ assessments agreed. Agreement was also studied between the individual surgeon reviewers and the neuroradiologists rating the PO images; these results show a 92% to 93% (95% CI [0.90–0.96]) agreement (Table 4).
Analysis of agreement using AC1 between surgeon reviewers from IO and PO images and between individual surgeon reviewers and the neuroradiologists rating the PO images.
The variance between ratings as optimal (Group 1) on IO images and as suboptimal (Group 2) on PO images might be considered an indication of a misplaced screw and could possibly lead to IO repositioning. The number of screws classified in Group 1 on IO images and in Group 2 on PO images by the reviewers was low: reviewer 1, 4 of 422 screws (0.95%); reviewer 2, 4 of 422 screws (0.95%); and reviewer 3, 7 of 422 screws (1.66%).
DISCUSSION
Posterior thoracolumbar spine stabilization using pedicle screws is the golden standard for treating many spine pathologies; however, pedicle screw misplacement can pose a risk to several vital structures such as vessels, nerves, and the spinal cord.16 Neurovascular complications may have devastating consequences for patients, such as bleeding, cerebral spinal fluid leakage, severe pain, and neurological deficit. Hicks et al found that the incidence of malposition of pedicle screws varies between 1.2% and 20%.17 Other studies on PO CT have shown the malposition rates to be around 16%.18
PO radiological examination can detect misplaced screws, which can potentially cause harm to the patient but also jeopardize the construct stability, leading to dislodgment, nonunion, and fixation failure. The Gertzbein and Robbins classification system is frequently used to classify pedicle screw positions on radiological images due to its simplicity. According to routine at our institution, all adult patients who undergo instrumented spine surgery are evaluated by neuroradiologists on PO CT images. However, in all cases, attending spine surgeons perform IO radiological control using IO 3D fluoroscopy images with O-arm. The IO assessment of the screw position enables detection of misplaced screws and allows for implant reposition while the patient is still in the operation room. This assessment enhances patient safety by mitigating the risk of PO revision surgery due to implant misplacement.
Metallic scattering artifacts are a source of error because they can obscure the screw contours and impede the assessment of the implant position. Rating pedicle screws on IO images may be advantageous as it allows for pedicle screws to be evaluated before the placement of additional implants such as rods, cages, wires, or hooks, eliminating further scattering artifacts. All IO images in this study were transferred to Sectra12 and reviewed therein, allowing for the built-in tools for scattering reduction to be applied for optimal image quality.
Screw misplacement can vary in degree. According to the Gertzbein and Robbins classification, only screws classified as A or B are optimal. In Gertzbein and Robbins’ original article, 167 thoracolumbar pedicle screws were rated using CT.11 The authors found 81% of screws were placed within 2 mm of the medial border of the pedicle, 6% were placed between 4 and 8 mm of the medial perforation violating the spinal canal, and 4% were placed with lateral perforation. Of the patients with >4 mm perforation medially, only 2 developed minor neurological complications. Of those with lateral breach, none developed related symptoms. The severity of a breach caused by a pedicle screw is not only determined by the rating but also by the clinical symptoms of the patients. Moreover, often the severity of the symptoms determines the need for revision surgery.
Our clinical experience is that the incidence of malpositioned pedicle screws has significantly decreased since image-guided spine surgery was established at our institution in 2013. This decrease can be explained by very high precision of screw placement due to strict navigation protocols. This explanation is confirmed in our study: most screws were classified as Group 1 A and B according to Gertzbein and Robbins classification. This data imbalance made statistical Kappa analysis unreliable. To overcome this obstacle, we performed the analysis as follows: To verify whether each surgeon reviewer rates consistently, we plotted crosstables over their pedicle screw ratings (Group 1 and 2) from IO and PO images and calculated the accuracy for each surgeon reviewer. This accuracy was shown to be high (95%–99%). We then continued by checking the compared ratings of all surgeon reviewers from IO and PO images as well as their accuracy (Supplemental Table 1). These results confirmed a high accuracy between reviewers (96%–97% on PO images and 97% on IO images). Then, we analyzed agreement between reviewers and between reviewers and the neuroradiologist reviewer to confirm that the ratings of pedicle screws by surgeons agreed with the ratings by other surgeons as well as with the neuroradiologists rating on PO images. These results showed agreement between 92% and 98%. The agreements with the neuroradiologist reviewer were between 92% and 93%, indicating a lower agreement than between surgeons (96%–98%). This discrepancy was not studied further.
The most important part of the study was to investigate the number of screws rated as Group 1 (Grade A or B) from IO images by surgeon reviewers and those rated as Group 2 (Grades C, D, or E) from PO images by the control reviewer, as this variance would suggest suboptimal screws being missed on IO images by surgeons. Suboptimally placed screws (Group 2) not detected on IO images and assessed as optimal (Group 1) would give a false reassurance of the correct pedicle screw position. We found only 0.96%–1.7% of the screws were mismatched between rating Group 1 on IO images and Group 2 on PO images. More importantly, none of the patients enrolled in the study developed any symptoms or complications related to screw malposition, and none were revised or reoperated due to screw misplacement. It is important to point out that the study does not account for screws being repositioned during surgery but only investigates the screw positions at the final IO 3D scan, which was saved in the patient’s file. In addition, the study does not consider pedicle screws intentionally placed with a violation of the pedicle wall (i.e., using techniques such as the in-out-in technique or instrumentation such as dysplastic and narrow pedicles).
Strengths and Limitations
The major strengths of this study are its prospective design and reviewers being completely blinded to each other’s assessments. The reviewers rated pedicle screws independently of each other based on the same instructions on classification using the Gertzbein and Robins classification system. To further minimize measurement bias between IO and PO images related to image recognition by reviewers, we presented all radiological images to the reviewers randomly in anonymized batches at different time intervals. The results from each reviewer were collected by first author (J.Å.), and statistical analysis was performed by second author, a statistician (A.B.). Neither J.Å. nor A.B. were involved in the radiological assessment and rating of the pedicle screw positions.
The biggest limitation was the data imbalance due to overall high precision of navigated screw placement according to assessment of the reviewers, which made Kappa analysis unreliable.
CONCLUSIONS
We conclude that there are several benefits to using a final IO 3D O-arm scan in the surgical protocol because our results show that IO imaging is reliable and sufficient to rate pedicle screw positions with high accuracy and detect potentially misplaced screws. Therefore, the requirement for PO CT imaging may be superseded, resulting in less radiation exposure, facilitating PO care, and lowering hospitalization costs without compromising patient safety.
Supplementary material
FIGURE S1.
Acknowledgments
The authors are grateful to Per Liv for contributing to the preliminary statistics of the project. Dimitrios Ikonomidis and Kajsa Burström, Department of Radiation Science at Umeå University Hospital, are also acknowledged for administering the radiological raw data for the study.
Footnotes
Funding Josefin Åkerstedt and Lukas Bobinski received research funding from the Medtronic External Research program for financing research time and costs linked to the research project.
Disclosures and Conflicts of Interest In addition to relationships disclosed under Funding, Lukas Bobinski has also received teaching honorarium from Medtronic. The remaining authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethics Approval Granted by the Swedish Ethical Review Authority, February 2019, Umeå, Sweden. Dno: 2019-00338. The analysis of data for this study was conducted in accordance with the Declaration of Helsinki.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.