


Abstract
Background The treatment of Kummell disease remains controversial, with a wide variety of options proposed in the literature. This study aims to introduce a unique and minimally invasive approach for the treatment of Kummell disease and present the clinical results of this technique.
Methods Twenty patients underwent surgery using the minimally invasive surgery transpedicular intrabody cage (MISTIC) technique from 2014 to 2016. Postoperatively, patients were seen at 3, 6, and 12 months after surgery. Visual analog scale and Oswestry Disability Index scores were collected, and patient outcomes were graded according to the modified MacNab’s criteria. Radiological outcomes were assessed through measurements of the anterior vertebral height (AH), mean vertebral body height (BH), and segmental angle (SA) on standing lateral radiographs pre- and postoperatively.
Results There was significant improvement in the SA, AH, and BH postoperatively. The SA improved from 15.2 ± 8.7° of kyphosis to 1.2 ± 5.2° (P < 0.01) in the immediate postoperative period. The AH increased from 13.3 ± 14.6 to 22.6 ± 12.2 mm (P < 0.01), and at the final follow-up, it was 21.9 ± 12.6 mm (P < 0.01). Similarly, the BH increased from 18.5 ± 6.8 to 25.6 ± 7.6 mm (P < 0.01) postsurgery, and at the final follow-up, it was 23.6 ± 4.4 mm (P < 0.01).
Conclusions The MISTIC technique offers significant correction of kyphosis and restoration of the vertebral anatomy following surgery. These results were maintained at 12 months postoperation, with a 100% union rate of the fractures. Additionally, patients experienced significant pain relief and improvement in their ODI scores that were maintained at 12 months.
Level of Evidence 4.
Introduction
Osteoporotic vertebral compression fractures (OVCFs) are common among the elderly population and typically occur with minimal or no trauma. Although most patients are treated conservatively, some patients develop avascular necrosis of the fractured vertebrae and require some form of intervention for symptomatic relief.1 Avascular necrosis of the vertebrae, also known as Kummell disease, is a progressive and disabling complication of OVCF due to failure of the healing process. Patients present with a delayed collapse of the fractured vertebral body and focal painful kyphotic deformity, which result in significant functional disability.2,3
The diagnosis of Kummell disease is made based on clinical features and imaging studies. Clinically, patients present with both progressive back pain and kyphotic deformity in the absence of significant trauma. Advanced imaging modalities such as magnetic resonance imaging (MRI) and computed tomography (CT) are required for the diagnosis of Kummell disease. Both MRI and CT help rule out other pathologies such as infection or malignancy, while the presence of an intervertebral cleft on MRI or CT is strongly suggestive of Kummell disease.4
The treatment of Kummell disease remains controversial, and a wide variety of options have been proposed in the literature. They include conservative treatment, corpectomy, and instrumented fusion with or without decompression.3,4 This study aims to introduce a unique and minimally invasive approach for the management of Kummell disease and present the clinical results of this technique.
Case Presentation
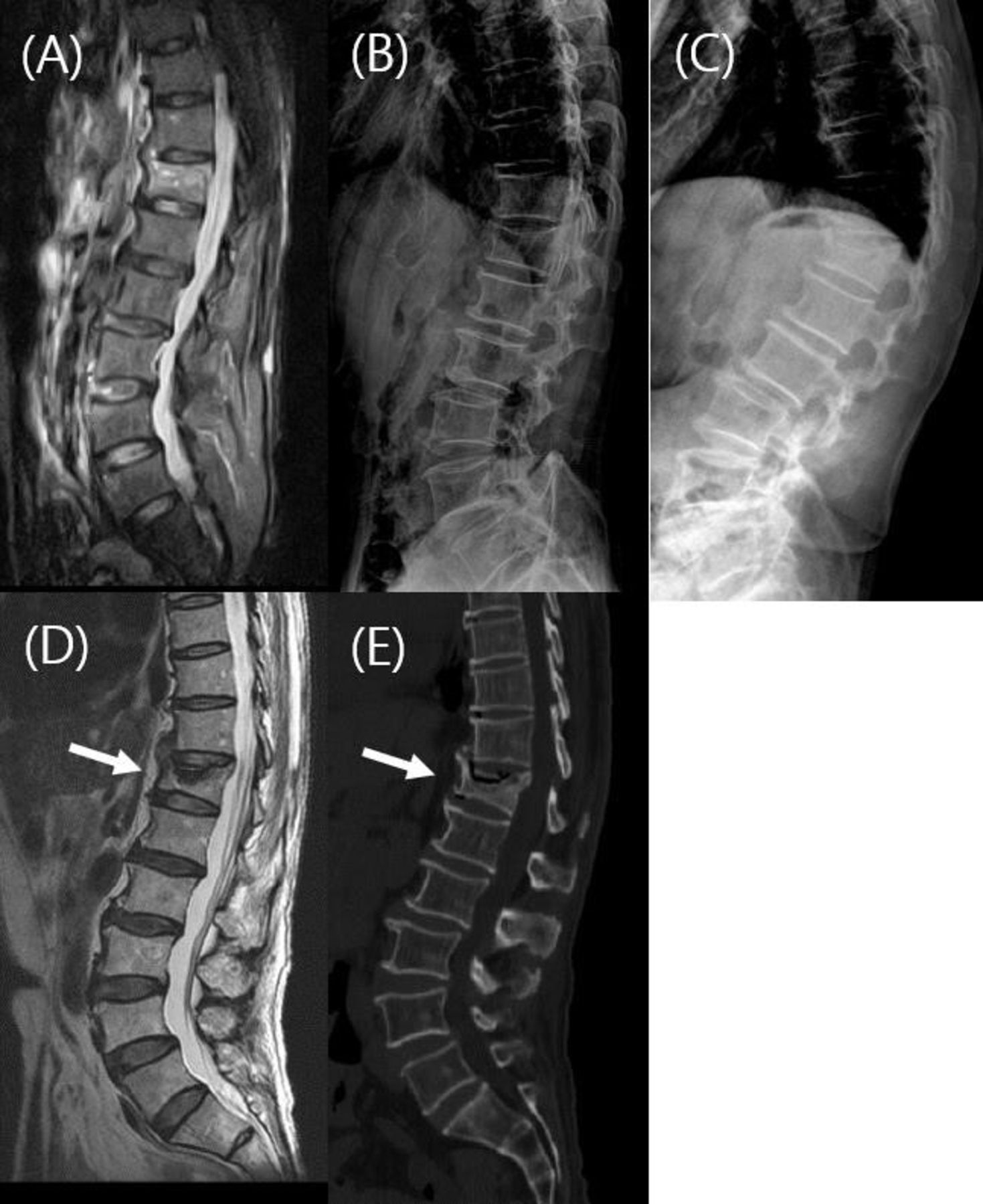
A 69-year-old man presented to our clinic with worsening back pain and increasing difficulty with ambulation over 4 months. He had a minor fall 4 months ago and he sought treatment at another hospital shortly after his fall. Radiographs and MRI were obtained at that time and revealed an acute T12 fracture (Figure 1A and B). He was advised for conservative management, but despite 2 months of bed rest, his back pain worsened and he was unable to walk because of the pain. On presentation to us, he had localized tenderness over the thoracolumbar junction and symmetrical motor strength in bilateral lower limbs with no sensory deficits.
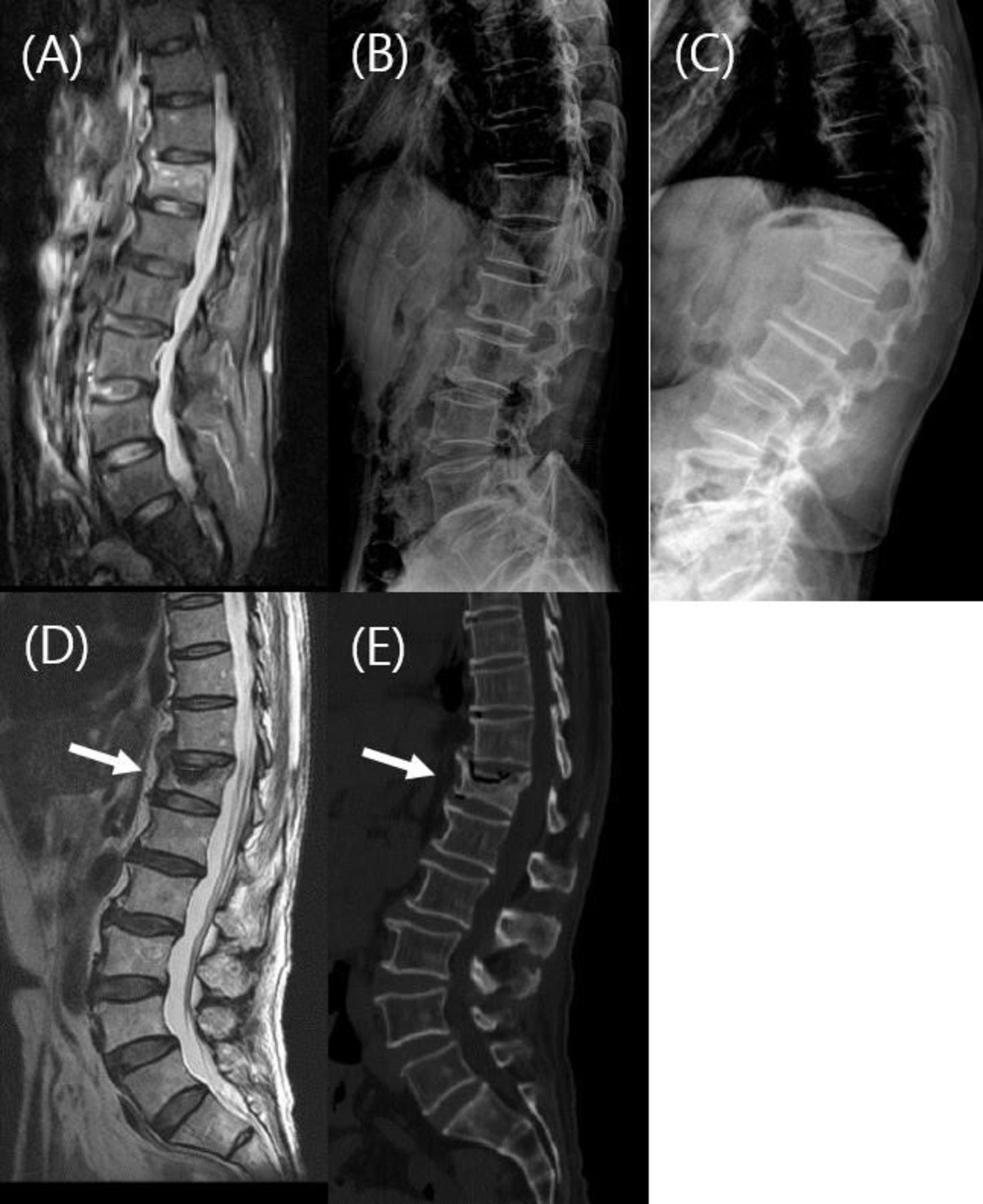
Initial magnetic resonance imaging (MRI) showing an acute T12 fracture (A). Initial lateral radiograph showing T12 fracture with superior endplate depression (B). Lateral radiograph after 4 months showing kyphotic deformity (C). MRI after 4 months showing intervertebral cleft sign (arrow) and kyphotic deformity (D). Computed tomography image after 4 months showing intervertebral cleft (arrow) and nonunion of T12 fracture (E).
Radiographs of the thoracolumbar spine were repeated, and they demonstrated interval collapse of the T12 vertebral body with worsening kyphotic deformity (Figure 1C). The MRI and CT demonstrated the presence of an intervertebral cleft and nonunion of the T12 fracture (Figure 1D,E). He was advised for surgical treatment given his progressive symptoms and failure of conservative management.
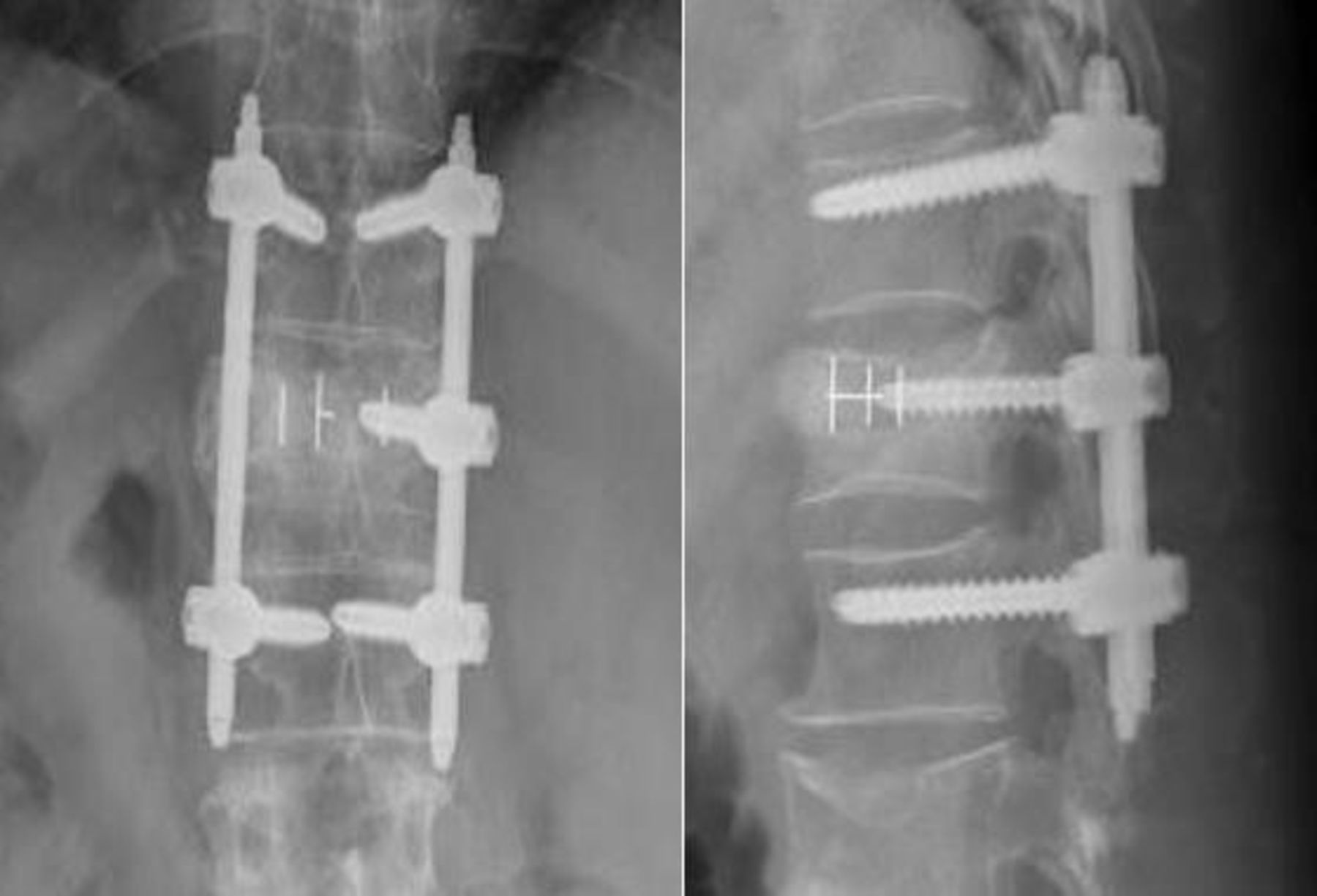
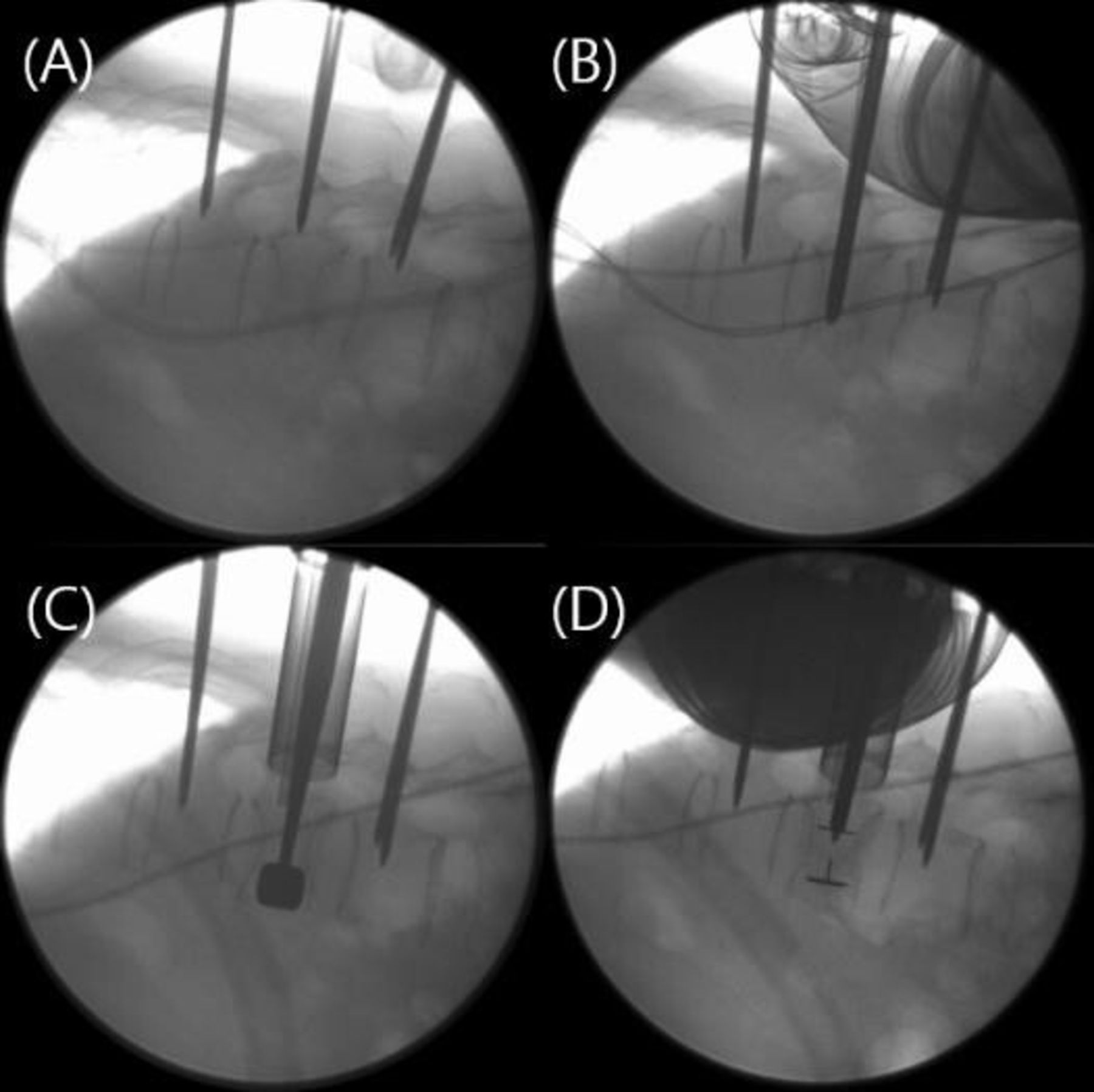
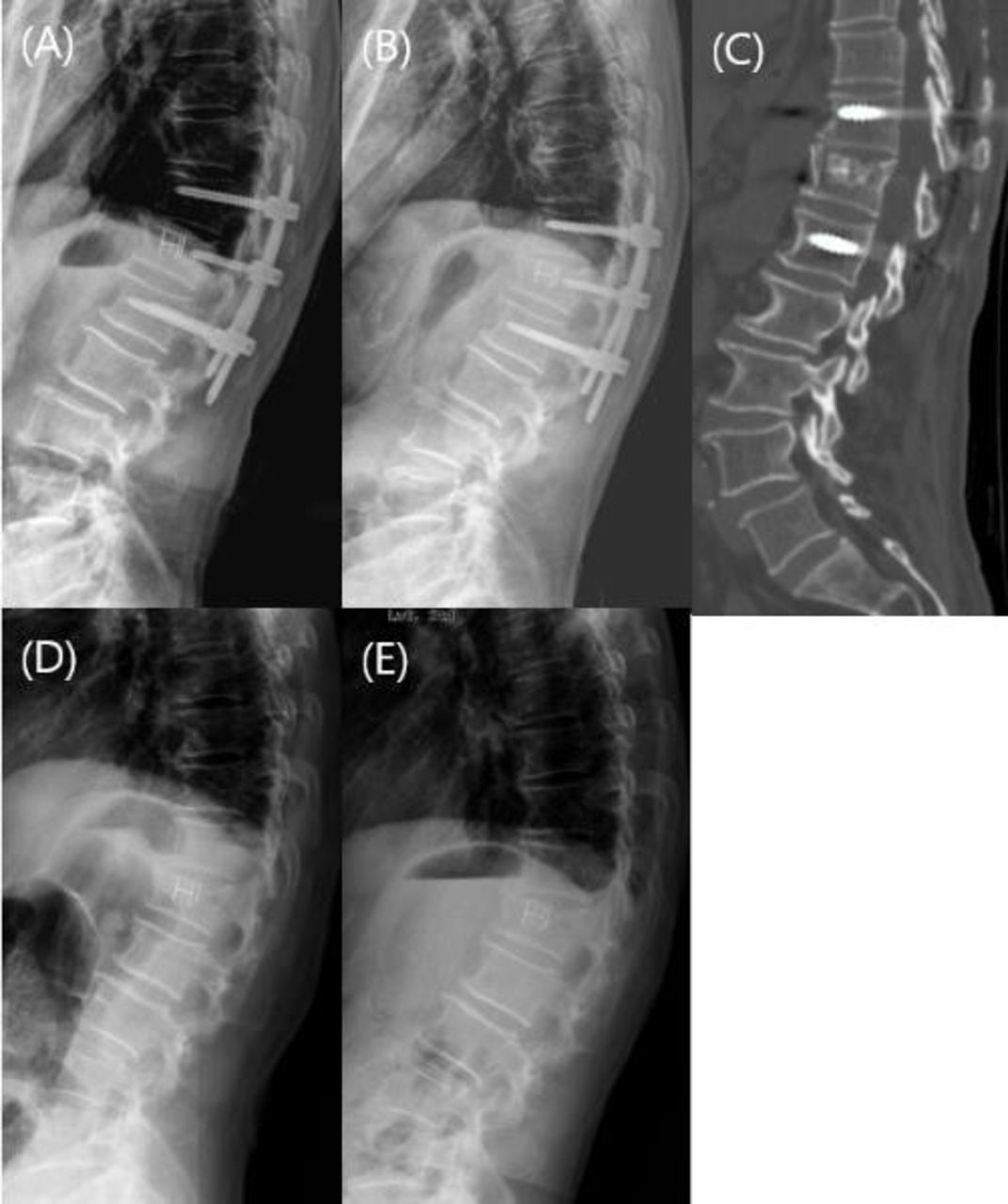
He underwent minimally invasive surgery transpedicular intrabody cage (MISTIC) insertion with posterior instrumentation to stabilize the fracture and correct the kyphotic deformity (Figure 2). Postoperatively, he had significant relief from his back pain, and his visual analog scale (VAS) score improved from 8 to 2. The radiographs taken after surgery showed significant correction of the deformity (Figure 3A), and the correction was maintained at 12 months postoperatively (Figure 3B). CT was performed at 12 months after surgery, the results of which demonstrated union of the T12 fracture (Figure 3C). The patient subsequently underwent removal of the implants due to the prominence of the screw heads. Radiographs taken after the removal of implants and 12 months later did not demonstrate any appreciable worsening of the kyphotic deformity (Figure 3D,E).
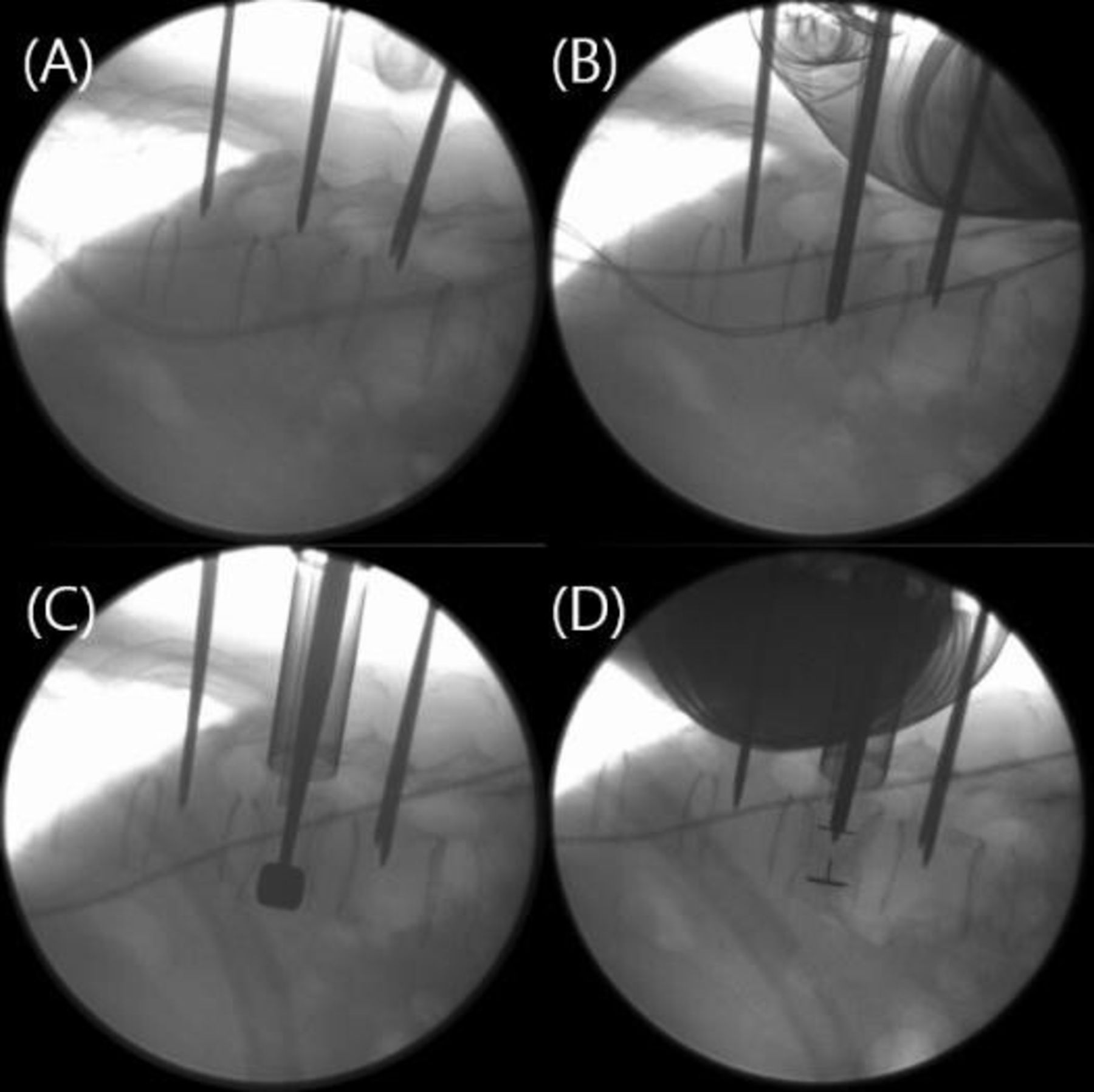
Intraoperative lateral radiograph after insertion of Jamshidi needles (A). Insertion of the METRx dilator through one of the pedicles at the fractured vertebrae. (B). Insertion of cage trial into the fractured vertebrae to restore the vertebral height (C). Postinsertion of crescent cage (Medtronic) demonstrates satisfactory vertebral height restoration (D).
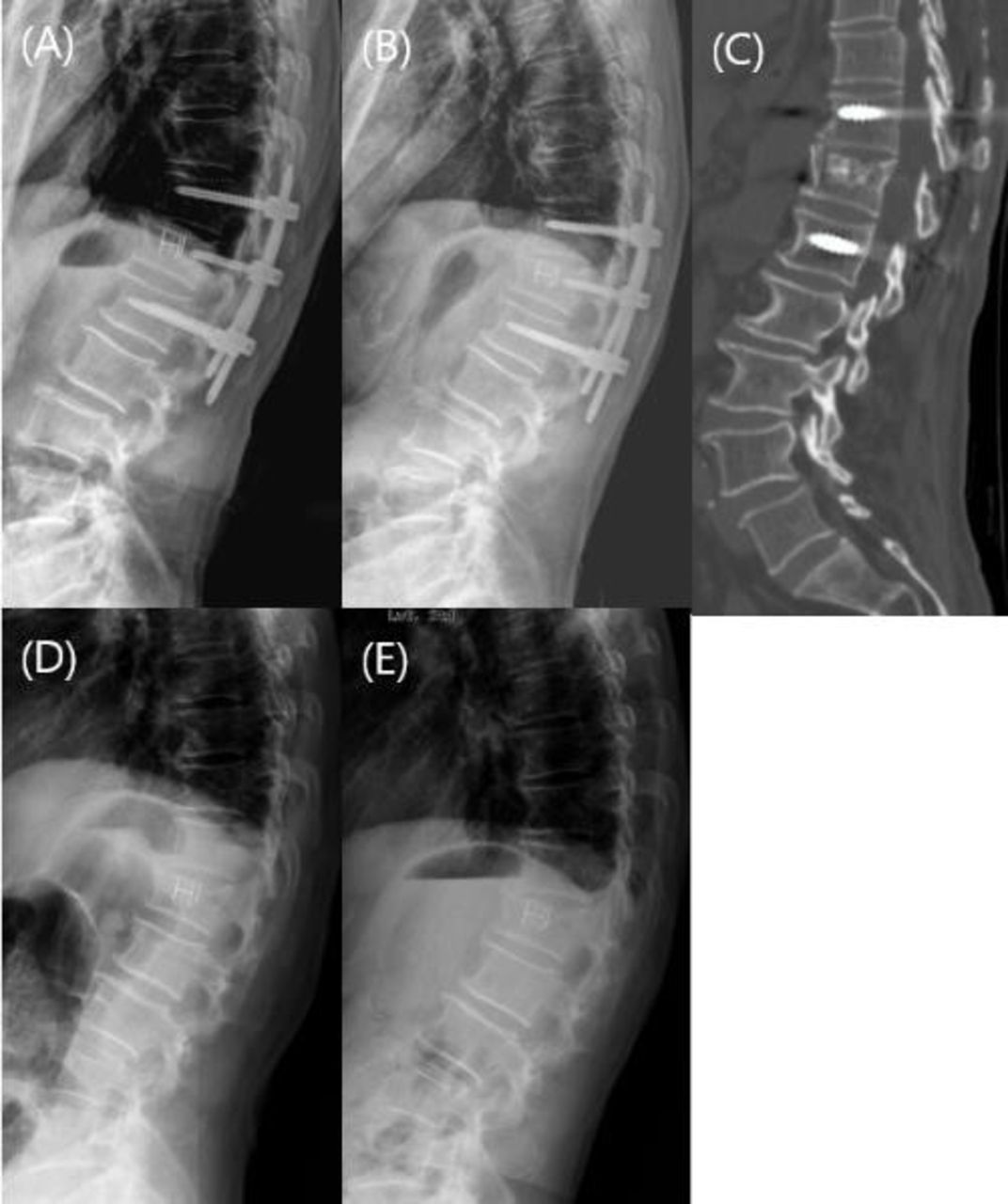
Immediate postoperative radiograph demonstrating correction of the kyphosis (A). Lateral radiograph at 12 months postoperation (B).The computed tomography at 12 months postsurgery demonstrating the union of the fracture (C). Radiograph immediately postremoval of implants (D). One year postremoval of implants (E).
Materials and Methods
A retrospective case review was performed after obtaining approval from our institutional review board. A total of 20 patients underwent surgery using the MISTIC technique at our institute from 2014 to 2016. Only patients with a diagnosis of single-level Kummell disease were included in this study. Patients with neurological deficits and multilevel fractures were excluded from this study. All patients presented with severe thoracolumbar pain that was unresponsive to conservative treatment. Radiographs showed the collapse of the vertebral body with kyphotic deformity, and preoperative CT and MRI showed intervertebral cleft with fluid collection. Patients were diagnosed with Kummell disease based on the CT and MRI findings together with the collapse of the vertebrae on radiographs. Postoperatively, 36-inch standing anterior-posterior (AP), lateral, and flexion-extension radiographs were obtained. Patients were seen at 3 months, 6 months, and 1 year after surgery. Radiographs were performed during each outpatient visit, and CT was performed 1 year after surgery to evaluate the status of fracture healing.
Patient-reported outcomes that were collected include a VAS score for back pain and the Oswestry Disability Index (ODI). Patient outcomes were graded as excellent, good, fair, and poor using modified MacNab’s criteria at the patients’ final follow-up visit. Radiological outcomes were assessed through measurements of the anterior vertebral height (AH), mean vertebral body height (BH), and segmental angle (SA) on standing lateral radiographs pre- and postoperatively. The measurements were performed independently by 2 spine fellows who were not involved in the surgeries. An average of the 2 measurements were taken as the final measurement. Other outcome measures that were obtained include operation time and intraoperative blood loss.
Surgical Technique
The patients were placed prone on a Jackson table with chest and thigh pads after general anesthesia that allowed for serendipitous correction of the kyphotic deformity. A left-sided approach is preferred for surgeons who are right-handed and vice versa. Under fluoroscopic guidance, a Jamshidi needle was inserted into one of the pedicles at the fractured level via a 2-cm incision. After confirming the satisfactory position of the Jamshidi needle on intraoperative radiographs, a guidewire was inserted through it and the Jamshidi needle was removed subsequently.
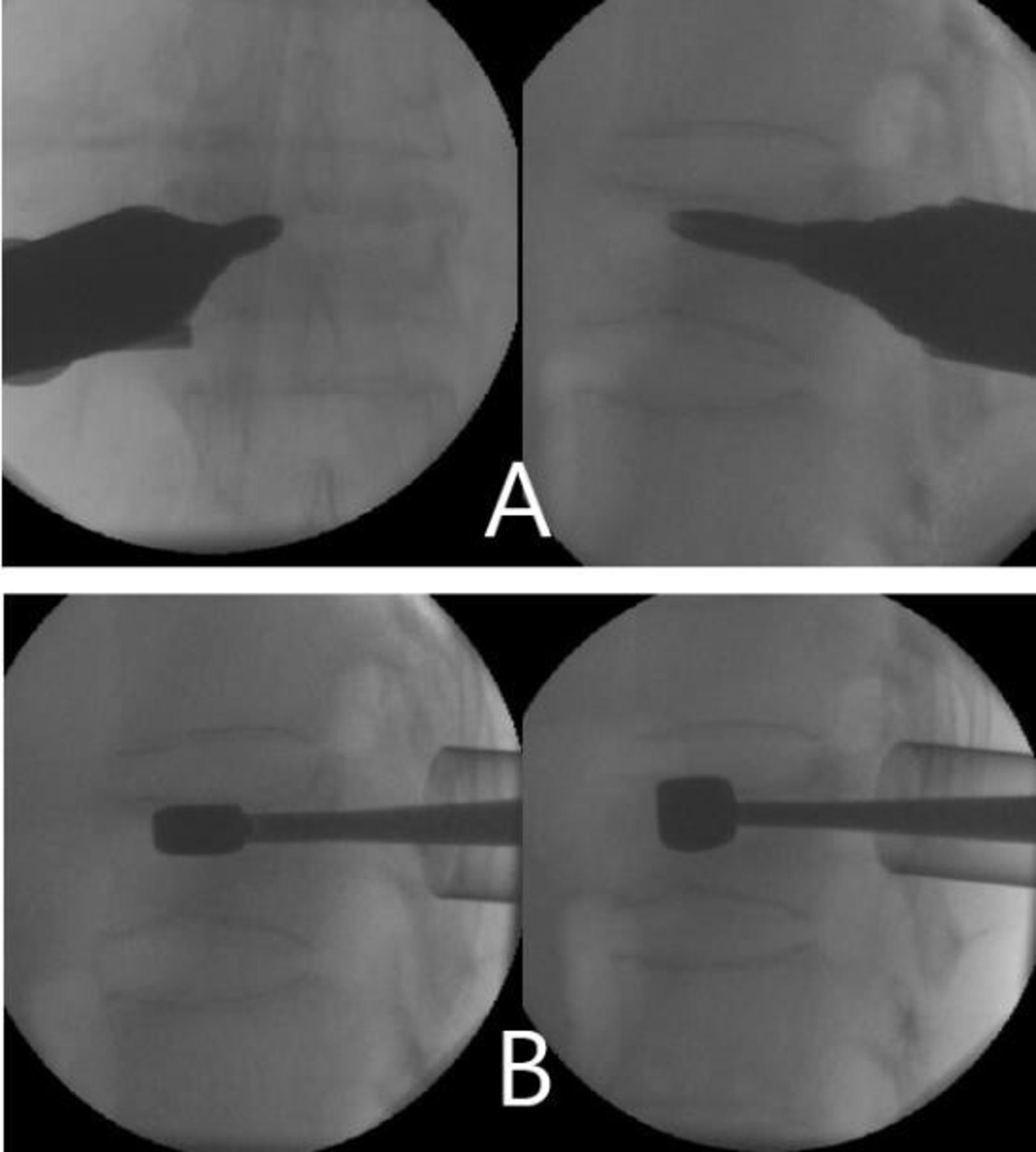
The fascia and muscles were dilated sequentially through the guidewire to allow for the placement of an 18-mm tubular retractor (METRx; Medtronic, Memphis, TN, USA) centered over the pedicle (Figure 4A). A tract through the pedicle and into the vertebral body was then created by using the smallest dilator or a large cannulated tap before the removal of the guidewire. Cage trials starting from the smallest size were introduced progressively through this tract and into the anterior column of the vertebral body (Figure 4B). It is important to insert the trial cages slowly once resistance is felt at the isthmus of the pedicle. This avoids fracturing the pedicle and allows creep to occur at the bottleneck junction. This is critical at the L1 and L2 vertebrae as the pedicles are smaller than the lower thoracic vertebrae. Radiographs were taken after the placement of each trial to assess the restoration of the vertebral body height. The corresponding size cage was selected once the vertebral body height had been adequately restored by the trial.
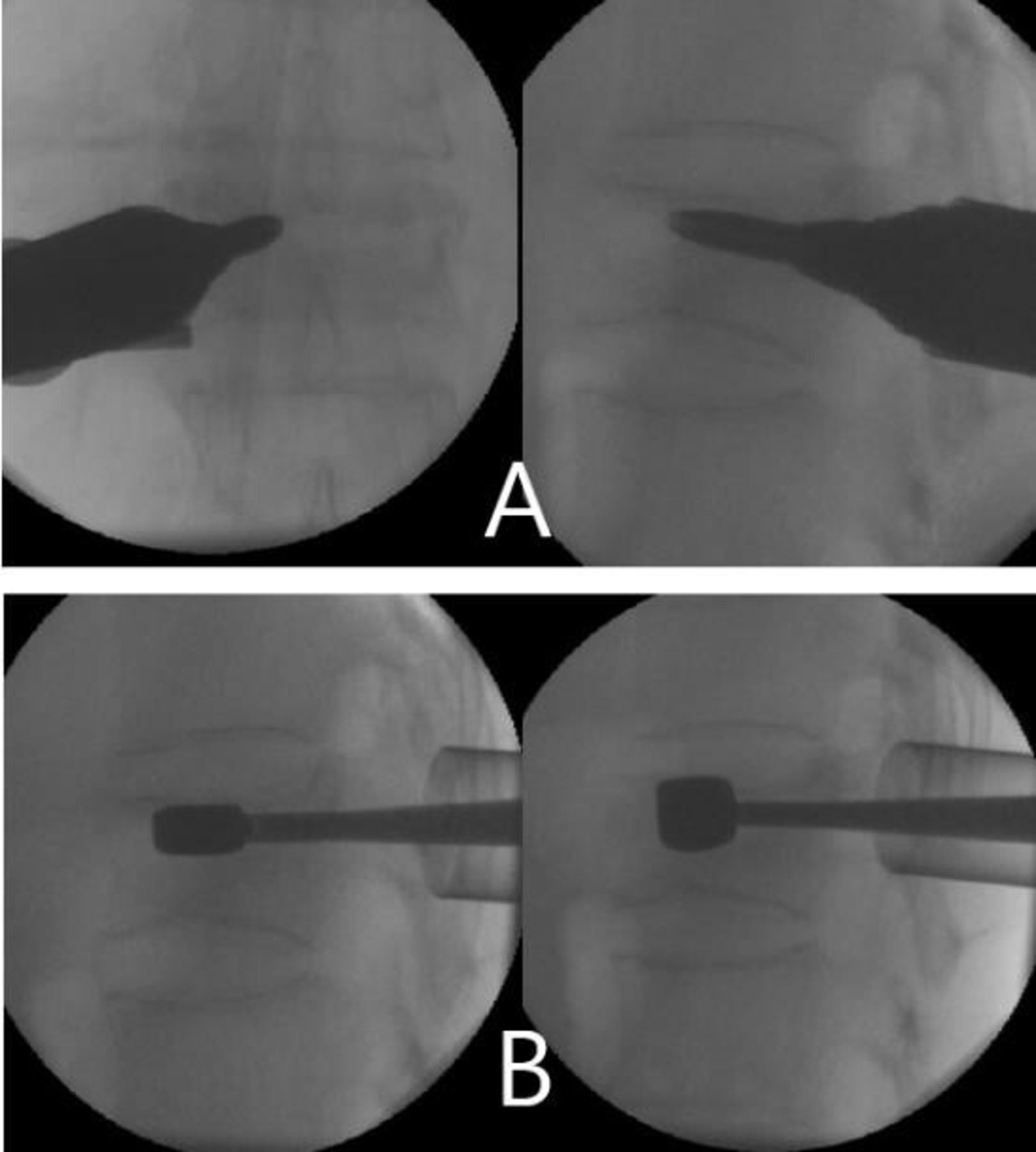
A tubular retractor is placed after serial dilatations via the guidewire (A). Serial cage trials were introduced into the anterior column of the vertebral body to restore the vertebral body height (B).
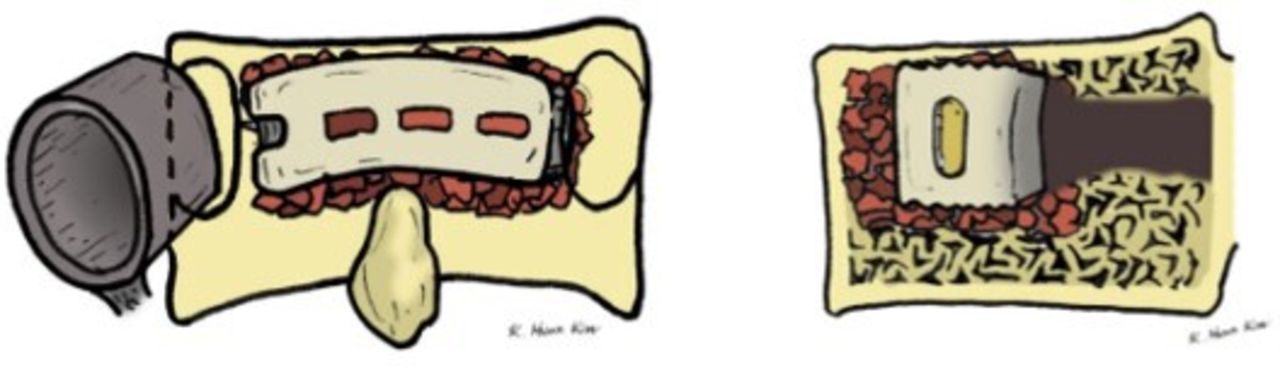
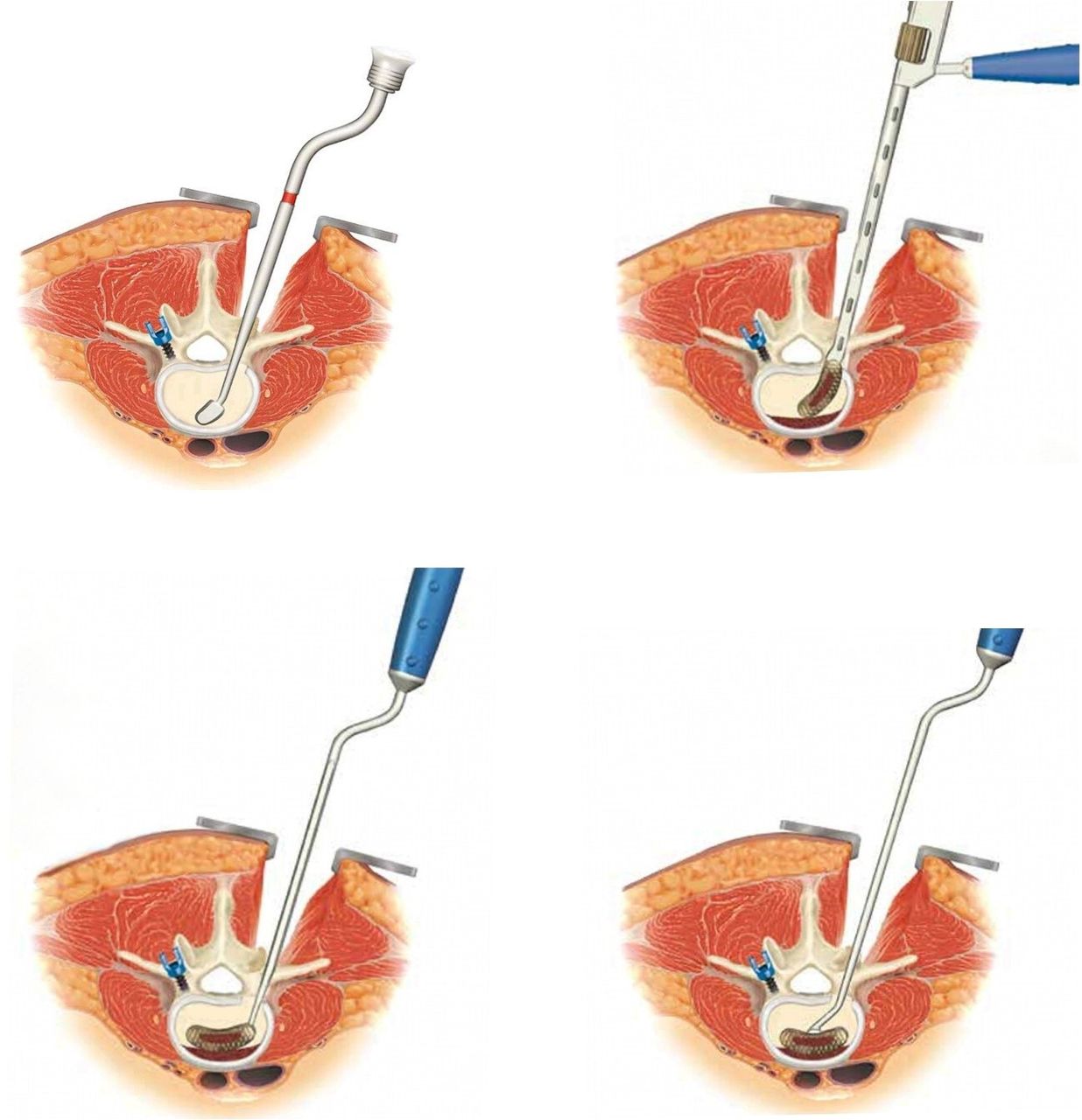
A banana-shaped polyetheretherketone (PEEK) cage (Crescent; Medtronic) packed with demineralized bone matrix (DBM) and allograft was implanted into the vertebral body in accordance with the manufacturer’s technique5 (Figure 5). The cage was first inserted obliquely into the vertebral body, and the cage inserter was subsequently removed. Using a ball-tipped or angled tamp, the cage was rotated into place through the gentle use of the mallet. The position of the cage was ascertained under fluoroscopy, and an anterior pusher was used to push the cage anteriorly if necessary5 (Figure 6). The remaining defect was filled with DBM and allograft bone chips, and the pedicle hole was packed with Gelfoam sponge. Percutaneous pedicle screws (CD Horizon Longitude; Medtronic, Memphis, TN, USA) were inserted one level cranial and caudal to the index level. A short pedicle screw (intermediate screw) was inserted at the index level into the contralateral pedicle for further stability. Titanium rods and set screws were inserted bilaterally, and compression or distraction maneuvers were performed as necessary (Figure 7). Last, the set screws were broken off, followed by removal of the extenders. The wound was subsequently closed without a drain.
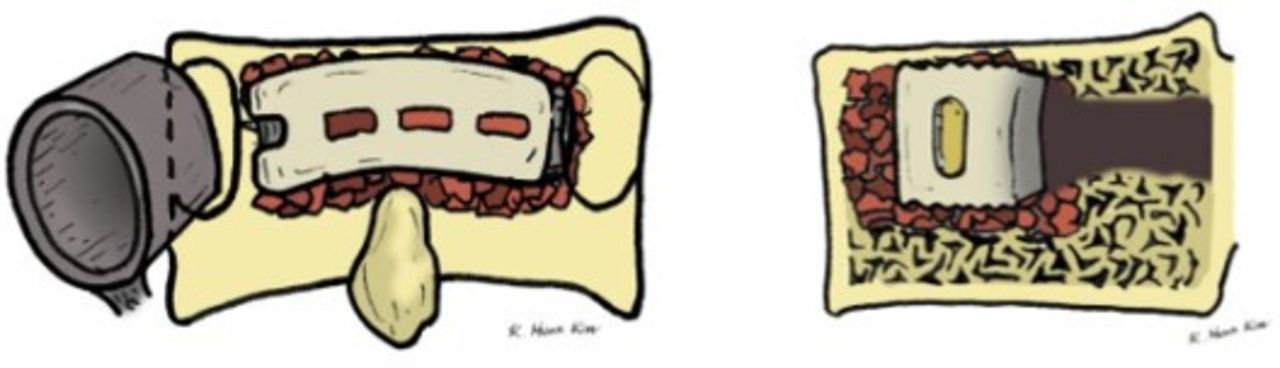
A banana-shaped polyetheretherketone cage filled with demineralized bone matrix and allograft was placed into the verterbae, restoring the height of the vertebral body.
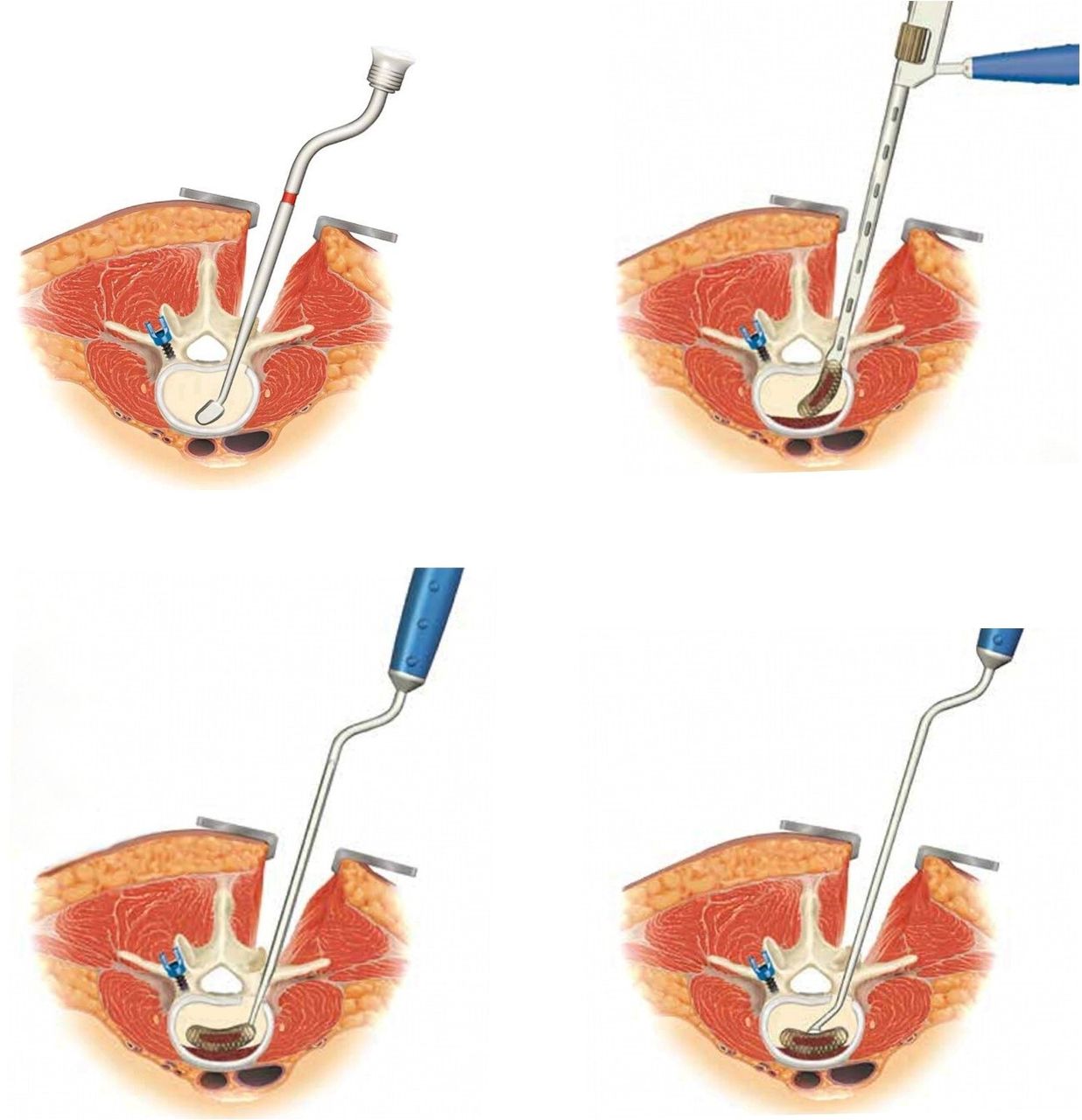
Progressive dilatation was first performed using sequential trials (A). The cage was inserted obliquely into the vertebral body using a cage holder (B). Using a ball-tipped tamp, the cage was rotated into place through the gentle use of the mallet (C). The position of the cage was ascertained under fluoroscopy, and an anterior pusher can be used to push the cage anteriorly if necessary (D).
A percutaneous pedicle screw was inserted into each pedicle at the cranial and caudal vertebrae. A short pedicle screw was inserted into the contralateral pedicle at the index level for further stabilization.
Statistical Analysis
A paired t test was used for the comparison of radiological and clinical outcomes between pre- and postoperative periods. A P value <0.05 was defined as statistically significant. All analyses were performed using SPSS 14.0K (SPSS Inc., Chicago, IL, USA).
Results
The mean age of the patients was 73.1 ± 6.1 years with 10 females and 10 males. The mean follow-up period was 18.4 ± 5.1 months. Intrabody cages were inserted from T11 to L3 with a mean surgical time of 118 ± 36.2 minutes and estimated blood loss of 216 ± 66.8 mL (Table 1).
Demographic data of patients.
There was a significant improvement in the SA, AH, and BH in the immediate postoperative period and at 12-month follow-up. The SA improved from 15.2 ± 8.7° of kyphosis to 1.2 ± 5.2° (P < 0.01) in the immediate postoperative period, and that improvement was largely maintained at the final follow-up. Although there was a mild increase in the kyphosis at the final follow-up, the mean SA was 3.6 ± 6.7° (P < 0.01), which was a significant improvement from presurgery (Table 2).
Radiological data.
Both the AH and BH increased significantly immediately after surgery, and the difference was maintained at 12 months. The AH increased from 13.3 ± 14.6 to 22.6 ± 12.2 mm (P < 0.01), and at the final follow-up, it was 21.9 ± 12.6 mm (P < 0.01). Similarly, the BH increased from 18.5 ± 6.8 to 25.6 ± 7.6 mm (P < 0.01) after surgery, and at the final follow-up, it was 23.6± 4.4 mm (P < 0.01) (Table 2).
All 20 patients showed union of the fracture at 12-month follow-up. CT at 12 months was not required in 8 patients because their radiographs showed union of the fracture and stable instrumentation at their final visits. Of the patients who underwent CT at 12 months, none showed loosening or haloing of the screws.
There were no complications in the perioperative period. VAS and ODI scores were significantly improved after surgery. The VAS had improved from 8.0 ± 0.9 before the surgery to 2.3 ± 0.5 (P < 0.01) at the final follow-up, while the ODI decreased from 43 ± 13.8 to 22.9 ± 15.2 (P < 0.05) (Table 3). Postoperative VAS and ODI scores were only collected at the 12-month follow-up as it would allow sufficient time for the fracture to heal and hence the scores would better reflect the patients’ definitive outcomes. One patient opted for the removal of implants at 12 months due to the prominence of the screw heads. At the final follow-up, 10 patients rated their clinical results as excellent (50%), 8 patients as good (40%), and 2 patients as fair (10%), according to the modified MacNab’s criteria.
Visual analog scale and Oswestry Disability Index scores.
Discussion
The incidence of vertebral compression fractures has been gradually increasing in South Korea due to an aging population and unique social and environmental factors.1 One of the complications of vertebral compression fractures is the development of avascular necrosis, which results in failure of fracture healing. This is also known as Kummell disease. While previously thought to be rare, there are increasing reports of Kummell disease in the literature. This condition causes 3 issues: (1) significant pain and functional disability due to instability at the fracture site, (2) kyphotic deformity, and (3) possible neurological compromise.2–4 The preferred treatment should ideally address all the issues that are presented by the patient.
The ideal treatment for Kummell disease remains controversial and therefore should be individualized according to the patient’s issues and preferences. Several treatment methods have been proposed for the management of Kummell disease. Vertebroplasty is a widely accepted minimally invasive procedure in the treatment of OVCFs, with many authors reporting successful outcomes even for patients with Kummell disease.3,6,7 However, cement leakage and loss of correction are common complications after vertebroplasty, with a greater incidence of cement leakage (75%) and recollapse of the vertebra in compression fractures complicated by osteonecrosis.8,9 Furthermore, there is evidence of progressive recollapse and worsening clinical outcomes over 2 years after vertebroplasty in such fractures.10 In a study by Heo et al, the kyphotic angle (SA) improved after vertebroplasty from 13.51° to 8.54°, but at 2 years after vertebroplasty, it returned to 13.62°.10 In comparison, the SA in our study improved from 15.2° to 1.2° postoperatively, and at 12 months, there was only a slight deterioration to 3.6°. The SA in our study is likely to be maintained in the long term as there is radiological confirmation (either CT or radiographs) of fracture union at the level of pathology. In another study by Ha et al, the ODI and VAS scores of patients with Kummell disease remained elevated at 48.5 and 4.5 points, respectively, despite vertebroplasty. Those patients had progressively poorer ODI and VAS scores of 55.4 and 5.9 points at the final follow-up, although it did not reach statistical significance.9 In our study, the ODI and VAS scores decreased significantly and remained low at 22.9 and 2.3 points at 12-month follow-up. Therefore, vertebroplasty might not provide the desired improvement in clinical outcomes or maintain its results in the long term.
In patients with neurological compromise, surgical treatment is preferred to decompress the spinal canal and stabilize the spine. Various surgical techniques have been proposed, ranging from the anterior approach alone, the combination of anterior and posterior approaches, to the posterior approach alone.11 Anterior approaches offer excellent reconstruction of the anterior spinal column and correction of the kyphotic deformity. However, 20% of patients still required posterior instrumentation due to the progression of kyphosis and early implant failure.12 Furthermore, most spine surgeons may not be familiar with anterior approaches because they are less commonly performed or an access surgeon may be required.
Both posterior long- and short-segment fusions have been utilized successfully to treat Kummell disease. In a meta-analysis by Yu et al, the authors concluded that both treatment methods are equally effective clinically, but short-segment fusions are inferior to longer constructs in maintaining their correction of kyphosis over time. None of the studies included in the meta-analysis described the insertion of an intrabody cage, while some studies performed vertebroplasty at the fracture site with posterior fusion.13 We believe that the addition of an intrabody cage provides increased stability and anterior column support, further augmenting the correction of the kyphotic deformity.
The insertion of intrabody cages in the treatment of Kummell disease had been reported in the literature previously.11,14,15 All studies reported good clinical outcomes and excellent correction of deformity, but all of the techniques were performed using an open surgical approach. To our knowledge, only 1 other article by Park et al described a similar technique.16 This is the first case series describing the treatment of Kummell disease using percutaneous or minimally invasive transpedicular insertion of an intrabody cage. In this study, we offer clinical outcomes and radiological results of at least 12 months to support the feasibility of this technique.
The MISTIC technique is an evolution of previous open techniques described by other authors and has several advantages. First, this minimally invasive surgical technique helps to avoid wide exposure-related complications, such as back muscle injury, bleeding, infection, and postoperative pain.17 Furthermore, the shorter operative time places less physiological stress on patients who are elderly or frail. This approach is also familiar to most spine surgeons, and the implants used are widely available.
Second, the intrabody cage offers the restoration of vertebral body height with anterior column support. There was only a mild reduction in the SA, AH, and BH at the final follow-up, and there were no cases of cage migration. The PEEK cage was filled with DBM and allograft, which promotes fracture union through its osteoconduction and osteoinduction properties. Additionally, this technique allows for the insertion of a pedicle screw at the fractured vertebra (intermediate screw) contralaterally, and this has been shown to improve biomechanical stability and reduce implant failures.18
There are several limitations of this study and technique. First, no fusion was performed at the instrumented levels. Although fracture union was achieved in all patients and the implants remained stable at the 12-month follow-up, there is a possibility that the pedicle screws may cut out or loosen over time due to motion at the unfused levels. However, this surgery aims to promote union of the fracture by using the instrumentation as an internal brace, and the implants can be removed once union is achieved. This allows for motion preservation but at the cost of requiring another surgery to remove the implants.
Second, there was no control group in this study and no comparisons were made between the MISTIC technique and other techniques. Thus, we are unable to prove that this technique provides significant advantages over existing techniques. However, it is well established that minimally invasive techniques lead to less blood loss and fewer complications, and this study’s technique provides some of the benefits associated with minimally invasive surgery.19
In addition, this technique alone may not be suitable for patients with neurological deficits, although the intrabody cage does allow for indirect decompression of the spinal canal through ligamentotaxis of the posterior longitudinal ligament (PLL) and correction of the focal kyphosis. By increasing the vertebral height, the PLL becomes taut, which reduces the retropulsed fragments caused by the fracture while correction of the kyphosis reduces the tenting and compression of the spinal cord. This principle is illustrated by Li et al, who showed that the reduction of the fracture alone is sufficient to decompress the spinal canal and therefore lead to neurological improvements.11 However, in our study, manual reduction of the fracture was not performed because we excluded patients with neurological deficits. For such patients, it may be possible to combine the MISTIC technique with manual reduction to eliminate the need for direct decompression.
Finally, this is a small study consisting of 20 patients with a short follow-up of less than 2 years. Although none of our patients had complications from this procedure, possible complications such as implant breakage, cage migration, nonunion, hematoma, and infection may occur. Larger studies are necessary to detect rare or uncommon complications such as adjacent segment fractures, major vessel injuries, major organ injuries, and others. Longer follow-up is necessary to detect loosening of the implants as no fusion was performed, and this may eventually lead to instrumentation failure or implant cut-out. Because this is a novel technique, further studies are also required to define the ideal indications and contraindications for this technique. Patients with single-level Kummell disease and without neurological deficits appear to be suitable candidates for the MISTIC technique.
Conclusion
The MISTIC technique offers significant correction of kyphosis and restoration of the vertebral anatomy following surgery. These results were maintained postoperatively at 12 months, and there was a 100% union rate of the fractures. In addition, patients experienced significant relief of pain and improvement in their ODI scores that were maintained at 12 months. We believe that this technique offers significant promise in the treatment of Kummell disease as there were minimal complications and the outcomes were reliable in the medium term. However, further studies are required to compare this technique with other procedures and to monitor the long-term outcomes of this technique.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Junseok Bae reports receiving support to attend meetings/travel from Joimax and
Medtronic. Junseok Bae and Sang Ho Lee serve in leadership roles for the Wooridul Spine Hospital. The remaining authors have no disclosures.
Disclosures The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.